
4
The Mammography Exemplar
WHY MAMMOGRAPHY IS A USEFUL EXEMPLAR
Strong evidence shows that health communication programs have played an important role in reducing disparities in mammography use among diverse groups. The committee chose mammography as an exemplar for this reason and several others. First, the risk of death from breast cancer, the most frequently diagnosed nonskin cancer among women in the United States, can be reduced significantly for women age 40 and older who get regular mammograms (see, e.g., National Institutes of Health Consensus Development Panel, 1997; American Cancer Society, 2001; Wingo, Calle, and McTiernan, 2000). Second, in 1987, when major promotions of mammography began, there were significant differences in use of mammography by age and ethnicity, including large disparities between African-American and white women. Over the past decade, these differences have been reduced so dramatically that national differences in screening rates for African-American, white, and Hispanic women no longer exist. Moreover, overall mortality from breast cancer has decreased,
partially because of increases in screening (Wingo, Calle, and McTiernan, 2000).
A third reason mammography was chosen as an exemplar is because variations still exist in incidence and mortality rates by age and ethnicity that require further attention. For example, although incidence rates are higher for white women with higher incomes, African-American women and women who have low incomes and lower levels of education have the highest mortality rates from breast cancer—a finding that is attributed partially to delayed diagnosis. Figures 4-1 and 4-2 show breast cancer incidence and mortality rates by race and ethnicity (National Cancer Institute, 2002; Edwards et al., 2002). Recent data (Caplan, May,
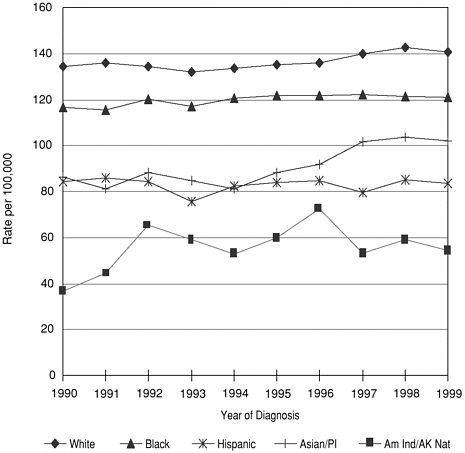
FIGURE 4-1 Breast cancer incidence rates by race/ethnicity, all ages.
SOURCE: National Cancer Institute, 2002.
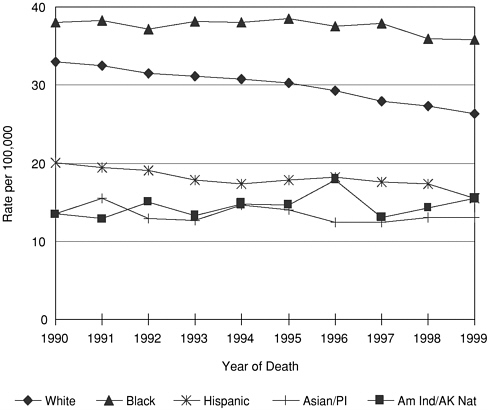
FIGURE 4-2 Breast cancer mortality rates by race/ethnicity, all ages.
SOURCE: National Cancer Institute, 2002.
and Richardson, 2000) indicate that African-American and Hispanic women had the longest intervals between abnormal mammogram and diagnosis of breast cancer, while Asian women and women in the “other/unknown” category had the longest treatment intervals.
A fourth reason for choosing this exemplar is that important lessons from mammography may be applied successfully to other health behaviors. These include the effectiveness of simple interventions, such as tailored and untailored reminders and brief counseling, that are effective for all populations. The addition of access-enhancing interventions improves mammography outcomes for diverse populations.
Most important, there is an extensive literature on interventions and their effectiveness for increasing the use of mammogra-
phy (e.g., Rimer, 1994; Snell and Buck, 1996; Wagner, 1998; Yabroff and Mandelblatt, 1999; Legler et al., 2002). This literature has three areas of strength: (1) studies have assessed a wide range of interventions both individually and in combination; (2) many of these interventions were grounded in behavioral and social science theory; and (3) many well-designed experiments have been conducted that provide solid outcome data. Moreover, many of the studies were directed toward or included diverse populations. When taken together, a strong case can be made for the effectiveness of several approaches to generally increase mammography use.
Although few studies were designed with enough statistical power to evaluate interventions in white versus diverse groups, a recent review of mammography-enhancing interventions for diverse women found that the same interventions that were effective for mainstream groups of women were effective for diverse groups, with the powerful exception of the addition of access-enhancing interventions for the latter group (Legler et al., 2002). Hundreds of useful mammography studies have been conducted. In this summary, we focus primarily on data from meta-analyses and other reviews of the intervention literature.
Before reviewing and assessing research on the design and evaluation of the interventions, we present a brief overview of (1) breast cancer incidence and mortality, with a focus on diverse populations, (2) the role of mammography in early detection and data on screening use, and (3) the common and culturally specific behavioral, geographic, and economic barriers to mammography use identified in the literature.
THE EFFECT OF BREAST CANCER ON DIVERSE POPULATIONS
In 2001, there were 203,500 new cases of invasive breast cancer and 40,000 deaths from breast cancer among women (American Cancer Society, 2001). These cases are disproportionately
distributed by age and ethnicity, as can be seen from the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) data and mortality data from the National Center for Health Statistics (National Cancer Institute, 2002) (see Figures 4-1 and 4-2). For example, more than three-fourths of all breast cancers are diagnosed in women age 50 and older (American Cancer Society, 2002). White women have the highest incidence rate for every age group, while Native American, Aleutian Islander, and Alaskan Native women are least likely to develop breast cancer (see Figure 4-1).
Although the racial/ethnic patterns for mortality differ only slightly from incidence patterns, the highest mortality rates are found among African-Americans, followed by white and Hispanic women (see Figure 4-2). SEER data from the National Cancer Institute (http://www.seer.cancer.gov/) suggest that the higher mortality rate for African-American women is partially because their cancer tends to be diagnosed later, when cancer is less amenable to cure (National Cancer Institute, 2002).
Progress is being made in the fight against breast cancer. In the last period for which comparisons were made, 1987–1999, there was a 0.5 annual percentage change (APC) in breast cancer incidence; the incidence increased, partially because of continued increases in mammography use. The incidence increase was 0.4 APC for whites and 0.9 APC for African-Americans (Edwards et al., 2002). In part, this probably reflects the somewhat later adoption of mammography by African-American women. From 1990 to 1998, breast cancer-related death rates decreased for white women (2.5 percent per year) and Hispanic women (1.2 percent per year), and did not change for African-American, Native American/Alaskan Native, and Asian/Pacific Islander women (Garguilly et al., 2002). In the latest statistics, from 1995 to 1999, breast cancer mortality decreased 3.2 percent per year for all ages, 3.5 percent per year for whites, and 1.2 percent per year for African-Americans (1993 to 1999). This reflects important improvement in reducing deaths from breast cancer.
THE ROLE OF SCREENING MAMMOGRAPHY IN THE EARLY DETECTION OF BREAST CANCER
Screening mammography is the most effective method for early detection of breast cancer (National Institutes of Health Consensus Development Panel, 1997). Strong evidence from randomized, controlled trials conducted around the world shows that regular screening mammograms can reduce breast cancer mortality by about 30 percent for women in their 50s and by 17 percent for women in their 40s (Hendrick et al., 1997; Berry, 1998). Thus, regular screening mammography is now recommended by most medical organizations for women age 40 and older (see, e.g., American Cancer Society, 2001; Eastman, 1997). Controversy remains, however, fueled most recently by a Lancet meta-analysis (Olsen and Gatzsche, 2001) that found no benefit from mammography for women of any age. However, reviews of this report have been conducted by the National Cancer Institute, the American Cancer Society, and other organizations. Despite the announcement that the U.S. Preventive Services Task Force will recommend regularly scheduled mammography for women age 40 and over, there is not widespread agreement among medical organizations that regular mammography should be recommended for women in that age group. Major efforts to promote screening mammography have been underway since 1987, with lead roles played by the American Cancer Society, National Cancer Institute, Centers for Disease Control and Prevention, associations of health professionals, and consumer advocacy groups, such as the Susan G. Komen Foundation and the National Alliance of Breast Cancer Organizations.
Since 1987, the proportion of women age 40 and over who report receiving regular mammograms has increased dramatically. The proportion of women age 40 and older who had a mammogram in the previous 2 years increased from 29 percent in 1987 to 68 percent in 1998. For women ages 50 to 64, the proportion increased from 34 percent to slightly over 75 percent during the same time interval (Breen et al., 2001). Data for 1998 show that
mammography use is now similar nationally for all ethnic groups— 68 percent for white women; 66 percent for African-American women; and 60 percent for Hispanic women. Increased use of mammography from 1987 to 1998 is also evident for different age groups, with the most striking changes noted among women over 60, whose rates have nearly tripled. However, some important disparities remain. For example, Wu, Black, and Markides (2001) recently reported that older Hispanic women were less likely than other women to have had recent mammograms and Pap tests.
However, there are still cultural groups for whom mammography use is lower. For example, in some areas of the United States, Hispanic women are less likely to have mammograms than women of other racial/ethnic groups (Breen et al., 2001). Recent immigrants also have lower use. In some areas of the country, such as eastern North Carolina, African-American women have lower rates of screening (e.g., O’Malley et al., 2001). A recent analysis of Behavioral Risk Factor Surveillance System (BRFSS) data with a focus on Appalachian women found that rates of mammography use were slightly below the U.S. population. Women over age 60, those with less than a high school education, and women who had not seen a doctor in the past year were also less likely to have had mammograms (Hall et al., 2002). Coughlin and Uhler (2002) reported BRFSS data from the United States and Puerto Rico for Hispanic women. The findings were similar in terms both of proportion screened and the variables that predicted underutilization. These data highlight the importance of educational and economic characteristics as determinants of screening. As Coughlin and Uhler stressed, more efforts are needed to provide access to services for the medically underserved.
The lowest mammography rates currently are found among women who have low incomes (rates are between 43 and 54 percent, depending on age) and who do not have high school diplomas (between 47 and 58 percent, depending on age). For example, women age 50 and older who live below the poverty line are 21 percent less likely than women living above the poverty line to have had a mammogram in the previous 2 years. Also, women in
this age group who do not have a high school education are 20 percent less likely to have had a mammogram in the previous 2 years compared to women with a high school education or higher (Breen et al., 2001). Screening rates are also lower among women who lack health insurance. There are other predictors of screening rates, but these are among the most important. However, in spite of the remarkable increase in the proportion of women who report ever having had mammograms, as well as having had recent mammograms, most women still are not getting regular mammograms (Breen et al., 2001).
PREDICTORS OF MAMMOGRAPHY USE IN MAINSTREAM AND DIVERSE POPULATIONS
This volume presents an integrative model that summarizes key concepts from various behavioral theories (see Chapter 2). We use this theoretical model to highlight the factors that have been important in predicting use of mammography. We examined the factors that seem to be shared across diverse populations as well as those that appear to be unique to one or more groups. Understanding these issues is important to determine whether audience segmentation is needed for diverse populations. We focus our discussion on three elements of the integrative model that have the most relevance for mammography use: (1) attitudes and beliefs toward mammography screening; (2) perceived norms; and (3) environmental influences. The literature on predictors of mammography has less to say about the role of self-efficacy (personal agency), intention, and skills in women’s compliance with recommendations on screening mammography. This is partly because, unlike changing diet, mammography, while volitional, is primarily under the control of health professionals. Some studies (e.g., Ryan et al., 2001) have asked women if they feel confident they could get a mammogram if they wanted to do so and have provided tailored advice in this area.
Our review and analysis of the literature on factors that influence the use of screening mammography are organized in accor-
dance with this integrative model. We covered a large number of peer-reviewed articles published between 1985 and 2000, with a focus on identifying variations among diverse groups. As noted earlier, although we reviewed articles that reported the results of individual studies, as well as meta-analyses, this chapter relies primarily on meta-analyses and reviews. There are a series of well-executed reviews that cover the literature. As the sections to follow show, many similarities exist between the general population and diverse groups in terms of their response to communication interventions. In fact, there are many more similarities than differences. In general, there are probably as many variations among women in any ethnic, income, or other group as between groups. Where differences were identified, they will be highlighted.
Attitudes and Beliefs
Knowledge, attitudes, beliefs, and behaviors are important factors that motivate people to take appropriate health actions. Most theories agree that getting a mammogram is partly a function of one’s beliefs that performing the behavior will lead to certain outcomes. It is assumed that a person will not perform a behavior (or form an intention) if the costs of performing the behavior outweigh the benefits. Thus, the most commonly used models in some way assess women’s perceived pros and cons or their perceptions of the benefits of and barriers to getting mammograms. Knowledge is a part of some behavioral theories, such as the Health Belief Model (Strecher and Rosenstock, 1996), and has been a consistent predictor of mammography use.
In 1987, when mammography use was significantly lower than it is today for all groups of women, the National Health Interview Survey reported that the most common reasons women gave for not having mammograms were (1) they had not thought about it; (2) it was not necessary because there were no problems/no symptoms; and (3) it had not been recommended by a physician (Rimer, 1994). Overall nationally, these are the most important attitudes and beliefs about mammography, regardless of age, ethnicity, in-
come, or education, although some regional differences exist. Mammography use is higher among women who understand the purpose of mammography, especially its value in the absence of symptoms, and the recommended age-based intervals (McDonald et al., 1999; Lee et al., 1999; Maxwell, Bastani, and Warda, 1997, 1998a, 1998b; Wismer et al., 1998; Fernandez, Tortolero-Luna, and Gold, 1998; Rimer, 1994). This is true across populations, including African-American and Hispanic women (e.g., Valdez et al., 2001). Older women who recognize that age is the most important risk factor for breast cancer and that older women are more likely to get breast cancer are more likely to report having had mammograms (Fox, Murata, and Stein, 1991; Fox, Roetzheim, and Kington, 1997). Similarly, physician knowledge of screening recommendations is an important predictor of physician practices, although this factor has received less attention in the literature (Fox, Roetzheim, and Kington, 1997).
A recent report indicated that Hispanic women were more likely than non-Hispanic women to agree with the statement that once you get cancer you will always die from it (Puschel et al., 2001). Health providers reported that Hispanic women were more likely than non-Hispanic women to resist breast exams, which providers ascribed to women’s fears of anything that might threaten their integrity as women (Puschel et al., 2001). Other studies have shown that older Hispanic women know less about breast cancer screening than other women (Puschel et al., 2001; Calle et al., 1993; Lantz et al., 1994; Stein and Fox, 1990; Fox et al., 1998). Most recently, Valdez et al. (2001) showed that Hispanic women who were more fearful were less likely to have had recent mammograms. In general, the low levels of knowledge about cancer screening among Hispanic women are more likely to be accounted for by socioeconomic factors, such as low education and low income, than by acculturation, language, or ethnicity (Zambrana et al., 1999; Schur, Leigh, and Berk, 1995; Fox and Roetzheim, 1994). Indeed, language is not a major barrier to screening if health care is accessible (Zambrana et al., 1999).
Further evidence of the role of cultural beliefs in women’s decisions to have a mammogram has been observed across cultural groups, including a reluctance to use Western health care among Chinese-American women (Facione, Giancarlo, and Chan, 2000); cultural beliefs about fate among Filipino Americans (Maxwell, Bastani, and Warda, 1997) or karma among Cambodian-American women (Taylor et al., 1999b); concerns about modesty (Schulmeister and Lifsey, 1999; Dibble, Vanoni, and Miaskowski, 1997; Kelly et al., 1996); and beliefs that breast cancer is tied to guilt and punishment among Arabian women (Brushin, Gonzalez, and Payne, 1997).
Perceived Norms
The factors discussed in this section include perceived norms about mammography—influences from providers of health care services, family, and community groups. Norms include the overall perception about what most “important” others are saying and doing about the behavior. According to a number of reviews (Snell and Buck, 1996; Wagner, 1998; Rimer, 1994; Rimer et al., 2000a), the strongest predictor of mammography use is a recommendation or referral from a physician, arguably the most “important other” in relation to recommended medical practices such as mammography. This finding is consistent across all ethnic and age groups (Burack and Liang, 1989; McDonald et al., 1999; Maxwell, Bastani, and Warda, 1997; Risendal et al., 1999; O’Malley et al., 1999). Moreover, this finding has been robust over time. Valdez et al. (2001) reported the importance of a doctor recommendation for low-income Hispanic women. Some studies indicate that women in lower socioeconomic areas who receive their health care from emergency rooms and clinics are less likely to be advised to have mammography recommended by their health care providers (Snell and Buck, 1996). O’Malley et al. (2001) noted that only about half the women in their study of low-income women in North Carolina reported that their physicians had advised them to have mammograms. White women were more likely to report such
recommendations than African-American women (55 percent versus 45 percent, odds ratio = 1.49). When education and income were controlled, the race difference disappeared. However, socioeconomic characteristics were related strongly to use of mammography.
A number of studies conducted in community health centers indicate that women in these settings are being screened at higher rates than the general population (e.g., Rimer et al., 1996; Zapka et al., 1993). Lower screening rates are found for Asians/Pacific Islanders who are treated by physicians of similar origin. Perhaps their providers reinforce the cultural belief that screening is needed only when changes in the breast are found through clinical examination (McPhee, 1997a, 1997b; Wismer et al., 1998). Thus, there is variation in the proportion of diverse women who report being advised by their providers to get mammograms. Women who have regular providers, including those at community health centers, are more likely to report having had mammograms when their providers advised them to do so. Also, women who report more physician visits are more likely to report having had mammograms (Wu, Black, and Markides, 2001). This is understandable because more visits may represent more opportunities to make a recommendation about and referral for mammography.
The patients’ ability to communicate effectively with their providers about cancer screening also influences screening practices. Patient age, for example, influences communication with physicians. Physicians are less likely to recommend screening mammography to older patients than to younger patients (Fox, Roetzheim, and Kington, 1997).
Another important factor in encouraging the use of breast cancer screening by women is the behavior of people around them— that is, the norms for performing the behavior within women’s social networks. Women who perceive that more of their friends and relatives had mammograms are more likely to have mammograms themselves (e.g., Rimer, 1994; Kang and Bloom, 1993; King et al., 1993). This finding is consistent across age, ethnic, and other diverse characteristics. One study found that Asians were
more likely to have screening mammograms if they perceived that family and friends were also having them and were supportive (Maxwell, Bastani, and Warda, 1997). Another study suggested that African-American women with large social networks were more likely to have mammograms than those without large networks (Kang, Bloom, and Romano, 1994). The way in which larger networks may operate to increase mammography use is not well understood.
Environmental Influences
A range of environmental influences may either pose barriers to or facilitate women’s use of mammography screening. Lack of access is the most important environmental influence for women with a lower socioeconomic status, especially those who live in rural areas (Breen et al., 2001). These findings are confirmed across all ethnic groups (Mickey et al., 1995; Pinhey, Iverson, and Workman, 1994; Serxner and Chung, 1992; Morgan, Park, and Cortes, 1995). One study (Kreher et al., 1995) reported that urban and rural women did not differ in their expressed intent to have mammograms in the next 2 years, but nearly twice as many urban women as rural women reported having had mammograms. Similar concerns have been observed for other groups as well; Kelly and colleagues (1996) reported that barriers for Cambodian women who should be getting mammograms included lack of transportation and fear of a large, technical medical center.
Indeed, access also may involve issues of comfort with health care systems. Women who do not speak English may have difficulty navigating the health care system, as shown by Morgan, Park, and Cortes (1995) in a study conducted on disadvantaged Hispanic women living in Bronx, New York. Foreign-born Hispanic women who are recent immigrants to the United States (and who have low levels of acculturation) are less likely to use mammography than Hispanics who have lived here for some time (O’Malley et al., 1999). Access factors may account for these differences, however. Indeed, access to screening appears to be a stronger pre-
dictor of screening than language and ethnic factors—indicators of acculturation. Like all women, Hispanic women with access to health care are more likely to be screened than are women without access to health care. A disproportionate percentage of Hispanic women, however, are low income; Hispanics are also more likely to report health insurance inadequacies and poorer quality of life, factors that are likely to interfere with maintenance of screening behaviors (Fox and Roetzheim, 1994; Zambrana et al., 1999). Nonetheless, whereas financial costs and inadequate reimbursement are barriers to screening, interventions directed only at screening costs have not been particularly effective in the absence of patient education. Indeed, even when the poor have adequate health insurance, they encounter more barriers to screening than upper income groups (Fox, Roetzheim, and Kington, 1997).
It is important to consider the assets and resources on which women of diverse groups may draw. As noted in the following sections, interventions can be designed to build environmental supports for screening. System-directed, access-enhancing, and policy-directed interventions provide important means of building these supports; indeed, access-enhancing strategies, including the provision of transportation or free mammograms, play a particularly crucial role in increasing screening rates.
THE IMPACT OF MAMMOGRAPHY-ENHANCING INTERVENTIONS ON DIVERSE POPULATIONS
This section provides a brief overview of the major findings on interventions designed to facilitate use of mammography screening. In 1994, Rimer reviewed the trends in interventions in the United States in the following areas: mass media campaigns (e.g., A Sa Salud project), individual directed (e.g., letters from physicians, mailed reminders, telephone counseling, posters), system directed (e.g., systemwide prompts, computer-generated reminders), access enhancing (e.g., mobile vans, special programs with cost subsidies), social networks (e.g., community-based programs such as Save Our Sisters), policy directed (e.g., changes in regula-
tions), and various combinations of the strategies listed. Selected interventions in each of these areas have made a positive impact on mammography use. This review places health communication interventions, such as mass media campaigns and individual-directed communication, in the broader context of public health interventions, including those aimed at contextual influences and environmental constraints.
As discussed throughout this volume, broad groupings—such as by race, ethnicity, or age—provide little information on which to base intervention development. Rather, women’s life experiences and social contexts, regardless of their age or ethnicity, play important roles in their attitudes and beliefs toward mammograms, in the social norms and environmental constraints they experience, and in the potential impacts of health communications. It is important to incorporate this information into the development of interventions for diverse groups of women. For example, understanding and addressing women’s barriers to and concerns about screening have contributed to effective interventions delivered to shoppers at Asian grocery stores (Sadler et al., 2000) and among Cambodian women (Kelly et al., 1996).
Meta-Analysis Methods
We relied on meta-analyses conducted by Meissner et al. (1998) and Legler et al. (2002) for this review; other reviews and meta-analyses provided confirmatory information (Yabroff and Mandelblatt, 1999; Yabroff et al., 2001; Bonfill et al., 2001).
Meissner et al. (1998) used Rimer’s (Rimer et al., 2000a) categories to examine the critical elements included in the published literature on breast and cervical cancer interventions. Of 528 studies identified, 58 screening mammography articles met the inclusion criteria: (1) the study measured the impact of an intervention to increase use of mammography and/or Pap smears in asymptomatic populations, and (2) the study focused on mammography; those focusing exclusively on breast exams (self or clinical) or an abnormal finding were eliminated. For each study, Meissner and
colleagues assessed the presence and quality of the reported needs assessment, intervention, study design, analysis methods, and study outcomes, specifically:
-
From 1960 to 1997, most studies were system/physician directed, individual directed, and access enhancing. There was one social network intervention, and no policy interventions.
-
Of the 58 studies, 21 were based on a behavioral theory. The largest number used the Health Behavior Model, followed by Social Learning Theory and the Stages of Change Model.
-
Studies were conducted in 20 of the 52 states and territories.
Legler et al. (2002) conducted a meta-analysis to determine which types of mammography-enhancing interventions are most effective for groups of women with historically lower use of mammography. The groups include the following categories under the label “diverse”: high school education or less; low income (defined by study authors); ethnic or racial group; age 60 or older; and/or living in a rural or inner-city area. Studies in any of these categories potentially were eligible for inclusion if they met other inclusion criteria as well. Ideally, one would want to compare the same interventions for diverse and mainstream populations, but the studies were not constructed to facilitate such analyses. Based on principles of targeting and tailoring, the interventions developed for diverse women often have had elements or nuances specific to those populations. Similarly, interventions developed for mainstream populations may have had insufficient numbers of diverse women for subgroup analyses. Here we first present the results of a meta-analysis to answer the following question: What is the effectiveness of different mammography-enhancing interventions for specific populations of diverse women? Then, we compare these results to the more general mammography meta-analysis literature in order to extract some lessons about how intervention effectiveness varies when the general literature is compared to that for diverse populations.
The methods for the meta-analysis are described more fully elsewhere (see Meissner et al., 1998, and Legler et al., 2002). Briefly, using accepted meta-analytic methods, the authors conducted extensive searches of the literature, then constructed a database of the 51 studies that focused on breast cancer screening. Articles that were retained in the analysis were those that met the following criteria:
-
Objectives were to increase use of mammography among asymptomatic women in diverse populations;
-
Reports of intervention outcomes were based on actual receipt of mammograms, either by self-report or verified report in a clinical database or medical record; and
-
Studies used experimental or quasi-experimental designs.
Ultimately, 38 controlled, experimental, and quasi-experimental interventions that specifically focused on or reported separate mammography outcomes for diverse populations were included in the meta-analyses.
Interventions were categorized according to Rimer’s (Rimer, 1994; Meissner et al., 1998; Rimer et al., 2000a) typology: access enhancing (e.g., transportation to appointments, mobile vans, vouchers, and reduced-cost mammograms), system directed (e.g., provider prompts), individual directed (e.g., one-on-one counseling, tailored and untailored letters and reminders, telephone counseling), community education, social network (e.g., peer leaders, lay health advisors), mass media, and multistrategy interventions (see Table 4-1).
The outcomes were study-specific adherence rates. The definition of adherence was provided by each study author. This allowed for the inclusion of a wider range of studies both with respect to followup time and study type. Because the field has been evolving, definitions have changed over time. Generally, study outcomes typically were described as obtaining a mammogram within a specified number of months; the time period varied from study to study.
TABLE 4-1 Estimated Intervention Effects
|
|
|
Combined Estimate Difference |
|
|
|
Intervention Type |
Number of Studies |
Unadjusted (95-percent confidence intervala) |
Adjusted for Monthsb |
Combined Estimate Odds Ratio (95-percent confidence intervala) |
|
Access enhancingc |
14 |
18.9 (10.4, 27.4) |
16.5 |
2.3 (1.7, 3.1) |
|
Individual directed associated with a health care setting |
15 |
17.6 (11.6, 24.0) |
14.1 |
2.5 (1.9, 3.4) |
|
Individual directed associated with a community setting |
13 |
6.8 (1.8, 11.8) |
7.0 |
1.3 (1.0, 1.6) |
|
Community educationa |
14 |
9.7 (3.9, 15.6) |
10.4 |
1.5 (1.2, 1.9) |
|
Media Campaignsa |
6 |
5.9 (0.3, 11.5) |
11.4 (1.0, 1.8) |
1.3 |
|
Social Networka |
7 |
5.8 (-0.2, 11.9) |
13.0 |
1.4 (1.0, 2.0) |
|
Estimated combined effect sizes with confidence limits for each intervention type. Random effects models. Studies may be classified as implementing more than one type of intervention. Entire group comparisons for primary outcomes. aConfidence intervals only approximate because cluster randomization is not taken into account. bModel includes outcome months. cControl groups do not include strategies of the same intervention type. |
||||
Results of Meta-Analysis for Diverse Populations
As the preceding sections of this chapter demonstrate, many effective interventions have been developed over the past decade. A substantial body of research has focused on identifying and overcoming women’s, physicians’, and system barriers to mammography (e.g., Rimer et al., 2000a; Meissner et al., 1998; Calle et al., 1993; Clemow et al., 2000; Fox, Roetzheim, and Kington, 1997; Hiatt and Pasick, 1996; Lane et al., 2000; Rimer, 1994; Vernon, Laville, and Jackson, 1990; Yabroff and Mandelblatt, 1999; Mandelblatt and Yabroff, 1999; Bonfill et al., 2001; Yabroff et al., 2001; Sin and Leger, 1999). In addition, there have been striking gains in U.S. mammography use by age-eligible women (Martin et al., 1996; Breen and Kessler, 1994).
A reasonable question is whether the interventions that have been developed to date for mainstream populations are effective for diverse populations of women. Often an assumption is made that special interventions are needed for diverse populations—that is, that health communications to segmented audiences will be more effective than generic communications. It is important to examine the data because the development of special interventions requires resources that many communities lack. Several recent meta-analyses of mammography interventions have shown that relatively simple interventions, such as reminder letters, telephone calls, and counseling, increase mammography use across population groups (Yabroff and Mandelblatt, 1999; Mandelblatt and Yabroff, 1999; Snell and Buck, 1996; Wagner, 1998). This is an important finding. However, the meta-analyses conducted to date have not focused on strategies most effective for diverse groups of women. Several authors of the meta-analyses mentioned this and called for a greater focus on diverse populations (Yabroff and Mandelblatt, 1999; Snell and Buck, 1996; Wagner, 1998; Bonfill et al., 2001). However, until recently, there were not enough studies to permit analyses by various subgroups.
Table 4-1 shows mammography effects by intervention type. Access-enhancing interventions had the greatest impact on mam-
mography use, with an estimated intervention effect of 18.9 percent (95-percent confidence interval [CI]: 10.4-27.4; 14 studies). These studies all used multiple types of interventions; the majority involved some form of person-to-person contact in addition to access-enhancing strategies, such as mobile vans, transportation to appointments, facilitated appointments, and vouchers for low-cost or free mammograms. A recent report by Segura et al. (2001) supports this conclusion. The authors found that for low-income women in Spain, the combination of a personal letter of invitation and direct contact with women in their homes by a trained woman of similar age was most effective in motivating women to get mammograms.
The magnitude of the impact of individual-directed interventions in health care settings was nearly identical to that of access-enhancing strategies, with an estimated effect of 17.6 percent (95-percent CI: 11.6-24.0; 15 studies) (see Table 4-1). Individual-directed efforts in community settings yielded effects of 6.8 percent (95 percent CI: 1.8-11.8; 13 studies), whereas effect sizes for community education, media campaigns, and social network were 9.7 percent, 5.9 percent, and 5.8 percent based on 14, 6, and 7 studies, respectively.
The use of multiple intervention types was effective, with intervention effects averaging 13.3 percent overall (95-percent CI: 8.6-18.0; 26 studies). With the exception of social network interventions, the estimated intervention effects were significantly greater than zero for all of the groupings. However, each grouping exhibited significant heterogeneity. The most effective combination of intervention types appears to be access-enhancing interventions combined with individual-directed interventions. These studies had an estimated combined intervention effect of 26.9 (95-percent CI: 9.9-43.9; 9 studies). The next largest effect was for the 5 studies combining access-enhancing and system-directed interventions; their effects were 19.4 (95-percent CI: 8.2-30.6). Caution should be used in interpreting these results because the number of studies available to examine pairs of combinations was quite small.
Additional analyses were conducted to examine the combined intervention effects for specific diverse populations (see Figures 4-3 and 4-4). The estimated intervention effect was greatest for older women—7.9 percent (95-percent CI: 10.5-25.4; 11 studies)—followed by an estimated effect of 12.7 percent (95-percent CI: 7.3-18.1; 26 studies) for comparisons consisting of more than 40 percent low-income women. When comparisons were made for intervention groups with more than 40 percent nonwhite women, the estimated effects were 12 percent (95-percent CI: 6.7-17.4; 24 studies) and 11.6 percent (95-percent CI: 6.4-16.7; 16 studies) if comparisons are limited to 40 percent or more African-American women. Again, significant heterogeneity between the studies was evident for each of these groupings.
As other Institute of Medicine reports (e.g., 2000, 2001) have recommended recently, the strongest interventions were those that increased access and addressed structural, economic, and geographic barriers to mammography use, along with intrapersonal and interpersonal factors (Skinner, Arfken, and Waterman, 2000; Skaer et al., 1996; Taylor et al., 1999; Rimer et al., 1992; Kiefe et al., 1994). That is, they combined communication interventions with others that were designed to enhance access. After all, mammography use does not occur in a vacuum. But individual-directed interventions in health care settings also showed impressive effects. Overall, the outcomes of combinations of certain kinds of interventions had the greatest impact on diverse women.
These results cannot be compared directly to studies conducted only among mainstream populations. However, the results can be compared to other mammography meta-analyses. Several meta-analyses of mammography-enhancing interventions previously have been reported. Although they all used different categories and inclusion/exclusion criteria, making direct comparisons impossible, the conclusions for general populations are consistent with, but not identical to, findings for diverse populations.
Wagner’s (1998) review focused on mammography reminders for general populations, and concluded that women who received reminders were more likely to be screened than those who did not
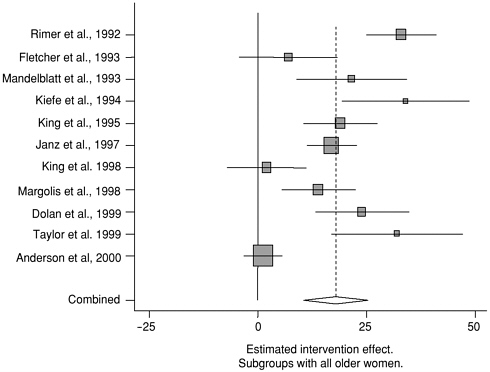
FIGURE 4-3 Individual and combined intervention effects for specific subgroups. Estimated intervention effects for individual studies and combined intervention effect estimates for studies with all older women and more than 40 percent with low incomes.
(OR = 1.48, p < .001 for n = 11 studies). Tailored reminders were more effective than generic ones, and effects of reminders were strongest in non-U.S. studies. Other reviews (e.g., Balas et al., 1997) have found that telephone calls to women increased mammography use.
Yabroff and Mandelblatt’s (1999) review employed a different categorization scheme. However, it had some important similarities to the analysis by Legler and colleagues (2002). Their access-enhancing category (effect size 18.9 percent, 95-percent CI: 10.4-27.4; 14 studies) was similar in content to Yabroff and Mandelblatt’s (1999) patient-targeted sociological interventions (effect size 12.6 percent; 95-percent CI: 7.4-17.9; 8 studies). Yabroff and Mandelblatt’s (1999) categories of behavioral (effect size 13.2 percent; 95-percent CI: 4.7-21.2; 5 studies) and cognitive
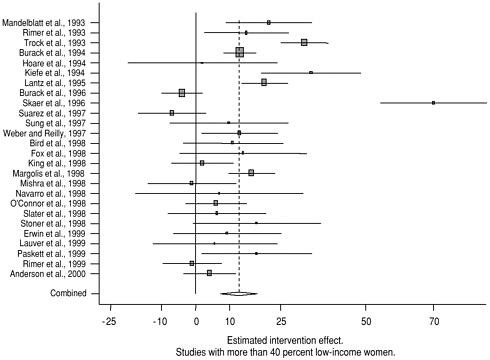
FIGURE 4-4 Individual and combined intervention effects for specific subgroups. Estimated intervention effects for individual studies and combined intervention effect estimates for studies with all older women and more than 40 percent with low incomes.
interventions (effect size 23.6 percent, 95-percent CI: 16.4-30.1; 2 studies) paralleled Legler’s individual-directed interventions (effect size 17.6 percent, 95-percent CI: 11.6-24.0; 15 studies). Legler and colleagues used different intervention categories and limited the focus to studies involving diverse populations, while Yabroff and Mandelblatt’s earlier analysis addressed general populations with fewer studies. Nevertheless, the results for diverse populations are similar to the findings for the general literature.
Yabroff and colleagues (2001) published an updated review that is particularly germane to the current volume. They examined the respective contributions of inreach and outreach interventions. What they found is noteworthy; the approaches had only modest differences. In every case, interactive strategies, delivered in person or by telephone, were much more effective than static inter-
ventions. Theory-based educational strategies delivered interactively increased mammography use by 10.7 percent in inreach settings and 19.9 percent in outreach settings. Communications of theory-based educational strategies combined with behavioral interventions had even greater impact—14 percent for inreach and 27.3 percent for outreach. Of special note for this volume, effects were similar across populations. The authors concluded that “the interventions should be similarly effective in minority or medically underserved populations” (p. 170). As Legler et al. (2002) and others have reported, sociologic interventions, such as lay health advisors, had a very modest impact, with effect sizes in the range of 10 percent. In a systematic review, using similar categories to those used by Legler et al., Sin and Legler (1999) concluded that “simple, brief, and effective interventions exist to boost breast cancer screening uptake. More complicated approaches are not necessarily any more effective” (p. 170). They went on to suggest that the most effective interventions are likely to be multistrategy, consistent with Legler et al.’s conclusions. They emphasized that such interventions should be suited to local needs.
In another meta-analysis, Bonfill et al. (2001) concluded that the most effective interventions were, in order of effect, mailed educational materials (2.81), letters of invitation plus phone calls (2.53), training and direct reminders to women (2.46), letters of invitation (1.92), and home visits (1.6). Their review included few, if any, of the studies Legler categorized as access enhancing. The strongest interventions fell into a category comparable to the individual-directed group. Similarly, Bonfill and colleagues concluded that combinations of effective interventions could have an important effect. The authors specifically recommended studies to explore the effect of interventions on diverse subgroups. Thus, previous reviews generally are consistent with Legler’s conclusions about the efficacy of individual-directed interventions, although effect sizes vary. Focusing on studies of diverse populations revealed the importance of access-enhancing approaches, along with individual-directed interventions in health care settings.
The results of the meta-analysis of mammography interventions for diverse populations show that the past decade’s investment in such interventions has translated into effective interventions for these groups. In general, the interventions for general populations are not so different from those that are effective with diverse populations, with the exception of the importance of access-enhancing interventions. This makes sense because access barriers may exert considerable negative impact for the women characterized here as diverse. But similarly, the interventions that have been effective in general, such as tailored and untailored letters and reminders and various forms of counseling, also are effective for diverse populations. Also encouraging is the fact that interventions aimed at diverse populations had strong effects. However, the results suggest that some interventions—such as social network and media interventions alone—that are widely used for diverse populations may not be sufficiently powerful to justify their use for these groups without additional interventions.
All interventions are not equal. In some cases, combinations of interventions will be needed. For example, mass media interventions can be used to increase awareness, while access-enhancing and individual-directed interventions can be used to overcome individual women’s barriers to getting mammograms. The forthcoming Guide to Community Preventive Services (http://www.thecommunityguide.org/) , led by the Centers for Disease Control and Prevention (CDC), will provide more detailed information on which interventions are most effective.
CONCLUSIONS
-
Further research is necessary to characterize the relationships between the race, ethnicity, and language of women and their health care providers in order to identify factors that contribute to differential patterns of communication and behavior change relevant to screening mammography. Examples of such factors might include social norms of the patient-provider relationship, training of practitioners, and communication norms around issues of breast
-
health and cancer screening. One frequently ignored aspect of the mammography experience is communication between women and radiologic technologists (Moyer et al., 2001). As noted by Moyer and colleagues, some racial and ethnic minority women (e.g., African-Americans) are less likely to understand the benefits of mammography, more likely to view cancer as fatal, and more likely to be more anxious about getting mammograms. Thus, communication and the opportunity to improve communication and increase the probability of subsequent adherence may be especially important for diverse populations.
-
The process of intervention development needs to take into account women’s life experiences and social contexts, which may not be reflected in their race/ethnicity, age, or other broad categorization.
-
Health behavior change is influenced at multiple levels, including at the individual, interpersonal, institutional, community, and policy levels. Health communications targeting individual or interpersonal factors alone are likely to be insufficient in the absence of environmental interventions, such as those that enhance coverage or increase access. Interventions to reduce access barriers to mammography are important if remaining disparities in screening use are to be reduced.
-
The mammography literature shows that, overall, women are more similar than different. However, although the predictors of mammography may be the same for diverse populations, their levels and intensity may vary. It is critical that interventions be built on a strong theoretical foundation using data accumulated from well-designed qualitative and quantitative studies to provide understanding of the variables that affect mammography for diverse populations. Health communications will be most effective when they are relevant, appropriate, and appealing to the specific audience targeted by the communication. Evaluations should include and report measures of fidelity and quality of intervention delivery.
RECOMMENDATIONS
-
Theory-based interventions need to be developed, tested, and disseminated to increase screening utilization among women who have never been screened and to facilitate regular screening among all women. Qualitative and quantitative research is needed to identify specific barriers and to develop interventions appropriate for this population. Research on mammography and related areas suggests that combinations of inreach and outreach strategies may be especially effective.
-
Authors should report sufficient detail about their interventions to enable readers to understand what was actually done. Where journal limitations preclude this, we encourage authors to put descriptive materials, including intervention descriptions, materials, and/or instruments, onto accessible Web sites.
-
We advocate the use of standardized, validated measures for breast cancer screening behaviors that will permit meaningful comparisons of outcomes across studies. This would include use of standardized mammography utilization questions from the National Health Interview Survey and the Behavioral Risk Factor Surveillance Survey.
-
Effective interventions should be widely disseminated. Practitioners are strongly encouraged to use previously validated, evidence-based interventions. The cancer screening chapter in the CDC-led Guide to Community Preventive Services should be a great advance in this regard (http://www.thecommunityguide.org).
-
Future research must be directed toward studies that are adequately powered to permit subgroup analyses of potential differential impact of intervention activities.



























