
Appendix A
Authored Papers
IMPLICATIONS OF RESTRICTIONS ON FOREIGN STUDENTS AND SCIENTISTS FOR INFECTIOUS DISEASE RESEARCH
Ronald M. Atlas, Ph.D.
Graduate Dean and Professor of Biology and Public Health Codirector, Center for Deterrence of Biowarfare and Bioterrorism
University of Louisville
Louisville, KY
It is clear that after September 11, 2001, we live in a new era, an era of fear—fear of foreigners who could be terrorists and fear of scientific information that could be misused by terrorists. The consequence is that we in the scientific and academic communities are now subject to new levels of public scrutiny that are manifest in the regulations governing visas for foreign students and visiting scientists and in the security clearance requirements for those with access to microorganisms and toxins (select agents) that are considered high-risk biothreats that might be used by terrorists. As graduate dean at the University of Louisville, dealing with foreign graduate students and visa issues being implemented under a post-9/11 regulatory framework, as a scientist involved in biodefense, and as a past president of the American Society for Microbiology (ASM), which has certainly been on the forefront of the debate on the select agent rules and the legislation that was passed after the anthrax attacks of Fall 2001 to reduce the threat of
bioterrorism, I have found myself balancing divergent norms of science and society and communicating across boundaries of national security, science, policy, and public concerns—trading the world of a laboratory scientist for a bully pulpit before journalists to reach the public, congressional hearing rooms to reach policy makers, and forums like this to reach fellow scientists.
We in the scientific community have an obligation to provide an educational forum that reaches far and wide, within the scientific community about the new legislation and regulations, and about how we need to comply to be good citizens of the world. Additionally, we need to educate the broader public as to the importance of international exchange in the scientific arena so as to ensure that regulations are constructed in ways that permit the advancement of biomedical research. We have a need to explain to the public and policy makers that the best defense against the threat of bioterrorism is to advance the research agenda against infectious diseases so that we have the vaccines, therapeutics, and diagnostics needed to combat emerging and reemerging infectious diseases as well as “plagues” that may be introduced by terrorists. We need to make clear that biomedical research is an international endeavor and that the battle against infectious diseases must be global. We also have an obligation to engage in a dialog with the national security community so that we understand the threats and vulnerabilities of our new world and can engage in activities—some of which will involve constraint and adherence to the new regulatory mandates—that will reduce the threat of the misuse of the life sciences by terrorists.
When the USA Patriot Act was first proposed, it would have banned all foreigners from entering a U.S. laboratory where a select agent was present. The ASM explained to the Congress that biomedical research is international in nature. We brought a clear message to the debate: infectious disease is a global health issue that requires international exchange and cooperation. Half of the manuscripts submitted to ASM journals come from outside the United States. If we curtail international collaborations, then we put the health of this and other nations at risk. If we cannot combat infectious diseases regardless of where they occur in the world, we put U.S. national security at risk as well. The Congress listened. When the Patriot Act was passed, such proposed global restrictions on foreigners were removed.
Having said that, we in the scientific community also made compromises concerning who could have access to select agents and the regulatory system overseeing possession of those agents. In my view, the compromises were critical for demonstrating that the scientific community was responsive to public concerns about bioterrorism and for achieving public support for biomedical research needed to advance biodefense capabilities.
I recognize that some people would accuse me of having entered into a Faustian deal for having agreed that we should restrict certain individuals
from having access to select agents within U.S. laboratories, namely, aliens from countries that the United States designates as supporting terrorism and those individuals who are not permitted to purchase handguns. When the ASM looked at the impact of restricting individuals from the few nations that are designated by the United States as supporting terrorism, and only restricting them in the laboratories where a limited number of select agents were present, we found that there were very few scientists and very few exchanges that were being affected in the United States. We agreed to accept that provision, which became a restriction in the Patriot Act and which was subsequently incorporated into the Biopreparedness Act, and thus, into the regulatory scheme of the Centers for Disease Control and Prevention and the U.S. Department of Agriculture oversight of select agents.
George Poste, who has been very outspoken about the hubris of the scientific community placing the United States in danger by not fully recognizing the potential for misuse of science, had made the claim that the Patriot Act and the implementation of the select agent rule are major impediments to industry that is multinational, and that the biotech industry would not fare well under the Patriot Act. The restriction imposed by the Patriot Act and subsequently incorporated into the Biopreparedness Act stated that individuals from nations that support terrorism may not have access to select agents in U.S. laboratories. Thus, it should have minimal impact on multinational corporations. It is true that implementation of the select agent rules involves a site-specific registration and clearance process. An individual cleared to work with certain agents in one laboratory who goes to work in another laboratory requires a new clearance. Additionally, the owners of each private laboratory in possession of select agents must be cleared. Potentially that can impact the ability to collaborate and to move personnel from laboratory to laboratory. We are still in the early phases of implementing the new select agent possession regulations and need to wait and watch carefully for real impacts. If we detect negative impacts, then we need to bring them to the attention of the relevant departments and agencies and insist that they be responsive. We also need to recognize that we have new responsibilities in the era of terrorism. Unfortunately, the days of a graduate student working alone in a laboratory with dangerous pathogens in the middle of the night are probably gone. But maybe this is for the good of all, as appropriate biosecurity measures should enhance biosafety.
Perhaps the greatest challenge for the scientific community will be developing a working relationship with the national security and law enforcement communities. The Biopreparedness Act requires that the Department of Justice clear individuals who have access to select agents. This responsibility has been given to the Federal Bureau of Investigation (FBI). This is a new system, and there is legitimate concern over how it will work. Can it provide appropriate security oversight without interfering with the
legitimate pursuit of science, especially as the magnitude of biodefense research increases exponentially? At this point, we do not have any data that suggest that the system is not going to work—but there is considerable concern.
Beyond the regulations and clearances imposed by the Biopreparedness Act, there is concern that some government laboratories, for example, Department of Defense laboratories, Department of Agriculture laboratories, and potentially other laboratories within the Department of Health and Human Services, will further restrict foreign nationals from entering those laboratories. The select agent regulations do not provide for such broad restrictions of international scientists. While there may be some areas where classified research is conducted and where restricted access for foreign nationals may be appropriate, it is important for the scientific and biomedical communities to highlight the value of international scientific exchanges for global health and national security.
Turning to the issue of visas for students and visiting scientists, the implementation of new regulations aimed at reducing the risk of terrorism is raising concerns in the academic and scientific communities. Resources are needed to ensure appropriate implementation of the new tracking and interview systems. Within the academic and scientific communities, we need to gather systemic data to document problems. The major educational organizations, including the American Association of Universities and the Council of Graduate Schools, requested that the requirement for interviews to obtain visas be implemented only if there were sufficient resources to prevent undue delays that would interrupt the flow of foreign students into the United States. The State Department promised to be responsive and quickly instructed the consular services to give preference to students for interviews so that educational exchanges are not inhibited.
The ASM asked the State Department to develop procedures and allocate resources necessary to assure prompt and appropriate action on visa requests for students and researchers seeking to study within the United States. The ASM pointed out that educational exchanges and training of students, researchers, and clinicians in microbiology and other scientific disciplines from countries around the world are critical for the advancement of biomedical science and public health. If we limit our ability to exchange scientific information and train scientists, then we will severely limit our ability to fight infectious diseases—and infectious diseases do not respect any political borders. The ASM therefore urged the State Department to eliminate the adverse impact of visa policies on the continued education and training of foreign students in the United States. Given that the ASM has supported appropriate measures to reduce the risk of terrorism, it did not urge laxness in processing visas. Rather, the ASM urged that screening processes be undertaken with a minimum of disruption of educational and
research endeavors, urging observance of the following principles in designing and implementing screening procedures:
-
Screening procedures must be developed, planned, and implemented in a manner and on a schedule that ensures that interviews or other processes do not interfere with legitimate scientific training.
-
The United States must devote the necessary resources to ensure that prudent procedures do not fail as a result of a lack of adequately trained personnel to implement the procedures in a timely manner.
-
Microbiology and other sciences must not be singled out as an area of concern or in a manner that admission of students for science education and training is impeded.
-
In light of inevitable limitations upon resources, procedures must be developed that expedite, on the basis of objective criteria, the processing of visas least likely to pose a threat so the overall system permits the timely admission of all qualified individuals legitimately interested in advancing their education or advisory role to U.S. governmental agencies.
-
The process for reentry of trainees who have been granted visas for training in the United States should be simplified, eliminating the requirement for reentry interviews for students who have been out of the United States only for a brief period.
In response, the State Department reiterated its commitment to protect international exchanges of students and researchers.
Thus, in many ways we are at a critical crossroads. We face a new regulatory environment—one crafted out of fear of terrorism. We face a critical need to advance biomedical science to combat the threat of bioterrorism as well as the emergence and reemergence of deadly infectious diseases. We must find the right balance between openness and security—between restrictions and free exchange impacting foreign students, visiting scientists, and international collaboration. This will require continuing dialogue among the scientific community, the national security community, policy makers, and the public. We must be ready to confront the challenges of infectious diseases in this new era of regulatory oversight of research and educational exchange.
TRAINING AND SUSTAINING THE PUBLIC HEALTH LABORATORY WORKFORCE—OUR FIRST LINE OF DEFENSE AGAINST INFECTIOUS DISEASE
Scott J. Becker, M.S.
Association of Public Health Laboratories
Washington, D.C.
Public health laboratories play a lead role in the detection and response to infectious disease. That role cannot be performed without a sound laboratory infrastructure—including highly trained staff and linkages with private-sector laboratorians—that must be in place well in advance of a crisis. However, an ongoing shortage of skilled laboratorians compromises the nation’s laboratory system and reduces our vigilance for infectious microbes. To remedy this situation and avert the consequences of more dire workforce deficiencies, public and private employers, trade groups, and relevant government agencies must find new ways to attract and retain the nation’s next generation of laboratory technicians and scientists.
Public Health Laboratories and Microbial Threats to Health
As vividly demonstrated by efforts to contain West Nile virus in 1999, anthrax in 2001, and severe acute respiratory syndrome (SARS) in winter 2003, public health laboratories play a crucial role in identifying and analyzing infectious organisms in support of public health disease investigations. Infectious disease testing is, in fact, one of the core functions of public health laboratories and encompasses a range of vital activities (CDC, 2002). These activities include:
-
Isolating and identifying causative agents—including emerging or reemerging pathogens—that are present in clinical specimens (e.g., blood, urine, saliva) or in unusual specimen matrices such as food and environmental samples.
-
Determining the source of infections by identifying human carriers and environmental sources of disease.
-
Providing specialized tests for low-incidence, high-risk diseases, such as tuberculosis (TB), rabies, botulism, and plague.
-
Confirming atypical laboratory test results and providing reference diagnostic testing to private-sector laboratories that may not have the ability to fully identify disease agents of public health significance.
In addition to hands-on testing to characterize infectious agents, public health laboratories perform a number of services to support and improve
testing programs and to manage laboratory data for effective disease surveillance (CDC, 2002). These services include:
-
Conducting research to develop and validate diagnostic tests for emerging infectious diseases and to improve existing infectious disease tests (for example, by developing rapid test methods).
-
Providing advice to private-sector laboratories regarding newly marketed tests.
-
Developing and overseeing quality assurance programs for private clinical laboratories through training, consultation, certification, and proficiency testing to assure the reliability of laboratory data used for communicable disease control.
-
Ensuring the ability to accumulate, synthesize, and communicate test results and other laboratory information essential for public health analysis and decision-making.
-
Providing a statewide disease reporting network.
-
Participating in national database systems for surveillance of diseases of national and global concern.
State public health laboratories are the critical link between the nation’s many private-sector clinical laboratories—which, by virtue of their primary diagnostic function, are often the first to report unusual laboratory results—and the public health establishment. They maintain strong ties with national laboratories at the Centers for Disease Control and Prevention (CDC) and other federal agencies, and with state health officers, state epidemiologists, and directors of state programs in sexually transmitted disease, tuberculosis control, maternal and child health, and environmental health.
It is easy to recognize that infectious disease outbreak investigations and disease prevention and control efforts depend on sound and timely laboratory data. It is similarly clear that all of these activities will be adversely affected by deficiencies in either public health laboratory capabilities (specific services performed) or capacity (volume of services that can be performed within a defined time period). Workforce limitations affect both.
Public Health Laboratory Workforce Shortage
The current shortage of skilled public health laboratorians is not a sudden phenomenon. Rather, it has been ongoing for some years. Public health laboratories, like other parts of the public health system, have suffered chronic underfunding. An October 2000 report concludes that long-term reductions in public health laboratory staffing and training have impaired the ability of state and local authorities to identify biological agents
(Smithson and Levy, 2000). More recently, a 2002 Institute of Medicine (IOM) report refers to the nation’s “antiquated laboratory capacity” that leaves Americans vulnerable to exotic infectious organisms as well as more mundane microbes (Committee on Assuring the Health of the Public in the 21st Century, 2003).
Unpublished data from a “straw poll” conducted in spring 2003 by the Association of Public Health Laboratories (APHL) show an average vacancy rate for state laboratory testing personnel of 8.6 percent. These data are comparable to data from the American Society of Clinical Pathologists’ (ASCP) 2002 wage and vacancy survey, which found that the average vacancy rate for staff-level medical technologists ranged from 6 to 10.2 percent, depending on geographic region (Ward-Cook et al., 2003). But some states greatly exceed the average. Tennessee is one. The state public health laboratory has been struggling since late 2001 to fill fully a third of its clinical microbiology positions (personal communication, J. Gibson, Director of Microbiology Laboratory, Laboratory Services, Tennessee Department of Health, August 11, 2003).
However, although these figures represent significant understaffing, they may be deceptively low. The number of staff positions authorized by states generally does not keep pace with the laboratory workload. That is, any vacancies likely represent a true reduction in laboratory capacity. In Kentucky, for example, the state laboratory is recruiting for two positions in 2003, including the laboratory director’s post, which had been vacant since December 2002. However, the state completely eliminated ten laboratory positions due to budget constraints, and these positions do not get counted as vacancies (Isaacs, 2003). There also is evidence that public health laboratories and other employers have increased the use of temporary staff and broadened the selection criteria for permanent positions, thereby filling vacancies with less qualified individuals (a medical laboratory technician in place of a medical technologist, for example) (ASCP, 2003).
The lack of adequate laboratory capacity was driven home during the bioterrorism incident that occurred in fall 2001, when many public health laboratories required overtime hours and halted much routine work because key personnel were diverted to testing for B. anthracis or to related support activities, such as sample log-in and screening. The Connecticut state lab brought in a team of volunteer microbiologists and the New York City lab arranged to borrow staff from the city’s private clinical labs to augment beleaguered public health laboratory workers (APHL, 2002; APHL, 2003a). Even the relatively mild SARS outbreak in the United States in winter 2003 strained laboratory capacity (APHL, 2003b). If two moderate infectious disease outbreaks were to coincide, the nation’s public health laboratories would be overwhelmed.
Where Have All the Lab Workers Gone?
The growing shortage of laboratory workers stems from three root causes: the ongoing retirement of a significant cohort of senior staff, including laboratory leaders; government hiring practices; and a shrinking pool of future laboratory professionals that impacts both the public and private infectious disease workforce. In many cases, public health laboratories are losing their most skilled personnel before they have a chance to recruit and train replacements. One northeastern state saw 20 percent of its laboratory staff—19 individuals—retire in June 2003. Ohio’s state laboratory director writes in Focus magazine, “What laboratory can replace the knowledge (and value) that a senior technologist with 29 years experience immersed in molds and fungi brings with them to work every day? How about trying to replace your senior chemists, bacteriologists, virologists, or immunologists?” (Becker, 2003).
Of particular concern, an APHL study anticipates an average of 13 vacancies in state public health laboratory director positions by 2006, with a candidate pool that more than two-thirds of current directors describe as either “not adequate” or “only marginally adequate” in size to meet future needs (Schoenfeld et al., 2002). In addition to scientific and technical expertise, public health laboratory directors must have management, public policy, and communication skills, making this position especially difficult to fill, but also especially important, since it is the directors who provide leadership in times of crisis and who advocate for the needs of the laboratories.
From one vantage point, the public health laboratory workforce shortage can be seen as part of an overall shortage of state government employees—one that is likely to get worse. According to a 2002 report by the Council of State Governments (CSG) and the National Association of State Personnel Executives (NASPE), both the pending retirement of current state employees (whose average age is 44.5 years) and mandatory state hiring freezes or other hiring limitations (in effect in 27 states) contribute to the declining number of state workers (Carroll and Moss, 2002). On average, the current vacancy rate of state government positions is just over 11 percent, but more than half of states report vacancy rates above the national average, including Alaska at 21.6 percent. The CSG/NASPE report predicts that state governments could lose more than 30 percent of their workforce by 2006 due to the twin problems of an aging workforce and continuing state budget shortfalls (Carroll and Moss, 2002).
From a second vantage point, the public health laboratory workforce shortage can be seen as part of a serious labor problem plaguing public health and private clinical laboratories throughout the nation. The U.S. Bureau of Labor Statistics projects that 122,000 new medical technologists and medical laboratory technicians will be needed between 2000 and
2010—or roughly 12,200 new clinical laboratorians each year—to replace retiring workers and meet the rising demand for laboratory tests (Hecker, 2001). Yet in recent years, on average fewer than 5,000 individuals have graduated from accredited training programs annually (U.S. Department of Labor, 2002; Painter, 2000). In 1999, the ASCP certified fewer medical technologists than it did in 1959 (2,216 and 2,349, respectively) (Painter, 2000).
A drop in the number of students interested in laboratory science has led to the closure of hundreds of training programs approved by the National Accrediting Agency for Clinical Laboratory Sciences (NAACLS), a fact that does not bode well for the future. There were about 1,000 NAACLS-approved programs in 1970, compared to about 500 today (Painter, 2000; NAACLS, 2003). California, the most populous state, had only eight clinical laboratory science programs in the 2003–2004 academic year, with a combined class capacity of just 89 students (AMA, 2003). And not all programs are necessarily filled to capacity. Lack of knowledge about professional laboratory careers (a byproduct of low recognition for current workers) and higher-paying job options in the science and allied health fields are the chief reasons cited for declining enrollments (Beckering and Brunner, 2003; CHP 2001).
In fact, public health laboratories are suffering from the combined effects of government workforce problems and adverse trends within the field of laboratory science.
Recruitment Issues
Recruiting laboratory scientists for any position is difficult in the current job market since qualified workers are scarce. But there are additional challenges. The field of laboratory science is evolving much more rapidly than ever before, and new entrants to the field must be prepared to constantly update their skills. Yet, despite the degree of technical expertise required, laboratorians receive little recognition for work that is largely unseen by the public. Moreover, many laboratory positions are in rural areas and inner cities—locations that tend to be less desirable. Potential public health laboratory recruits also face government hiring constraints, limited career mobility, and generally lower salaries and greater on-the-job learning curves than in the private sector.
The 2001 terror attacks and recent SARS outbreak afforded laboratorians some measure of public appreciation for their work, but also raised fears of extraordinary biosafety risks for all infectious disease laboratorians. In addition, the terror attacks spawned new federal legislation that complicates the hiring process for some laboratories, including all state public health laboratories and many university-based research facilities.
Challenges to recruitment include:
Rapidly Changing Technology
Ten years ago, infectious disease laboratorians were expected to be proficient in classic methodologies to identify infectious organisms: microscopy, culture techniques, and serology. Those methods are still used. But today they exist alongside an ever-changing and increasingly complex set of newer methods that staff members in more advanced laboratories must know or be prepared to learn quickly: commercial nucleic acid amplification tests (used for tuberculosis and sexually transmitted diseases), conventional polymerase chain reaction (PCR), real-time PCR (used for emerging infectious diseases and agents of bioterrorism), pulse field gel electrophoresis (a molecular “fingerprinting” technique used for outbreak investigations), and the latest methods—spoligotyping and variable number tandem repeat analysis. In addition to mastering these techniques, laboratorians must also possess above-average computer software skills to track specimens, analyze data, and communicate test results to relevant parties (e.g., specimen submitters, state health officials, national disease databases).
Unique Public Health Skill Sets
In order to work in a public health setting, a laboratory scientist must have an added skill set above and beyond the technical expertise described above. The average university-trained molecular microbiologist, for example, lacks a working knowledge of infectious disease outbreak management, quality control practices, the principles of population-based disease surveillance, Biosafety Level 3 work practices, and the role of the state epidemiologist and other state and national health officials with whom the laboratory must interface on a regular basis.
Ultimately, to work well within a public health laboratory, technical staff must understand the public health relevance of clinical testing. Whereas a private-sector laboratorian will test a sputum sample to determine whether a specific patient is positive for tuberculosis, public health laboratorians will sometimes process the same sample, but to other ends. The public health scientist wants to identify the exact strain of TB infecting the patient and to compare it to TB isolates from other individuals. Is the same strain responsible for multiple TB cases within the state? Do current cases represent the leading edge of a larger infectious disease outbreak? The public health laboratorian may also conduct susceptibility testing to gauge the pathogen’s resistance to a host of antimicrobial agents and work with epidemiologists to forward this information to infection control practitioners and clinical laboratories throughout the state.
New public health laboratory recruits must be willing to learn public health principles and to acquire the additional technical and communication skills needed to make them effective partners within the larger health system.
Government Employment Practices
By definition, public health laboratories are embedded within government agencies and are therefore subject to the vagaries of government employment practices, which are shaped by fiscal and political considerations, as well as plain bureaucratic inertia. In many states, even after a new position has been authorized and fully funded, it can take up to a year to process paperwork, advertise the post, interview applicants, and finally fill the vacancy. In the meantime, existing staff must cope with any extra workload. Once the new recruit is on the job, his or her position may not be secure. Some state public health laboratory personnel work under collective bargaining agreements forged by unions, and, when layoffs occur they affect those employees with least tenure. Moreover, positions that are funded through federal grants or fee-for-service programs are only as secure as the revenue stream. Finally, junior laboratory personnel have limited opportunities for advancement, since there tends to be low turnover among senior public health laboratorians. When senior positions do become vacant, they typically must be filled through a competitive hiring process that may or may not favor in-house applicants.
Legal Hurdles
Even before prospective employees can be considered for laboratory work, a slew of government laws and regulations narrow the applicant pool. The Clinical Laboratory Improvement Amendment (enacted by the federal government in 1967 and updated several times since) requires directors of all laboratories that test human specimens to hold either an M.D. or Ph.D. with board certification, thus excluding otherwise qualified candidates, including individuals who have been mentored under current directors but lack an appropriate advanced degree.
The USA Patriot Act, which became law after the 2001 terror attacks, raises a number of legal hurdles for employees in all laboratories that work with so-called select agents—high-consequence organisms such as anthrax, ebola, and Yersinia pestis. In practice, most of the diagnostic laboratories affected by the legislation are public health laboratories. These facilities are barred from hiring nationals of countries of concern, as designated by the Act. In addition, they must screen all current and prospective workers, who, as a condition of employment, are required to sign a Federal Bureau
of Investigation information release form and undergo background checks and fingerprinting that some employees have found intrusive.
Finally, some states have their own licensure requirements for public-and private-sector laboratorians.
Where Do We Go from Here?
The preface to the IOM’s recent report on microbial threats to health states, “We must trumpet the message of urgency and concern, but our more demanding task is … to consider what further investments of fiscal and political capital are needed if we are to keep pace with our microbial competitors” (IOM, 2003). Certainly, one area in need of further investment is the nation’s infectious disease workforce, and, in particular, the clinical laboratory scientists who come face-to-face with the microbes themselves.
If a severe shortage of laboratory scientists is to be averted, steps must be taken to increase awareness of laboratory careers and to make those careers more attractive: better wages, improved opportunities for training and advancement for practicing laboratorians, measures to address biosafety risks, relocation assistance, and—importantly—increased recognition for laboratory technicians and scientists. Indeed, the scarcity of qualified laboratorians has already begun to place an upward pressure on salaries, which are rising just ahead of inflation (at least in the private sector) (Ward-Cook et al., 2003).
But while hospitals and other private clinical labs are able to institute sign-on bonuses and offer flexible schedules and other work incentives, public health laboratories are generally constrained by government employment rules, forcing them to consider innovative solutions. In the wake of the anthrax scare, the Alaska state laboratory pressed for a separate job classification for public health microbiologists to permit greater salary increases. The New Hampshire state laboratory attempted to use an international employment agency to expand its search for traditionally trained microbiologists, but found that none exists. (In any case, the Patriot Act now restricts the hiring of foreign-born nationals.)
Other state laboratories have offered laboratory rotations to medical students and those pursuing degrees in relevant sciences and enlisted senior laboratorians as adjunct faculty to local universities in an effort to improve awareness of laboratory careers. Efforts to incorporate laboratory courses in public health curricula and public health courses in curricula for medical technologists are also under way.
The Tennessee public health laboratory, in an attempt to fill longstanding vacancies, has established two programs to help potential employees obtain the national certification and state licensure required to work in state laboratories. The first is an affiliation with a local university. Students
spend 6 months in traditional on-campus courses, followed by a 6-month paid internship at the Tennessee state laboratory. The second program, geared for students who have already fulfilled academic requirements, is a 1-year paid internship comprising clinical laboratory lectures and practice rotations at the state laboratory.
The APHL Emerging Infectious Disease (EID) Fellowship program was begun in the mid-1990s to introduce recent college graduates at the bachelor’s, master’s, and doctoral levels to the practice of public health laboratory science. To date, more than 200 fellows have been placed in local, state, and federal public health laboratories throughout the United States and abroad. Domestic and international EID fellows have participated in nearly 40 outbreak investigations and contributed to over 200 publications in peer-reviewed journals. Following their training, many fellows accept positions in public health laboratories or continue their education and pursue careers in other health-related fields. Applications for the 2004 class of fellows were up 40 percent over the previous year, possibly reflecting an increased awareness in the lay population about infectious disease threats.
The APHL is also working to expand continuing education opportunities for current public health laboratorians through its National Laboratory Training Network (NLTN) and newly established National Center for Public Health Laboratory Leadership (NCPHLL). The NLTN (www.nltn.org) is a collaborative program between the APHL and the CDC. Since its inception in 1989, it has delivered more than 3,200 wet workshops and training activities reaching over 100,000 laboratorians. This type of targeted training—including courses in rabies, bioterrorism, tuberculosis, virology, investigation of food-borne outbreaks, molecular laboratory methods, and more—is not available from any other source.
The NCPHLL was established to address the growing leadership vacuum in public health laboratories. Other than through the center’s activities and on-the-job experience, current laboratorians have almost no mechanism to acquire the managerial, public policy, communications, and other leadership skills essential to oversee the complex workings of a public health laboratory. The center is identifying and disseminating the knowledge needed for effective decision-making in public health laboratories and also providing technical assistance—such as workshops in grant writing, media relations, and the regulatory inspection process—to support current laboratory leaders.
All of these efforts are helpful in building the strong national laboratory system that must undergird any serious effort to curb microbial threats to health. Yet more must be done. The Medical Laboratory Personnel Shortage Act of 2001 (HR 1948) is in legislative limbo. If enacted, this bill would expand the National Health Service Corps scholarship and loan repayment program to medical technologists and increase funding for the
Allied Health Project Grants Program, which helps attract laboratory professionals to the field (especially in rural and underserved communities).
The IOM has recommended that the CDC, the Department of Defense, and the National Institutes of Health develop new programs and expand current programs to train the infectious disease workforce, incorporating hands-on experience at public health agencies whenever possible (IOM, 2003). Stints in public health laboratories should be a prominent part of these programs.
Of pressing concern, more must be done to interest younger students—at the middle school and high school levels—in laboratory science. The Coordinating Council on the Clinical Laboratory Workforce and the American Society for Clinical Laboratory Sciences are developing a recruitment “tool kit” to suggest ways that high school science teachers and counselors can attract students to laboratory science careers. This project is a promising start.
A lot is riding on our collective efforts to assure a robust network of private and public health laboratories. Without qualified personnel to process routine diagnostic tests, to support national disease surveillance, and to identify the next novel microbe, the health of Americans will surely suffer.
References
AMA (American Medical Association). 2003. Health Professions: Career and Education Directory, 30th Edition, 2002-2003. Chicago, IL: AMA Press.
APHL (Association of Public Health Laboratories). 2002, September–October. Connecticut public health laboratory recognized for anthrax testing; preparing for future biological, chemical terror threats. The APHL Minute, pp. 4, 17–18.
APHL. 2003a, July–August. Annual meeting explores labs’ readiness for public health emergencies. The APHL Minute, pp. 12, 14.
APHL. 2003b, July–August. State public health laboratories put to the test with SARS. The APHL Minute, pp. 1, 4–5.
ASCP (American Society for Clinical Pathology). 2003, July 24. Press release. ASCP Releases New Wage and Vacancy Report on Clinical Laboratory Workforce. Chicago, IL: ASCP.
Becker W. 2003. Public health laboratories—The forgotten opportunity? Focus, p. 4.
Beckering R and Brunner R. 2003, June. The lab shortage crisis: A practical approach. Medical Laboratory Ob Server, pp. 49–50.
Carroll JB and Moss DA. 2002. State Employee Worker Shortage. The Impending Crisis. Lexington, KY: Council of State Governments and National Association of State Personnel Executives.
CDC (Centers for Disease Control and Prevention). 2002. Core functions and capabilities of state public health laboratories: A report of the Association of Public Health Laboratories. MMWR 51(No. RR-14):1–8.
CHP (Center for Health Professions). 2001. Clinical Laboratory Scientists and Medical Laboratory Technicians: Options for Addressing California’s Crisis. Allied and Auxiliary Health Care Workforce, Center for the Health Professions, University of California, San Francisco. Unpublished.
Committee on Assuring the Health of the Public in the 21st Century. 2003. The Future of the Public’s Health in the 21st Century. Washington, DC: The National Academies Press.
Hecker DE. 2001. Occupational employment projections to 2010. Monthly Labor Review 124(11):57–84.
Isaacs B. 2003, July 23. State health lab on fast track in identifying bioterror germs. Lexington Herald-Leader, p. A1.
IOM (Institute of Medicine). 2003. Committee on Emerging Microbial Threats to Health in the 21st Century. Microbial Threats to Health: Emergence, Detection, and Response. Washington, DC: The National Academies Press.
NAACLS (National Accrediting Agency for Clinical Laboratory Sciences). 2003. Search of All Certified and Approved Programs on NAACLS Web Site. [Online]. Available: www.naacls.org [accessed August 28, 2003].
Painter PC. 2000. What Has Happened to All the Techs? [Online]. Available: www.ivdtrials.com/TechStaff.htm [accessed August 14, 2003].
Schoenfeld E, Banfield-Capers SY, and Mays G. 2002. Who Will Run America’s Public Health Labs? Educating Future Laboratory Directors. Washington, DC: Association of Public Health Laboratories.
Smithson A and Levy L. 2000. Ataxia: The Chemical and Biological Terrorism Threat and the U.S. Response. Washington, DC: The Henry L. Stimson Center.
U.S. Department of Labor, Bureau of Labor Statistics. 2002. Occupational Projections and Training Data, Bulletin 2542. Washington, DC: U.S. Government Printing Office.
Ward-Cook K, Chapman S, and Tannar S. 2003. 2002 wage and vacancy survey of medical laboratories. I. Salaries continue to show moderate gains. Laboratory Medicine 34(9):631–638.
WHO WILL LIVE IN THE “HOUSE OF GENOMICS”?
Tara Acharya,a Halla Thorsteinsdóttir,a,b Peter A. Singer,a,c,d and Abdallah S. Daar* a,b,c,e,f
INTRODUCTION
Francis Collins’ vision of the future of genomics research is likened to a house founded on the Human Genome Project with three levels of research projects: genomics to biology, genomics to health, and genomics to society (Collins et al., 2003). But who will occupy this house, and which societies stand to gain from the genomics revolution? Will the beneficiaries be only the privileged in the developed world? Of the 15 challenges framed by Collins et al., only one relates explicitly to the health of 5 billion people in developing countries. In this future, exciting though it is, it is difficult to imagine the benefits of the Human Genome Project reaching the people in developing countries who need them the most. Here we show that, contrary to common perception, genomics and related biotechnologies are relevant to and should be harnessed for purposes of global development and health, and we point to strategies to help make this happen. This is particularly relevant for the “infectious diseases workforce of the twenty-first century,” the subject of this symposium, for we must understand the context in which that workforce will be functioning and the technologies that will be utilized to address the diseases. Only then can we plan for the education and training needs of that workforce.
Science and Technology Must Be Harnessed for Developing Countries
In the face of growing global health disparities, the potential of science and technology to improve global health cannot be ignored. To improve the health of millions of people in developing countries, we need to reap the benefits from our vast expansion in scientific knowledge and from the multitude of technologies we have developed. This is a plea policy makers,
advocacy groups, scholars, and other concerned people have recited for many years but sadly still needs to be repeated. Most health resources and 90 percent of all medical research are targeted at problems affecting only 10 percent of the world’s population (Global Forum for Health Research, 2002). United Nations Secretary-General Kofi Annan stresses that the benefits of sciences should be for humankind as a whole: “This unbalanced distribution of scientific activity generates serious problems not only for the scientific community in the developing countries, but for development itself. It accelerates the disparity between advanced and developing countries, creating social and economic difficulties at both national and international levels” (Annan, 2003).
With new advances in genomics technology,1 there is now tremendous potential to address health and development issues in developing countries. The World Health Organization (WHO) declared genomics to be a promising tool to improve global health, even though it warned that changing medical practices based on new technologies takes time and are not likely to happen overnight. The then Director-General of the World Health Organization, Dr. Gro Harlem Brundtland, stated in this report that it is: “clear that the science of genomics holds tremendous potential for improving health globally…. The specific challenge is how we can harness this knowledge and have it contribute to health equity, especially among developing nations” (Advisory Committee on Health Research, 2002).
The central premise for health equity is global solidarity (Benatar et al., 2003). Global solidarity can achieve health equity through (1) respect for the dignity of human life; (2) addressing the relationship between human rights, responsibilities, and needs; (3) ensuring freedom of choice; (4) democratic principles of accountability, representation, cooperation, and good governance; (5) and recognizing the importance of the environment and sustainability for the future. These concepts are intertwined with the promotion of enlightened self-interest. For instance, promoting global health equity is in the interest of the developed world: healthy developing world populations not only represent expanded market opportunities for products from industrialized countries, but the control of infectious diseases is becoming a major security issue for countries like the United States. As Martin Luther King said, “It really boils down to this: that all life is interrelated. We are caught in an inescapable network of mutuality, tied into a single garment of destiny. Whatever affects one directly, affects all indirectly” (King, 1968).
Genomics Has the Potential to Improve Health in Developing Countries
That genomics will revolutionize biological research is undeniable (Collins et al., 2003, p. 837). With regard to the impact of genomics on health, however, there is still a misconception in the global health community that genomics and related biotechnologies are not relevant to developing countries. We argue here that genomics has tremendous potential to alleviate health problems the world over, not just in developed countries. Take for example the case of malaria. Genomics and bioinformatics, in the hands of innovative researchers, resurrected the little-used drug fosmidomycin off the shelf and brought it into clinical trials as a novel anti-malarial drug in less than 2 years (Jomaa et al., 1999). The team successfully searched the Plasmodium falciparum genome for the gene of an enzyme targeted by fosmidomycin, an antibiotic developed and manufactured by a Japanese pharmaceutical company. In vitro studies have indicated that fosmidomycin inhibits the growth of multi-resistant strains of P. falciparum. When administered to adults in Gabon with malaria, fosmidomycin was found to be a safe and effective method of treatment (Missinou et al., 2002). Using a drug that has already been developed reduces the cost of the treatment, thereby making it a realistic opportunity for developing countries.
Genomics and related health biotechnologies do have the potential to improve health of people in developing countries, but considering that resources in developing countries are limited there is an urgent need to prioritize the most promising technologies. In order to identify these technologies, the University of Toronto Joint Centre for Bioethics carried out a technology foresight exercise where an international group of eminent scientists with expertise in global health issues were asked to identify and prioritize the top 10 biotechnologies for improving health in developing countries within the next 5 to 10 years (Daar et al., 2002). The results are presented in Table A-1 and highlight the relevance of genomics and related biotechnologies to health needs in developing countries.
The top 10 list includes technologies and technology platforms to address a range of developing world problems including infectious diseases, non-communicable diseases, malnutrition, and environmental contamination. These include:
-
Simple hand-held devices using molecular-based diagnostics to conduct rapid, low-cost testing for a variety of infectious diseases, such as HIV and malaria. Researchers have made breakthroughs already with these technologies in Latin America in the diagnosis of leishmaniasis and dengue fever (Balmaseda et al., 1999; Harris et al., 1998);
-
Genetically-engineered vaccines that are cheaper, safer, and more effective than current vaccines, and which hold new promise in fighting
TABLE A-1 Top 10 biotechnologies to improve health in developing countries
|
1. |
Molecular diagnostics |
|
2. |
Recombinant vaccines |
|
3. |
Vaccine delivery systems |
|
4. |
Bioremediation |
|
5. |
Sequencing pathogen genomes |
|
6. |
Female-controlled protection against sexually transmitted infections (STI) |
|
7. |
Bioinformatics |
|
8. |
Nutritionally-enhanced genetically modified (GM) crops |
|
9. |
Recombinant therapeutic proteins |
|
10. |
Combinatorial chemistry |
-
HIV/AIDS, malaria, and tuberculosis. For example: using DNA technology to design an AIDS vaccine candidate specifically for Africa; or plant-made vaccines incorporated into potatoes and other vegetables and fruits to protect against hepatitis B, cholera, measles, and other ailments
-
Alternatives to needle injections (e.g., inhalable drugs, powdered vaccines) that could make vaccine and drug delivery safer, easier to administer, and potentially less expensive
-
Genetically modified bacteria and plants that can clean up contaminated air, water and soil
-
Vaccines and vaginal microbicides that empower women to protect themselves from sexually transmitted infections and achieve contraception without needing consent from male partners
-
Computer-based tools to mine data on human and nonhuman gene sequences for clues on preventing and treating infectious and non-communicable diseases
-
Genetically modified staple foods such as rice, potatoes, corn, and cassava with enhanced nutritional value
Even though we highlight the potential of biotechnologies for improving health in developing countries we are not dismissing the value of conventional ways to improve health in developing countries—such as water sanitation, or access to mosquito bed-nets. We suggest instead that there should be an appropriate balance between the use of new technology and more conventional public health strategies. There is a common perception in the global health community that the health needs of developing countries are best addressed by existing public health interventions at the exclusion of new technologies, but clearly this is a false dichotomy. For example, vaccines are biotechnology products that over the years have become indispensable public health tools. Malaria control needs better water drainage
systems, widespread public acceptance, and use of bed-nets, but also new effective drugs and vaccines and “smart” insecticides based on molecular recognition.
Genomics Has Definite Global Public Goods Characteristics
Clearly, genomics and other health biotechnologies encompass important scientific knowledge that is relevant not just for the health of the developed world but also for developing countries. However, due to the enormous inequities in global health and global health research discussed above, knowledge—including genomics knowledge—is not optimally developed or utilized for improving the health of people in developing countries. In a closely interconnected world, localized sub-optimal utilization of scientific knowledge to alleviate misery and protect against diseases such as HIV/AIDS can have global repercussions. The global public goods characteristics of genomics provide justification for collective action to harness genomics for public health.
“Goods” can be defined along a spectrum from pure “private” goods to pure “public” goods. An apple is a private good since its consumption can be withheld until a price is paid (i.e., it is excludable), and once eaten by someone, it cannot then be eaten by someone else (i.e., it is rivalrous in consumption). In contrast, the benefits of public goods are enjoyed by all (non-excludable), and consumption by one individual does not deplete the good and does not restrict its consumption by others (non-rivalrous) (Sandler, 1997). For example, the Internet is typically open to all (i.e., is non-excludable), and downloading information from the Internet does not deplete the information (i.e., it is non-rivalrous). Global public goods possess properties of “publicness” across national boundaries (Kaul et al., 1999). Many goods are not easily classified, often falling somewhere along the spectrum between public and private categories (Woodward and Smith, 2003).
Genomics has significant global public goods characteristics that are expressed in diverse ways (Thorsteinsdóttir et al., 2003). For example, genomics is based on a worldwide resource, the human genome, that has a strong public nature. In a symbolic sense, the human genome has been declared to be a common global heritage of humanity (UNESCO, 1997). The very input to genomics is thus the non-excludable, non-rivalrous, genome. Genomics knowledge, like other types of knowledge, can also be considered the archetypal public good (Stiglitz, 1999). Genomics knowledge, especially sequence data, is typically open to anyone able to acquire it (non-excludable) and in general, made public via genomics databases on the Internet and journal publication. Because knowledge is non-rivalrous in consumption (i.e., it is not depleted by use) it is possible for many individuals to use the same knowledge for various purposes.
Although genomics knowledge has global public goods characteristics, the application of genomics knowledge may be open to exclusion or rivalry. At the individual level therapeutics based on genomics are, for example, private goods as they are both rivalrous and excludable when consumed by an individual. For example, more than one individual cannot consume a tuberculosis drug, and a diagnostic test is usually good for only one use. Nonetheless, the externality effects of rapid diagnosis and accurate treatment (i.e., controlling the spread of infection) point to potential benefits for an entire community, much like herd immunity conferred by vaccination programs.
But genomics as a global public good is not only born; it is also made. In other words, genomics has certain innate characteristics reviewed above that make it a global public good, but the social and political organization of initial genomics research has enhanced its global public goods characteristics. The way the Human Genome Project was funded and undertaken, and the emphasis on placing the resulting knowledge in the public domain where it can be freely shared are factors that strengthen the global public goods characteristics of genomics. If the field had developed without extensive international collaboration and without the strong emphasis on disseminating the resulting knowledge so rapidly in the public domain, then that would have diminished the global public goods characteristics of genomics. Ensuring that this knowledge remains accessible to people from all countries will help leverage it for development needs rather than restrict it and its potential benefits for the developed world.
Developing Countries Need to Build Local Capacity to Be Active Participants in Genomics
Although knowledge is theoretically free to be disseminated, in practice constraints are often put on its use. In order to absorb and make use of scientific knowledge, considerable investment is required (Pavitt, 2001). For example, education and training, physical access to journals or the Internet, research infrastructure, and the ability to establish the necessary production processes to turn genomic knowledge into a useful product are necessary access goods for genomics, and all challenge the ability to make practical use of genomics knowledge. Genomics is, in this sense, only a “public” good to those countries that have the capacity to exploit genomics knowledge and to conduct genomics research, which regrettably leaves out most developing countries. The challenge of taking genomics to society goes far beyond issues of privacy, medical insurance, and employment, which often are emphasized in developed countries and are singled out by Collins et al. in their paper (Collins et al., 2003). While it is important to regulate the potential misuse of genomics, it is at least as important to
ensure that the benefits of genomics reach all societies. In order for this to happen, there is a need to optimize the global public goods characteristics of genomics worldwide, with a special focus on developing countries that are currently lagging behind.
Some developing countries have started to build up their own capacity in genomics and other health biotechnologies. They include countries such as China, Cuba, India, and South Africa. They have followed different approaches where, for example, South Africa places emphasis on utilizing its biodiversity and traditional knowledge resources, but Cuba’s niche has been to develop vaccines to meet the health needs of its population, a demand that is accentuated by the United States trade embargo with Cuba. Genomics development requires a complex system of innovation, where diverse actors and policies are required for encouraging the production of innovative knowledge. A recent research project at the University of Toronto Joint Centre for Bioethics examining the factors and conditions that have encouraged capacity building and health innovation in developing countries may help to identify best practices that can be used by other developing countries in the fields of genomics and related biotechnologies (Thorsteinsdóttir et al., 2004). Building such capacity in developing countries not only encourages these countries to produce appropriate health products for their populations but can also generate extra income opportunities, which ultimately can improve the economic conditions in these countries.
International Collective Action Is Needed to Strengthen Genomics in Developing Countries
International collective action is also needed to mobilize genomics for global health and help bring genomics to society. Such action can drive efforts to improve research infrastructure, education, and training to provide developing countries with the “access goods” they need. Effective north–south and south–south partnerships are an important strategy to promote capacity-building. As Pang has suggested, “At the beginning of the new millennium, it is apparent that developing countries should participate in managing their own futures and thus be invited to work together in equal partnership toward a healthier world” (Pang, 2003). Political and financial commitment on the part of governments of both industrialized and developing countries is needed, as highlighted in the report from the Commission on Macroeconomics and Health (Commission on Macroeconomics and Health, 2001). Public–private partnerships such as the Malaria Vaccine Initiative, Global Aids Vaccine Initiative, Médicins Sans Frontières’ Drugs for Neglected Diseases Initiative, and most recently, the Bill & Melinda Gates Foundation’s Grand Challenges in Global Health initiative are very
important efforts that seek to leverage scientific discovery and international research efforts for developing country needs.
To spur the use of genomics as a global public good, we further propose a Global Genomics Initiative (Dowdeswell et al., 2003; Acharya et al., 2004). This global network should be loosely structured and should have the speed and agility to address the multi-faceted and rapidly evolving features of genomics and related biotechnologies. It should involve partners from multiple sectors to face the challenging complexities of biotechnology: academia, private sector, national governments, public-interest groups, nongovernmental organizations, and media. Its inclusive nature could facilitate collaborative decision-making and help to minimize risks associated with new technologies (restricting new technologies to a “club” potentially encourages dangerous misuse by those who are excluded). And it should encourage participation and leadership from developing countries rather than only from the developed world. A focused, collaborative initiative—such as the Global Genomics Initiative—that aims to promote genomics as a global public good could reinforce these efforts and channel them towards one of the most pressing issues of our time—improving global health.
Genomics and related biotechnologies are relevant to and should be harnessed for purposes of global development and health so the benefits of the Human Genome Project will reach the 5 billion people who need them the most—not just the privileged 600 million in the developed world. It will increase the likelihood that the inhabitants of Collins’ genomics house will come from all over the world.
Funding
This work was funded by the Canadian Program on Genomics and Global Health (CPGGH). CPGGH receives most of its funding from Genome Canada and the Ontario Research and Development Challenge Fund. A full list of funders is available at www.geneticsethics.net. Abdullah S. Daar is supported by the McLaughlin Centre for Molecular Medicine at the University of Toronto, and Peter A. Singer is supported by a Distinguished Investigator award from the Canadian Institutes of Health Research.
References
Acharya T, Daar AS, Thorsteinsdóttir H, Dowdeswell E, and Singer PA. 2004. Strengthening the Role of Genomics in Global Health. PLoS Med 1(3):e40.
Advisory Committee on Health Research. 2002. Genomics and World Health. Geneva: WHO.
Annan K. 2003. A Challenge to the World’s Scientists. Science 299:1485.
Balmaseda A, Sandoval E, Perez L, Gutierrez CM, and Harris E. 1999. Application of Molecular Typing Techniques in the 1998 Dengue Epidemic in Nicaragua. Am J Trop Med Hyg 61:893–897.
Benatar SR, Daar AS, and Singer PA. 2003. Global Health Ethics: The Rationale for Mutual Caring. International Affairs 79:107–108.
Collins FS, Green ED, Guttmacher AE, and Guyer MS; U.S. National Human Genome Research Institute. 2003. A vision for the future of genomics research. Nature 422: 835–847.
Commission on Macroeconomics and Health. 2001. Macroeconomics and Health: Investing in Health for Economic Development. Geneva: WHO.
Daar AS, Thorsteinsdóttir H, Martin DK, Smith AC, Nast S, and Singer PA. 2002. Top 10 Biotechnologies for Improving Health in Developing Countries. Nat Genet 32:229–232.
Dowdeswell E, Daar AS, and Singer PA. 2003. Bridging the Genomics Divide. Global Governance: A Review of Multilateralism and International Organization 9:1.
Global Forum for Health Research. 2002. 10/90 Report on Health Research 2000–2001. Geneva: Global Forum for Health Research.
Harris E, Kropp G, Belli A, Rodriguez B, and Agabian N. 1998. Single-Step Multiplex PCR Assay for Characterization of New World Leishmania Complexes. J Clin Microbiol 36:1989–1995.
Jomaa H, Wiesner J, Sanderbrand S, Attincicek B, Weidemeyer C, Hintz M, Turbachova I, Eberl M, Zeiler J, Lichtenthaler HK, Soldati D, and Beck E. 1999. Inhibitors of the Nonmavalonate Pathway of Isoprenoid Biosynthesis as Antimalarial Drugs. Science 285:1573–1576.
Kaul I, Grunberg I, and Stern MA. 1999. Global Public Goods: International Cooperation in the 21st Century. New York: Oxford University Press.
King, Jr, ML. 1968. Remaining Awake through a Great Revolution. Speech Delivered at the National Cathedral, Washington, DC, on 31st March. Congressional Record, 9 April 1968.
Missinou MA et al. 2002. Fosmidomycin for Malaria. Lancet 360:1941–1942.
Pang T. 2003. Equal Partnership to Ensure that Developing Countries Benefit from Genomics. Nat Genet 33(1):18.
Pavitt K. 2001. Public Policies to Support Basic Research: What Can the Rest of the World Learn from U.S. Theory and Practice? (And what they should not learn). Industrial and Corporate Change 10(3):761–779.
Sandler T. 1997. Global Challenges: An Approach to Environmental, Political and Economic Problems. Cambridge: Cambridge University Press.
Stiglitz JE. 1999. Knowledge as a Global Public Good. In: Kaul I, Grunberg I, and Stern MA, eds. Global Public Goods: International Cooperation in the 21st Century. New York: Oxford University Press. Pp. 308–325.
Thorsteinsdóttir H, Daar AS, Smith RD, and Singer PA. 2003. Genomics: A Global Public Good? Lancet 361:891–892.
Thorsteinsdóttir H, Quach, U, Daar, AS, and Singer PAS. 2004. Conclusions: Promoting Biotechnology Innovation In Developing Countries. Nature Biotechnology 22(Supplement):DC48–DC52.
UNESCO. 1997. Universal Declaration on the Human Genome and Human Rights. Geneva.
Woodward D and Smith RD. 2003. Global Public Goods for Health: Concept and Policy Issues. In: Smith RD, Beaglehole R, Woodward D, Drager N, eds. Global Public Goods for Health: A Health Economic and Public Health Perspective Oxford: Oxford University Press.
PUBLIC HEALTH FOR ALL: WORKFORCE DEVELOPMENT THROUGH AN INTEGRATED APPROACH TO HEALTH CARE CURRICULA
Walid El Ansari, M.D., D.T.M.&H., M.P.H., Ph.D.
Postgraduate Public Health Programme
School of Health and Social Care, Oxford Brookes University
Oxford, United Kingdom
There have been calls for a worldwide change in the education of health professions to ensure that the actions of graduates will contribute to the improved health status of populations. The new investments in workforce development are unprecedented (Potter, 2001), triggered by the increasing costs of care. This has prompted the training in the health professions generally and public health (PH) particularly to focus on improving efficiency and cutting costs, while maintaining gains in life expectancy and morbidity reduction. More and more evidence suggests that for the broader socio-health needs to be tackled, a more coherent community-based PH mind-set will be required (Ewles and Simnett, 1999; El Ansari and Phillips, 2001; El Ansari et al., 2004).
In the face of such sentiments, however, a wide range of health professionals are poorly equipped to think in terms of and deal with population-based health principles and philosophies. Thus, there is an increasing need for educational programs that can improve the breadth, awareness, and training of a wide variety of health professionals on PH concepts and thinking, as well as on epidemiologic approaches and methodologies. Different health problems will require PH responses mounted at various local, regional, state, or international levels (Veenema, 2001). This fact highlights the greater need for PH competencies within primary care (Colin-Thomè, 1999). Well-trained PH-oriented health professionals can form the basis of a strong national health care system. Hence, different groups, including clinicians, policy makers, academics, and educators, could promote the PH perspective, providing that they are better educated in epidemiology, health service evaluation, and health promotion (Dalziel, 2000). Consequently, incorporating public health threads and concepts into the health professions’ curricula offers a way forward (El Ansari et al., 2003a).
As illustrated in Figure A-1, the workforce necessary to accomplish the needed improvement in the population’s health must be supported with strong training programs that bring to attention a variety of health education and health promotion roles, while providing an increased understanding and awareness of the wider PH context in which health professionals practice (Latter and Westwood, 2001). In order to ensure a prompt and
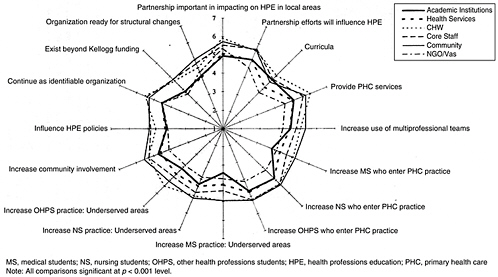
FIGURE A-1 An integrated view of the public health workforce.
SOURCE: El Ansari, W. 2003. “Educational Partnerships for Health: Do Stakeholders Perceive Similar Outcomes?” Journal of Public Health Management and Practice 9(2): 136-156, Figure 2. Reprinted with permission.
effective response to overarching population problems, the knowledge and skills required for the promotion of community health (Bollag et al., 1982) need to be better integrated into the training of all health professionals. To accomplish this, it will be necessary to weave together the various skills, knowledge, attitudes, and worldviews of the multiple professions. When public heath workers are all those responsible for providing the essential services of public health regardless of the organization in which they work (DHSS, 1994), the importance of the “general” workforce contribution to an effective public health infrastructure comes to the fore. The vision is to broaden knowledge about health and disease by an inclusive designation of a primary care-oriented, disease-oriented, patient-oriented, population-oriented, and prevention-oriented PH education. As such, widening the PH infrastructure will have to take into consideration both the clinical affiliations of students and graduates and their PH credentials (Rowitz, 1999).
There are many published reports on the range of public health competencies required in primary care (Carlson and El Ansari, 2000; El Ansari, 2004) and the training of “specialist” PH professionals (Carlson and El Ansari, 2001). Likewise, the development of both postgraduate PH programs (El Ansari et al., 2003b) and health protection programs (El Ansari and Privett, 2005) for the advancement of a “dedicated” PH workforce (Potter, 2001) have also been described. What emerges is that the literature on the widening of the PH human infrastructure, the “broader” PH workforce that could be capitalized on, is sparse. For instance, the introduction of PH concepts into a wider range of health care curricula seems to have received less attention (El Ansari et al., 2003a). These considerations form the underpinning of this report.
Aim and Methods
The aim of this report is to emphasize some of the issues that require attention in developing a strategy for the establishment and development of appropriate team concepts in heath care curricula. The insights reported represent the initial “brainstorming” sessions that were held separately by the author with each of five staff members of the Department of Public and Community Health at the School of Health and Social Care, Oxford Brookes University, Oxford, United Kingdom. The purpose of the sessions was to explore the members’ perceptions of the way forward so that PH principles could be incorporated into the school’s wider health care curricula. After the initial brainstorming, SWOT (Strengths, Weaknesses, Opportunities, and Threats) analysis sessions were undertaken, and the author grouped the emerging themes and concerns into categories. The focus was fourfold: to highlight the areas of strengths that are already present, to capitalize on the potential opportunities that could be anticipated, to draw attention to the
aspects that represent weaknesses to the endeavor, and to identify possible threats that could affect the effort. Originally, the SWOT analysis generated a long list of topics. The Delphi technique was then used to condense the list by employing several rounds of refinements (Yuen et al., 2002). The five participants were asked to highlight the issues they felt were pertinent. Three rounds of refinements were undertaken, and after each round of fine-tuning topics were eliminated from or added to the list. Thus, the more pertinent issues were progressively distilled and focused on, while the less influential ones were gradually withdrawn. The main findings of this exercise are depicted below.
Findings
It was not straightforward to categorize the different factors that emerged from the sessions into strengths or weaknesses (or alternatively, as opportunities or threats), as according to the specific circumstances of each institution, a particular factor could sometimes represent a potential strength or alternatively a possible weakness. This SWOT categorization (see below) also needs to take into account the time frame of operation of any factor in question: a particular weakness today could, if acted on, be rendered a formidable strength tomorrow. The fluid nature of the factors exhibited below meant that they are subject to a range of country- and institution-specific aspects: for instance, the overall political situation, the prevailing health policy directives, the vision of the institution’s senior management, and funding arrangements, as well as professional requirements and legislation, can all determine whether a factor is seen to be a strength or a weakness. In order to highlight the factors and their subdivisions, they have been italicized.
Strengths
Policy
At the national level, the questions will have to address the presence or absence of government policies and the national climate in favor of PH. At the institution or the school levels, a parallel political commitment of the institution’s senior management is necessary. The presence of market forces pointing to a need for health professionals with PH knowledge and background, and the availability of a local and national market niche for multidisciplinary PH, are favorable points. The commitment and motivation of a critical mass of the institution’s staff to PH and their motivation in taking the PH agenda forward is another positive aspect. However, resources need to be considered in terms of the availability of a fair amount of dispersed PH knowledge and expertise within the institution, or whether
some PH concepts already present in a number of areas of the school’s curricula provide a modest starting foundation to build on. Here, baseline information about the available quality and quantity of PH in the curricula or whether any curriculum audit or mapping exercise had been undertaken would be useful. Finally, external contacts, such as local influential organizations, deaneries, PH resource agencies, or other local/regional universities, are seen as definite strengths. Similarly, other assets include any national links that some of the PH-enthusiastic members of the institution are already engaged with or international networks to which they contribute.
Weaknesses
Resistance and Anxiety
The reasons for any resistance to the move toward introducing PH principles within the broader health care curricula will need to be understood. For instance, is there poor staff understanding about where PH could fit in their curricula? At times, resistance could be partly attributable to the patchy nature of PH and health promotional activity within the national health system and health policy atmosphere of the country. As a response, health students might perceive that this topic relates little to their everyday practice world. The internal politics of the institution may also play a role: are some staff unwilling to cooperate with PH initiatives as a reaction to negative foregone situations? On the other hand, with too many initiatives going on, some staff could be suffering from change fatigue. Similarly, anxiety about PH could be generated due to insufficient background training of staff to teach or learn epidemiologic and population concepts or due to the complexities of the highly contextualized PH problems where the social and psychological domains are important. Such problems might represent challenges to the more “traditional” work of the institution.
Commitment and Resources
Low commitment to PH in some sectors of the institution represents one weakness. Already over-stretched time and other resources represent another. The pressures on course leaders to respond to many stakeholders’ wishes for programs to incorporate current national and local policy priorities might affect their commitment to exploring the introduction of PH elements in their curricula.
Operationalization and Empowerment
In order to operationalize the PH concept, there needs to be a good fit between the agreed-upon school policy and the operationalization of such policy at a senior level. Hence, the lead department introducing the strategic changes should not be isolated from other departments within the school. This could be further complicated if the school is multi-sited and is dispersed on several campuses, as such geographical fragmentation might affect the way that strategic change takes place. A related point has to do with empowerment: are staff members who are responsible for policy implementation and operationalization of the initiative empowered by the institution to actually “make the change happen”?
Control and Reactivity
At times, staff might believe that nursing is a “mystical” thing, and that the PH agenda being set by the government is increasingly radical. So a question to address is whether there exists a general domination in the school by certain professional groups that may not always be conducive to the acceptance of the PH agenda. An associated aspect is whether there is a lack of PH interest in some areas of the school with whom members of the lead department do not have regular and strong links. It frequently proves beneficial to an institution to be proactively responding to the health policy directives rather than being reactive as the directives become imperatives.
Opportunities
Political Drive and Advocacy
Opportunities for more PH-oriented health care curricula present themselves when there is a political drive for a PH focus both in higher education and health service provision. Similarly, a prevailing atmosphere of national advocacy and local policies in favor of PH is conducive to the initiation and maintenance of change.
Interest, Debate, and Resources
A good sign at the policy level is any provisional interest in PH indicated by the institution’s senior management. The presence of debates and deliberations on the appropriate mechanisms for bringing PH into the health care curricula at pre-registration and post-qualifying levels is seen as an opportunity window. At the financial and human resource allocation levels, any incoming research funds of the lead department instigating the change
can contribute to enhancing its reputation and may offer opportunities for recruiting more PH-skilled teaching support for the needs of the wider school.
Joint Working and Partnerships
Some of the questions to address in this domain include whether there is any interest in linking up with other partners (e.g., PH resources of the Department of Health and other regional universities) in order to develop a fellowship of PH education providers. Furthermore, any already established links with other PH institutions in the area that have a research focus could be capitalized on.
Reforms and Restructuring
In academic institutions, there are often strategic reforms of one sort or another being planned or implemented. Any current reorganization or restructuring of the school and/or university could serve as opportunity for initiating the required change to PH-oriented curricula. An interconnected aspect is whether the institution has already begun to make changes that indicate that PH “has to happen.”
Collaborative Links
Such connections focus on the possibilities for linking with other PH-related initiatives and programs within the institution. These links need to adopt a two-pronged approach. Around the university, the prospects include whether there are various PH strands within the institution, even if they have no specific focus, which could be linked into. Hence, networking with other departments that already are examining PH or primary care issues or linking with PH-orientated initiatives that the institution subscribes to (such as the Healthy Universities Initiative or Environmental Management Programs) are all important assets. The vision is to attempt to create a PH “critical mass” by way of forging connections between such initiatives, suitable schemes and parallel programs, and the lead departments. The second approach, within the school, focuses on teaching programs that already include a fair amount of PH that could act as a preparatory or initial platform for dissemination of the epidemiologic and population concepts. However, the vocabulary and terminology used by such programs will need to indicate and ascertain its PH content. When feasible, it could be useful to compare the lead department’s PH educational outcomes vis-à-vis other programs and modify where necessary. Capitalizing on school-wide change is also good practice: are there other areas of change that need to take place across the school curricula (such as inclusion and diversity), and could these be taken forward simultaneously?
Threats
The Department Leading the Change
A group of factors has to do with the lead department’s credibility, influence, and expertise. The lack of external or internal credibility of the lead department for the greater integration of PH across programs and other scholarly activity could act as a threat to the initiative. Some of the factors to address include whether the lead department is convincing and influential within the institution, and whether there are some members of the lead department with a high level of PH expertise and credibility. Is the size of the lead department and its academic team conducive to supporting the proposed changes? Does the lead department have sufficient resources in terms of funding and time to take this initiative forward across the whole school? Is there competition of the lead department with other established programs of international reputation?
Priorities, Competition, and Resources
The institutional priorities may sometimes override other efforts. For instance, there frequently are other initiatives that are being simultaneously implemented that could compete for institutional resources (for example, in the United Kingdom, the National Service Frameworks with Clinical Governance initiatives). In such cases, there will be a need to consider whether all the initiatives can be accommodated simultaneously within the institution. More common these days are funding cuts or impending threats, where staff are increasingly pressured to demonstrate more value for money.
Vision and Directives
This is critical. Required is a vision from the institution about where it should place itself within the local/national PH community. Sufficient, clear, and unambiguous directives from the senior management in relation to such issues are imperative; otherwise, PH could be viewed as another political “fad” that might just pass. Hence, any lack of senior staff conviction to invest speculatively in this area must be addressed.
Uncertainty
This presents a definite threat. When there are high levels of strategic change across the school and university, there usually are uncertainties about how and where the new policies and structures involving the institution’s or school’s reorganization and restructuring are going to settle.
This could be further complicated by uncertainties about sympathetic program leaders who could be leaving the institution, resulting in less support for the initiative.
Resistance and Barriers
Administrators and educators will have to identify what resistance to PH is encountered in which parts of the school. What are the origins of the barriers to incorporating PH concepts in the wider health care curricula? The factors that could contribute to resistance are varied and include the lack of staff members’ knowledge about PH concepts/skills, barriers of time and effort to be invested in the teaching of PH principles, barriers of ignorance, lack of awareness of potential solutions, and change anxiety, as well as personality clashes and low motivation. Similarly, beliefs that PH is “everybody’s responsibility but nobody’s business,” or little faith that the PH approach might improve the population’s health, are important threats to look out for.
Generalists or Specialists?
For 30 years medical educators, health professions students, and physicians in training have been hearing from the general public that health professionals should think more about primary care and less about specialization (Rosenberg, 1999). The generalist–specialist debate needs to be considered: is there evidence that specialization in some areas of health care squeezes out the PH agenda from the curricula, particularly where the specialization is in the form of technical procedures, technological measures, and other roles that are currently “falling off of the doctor’s table”?
Discussion
In the United Kingdom, public health skills deficits in qualified nurses have been identified through skills audits and training needs analysis (Latter and Westwood, 2001), and schools of health care and of medicine are increasingly aware of the need for developing competencies in public heath (Ibrahim et al., 1995). Similarly, in the United States concerns regarding the ability of the PH workforce to meet the changing needs of the American people have been voiced (DHSS, 1997), where the health of communities depends on the competence of 500,000 physicians, nurses, environmental health scientists, health educators, epidemiologists, and mangers working at the front lines of PH (Lichtveld et al., 2001). The vision becomes: how can a narrow base of frontline PH specialist workers be complemented with a “second line” of PH-oriented health professionals? To ensure the general
improvement in the health of the population, it will be necessary for those who are not PH specialists to understand the underlying principles of population health constructs and values (Dalziel, 2000). To these ends, this report has provided a melange of factors that will need to be considered in order to piece together the puzzle that academic and teaching institutions are likely to face when incorporating and consolidating PH principles in their health and social care curricula.
Until recently, the vast majority of state health agencies were led by individuals without PH education or experience (Association of State and Territorial Health Officials, 1997). But at the heart of all successful PH activities are the PH workers, who with their focus on populations and communities take their own work beyond their individual professional and technical skills. On the one hand, PH agencies are providing more population-focused services to entire communities and fewer personal services to individuals (Gebbie, 1999). But on the other hand, there also is a need to include in the new PH movement the vast majority of heath professionals who are providing more patient-focused interventions. If the PH infrastructure is to be widened, then the skills and abilities of the different health profession groups must be challenged with up-to-date knowledge and skills to deliver essential PH service effectively. Since PH is an interdisciplinary field, no effort to improve the skill of the workforce can succeed by concentrating on a single profession (Gebbie, 1999). Only by focusing on all the health professions, and within a collective and preventive population-oriented context, will health and social workers be able to address the real determinants of disease and infirmity while promoting health.
Such aspirations are attainable only if PH notions are integrated into the education of the different health professions, preferably at the undergraduate level. But the delivery of quality PH concepts and training to non-specialist health professionals working in the field is also a challenging endeavor. Nevertheless, well developed and appropriately timed training, focused on the main PH competencies that a non-specialist PH worker would require, could play a key role in widening the competency base necessary to meeting the challenge of a narrow and constricted PH infrastructure.
Making the change toward more PH-oriented curricula is neither a straightforward effort nor an easy undertaking. For this reason, committed leadership will be critical to setting the change process in motion. Leading the change in organizations is an incremental process (Kotter, 1996). Thus, the initiators of the effort will need to exhibit leadership focused on overcoming barriers. Therefore, their first step would be the motivation of other departments/staff members to consider both the necessity and benefits of introducing PH notions into the curricula. The initiators could also establish a sense of urgency, garner support, and aid in the development of a vision and strategy. Because old practices do not change overnight, and
resistance to changing established practices is a predictable human response (Lorsch, 1986), senior management will be required to empower the staff for broad-based action, to consolidate the gains, and ultimately to anchor the new approaches in the organization’s culture (Kotter, 1996).
It is only realistic to expect resistance. Therefore, it will be necessary to be prepared to cope with resistance by understanding what causes it. Silence is the toughest form of resistance and should never be taken for implicit consent to the change. To keep the initiation of change momentum, an understanding, rather than agreement, needs to be the goal. Hence, lead departments need to understand the relevant internal and external actors’ behavior, intentions, interrelations, agendas, and interests that could influence decision making (Blair et al., 1990). Undertaking a force field analysis (Ewles and Simnett, 1999) could help identify the helping and hindering forces. Here, the lead department will need to reflect on some questions regarding the range of stakeholders, their attitudes and power, and their criteria for agreeing to the change. If shifting the “traditional” health care curriculum to a more “innovative” public health-oriented one is to be successful, then PH and primary care need to be in free love rather than in an arranged marriage (Sim and Mackie, 2002).
Conclusion
If health professions graduates are to contribute to the improved health status of the population, then there is a pressing need for a change in their education. The aspects that necessitate consideration in such educational efforts span the macro, meso, and micro levels. They include such potential strengths as the prevailing policy, market forces, commitment and motivation to the effort, and the availability of resources, information, and external contacts. Features such as political drive and advocacy, interest in the education debate, collaborative links through joint working and partnerships, and ongoing internal reforms and restructuring could all act as opportunities. However, resistance and anxiety are stumbling blocks, the operationalization of the effort and empowerment of those leading it need to be considered, and issues of control and interests are critical. The presence of conflicting priorities and competition, the lack of vision and directives, and/or uncertainty about change could act as threats and barriers to the effort.
Within primary care, widening the foundation of health professionals with PH competencies suggests that higher education bodies will need to adapt their curricula to an approach that highlights population-based health principles, preventive philosophy, and PH concepts and methods. However, a way forward would need to embrace a multi-pronged approach.
National/local data on the composition and distribution of PH-oriented teachers and health professionals is important. A dynamic staff develop-
ment program that discusses PH on an individual, group, and community level could prove useful. Similarly, curricular modification might require to be placed as a separate item on the agendas of program boards, and program leaders and directors could be invited to discuss how the national PH agenda is reflected in their curricula. A parallel approach would be to ensure that the school’s programs are set within an educational trajectory that is strategically linked to the continuing professional development within the various service providers with whom the school “contracts.” PH concepts could also be included in mentor preparation sessions and in discussions by link lecturers with mentors and practitioners. Monitoring the changes locally within the institution could be accomplished by including PH as a specific category in the annual review process of the programs. Nationally, the Faculty of Public Health, the Nursing and Midwifery Council, and/or the Workforce Development Confederations could scrutinize the PH program content through course validation and approval processes. The instigation of standards for the PH learning objectives is an asset, and a national framework for certifying/credentialing of the PH content of curricula would also be an advantage. Hence, a coherent policy framework as well as a national agenda on workforce development will need to be in place. However, research will be required to verify that “learning PH concepts” actually leads to the use of such population elements by health professionals in their later everyday practice. If shifting the traditional health care curriculum to a more innovative PH-oriented one is to be a success, then administrators of educational change will need to take into account a mélange of factors and stakeholders involved in a gradual and incremental process.
References
Association of State and Territorial Health Officials. 1997. 1997 Salary Survey of State and Territorial Health Officials. Washington, DC: Association of State and Territorial Health Officials.
Blair JD, Slaton CR, and Savage GT. 1990. Hospital–Physician Joint Ventures: A Strategic Approach for Both Dimensions of Success. Hospital and Health Services Administration 35:3–26.
Bollag U, Schmidt HG, Fryers T, and Lawani J. 1982. Medical Education in Action: Community-Based Experience and Service in Nigeria. Medical Education 16:282–289.
Carlson CL and El Ansari W. 2000. Squaring the Circle: Developing Public Health Competencies in Primary Care. Nursing Times Research 5(2):2–14.
Carlson C and El Ansari W. 2001. Improving Health: Postgraduate Public Health Education—Experience from the UK. Africa Journal of Nursing & Midwifery 3(1):25–29.
Colin-Thomè D. 1999. Primary Care Perspectives. In: Griffiths S, and Hunter D, eds. Perspectives in Public Health. Oxford: Radcliffe Medical Press.
Dalziel M. 2000. Leadership for Health. How Can We Ensure that the Values and Principles of Public Health Become Central to Health and Social Policy? Journal of Epidemiology and Community Health 54:703–704.
DHHS (Department of Health and Human Services). 1994. The Public Health Workforce: An Agenda for the Twenty-first Century. Washington, DC: U.S. Government Printing Office.
DHHS (Department of Health and Human Services). 1997. The Public Health Workforce: An Agenda for the 21st Century. A Report of the Public Health Functions Project. Washington, DC: Government Printing Office.
El Ansari W. 2004. Appraisal Skills as a Public Health Competency for Evidence-Based Care: Student Satisfaction with their Research Education. Journal of Public Health Management and Practice 10:354–365.
El Ansari W and Phillips CJ. 2001. Empowering Health Care Workers in Africa: Partnerships in Health—Beyond the Rhetoric Towards a Model. Critical Public Health 11:231–252.
El Ansari W and Privett S. 2005. Health Protection: Communicable Disease, Public Health and Infection Control Educational Programmes—A Case Study from the UK. Public Health 119:328–340.
El Ansari W, Russell J, Spence W, Ryder E, and Chambers C. 2003a. New Skills for a New Age: Leading the Introduction of Public Health Concepts in Health Care Curricula. Public Health 117(2):77–87.
El Ansari W, Russell J, and Wills J. 2003b. Education for Health: Case Studies Of Two Multidisciplinary MPH/MSc Public Health Programmes in the UK. Public Health 117:366–376.
El Ansari W, Phillips CJ, and Zwi AB. 2004. Public Health Nurses’ Perspectives on Collaborative Partnerships in South Africa. Public Health Nursing 21:277–286.
Ewles L and Simnett I. 1999. Promoting Health. A Practical Guide. 4th ed. Edinburgh: Balliere Tindall.
Gebbie KM. 1999. The Public Health Workforce: Key to Public Health Infrastructure. JAMA 89(5):660–661.
Ibrahim MA, House RM, and Levine RH. 1995. Educating the Public Health Workforce for the 21st Century. Family & Community Health 18:17–25.
Kotter JP. 1996. Leading Change. Cambridge MA: Harvard Business School Press.
Latter S and Westwood G. 2001. Public Health Capacity in the Nursing Workforce. Phase 1: A Pilot Project to Identify Current Practice in Educational Preparation. School of Nursing & Midwifery: University of Southampton. [Online]. Available: www.hda-online.org.uk/html/resources/publications.html [accessed April 18, 2002].
Lichtveld MY, Cioffi JP, Baker EL, Bailey SBC, Gebbie K, Henderson JV, Jones DL, Kurz RS, Margolis S, Miner K, Thielen L, and Tilson H. 2001. Partnership for Frontline Success: A Call for a National Action Agenda on Workforce Development. Journal of Public Health Management and Practice 7(4):1-7.
Lorsch J. 1986. Managing culture: The Invisible Barrier to Strategic Change. California Management Review 28:95–109.
Potter MA. 2001. A Twenty-First Century Call for Public Health Workforce Development. Journal of Public Health Management and Practice 7(4):vi–vii.
Rosenberg LE. 1999. Physician–Scientists: Endangered and Essential. Science 283(5400): 331–332.
Rowitz L. 1999. The Mystery of Public Health Workforce Development. Journal of Public Health Management and Practice 5:101–105.
Sim F and Mackie P. 2002. Editorial: Public Health and Primary Care; Arranged Marriage or Free Love? Public Health 116:67.
Veenema TE. 2001. An Evidence-Based Curriculum to Prepare Students for Global Nursing Practice. Nursing and Health Care Perspectives 22:292–298.
Yuen PP, Gould D, and Cheng MY. 2002. Rationing Hospital Services in Hong Kong: Priority Setting by Clinicians Using the Delphi Method. Health Services Management Research 15:1–13.
STAKEHOLDERS’ PERCEPTIONS OF OUTCOMES IN PUBLIC HEALTH EDUCATIONAL PARTNERSHIPS
Walid El Ansari, M.D., D.T.M.&H., M.P.H., Ph.D.
Postgraduate Public Health Programme
School of Health and Social Care, Oxford Brookes University
Oxford, United Kingdom
Partnership building has been considered an imperative for the new millennium. Partnerships have emerged as widespread components of public health strategies on a wide range of issues and platforms. At the local level, partnership building has been recognized as a strategy for the reduction of immunization disparities (Findley et al., 2003) and the decrease of ethnic discrepancies in the utilization of community services and the improvement of preventive care in vulnerable populations (Crist and Escandon-Dominguez, 2003). At the national level, partnerships have been used in diverse public health policy perspectives, from public health preparedness in the United States (Morse, 2003) to improving the coordination of health and social care in the United Kingdom (Department of Health, 1992). At the international level, the World Health Organization (WHO) and the International Labor Organization are strengthening the concept of public–private partnerships (Haroon, 2003), the Stop TB partnership initiative of the WHO advocates national partnerships for tuberculosis control (Steenbergen and El Ansari, 2003), and global public–private partnerships (Buse and Walt, 2000) and community-health services partnering for HIV/AIDS prevention (Goede and El Ansari, 2003) are becoming increasingly common. Whether the partnership is at the local (micro), national (meso), or international (macro) level, strategic planning has given way to strategic partnering, and the notion of competitive advantage has been transformed into the idea of collaborative advantage (Shannon, 1998). This report will focus on partnerships of the micro order: the local level where health providers, nursing teaching institutions, and community organizations and agencies come together.
Effective partnerships among government agencies, community-based organizations, and academic and medical institutions are advancing public health in the United States (Northridge, 2003) and South Africa (El Ansari et al., 2002). As the journey to tackling the long-standing health challenges progresses, there is a recognition that solutions lie within a broader framework than any individual efforts. Hence, there has been an expansion of the notion of partnerships to embrace those within and outside the health sector who can work collaboratively toward eliminating health disparities
and other inequalities (Northridge, 2003). Collaboration involves working jointly with others on a project, where the participating agencies take on specified tasks within the project and share responsibility for its ultimate success (Michigan State University, 1996).
El Ansari et al. (2001) reported that although the literature makes distinctions among the terms “collaboration,” “partnership,” and “joint-working,” they are used interchangeably to describe collective actions by individuals or their organizations for a more shared communal benefit than each could accomplish as an individual player. However, as there are many factors that could sustain or frustrate collaborative efforts (El Ansari and Phillips, 2001a), it is reasonable to expect that some arrangements for collaboration are more effective than others (Levin et al., 2002). By the same token, the many dimensions that are associated with partnership effectiveness indicate that such alliances will need continuous and ongoing attention and fostering if they are not to be fragile entities (Waddock and Bannister, 1991).
A central concern for public health partnerships is the accomplishment of the outcomes they set out to attain (El Ansari, 2003). On the one hand, the parties participating in partnership efforts might perceive a variety of challenges to collaborating because the outcomes are uncertain. On the other hand, the outcomes of collaboration have, in many instances, far exceeded the expectations of all the parties (Gray, 1989). Furthermore, short-term successes need not be mistaken for ultimate solutions to chronic problems and endemic concerns. While short-term effects are the immediate results of a program, long-term effects often extend from short-term effects (Linney and Wandersman, 1991) to encompass system changes in service delivery, system reform, cross referrals among agencies, and new community linkages (Kagan, 1991).
The achievement of the outcomes of partnerships is a critical variable to include in studies of partnership behavior (Murnighan, 1978). Nevertheless, any measurement/s pertaining to the attainment of the desired expectations will need to consider whether the “gaze” and scope of the evaluation is on macro- or micro-level outcomes, individual or social impacts, and the utility of employing proximal or distal indicators (El Ansari et al., 2001). Such dichotomies must take into account the different types and sources of data to be accessed, the variety of criteria to be available for purposes of assessment, and a judgment about the potential tradeoffs between them (Phillips et al., 1994). When all of these points have been deliberated, a question then arises: do stakeholders with different value systems and diverse cultural backgrounds actually perceive similar outcomes of their partnership efforts? These considerations formed the underpinning of this report.
Aims and Methods
The aims of this report are to:
-
Describe five South African community partnerships for health professions education and a range of their anticipated outcomes.
-
Test the appropriateness of employing “generic” stakeholder groups in partnership research. This is accomplished by examining whether certainty levels about outcomes would differ when the two generic stakeholder factions were broken down into six tightly defined “specific” partner groups.
-
Explore whether those groups out of the six specific partners who perceived greater certainty about the outcomes would also experience higher ratings on other related partnership functioning contentment parameters.
In fulfilling these aims, the concepts that are presented are premised on the findings of a research study that was undertaken by the author with the participation of five community partnerships in various locations in South Africa. The research tools employed in the study comprised self-administered questionnaires (N = 668) (El Ansari, 1999; El Ansari and Phillips, 2001b) and interviews (N = 46) (El Ansari and Phillips, 2001c), both of which have been detailed elsewhere and are beyond the scope of this report.
The W. K. Kellogg Foundation Initiative
The Kellogg Foundation launched its programs in Africa in 1986. Within 5 years, the foundation was to support the development of a major initiative: Community Partnerships for Health Professions Education (Henry, 1996a). This initiative was patterned along the lines of similar efforts begun in the United States in 1990 and in Latin America in 1992. The main purpose of this enterprise was to improve health care for communities by reorienting the education of health personnel through a partnership between health professionals and communities in order to reach a broad understanding of health issues within a specific social context. Hence, the essential strategy for these initiatives was the sharing of models of academic–community partnerships, and the focus was on population groups and individual persons, while also taking into account the health needs of the communities concerned (WHO, 1987).
Starting as early as 1992, a number of South African community partnerships (CPs) for health professions education (HPE) were created as
linkages between communities and educational institutions. The aim of these partnerships was to address the reform of the way medical, nursing, and allied health professions were trained. Engineered as joint ventures between the local and regional health service providers and the academic medical and nursing training institutions, on the one hand, and the beneficiary communities and their civic organizations, on the other hand, the CPs were intended to train health professionals in an interdisciplinary, community-oriented, and community-based fashion. Such sentiments were appropriate for the young democracy that was evolving in South Africa. Within this context, a broad range of health personnel were required to address the overwhelming needs of the majority of people who were previously excluded from quality health care (El Ansari, 2002). These responses were clearly demonstrated by the emphasis on program activities of each of the partnerships. In the section below, the partnerships are made anonymous for reasons of confidentiality.
Partnership No. 1
This partnership comprised a consortium of the health services development unit of the university in the region, the local health service providers at two local hospitals, and four local communities. As such, the partnership had a solid foundation in the community and in the institutions in the area. The project’s focus was on the development of a community college. It was envisioned that the college would serve to bridge the gap between secondary and tertiary education as well as including adult literacy training and programs for health workers. The partnership activities included bridging programs, vocational training, and health worker programs. The communities involved had been politically active and represented a strong stakeholder group. Through local civic and traditional/tribal systems, the partnership has been able to set up successful management systems that link the community with the health services. Stronger links with the university and other medical and nursing educational institutions were on their way to being established.
Partnership No. 2
In this partnership, the university had committed to initiate affirmative action in student selection and to develop support systems for disadvantaged students at the university. The vision was to promote more effective community-oriented health professions training as well as the development of relevant training for community health workers. With wide community support, and a decision to approach governmental and nongovernmental sources for funding, a multipurpose community center was strategically set
up within the beneficiary community, as such a center was beyond the resources of the local government. The center provided a primary health care (PHC) service component, a PHC development unit for income generating activities, and also served as a community resource center. In parallel, the local health service (the provincial administration of the region) had pledged funds toward the development of part of the community center. By a process of consultation and networking with the existing health services that were provided by the municipality, the partnership aimed to improve the primary level health services of the people.
In view of the disadvantaged nature of the community, it was not possible to engage the community in a project that only addresses primary health care. The community perceived its urgent needs to be wider and of a higher priority than health care. It was envisaged that the community health center would serve as a focus for members of the community to move to deal with their priorities themselves. Outside the field of health care, the university was a valuable source of expertise. Activities at the center would facilitate the transfer of skills to the community.
In this partnership, all three of the partners were fully committed to the initiative, and they were highly respectful of each other. Since the initiative, there has been an increase in the number of “Black” students admitted to this once Whites-only regional university. Students now had a choice of receiving instruction in either Afrikaans or English, an option that did not exist before. Similarly, first-language Afrikaans faculty members were taking English courses, and the number of “Blacks” on the university faculty was increasing.
Partnership No. 3
The region where this partnership was set has a predominantly native African population. It was 95 percent rural and lacking in such infrastructure as water, sanitation, roads, and health facilities, due to the previous apartheid regime. The partnership comprised the university as the academic institution partner, the Department of Health and the municipality as service providers, and four local communities. The university was established in 1985, and from its inception, unlike the traditional medical schools in South Africa, it had been mandated to implement a community-based curriculum for medical training.
The partnership enabled the university to expand its vision to include a wide cross-section of health professionals. Thus, in addition to medical students, nursing and health education students and community health workers were trained. The main focus of the partnership was on appropriate training of health personnel and community health development, through initiating water, sanitation, and other projects.
Partnership activities included the development of academic community-based centers. Through the initiative, there was a move toward developing comprehensive health services, which were not previously available in this region. The stakeholders felt that the health service component was strong in this partnership, and that there was a great need for the university to strengthen its professional teaching staff by way of development of their capacities. Other activities included the establishment of the Department of Health Professions Education at the university, whose role included the whole medical school program in addition to the activities of the partnership, as these were inseparable. There was also a host of community development and social activities.
Partnership No. 4
This partnership comprised the two local nursing colleges and the nursing science department of the regional university as the academic partners. The health service providers were individually approached, and consisted of the provincial administration health services, which ran the heath care center in the locality, together with the regional Department of Health and the Department of National Health. The beneficiary communities in the region were approached through their residents’ association/s. The objectives were to prepare the partners for participation and, through developmental workshops, to strengthen the partnership’s management by enlisting 50 percent of the members from the community stakeholders. Other goals were to choose one community for the development of a PHC Teaching and Research Center, and to become involved in the training of community-based health workers.
The development of the PHC Training Center was accepted by the community and a steering committee was formed. The health service partners in the area were individually approached for their involvement. They responded by appointing representatives to serve on the partnership’s steering committee. Two of the training institutions in the area sent their students for community-based experiences at the beneficiary community where the health center was initiated. Lecturers from these educational institutions were on the partnership’s management committee.
Partnership No. 5
This partnership had as its goal the promotion of improved health care and health status of their disadvantaged communities through developing a model of HPE that is community-based. This was to be achieved through a partnership among the communities, the academic institutions, and the health service providers.
Three communities participated in this partnership. These communities were the most disadvantaged communities in the area. They were isolated, underdeveloped, lacked infrastructure, and had high levels of poverty and unemployment. The academic partner consisted of a wide array of training institutions: the health sector at the local university encompassed community health sciences, nursing, social work, psychology, physiotherapy, occupational therapy, child guidance, dietetics, human ecology, student counseling, and dentistry. Another participating educational institution was a local technikon, with its department of public health, department of paramedical services, and department of dental services. The health services partners included the regional services council and the provincial administration. The service providers at all levels had been very supportive of the partnership. For instance, frontline workers had been actively involved in managing the partnership, in training and supervising students in the field, and in research (planning and implementation of community surveys), as well as in teaching at the university.
The partnership recognized and accepted the idea that different models of community-based education would be developed at different sites, and in turn identified appropriate entry points into their target communities. The Community Health Center was employed as an entry point into one of the partnership’s beneficiary communities. Then there was a process of engaging the structures in the community sites with the goal of community-based interdisciplinary learning. Several academic departments were already active in the area, and it was envisaged that the local community health center could be transformed into an academic PHC center.
Common Challenges
The partnerships initially faced many common challenges. While some of the challenges had to do with the South African setting and context, others had to do with the principles and notions of partnership working. For instance, poverty in South Africa was and continues to be a primary cause of many health problems (UNICEF, 1989). Despite the fact that South Africa ranks as an upper-middle income country, the majority of its citizens live in poverty (Carter and May, 1999; Zimmerman, 2000). Combined with the lack of education about health, the people who were most in need of public health services often did not receive it. Furthermore, the South African health care system was divided according to race, geographic area, the public sector (further divided into local, provincial, and central health authorities), and the private sector. Today, the right of access to health care services is guaranteed by the South African Constitution (Ngwena, 2000).
There were no similar models of partnership initiatives in Africa from which to learn and benefit. For inspiration and models of partnership prac-
tice and fostering, stakeholders and partners had to look to the West. In addition, some institutional leaders were convinced that the community-based focus of these educational efforts would lead to a “lowering of standards.” An added aspect was that the leadership in some of the partnerships comprised people from cultural backgrounds different from that of the community/ies involved in the same partnership. In parallel, at the beginning of the efforts, the students who were undergoing the training in most of the institutions that participated in the partnerships were not from the communities that were partners in the initiative, nor did they come from the same cultural backgrounds. This was complicated by the fact that, because of the legacy of apartheid, there were inherent initial inequalities in these initiatives, where the communities were a “disadvantaged partner.” Finally, several of the partnerships had lost many of their leaders to jobs in government institutions and in the nongovernmental organizations sector.
Outcomes
As the partnerships aimed to achieve educational reforms for health professionals, the definition of success for the partnerships had critical implications. A number of ambitious outcomes were aspired to. These included HPE impact, curricular, and services outcomes, as well as student, community, policy, sustainability, and structural change outcomes.
Health professions education impact outcomes. One anticipated outcome of the community partnerships was to improve health professions education by way of creating alternative settings for the education of health professions.
Curricular outcomes. Another desired product was to modify the HPE curricula so that they revolve around responsiveness to community health needs, to become more community-based and to enable students’ participation. This was to be accomplished by changing the setting where learning takes place and linking with the communities by a process that included redesigning the curricula.
Services outcomes. The aim of the CPs was to provide an appropriate mix of quality primary care services that meet the needs of the community. Such a task needed to take into account issues surrounding teamwork activities between health and social care professionals.
Student outcomes. Another goal was to stimulate an increase in the number of qualified health and allied professionals who would appreciate the “community,” be responsive to the community, choose and enter primary health care practice as a career, and serve in underprivileged areas once they finish their training.
Community outcomes. Community involvement in health care reforms is a treasured outcome of the partnerships. The participation of local people,
the development of citizen-driven community action structures, and the empowerment of the community to participate as an active partner are all important to both the success and sustainability of the partnerships. The opportunities included offering the community partners specific active roles in the educational courses of the partnerships as well as improved community understanding of the university.
Policy outcomes. The CPs were promoting a primary care-oriented and community-based approach to health professions education. For such reasons, policy changes through the mobilization of a collective power base represented prized outcomes for the partnerships. The differing cultures, structures, and dynamics of community and academe come into play in the policy arena as they do elsewhere (Richards, 1996).
Sustainability outcomes. Long-term viability of CPs is associated with relationship building and group ownership (El Ansari, 2000a). Success in partnership work can be measured in terms of longevity (Staggenborg, 1986), where a more enduring effort is more likely to have impact (Kumpfer et al., 1993). Consequently, for extended survival, a variety of personnel, organizational, structural, financial, operational, and human factors and barriers need consideration (El Ansari and Phillips, 2001a).
Structural change outcomes. These outcomes embrace capacity building and social planning as well as system changes in service delivery, system reform, and new community linkages (Kagan, 1991). Accordingly, the extent to which the partnership efforts produce permanent changes for the participating professional institutions (Henry, 1996) and community lay organizations (El Ansari, 2000b; El Ansari and Phillips, 2001b) needed to be monitored.
Findings
The data collected from the five partnerships were pooled together, and the entire sample (N = 668) was initially categorized into two intuitive “generic” groups according to the organizations that the participants represented. The “professional” side of the partnerships (N = 301) comprised the health services providers, academic training institutions, and partnerships’ core staff (full-time, paid employees of the partnerships). Alternatively, the “community” side (N = 367) included the lay community, community health workers, and nongovernmental and community-based organizations and voluntary agencies. The levels of certainty of the two groups in relation to the accomplishment of 16 different anticipated partnership outcomes (clustered under the eight categories described above) were then compared.
The two generic groups had similar levels of certainty in 45 percent of the 16 outcomes under investigation. For the remainder of outcomes, the professionals were more conservative in their perceptions that such out-
comes would be accomplished. This was particularly true in relation to the policy outcomes (that the partnerships would influence the policies governing HPE), the sustainability outcomes (that the partnerships would continue as identifiable organizations or exist beyond Kellogg funding), and the structural change outcomes (that participating organizations were ready to implement structural changes to support the partnership). Similarly, for the student outcomes, the professionals were wary about whether the partnerships would affect the specializations that the medical students would choose to dedicate themselves to and the localities where they would serve once they completed their training. However, for all the outcomes, the range of responses of the groups indicated a moderate to good level of certainty that their partnerships would achieve the aims that they set out to attain.
Next, the two generic stakeholder groups were broken down into six different and more precise specific partners: the academic training institutions (N = 130), the health and other government services personnel (N = 111), community health workers (N = 70), core staff (N = 60), lay community (N = 166), and nongovernmental and community-based organizations and voluntary agencies (N = 131). Once more, the certainty levels of the six groups in relation to the accomplishment of the 16 anticipated partnership outcomes under study were compared.
A different picture emerged. When the partners were broken down into their specific groups, their responses indicated remarkable and significant differences in the levels of certainty in relation to the partnerships’ anticipated outcomes. First, for all the outcomes, the range of responses of the six partner groups indicated a fair to good level of certainty that their partnerships would achieve the activities that they set out to attain. Second, the emerging pattern was that the community members, the community health workers, and the partnerships’ core staff perceived more certainty about the outcomes. On the other hand, the academic institutions, the health service providers, and, especially, the representatives of nongovernmental organizations and voluntary agencies were more cautious about whether the intended outcomes would be achieved. There seemed to be a “certainty” gap between these two polar partner groups. This certainty gap was wide and distinct for some of the anticipated services, sustainability, and community outcomes, and conversely the gap was narrow and hazy in relation to the health professions education impact outcomes as well as structural change outcomes.
Third, there was an “onion skin” appearance in the levels of each group’s certainty. Each of the stakeholder groups frequently had a “harmonious” level of certainty about most of the outcomes related to their partnerships. Each partner group exhibited an “orbit” of assertion where most of their responses were located. Different stakeholders orbited had dissimi-
lar levels of confidence in the accomplishment of outcomes. At most times, each group was more or less confined to its orbit. However, for certain outcomes, groups momentarily departed from their established certainty levels (orbit) to other higher or lower ones. Hence, the term “orbital” hypothesis was employed to refer to the onion-skin appearance of the relatively distinct, multiple, successive, and incremental levels of certainty that different specific stakeholders and partners exhibited in relation to their partnerships’ outcomes.
In order to verify further whether such an orbital hypothesis held true not only for the partnership outcomes but also for other partnership variables, the study went on to explore whether the six specific partners who perceived greater certainty about the outcomes would also experience higher ratings on other related partnership parameters. Hence, the groups’ perceptions as regards another 15 partnership “feel-good” (contentment) variables, inspired from the literature as being critical to the effective fostering of collaborative efforts (El Ansari and Phillips, 2001a), were measured. These contentment variables addressed a wide range of fulfillment and approval issues: for example, satisfaction with the partnerships’ operations, sense of ownership for the partnerships’ accomplishments, and commitment in terms of endorsing or adopting the partnerships’ missions. They also focused on partnership and member participation: for example, the partnerships’ involvement in the educational activities of the targeted beneficiary localities, and members’ personal contribution and involvement in their partnerships. The feel-good dimensions similarly included whether there were formalized rules and procedures, adequate operational understanding of the partnerships’ operations, good quality flow of information, and appropriate leadership skills. Several authors (Gottlieb et al., 1993; Herman et al., 1993; Rogers et al., 1993) have highlighted the importance of these parameters.
The stakeholder perceptions of the feel-good variables that are critical to partnership fostering suggested that, with some exceptions, the three partner groups who scored the highest certainty levels in relation to the anticipated outcomes of the CPs were the same groups that scored highest on the other feel-good variables. These findings provide direct supportive evidence for the certainty gap referred to above. For instance, the community health workers, the partnerships’ core staff, and the community members exhibited significantly higher levels of sense of ownership, commitment, and contentment with the flow of information in their partnerships. Similarly, significantly more participants from these groups indicated high involvement levels in their partnerships, had more belief that their partnerships had long-range plans, and knew the organizational structure and staffing of their partnerships and what their roles in the partnerships were. In addition, more of them reported contentment with the information they
receive from their partnerships’ leaderships. These findings lent additional support for the orbital hypothesis: stakeholder groups’ perceptions of the multiple facets of their partnerships are usually harmonious, forming rather discrete orbits of opinions and experiences for each partner, which are at times departed from, but usually returned to.
Such findings have direct and important implications in relation to the research and evaluation challenges that pose themselves when measuring stakeholder satisfaction to the multiple facets of partnership fostering. If the orbital hypothesis is verified by further research in a range of partnership contexts and settings, then its applications could be staggering. Researchers and partnership administrators could finally be able to measure a mere handful of aspects of the stakeholders’ perceptions of their partnerships’ functioning, and the findings could then provide fairly factual information to the researchers (as well as donors) about a multitude of other aspects of the partnerships, without having to measure them. This would offer critical savings in terms of time, resources, and effort, and would lead to less work disruption, when undertaking partnership research, because collaborative ventures usually exhibit multiple facets, display a wide range of perspectives, and include multiple stakeholders, each with a special interest in a particular aspect of the evaluation (El Ansari et al., 2004).
Discussion
Partners working together in a collaborative mode need not be considered homogenous entities. The groups come from different backgrounds, organizations, and cultures. They view the benefits and costs of participating in their partnerships differently (El Ansari and Phillips, 2004), and as the findings of this report have suggested, their opinions about the certainty that their partnerships’ outcomes will be accomplished also vary to different degrees.
Hence, the complexity of each partner needs be recognized, as each generic partner is far from representing a homogenous unit. The partners may not be able to agree quickly on a common course of action (within the entity) necessary for their partnership. Many of them may not even see the partnership as defined in the initiative as a priority. Furthermore, partners in joint working arrangements value miscellaneous and diverse aspects of the partnerships in which they participate.
The first aim of this report was to describe five South African community partnerships for health professions education and a range of their anticipated outcomes. To this end, an overview was provided of each of the partnerships, as well as the collective challenges they faced and their anticipated outcomes. The findings suggested that the two generic stakeholder
groups had similar levels of certainty in 45 percent of the outcomes under investigation. Other studies (Rogers et al., 1993) also found no statistically significant differences in outcomes efficacy between the staff and members of 61 partnerships in the United States. However, for this investigation, as regards the remaining outcomes, the professionals were significantly more cautious in their perceptions that such outcomes would be accomplished.
The second aim was to test the appropriateness of employing generic stakeholder groups in partnership research as opposed to tightly defined specific partner groups. Utilizing more specific stakeholder groups reflected a more precise depiction of the events, which might be concealed by generic grouping analyses. Furthermore, each specific group exhibited an orbit of assertion where the majority of their responses were located. This confirms that partner groups are not homogeneous (El Ansari and Phillips, 2001b), and neither are the individuals who volunteer to participate (Merrell, 2000); rather, they comprise diverse and resourceful member organizations. Hence, methodological issues become important as researchers get involved in the operational tasks of measuring (Gelmon et al., 1998) and the analytical tasks of comparing performance (Mays and Halverson, 2000; El Ansari et al., 2001).
The third aim was to explore whether those groups out of the six specific partners who perceived greater certainty about the outcomes would also experience higher ratings on other related partnership functioning contentment parameters. The findings suggested that the answer to the question is a qualified “yes.” If a particular stakeholder is confident that the anticipated outcomes would be accomplished, then that stakeholder is more likely to be also satisfied with the partnership, committed to its work, feel a sense of ownership, and exhibit high participation and involvement in the partnerships’ activities.
Conclusion
This investigation has confirmed that in partnership settings, employing generic groups could, at times, be more feasible—and indeed might offer its own set of usefulness in drawing an empirical portrait. However, employing tightly defined stakeholder groups holds more promise for a more precise depiction of events. The general impression is that each partner is unique. Hence, the attitude to be created in collaborative interventions is one of a clear understanding that embraces the different origins and aspirations of the stakeholders and recognizes their mutual roles, responsibilities, resources, and limits. Only by paying due attention to their individual value systems and weaving those beliefs into a common vision can the partnership process be advanced.
Acknowledgment
The author would like to thank the Community Partnerships that participated in this initiative.
References
Buse K and Walt G. 2000. Global Public–Private Partnership: Part I—A New Development in Health? Bulletin of the World Health Organization 78(4):549–561.
Carter MR and May J. 1999. Poverty, Livelihood and Class in Rural South Africa. World Development 27(1):1–20.
Crist JD, and Escandon-Dominguez S. 2003. Identifying and Recruiting Mexican American Partners and Sustaining Community Partnerships. Journal of Transcultural Nursing 14(3): 266–271.
Department of Health. 1992. The Health of the Nation. London: HMSO.
El Ansari W. 1999. A Study of the Characteristics, Participant Perceptions and Predictors of Effectiveness in Community Partnerships in Health Personnel Education: The Case of South Africa. University of Wales College, Newport, UK (unpublished doctoral thesis).
El Ansari W. 2000a. Health Improvement Programmes—The Future: Partnerships for Better Health. Report to The Scarman Trust. Birmingham, UK: The Scarman Trust.
El Ansari W. 2000b. Narrowing the Health Gap? Partnerships: Problems and Possibilities. In: Turpin A, Battel-Kirk B, eds. Narrowing the Health Gap. Health Promotion: Working for Social Inclusion, ed. Glasgow, UK: Society of Health Education & Health Promotion Specialists (SHEPS). Pp. 47–51.
El Ansari W. 2002. Community Development and Professional Education in South Africa. In: Mitchell S, ed. Effective Educational Partnerships: Experts, Advocates, and Scouts. Westport, CT: Praeger. Pp. 217–236.
El Ansari W. 2003. Educational Partnerships for Health: Do Stakeholders Perceive Similar Outcomes? Journal of Public Health Management and Practice 9(2):136–156.
El Ansari W and Phillips CJ. 2001a. Empowering Health Care Workers in Africa: Partnerships in Health—Beyond the Rhetoric Towards a Model. Critical Public Health 11(3):231–252.
El Ansari W and Phillips CJ. 2001b. Interprofessional Collaboration: A Stakeholder Approach to Evaluation of Voluntary Participation in Community Partnerships. Journal of Interprofessional Care 15(4):351–368.
El Ansari W and Phillips CJ. 2001c. Partnerships, Community Participation and Intersectoral Collaboration in South Africa. Journal of Interprofessional Care 15(2):119–132.
El Ansari W and Phillips CJ. 2004. The Costs and Benefits of Participants in Community Partnerships. Health Promotion Practice 5(1):35–48.
El Ansari W, Phillips CJ, and Hammick M. 2001. Collaboration and Partnerships: Developing the Evidence Base. Health & Social Care in the Community 9(4):215–227.
El Ansari W, Phillips CJ, and Zwi AB. 2002. Narrowing the Gap Between Academic Professional Wisdom and Community Lay Knowledge: Partnerships in South Africa. Public Health 116(3):151–159.
El Ansari W, Phillips CJ, and Zwi AB. 2004. Collaboration in Health: Public Health Nurses’ Pespectives. Public Health Nursing 21(3):277–286.
Findley SE, Irigoyen M, See D, Sanchez M, Chen S, Sternfels P, and Caesar A. 2003. Community-Provider Partnerships to Reduce Immunization Disparities: Field Report from Northern Manhattan. American Journal of Public Health 93(7):1041-1044.
Gelmon SB, Holland BA, Shinnamon AF, and Morris BA. 1998. Community-Based Education and Service: The HPSISN Experience. Journal of Interprofessional Care 12(3):257–272.
Goede H and El Ansari W. (eds.) (2003). Partnership Work: The Health Service–Community Interface for the Prevention, Care and Treatment of HIV/AIDS. Report of a WHO consultation, 5–6 December 2002, Geneva, Switzerland. [Online]. Available: www.who.int/hiv/pub/prev_care/hivpub43/en/; www.who.int/entity/hiv/pub/prev_care/en/37564_OMS_interieur.pdf.
Gottlieb NH, Brink SG, and Gingiss PL. 1993. Correlates of Coalition Effectiveness the Smoke Free Class of 2000 Program. Health Education Research: Theory & Practice 8(3):375–384.
Gray B. 1989. Collaborating: Finding Common Ground for Multiparty Problems. San Francisco: Jossey-Bass.
Haroon A. 2003. Employers Encouraged to Help Control TB. WHO and the International Labour Organisation Strengthen Public/Private Partnership for Tuberculosis Control. Lancet 361(9375):2135.
Henry RC. 1996. An Update on the Community Partnerships. In: Richards RW, ed. Building Partnerships: Educating Health Professionals for the Communities They Serve. San Francisco: Jossey Bass. Pp. 33–49.
Henry RC. 1996a. Community Partnerships: Going Beyond Curriculum to Change Health Professions Education. Medical Education Online: 1-4. Available at www.msu.edu/~dsolomon/f0000004.pdf [accessed December 8, 2005].
Herman KA, Wolfson M, and Forster JL. 1993. The Evolution, Operation and Future of Minnesota SAFPLAN: A Coalition for Family Planning. Health Education Research: Theory & Practice 8(3):331–344.
Kagan SL. 1991. United We Stand: Collaboration for Child Care and Early Education Services. New York: Teachers College Press.
Kumpfer KL, Turner C, Hopkins R, and Librett J. 1993. Leadership and Team Effectiveness in Community Coalitions for the Prevention of Alcohol and Other Drug Abuse. Health Education Research: Theory & Practice 8(3):359–374.
Levin E, Davey B, Llife S, and Karicha K. 2002. Research Across the Social and Primary Health Care Interface: Methodological Issues and Problems. Research Policy and Planning 20(3):17–31.
Linney JA and Wandersman A. 1991. Prevention Plus III Assessing Alcohol and Other Drug Prevention Programs at the School and Community Level: A Four Step Guide to Useful Program Assessment. Rockville, MD: Office for Substance Abuse Prevention.
Mays G and Halverson P. 2000. Conceptual and Methodological Issues in the Public Health Performance Measurement: Results from a Computer-Assisted Expert Panel Process. Journal of Public Health Management and Practice 6(5):59–65.
Merrell J. 2000. Working with Volunteers in a Community Well-Woman Setting. Community Practitioner 73:466–469.
Michigan State University. 1996. Points of Distinction: A Guidebook for Planning & Evaluating Quality Outreach. East Lansing, MI: Michigan State University.
Morse SS. 2003. Building Academic–Practice Partnerships: The Center for Public Health Preparedness at the Columbia University Mailman School of Public Health, Before and After 9/11. Journal of Public Health Management and Practice 9(5):427–432.
Murnighan JK. 1978. Models of Coalition Behavior: Game Theoretic, Social Psychological, and Political Perspectives. Psychological Bulletin 85(5):1130–1153.
Ngwena C. 2000. The Recognition of Access to Health Care as a Human Right in South Africa: Is It Enough? Health and Human Rights 5(1):26–44.
Northridge ME. 2003. Partnering to Advance Public Health: Making a Difference Through Government, Community, Business, and Academic Vocations. American Journal of Public Health 93(8):1205–1206.
Phillips CJ, Palfrey C, and Thomas P. 1994. Evaluating Health and Social Care. Basingstoke, UK: Macmillan.
Richards RM. 1996. How Public Policy is Shaped. In: Richards RM, ed. Building Partnerships: Educating Health Professionals for the Communities They Serve. San Francisco: Jossey Bass. Pp. 51-67.
Rogers T et al. 1993. Characteristics and Participation Perceptions of Tobacco Control Coalitions in California. Health Education Research: Theory & Practice 8(3):345–357.
Shannon VJ. 1998. Partnerships: The Foundation for Future Success. Canadian Journal of Nursing Administration 11(3):61–76.
Staggenborg S. 1986. Coalition work in the pro-choice movement: Organisational and environmental opportunities and obstacles. Social Problems 33(5):374–390.
Steenbergen G and El Ansari W. 2003. The Power of Partnership. Stop TB Partnership, World Health Organization. Geneva, Switzerland: WHO. WHO/HTM/STB/2003.24. [Online]. Available: www.stoptb.org/documents/WHO-HTM-STB-2003.24-PocketG-2colorsfin.pdf [accessed on December 7, 2005].
UNICEF. 1989. Children on the Front Line. New York: UNICEF.
Waddock SA and Bannister BD. 1991. Correlates of Effectiveness and Partner Satisfaction in Social Partnerships. Journal of Organizational Change Management 4(2):64–79.
WHO (World Health Organisation). 1987. Community-based Education of Health Personnel. Report of a WHO Study Group. Technical Report Series 746. Geneva, Switzerland: WHO.
Zimmerman FJ. 2000. Barriers to Participation of the Poor in South Africa’s Land Distribution. World Development 28(8):1439–1460.
HEALTH PROTECTION: COMMUNICABLE DISEASE, PUBLIC HEALTH AND INFECTION CONTROL EDUCATIONAL PROGRAMMES—A CASE STUDY FROM THE UK
W. El-Ansari and S. Privett
Postgraduate Public Health Programme, School of Health and Social Care, Oxford Brookes University,
Sandringham House, Heritage Gate, Sandy Lane West,
Oxford OX4 6LB, UK
Received 15 December 2003; received in revised form 12 May 2004; accepted 2 June 2004
Published in the Journal of the Royal Institute of Public Health (2005) 19:328-340.
Summary
The health protection (HP) landscape is changing. Issues related to infectious diseases in the context of global health are receiving the attention of world leaders and policy makers. In the UK, the national health policies resonate with such transformations, presenting a range of opportunities and challenges. The opportunities include the formation of a new national organisation dedicated to protecting the people’s health and reducing the impact of infectious disease, the Health Protection Agency. The opportunities also include the opening of non-medical specialists’s pathways in public health. The challenges represent the limited number of centres offering infection control education; the hospital focus and bias of the courses; new, resurgent and emerging infections; globalisation and travel; bacterial resistance; vaccine safety and coverage; bioterrorism; global response capacity; and visa restrictions. Within this context, this paper presents a case study of an HP educational programme at a British university in the south of England. It outlines the course design and philosophy, participants, recruitment, aims, descriptions and learning outcomes. A range of teething problems associated with the initiation and running of such programmes is considered. These include aspects related to the university, features associated with the modules, characteristics of the students, and other interconnected larger scale international issues. Some suggestions for the way forward are presented. Collectively, attention to the suggested measures can ensure that
© 2004 The Royal Institute of Public Health. Published by Elsevier Ltd. All rights reserved.
the processes that teaching programmes embrace to refine their content and delivery will equip tomorrow’s professionals with the requisite HP knowledge and skills.
Introduction
Infectious diseases are a major threat to mankind’s survival, health, wellbeing, prosperity, social stability and security (Chief Medical Officer, 2002). They account for 41% of global disease and are responsible for millions of deaths each year (Chief Medical Officer, 2002). Recent events have put microbial threats and public health into the forefront: “SARS has emphasized that infectious diseases can come out of nowhere” (Lovinger, 2003). Such realities highlight the importance of public health and health protection (HP). Globally, as well as nationally in the UK, there have been emerging opportunities as well as growing challenges on several fronts with regard to HP. Although HP includes communicable disease (CD) control, protection against non-communicable environmental hazards, and emergency planning and response (Regan, 1999), this paper will focus on the first of these: the CD function.
Health Protection: Opportunities
Two major positive developments stand out. First is the publication of a HP strategy for England and the formation of the Health Protection Agency (HPA). The HPA is to deal with the health threats from infectious diseases, chemicals, toxins and radiation hazards. As infectious diseases pose an everchanging risk because the problem is never static, HP is in the premier division of health priorities (Chief Medical Officer, 2002). However, this presents a number of challenges in relation to the development and training of the workforce (Nicoll and Murray, 2002). Second, a medical qualification is no longer a requirement for directors of public health. Non-medical public health specialists’ pathways have been accepted by the UK Faculty of Public Health (Somerville and Cornish, 2001). In the past, there were fewer training opportunities for non-medically qualified workers from many disciplines and professions wishing to work in specialist public health (El Ansari et al, 2003a). As a result of these changes, the preparation for a new cadre of public health professionals is underway. Many students undertaking postgraduate education as an initial component of public health training require instructional courses in recognition, prevention and control of CDs.
Health Protection: Challenges
The range of challenges to HP is broad. Table A-2 depicts some contributory factors that underline the need for HP, considering lifestyle and environmental influences. Health threats include infections transmitted through animals, insects, and food and water, as well as illnesses resulting from environmental toxins, misuse of antibiotics and bioterrorism (King and Khabbaz, 2003).
CDs and infection control have had a low profile in the UK with limited educational opportunities (Pratt et al, 2002). Such training had a strong hospital focus and less regard to the wider community impact (Pratt et al, 2002), despite the fact that care is increasingly provided in the community (McGarry, 2003). Protecting patients with indwelling devices or receiving enteral nutrition, and protecting carers from infections has extended the interest in microbial threats to out-of-hospital care settings (Friedman, 1999).
New and emerging infections have come to the fore. Since the 1970s, about 30 previously unidentified infectious diseases have become important (Chief Medical Officer, 2002; Pennington, 2003), emphasizing the necessity to strengthen the infection control infrastructure. Similarly, the re-appearance of old adversaries such as tuberculosis and syphilis (Public Health Laboratory Service, 2001), as well as opportunistic infections, requires coordinated responses. Likewise, malaria is reappearing, and the influenza pandemic is long overdue.
The effect of globalisation underscores the need for HP. Rapid travel of people, food and other products conveys many infectious agents (Lovinger, 2003). Travellers need to know how to avoid illness, and health professionals need to be able to assess those who return with an illness (Spira, 2003). In parallel, the threats associated with health care are increasing as bacterial resistance to antibiotics continues and hospital-acquired infection remains a concern (Croxson et al, 2003).
Vaccine safety and public expectations emphasise the need for HP (Nicoll and Murray, 2002). Pertussis has re-emerged due to poor efficacy vaccines (Canada, Sweden) (Skrowronski et al, 2002). In the UK, parental confidence in childhood immunization was dented after adverse publicity (Begg et al, 1998). Low vaccination coverage also poses threats (Communicable Disease Report Weekly, 1999), and suggests that measles can be severe and fatal in industrialised countries (Ciofi Degli Atti, 2003). BCG (Dobson, 2002) and Measles Mumps and Rubella (MMR) (Blackwell et al, 2002) vaccination rates among UK asylum seekers were found to be below that required to provide adequate population immunity. Even with high coverage, the threat is not totally avoided. Resurgence of whooping cough was reported in countries with high vaccination coverage (Crowcroft, 2002).
TABLE A-2 The need for health protection: lifestyle and environmental influences
|
Issue |
Example |
|
Travel |
Malaria infections when travelling in warm countries |
|
Trade |
Incidents of food poisoning from imported food (e.g., coconut) |
|
Increasing antibiotic resistance |
MRSA. Vancomycin-resistant Enterococci |
|
Increasing elderly population |
In the UK from 1901 to late 1990s, the population over 65 years of age quadrupled. This is likely to impact on future care as the elderly are more prone to infection |
|
Increasing immature neonates surviving |
Survival of premature/low-birthweight babies has improved. The increase of babies needing invasive devices to provide life support increases the risk of infection |
|
Immunosuppression due to chemotherapy or transplant |
Patients with leukaemia and other immunosuppressive diseases are at higher risk of microbial infections |
|
Immunodeficiency states |
HIV/AIDS |
|
Deforestation and animal movement |
Exposure of workers (arthropods); loss of protective wildlife (predators) who kill rodents. Ebola haemorrhagic fever is believed to have first infected a forest worker clearing trees when bitten by an infected monkey |
|
Global warming |
Has brought floods and droughts. Heavy rain provides breeding sites for malaria and causes flooding, which contaminates clean water supplies |
|
Health care associated infections |
In 1999, it was estimated that healthcare-associated infections cost the NHS almost £1 billion per year |
|
Fear of bioterrorism |
Anthrax scare in the United States and fear of smallpox release |
|
Changes in animal husbandry |
vCJD speculated to be caused by eating beef from cattle with bovine spongiform encephalopathy, believed to be due to feeding animals with animal byproducts |
|
Vaccination |
Meningitis C and Hib vaccinations led to a decrease in numbers of infected individuals |
|
Media hype |
MMR vaccine safety scare (UK) could have contributed to decrease in vaccination take up, increase in infected individuals and concern about outbreaks |
|
Lifestyle changes |
Legionella pnemophila colonises air conditioning systems, inhalation of contaminated aerosols leads to infection |
|
MRSA, methicllin-resistant Staphylococcus aureus; vCJD, new variant Creutzfelt-Jacob disease; Hib, Haemophilus influenza serotype B; MMR, measles, mumps and rubella; HIV, human immunodeficiency virus, AIDS, acquired immunodeficiency syndrome; NHS, National Health Service |
|
Bioterrorism and the release of biological agents necessitate HP. Release of anthrax (United States) as a biological weapon, or the deliberate contamination of restaurants with Salmonella can cause widespread illnesses (Torok, 1997). Such threats are considered to be low in the UK (Lightfoot, 2001), but ricin has been found in London (Mayor, 2003).
Education for CD and infection control has been underdeveloped with no single pattern of provision (Public Health Laboratory Service, 2002). Globally, there are calls to address the deficiencies in this area (Ronald and Memish, 2001). What emerges from the literature and state of affairs is the need for a competent workforce able to respond to microbial threats. A capable workforce must be underpinned by CD prevention and control training programmes (IOM, 2003). Hence knowledge (education) and skills (training) to confront microbial threats will need to be integrated into the preparation of a wide range of health care professionals (El Ansari et al, 2003b) for effective responses to a variety of infections (El Ansari et al, 2003b). Such a task is challenging when, “there is no global definition of ‘infectious diseases’ physicians and cover competency”(Ronald and Memish, 2001:50). Collectively, these ideas formed the basis for the HP educational courses (“CD and public health” and “Infection control in practice” modules) described here, where the focus is on the CD function (Regan, 1999) of HP.
Aim of the Paper
This paper is a study of HP educational developments at the postgraduate programme in Public Health, Oxford Brookes University, UK. The aims of this paper are:
-
to highlight some emergent opportunities as well as growing challenges in relation to HP;
-
to describe an HP educational programme at a British university;
-
to identify the teething problems associated with the initiation and running of such a programme and suggestions for the way forward.
Case Study: Background
This paper employed a case study approach (Yin, 1994). The case is the HP educational programme addressing CD and infection control modules at Oxford Brookes University, UK. The case was selected as it was initiated at the time when HP was receiving international attention and the HPA was being instigated nationally. Hence, there was an opportunity to incorporate the latest recommendations regarding CD, infection control practice and workforce developments for microbial threats into the modules design.
Figure A-2 depicts HP as a triad of international concern, national responsibility and local commitment. It illustrates the temporal interrelationships between these three dimensions in relation to the HP modules described in this paper.
In recognition of the need for HP education, the university sought to develop a training course for health care professionals and infection control nurses. The university was already providing two modules for infection control practitioners. The first, infection control in practice, focused on acute hospital care, and the second is an introduction to clinical microbiology. Recognising the provision of more community-oriented services and the global challenges of microbial threats, it was felt that another new module was required to encompass CD and the problem of infection control in the community.
This view was subsequently supported.
With careful planning, the new module could augment the existing infection control training. However, it would have to meet the needs of both the infection control practitioners (study at Level 3 after qualifying) and those working in public health (usually postgraduate study, Level 4). To satisfy both these learner groups, the new module (CD and public health) was designed to be taken at either Level 3 or 4. Both cohorts attend the same lectures but assessment is different to reflect study at postgraduate level. Students specialising in infection control are encouraged to undertake the set of four modules outlined in Figure A-2. Planning commenced in 1999 and the new module was established as the Chief Medical Officer’s (CMO’s) report was published in January 2002 (Chief Medical Officer, 2002). The report supported the local view that there was a need for “stronger professional education and training programmes” (Chief Medical Officer, 2002:15). This amalgamation of national responsibility and local commitment acted as the driver of the initiative.
Course Design and Philosophy
Modular programmes at the university generally run for 1 day a week for 8 weeks. Two features characterise this HP programme. Firstly, it runs as an intensive 1-week block module (Monday–Friday, 9.00 am–5.30 pm). The rationale was that students would be totally away from their workplace, focusing exclusively on the course, the course work and the required assessments. Students would attend the lectures and would be able to network over break times. Such “block” delivery would enable participants living away from Oxford, and unable to commute each week for 8 weeks, to stay in Oxford for the module’s duration. The second feature is that as collaborative approaches are required to control outbreaks rapidly and efficiently, this is reflected in the variety of university staff and non-
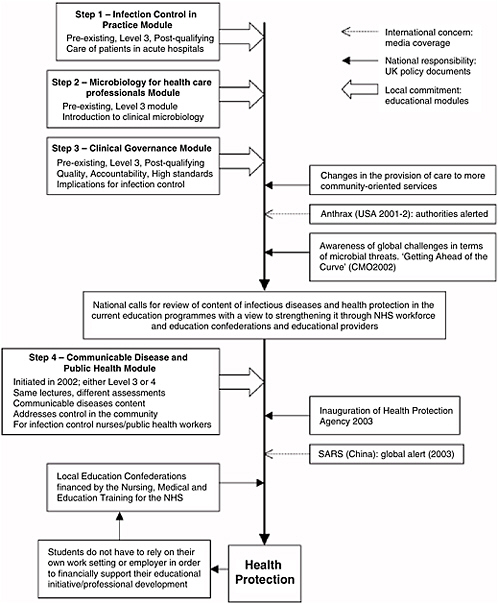
FIGURE A-2 Health protection: temporal relationships between international concerns, national responsibilities and local commitments. *Chief Medical Officer. Getting Ahead of the Curve, a Strategy for Combating Infectious Diseases (including Other Aspects of Health Protection). London: Department of Health, 2002.
university contributors who are involved in the teaching. In practice, CD and infection control cannot be dealt with by one individual, and involving external speakers enhances the student’s appreciation of the roles and responsibilities of others with whom they need to collaborate.
The course philosophy is premised on increasing the student’s knowledge about pertinent topics of CD and infection control. Through planned sessions, participants learn about a range of issues and disease agents, sources of information and risks of exposure, data on safe practices, public safety agencies and avenues for advice. The course also maintains the flexibility to respond to identified individual learning needs. At the start of each module, students are asked to review the programme and identify particular topics that they need to learn about but which are not already included. If it is deemed an appropriate addition, the module team then does its utmost to include such topics in the content. The course is also mindful of relevant incidents and responds by bringing the participants “up to speed” with current global and national events. As anthrax and Severe Acute Respiratory Syndrome (SARS) became international concerns, both were swiftly added to the course content in their respective years.
By using learning sets, the module stimulates students to exchange ideas, share challenges, network and ‘bond’ within the duration of the course. This involves a great deal of interaction between students and presenters. Students work together to plan how they would collaboratively manage incidents such as a food poisoning outbreak or public water supply contamination. Infection control and CD control are ideally suited to this since no single health care professional group has all the responsibility. Management improves when everyone involved acknowledges their duties and recognises the significance of working together. A classroom where the students are removed from their work responsibilities provides an ideal non-threatening forum to debate the multifactorial influences. Such shared learning contributes to establishing future sources of contact, support and expertise between the participants. These connections and relationships could assist the students in identifying and managing future incidents, liaising with experts and working as teams.
Course Participants: Recruitment and Professional Profiles
Recruitment has been good although the university had not advertised this module and its reputation relied entirely on “word of mouth.” In spite of this, at the time of the writing of this paper, it had run three times in 14 months. The first run was immediately after the validation of the module; due to the short notice, there were seven students. With the spread of the news, the number of students quadrupled in each of the subsequent two runs. Interest in the module is high, based on the number of queries that are
received. If such demand is sustained, it might be necessary to run the module twice in the academic year 2003/2004. The students come from a range of backgrounds and disciplines representing many professions. Table A-3 shows the student numbers that attended each of the three “runs” of the course, the range of their professions, the student’s geographical distribution indicating the distance each had to travel in order to attend the course, and some of their feedback as regards their teaching and learning experiences at the university. The diversity of the students’ professional profiles poses challenges to the teaching and learning strategies.
Course Aims, Descriptions and Learning Outcomes
Whilst the course organisers acknowledge that there is no substitute for “hands-on” experience, the modules are designed to enhance knowledge and skills in dealing with microbial threats. In the time available for the modules, the programme does not assume to produce expert practitioners. The modules do, however, inform the learners of frequently encountered pitfalls and provides them with knowledge of how to deal with microbial threats, who to contact and how to utilise the available resources. Upon completion of the modules, students are not expected to be “experts,” but should be safe and informed practitioners with a wealth of information and useful networks of contacts. “The control and prevention of infectious diseases is a responsibility of all healthcare professionals—not just the specialists” (Chief Medical Officer, 2002:142).
The course aims to understanding the methods of spread of infection and implementation of safe practice. Hence, the relationships between the methods of disease spread and the behavioural aspects that influence the outcomes are explored. There is emphasis on communication and collaborative working for productive relationships between the different professional groups. The infection control in practice module focuses on principles of infection control incorporating infectious diseases and epidemiology, both in hospital and community settings. The CD and public health module has a broad public health perspective, and examines the disease epidemiology, trends of emerging infections, surveillance, screening, vaccination, and legal and ethical aspects.
Table A-4 depicts the learning outcomes and session outlines of the HP modules. The two modules examine the systems required to prevent, investigate and control the threat of infectious diseases. In addition to the emphasis on collaboration, they also explore how socioeconomic and cultural factors influence the outcomes of CD control practices. They aim at good surveillance, early assessment and prompt action.
TABLE A-3 Recruitment: student numbers, professions, distance traveled and feedback
|
Professions |
Locations |
Some feedback |
|
First run—seven students |
||
|
3 infection control nurses |
All within 50 miles |
Good venue |
|
2 acute hospital nurses |
Wonderful speakers |
|
|
1 community nurse working with the homeless |
Interesting topics covered |
|
|
1 MPH student |
International student |
Handbook very helpful |
|
Second run—22 students |
||
|
1 acute hospital nurse |
Local |
Overall feedback was good; problem solving gives the opportunity to see what you know in practical situations—good learning exercise |
|
1 health visitor |
Local |
|
|
1 deputy director of PH |
Local |
|
|
1 director of PH |
30 miles |
|
|
1 nursing in general practice hours |
40 miles |
This was an “extra run” put on at the beginning of term-the library were limited which the students did not like |
|
1 nursing officer (PH) |
50 miles |
|
|
1 policy analyst |
120 miles |
|
|
Remaining students either on fast-track PH training or studying for MPH |
Local and international |
[Wanted] more information on the newly emerging HPA; [Wanted] an early finish on the last day |
|
Third run—26 students |
||
|
15 students (Infection Control Award) |
45 miles |
Excellent, lots of information, very interesting; intense, compact; brilliant, lots of information gained, stimulating; thought provoking; high standard of lecturer input, consistently good handouts |
|
2 students taking as a stand-alone module |
Local |
|
|
1 environmental health officer |
35 miles |
Too long; mentally exhausting; very busy, not enough time to absorb information |
|
1 health development manager |
Local |
|
|
3 PH specialists; 1 PH manager; |
Local to 120 miles |
Much better understanding of community health groups and how issues are dealt with |
|
1 PH nurse; 1 assistant director of PH |
|
|
|
PH, public health; MPH, Master’s of Public Health; HPA, Health Protection Agency |
||
TABLE A-4 Health protection modules: some learning outcomes and session outlines
|
|
Infection control in practice |
Communicable disease and public health |
|
Learning outcomesa |
Micro-organisms: spread and interactions |
Biological, socio-economic and environmental factors |
|
Practices and policies of IC |
Prevention and control measures |
|
|
IC for individual clients and the workplace |
Legal and ethical issues |
|
|
Environmental audit and risk management |
Information analysis |
|
|
Evidence-based change |
Disease surveillance |
|
|
Session outlines |
Introduction; history of IC control |
Introduction; history of CD |
|
Handwashing; waste disposal and ward cleaning; sterile supplies department (visit) |
Organisation of the NHS; key workers in CD control; epidemiology; morbidity and mortality; surveillance |
|
|
Specimen collection; disposal of equipment antibiotic resistance; infection control audit |
Groupwork: working in teams; identification of individual learning needs; transmission; decontamination |
|
|
The ventilated patient; untoward incidents; catheter/invasive-devices-related infections; blood-borne infections; managing infection |
Basic microbiology; Public Health Laboratory Services; basic immunology; combating infectious diseases; environmental influences; outbreak investigation |
|
|
Surveillance; meningitis; caring for the deceased Busby box: practical exercises clinical governance; implementing change |
Legal, organisational and ethical aspects of CD control; groupwork; immunity and immunisation; Busby box: preventing/controlling infectious diseases |
|
|
aAdapted from Oxford Brookes University, 2001, 2002. IC, infection control; CD, communicable diseases; NHS, National Health Service |
||
Teething Problems: Considerations for Course Design
The programme team encountered some teething problems during the initiation and running of the HP modules. These included university issues such as the delivery format, classroom accommodation, staffing and administration; module features such as flexibility, and teaching and learning methods; characteristics connected to the students such as the interprofessional background of students, workplace demands and practice links; and international large-scale issues such as the global response capacity and visa restrictions.
Delivery Format
The delivery of a 1-week intensive module meant that students required workplace release for the entire week. Although this can be difficult, the advantages could outweigh the problems. The rationale was that although a week’s release could be more difficult to obtain, the students are able to focus their undivided attention on the course.
Classroom Accommodation
The module delivery is a daily 1-week block rather than the standard format (8 weeks). Securing suitable accommodation when running modules that do not fit the usual university configuration could be tricky. Utilising the same room for the whole delivery week is desirable, as students have considerable workloads, and seeking different rooms each day on an unfamiliar campus is unpleasant. The team found that obtaining the same room for a week was not always simple and early communication with room-booking systems is imperative. It is also important to have conveniently located “breakout” rooms for the groupwork. Running the module outside of the university’s normal timetable meant that the library hours were restricted as were other support services, such as the refectory.
Staffing and Human Resources
A full-time lecturer with CD/public health experience participated in the planning, but had other administrative responsibilities. A part-time lecturer with infection control/CD experience was employed to develop, validate and lead the module, but also had other responsibilities. As the first lecturer left the university, one person remained to run the module. In such circumstances, the quality of the delivery might suffer. However, with the support of colleagues, staff members, and external speakers, the validity of the module has not been compromised (confirmed by stakeholders’/students’
feedback). This highlights the importance of planning for adequate/stable staffing and for having sufficient external support.
Administration
Running the module at two different academic levels represents a difficult enrollment process. It is important to ensure that the students are registered for the correct level. Likewise, admission requirements are difficult to standardise due to the diversity of student’s backgrounds and experiences.
Flexibility
The everchanging nature of microbial threats means that the inclusion of topical issues is critical. The team have kept abreast in identifying relevant national and international microbial incidents and swiftly included them into the curriculum, e.g., foot and mouth disease (UK), SARS (Hong Kong and China) and anthrax (USA). Ongoing “surveillance” of occurrences that represent rich material for discussions and “real-life” platforms for debates is important. Such flexibility has been favourably received by the students.
Teaching and Learning Methods
The team has implemented several strategies to facilitate learning. Students attend lectures and seminars, engage in problem-solving activities, reflect on both their own experience and that of peers, and engage in discussions and debates on a range of issues. Employing such a multipronged approach to learning is a useful tool in maintaining the student’s attention. It has been important to recognise that students come from widely varying professional and educational backgrounds and to provide support and encouragement, ensuring that all views are considered.
Interprofessional Learning
Satisfying the diversity of the student’s backgrounds, and quantity and quality of their professional experience is challenging. However, this diversity is a richness to be capitalised upon, as it is useful in forming networks and appreciation of others’ work and duties. Student learning comes not only from the lecturers, but also from each other’s experiences. For instance, one request was to explore the practical problems of infection control in resource-limited developing countries. A group discussion was greatly enhanced with a presentation by a student with first-hand experience of working in such settings.
Workplace Demands
Some students requested deferral of the dates for submission of their written assignments due to their individual workloads. However, this is challenging since acceptance of work outside of the agreed timetable affects equal opportunity, and disrupts the validation of results and their approval by the external examiner.
Practice Links
The team ensured the involvement of current practitioners from practice areas relevant to both the students and the curriculum. This ensured relevancy to current practice and policy.
Global Response Capacity
Infectious diseases are a global threat requiring global responses, and this needs to be reflected in the curricula. As permeable international borders have replaced the geographic isolation that used to contain disease outbreaks, the curriculum needed to focus on the global burden of disease. Developing countries carry the greatest burden. The team had to make choices about the inclusion of topics that were not very prevalent in the UK but had global relevance. Curricula should develop capacity to monitor/address microbial threats as they arise.
Visa Restrictions
Foreign scientists and academics can encounter problems in gaining access into a country where courses/conferences are running. No such problems have been encountered with the courses described here.
Discussion
In the 1960s, a U.S. Surgeon General, impressed with the rapid progress of antibiotics and vaccines, announced, ‘The time has come to close the book on infectious disease.” As with many predictions of the future, that standpoint was premature (Pennington, 2003). On the other side of the Atlantic, the postwar development of drugs to treat infection led to a view in the 1960s and 1970s that infectious diseases might be conquered (Chief Medical Officer, 2002). Such optimism was also unfounded.
Infectious disease is ubiquitous and persistent with new, emerging and re-emerging infections. Much infection goes unreported or is undernotified, so routine surveillance portrays an incomplete picture of the magnitude and
nature of the threat (Chief Medical Officer, 2002). Prevalence and incidence pyramids are important in infectious diseases; those identified engage only the tips of the pyramids, and surveillance figures are likely to underestimate the real burden (Pennington, 2003).
In the UK, these facts have been realised and responded to by the establishment of the HPA in 2003. The HPA represents a new national organisation, dedicated to protecting health and reducing the impact of infectious disease and other hazards. The prospects now exist for England to have the best HP in the world in 5 years (Nicoll and Murray, 2002). However, accepting that specialised training is not often undertaken (Nicoll and Murray, 2002), the HPA aims to improve knowledge about HP through development, education and training. Consequently, there are calls for a focused educational strategy on CDs and to “review the content of infectious diseases and HP in the current education programmes with a view to strengthening it through NHS workforce and education confederations and educational providers”(Chief Medical Officer, 2002:142).
In response to these calls, this paper focused on the learning and training needs for HP, with attention on infectious diseases. In undertaking this task, the paper employed a holistic, singular case study approach. However, there are many subsections (e.g., philosophy, course organisation, structure, teaching methods, educational and learning outcomes, challenges) that comprise complex domains (Lincoln and Guba, 1985). Hence the contextual details have been outlined in order that readers can judge the relevance of the findings. The paper has detailed the HP educational courses as a component of the postgraduate programme in public health at Oxford Brookes University. Such a “home” for the modules within postgraduate public health is natural given that HP is seen as an integral subspeciality of public health, and basic public health skills (Carlson and El Ansari, 2000) are essential to its delivery (Nicoll and Murray, 2002).
The first aim of the paper was to highlight some emerging opportunities as well as growing challenges in HP. To this end, the paper has discussed some recent advancements that represent opportunities for the HP agenda in the UK. A competent workforce is critical; without it, a public health agency is as useless as a new hospital with no health care workers (Gebbie et al, 2002).
The paper has also shed light on a range of challenges that underline the need for developments in HP. These include the scarcity of infection-control-trained personnel and programmes; traditional hospital focus of infection control educational courses; new, emerging and resurging infections; globalisation and increasing travel; threats associated with health care; vaccine safety and public expectations; and bioterrorism.
These challenges are important as they invite detailed planning, staffing and budgets, as well as integration and implementation. The human
resources for the discipline of infectious diseases are inadequate in many countries (Ronald and Memish, 2001). Strengthening the infrastructure and resources required to address the challenges posed by disease outbreaks is critical (IOM, 2003), but the CMO’s report does not provide detailed implementation strategies (Nicoll and Murray, 2002). While a 2001 survey found “great deficiencies at local level where staffing was surprisingly variable” (Communicable Disease Surveillance Centre, unpublished data), greater use is now being made of non-medical specialists by opening up the opportunities for full membership of the Faculty of Public Health (Frankel, 2003). However, with limited funding, the local level becomes a priority for HP investment (Nicoll and Murray, 2002). Although there is no integrated approach to encompass the aspects of HP from national, to regional, to local level (Nicoll and Murray, 2002), a vision for the future has been proposed.
The second aim of the paper was to describe a HP educational programme that addresses CD and public health and infection control in practice modules. The paper has highlighted the rationale of the modules, their design, recruitment, philosophy and aims, and descriptions of learning outcomes and session outlines. The course philosophy responds to a “seamless service” and collaboration between agencies involved in planning and delivering community services (Glen and Leiba, 2002). Incorporated within the modules is the ability to react quickly to developments and to acknowledge he individual needs of students. In the UK, a recent document reported that the current education provision is failing to meet the needs of practitioners as regards infection prevention in the community (Pratt et al, 2002). This echoes the previous shortcomings and the proposed actions for stronger education and training programmes (Chief Medical Officer, 2002). The necessity of educating and training a microbial threat workforce has been acknowledged (IOM, 2003).
However, the published literature describing infection control and CD education is sparse. In the past, few courses existed in the UK. Hence, this paper did not find much literature with which to contrast its findings or to highlight similarities. However, an important point is that the number of infection control and CD courses around the UK is increasing. For instance, the HPA implements an introductory course in epidemiology and surveillance of infectious diseases, but it is more suitable for public health medicine trainees (Anonymous, 2003). Some institutions provide community/infection control study at Master of Science (MSc), Diploma, or Certificate levels (University of Essex, 2003; UHI Millennium Institute, 2003) which are longer and more demanding levels of study. Similarly, other programmes consist of four modules delivered over four 1-week study blocks (University of Leeds, 2003). Other universities (University of Hertfordshire, 2003) run similar courses but depict very limited information on their websites, are
more focused on the control of infections in hospitals (London School of Hygiene and Tropical Medicine, 2004), or represent courses that seem to be aimed at qualified nurses (London South Bank University, 2004). Yet others incorporate chemical and radioactive hazards (University of Bristol, 2003) or are part of Master’s of Public Health Degrees (Northumbria University, 2004). The courses highlighted here do not represent an exhaustive list of all the courses in the UK.
The range of threats to health is broad and includes international movement, complex food systems, environmental changes, and the wildlife population (King and Khabbaz, 2003). Meeting these challenges and facilitating training of the workforce (IOM, 2003) requires interdisciplinary and collaborative links between human and animal health clinicians, researchers, laboratorians and public health officials (King and Khabbaz, 2003).
As the HPA brings together the expertise of health and scientific professionals working in public health, CDs, emergency planning, infection control and laboratories, so do the modules. The teaching teams include inputs from a range of “external” contributors (former and current consultants in CD control, professor of microbiology, HPA senior member, consultant microbiologist and environmental health officer) and “internal” contributors (the course organiser, a former infection control practitioner and the programme leader, a reader in public health). Such a knowledge matrix is hoped to alert students to the need for partnerships that respect contributions and successful collaborative efforts that span organisational lines (El Ansari, 2003) and professional boundaries (El Ansari, 2001). This concurs with the complexity of infectious disease that requires many disciplines and sectors. Opportunities for synergism are enhanced when disciplines collaborate to discuss the problem, avoid lost opportunities and reduce effort and expense redundancies (IOM, 2003). Recent events highlight the role of partnerships (El Ansari, 2001; El Ansari, 2004) and multi-agency responses (Chief Medical Officer, 2002), as public health prevents disease and promotes health through a growing circle of partners (Steenbergen and El Ansari, 2003; Goede and El Ansari, 2002).
The third aim of the paper was to identify the teething problems associated with the initiation and running of such a programme and to suggest some potential solutions. The paper has reported some factors that could act as threats. These include university- or module-associated issues such as the module’s delivery format and its implications for full-time employed mature students, classroom accommodation, module staffing, and the teaching and learning methods. In education, such issues have received attention (El Ansari et al, 2003; El Ansari, 2002; El Ansari, Pearson, and Davis, 2002).
Another group of challenges involves the student’s characteristics. With diverse backgrounds, experiences and cultures of students, the University
views interprofessional learning as important. Encouraging collaborative learning among culturally diverse students is both advocated and practiced. It is important for the class to move from a cluster of individuals to a working group. Hence students need to have shared understanding of each other’s values, cultures, differences, skills and expertise. Through discussions and deliberations, the module’s designs address the relationship of professional groups to develop appropriate attitudes and motivations for working with others and competencies to practice collaboratively (Glen and Leiba, 2002). Such a weaving of world views of the various professions is desirable (Gebbie et al, 2002), and could contribute to increasing the interaction between professionals of different disciplines. These are important advantages of collaborative education.
A challenge to workforce development is the resources allowing official health agencies to partner the wider circle of public health workers. The courses maintain many links with practice through the invited speakers, planned visits and group debates. Such practice linkages between academic public health and HP agencies, with exchange of faculty and agency professionals, gives students the opportunity to learn from hands-on practitioners (El Ansari et al, 2003a).
Additional challenges represent international large-scale issues such as the global response capacity. Infectious diseases are a leading cause of death and disability in developing countries and are re-emerging as a serious health problem in developed nations. They require global responses (Chief Medical Officer, 2002; IOM, 2003) spanning both the industrialised and developing nations. To an unprecedented extent, infectious diseases in the context of global health are on the agendas of world leaders and health policy makers (Fauci, 2001). For instance, the European Union has plans for its own centre for disease prevention and control (Weiss, 2003).
However, the burden of infectious disease occurs within developing countries where an estimated one in every two people dies from such a disease. Such sentiments will need to be reflected in the curriculum. Global actions from national governments and non-governmental organizations, as well as the professions as regards public health measures, are critical. These could focus on poverty reduction or stepping up immunisation programmes, and on lessening the chances of introducing new diseases
to the dissemination of preventive knowledge and the monitoring of disease outbreaks. Simultaneously, the strengthening of infection control precautions, legislative responses and institution of surveillance all contribute.
In a parallel vein, in the United States, the potentially negative impact of visa restrictions on scientific enterprise has been recognized (Gebbie et al, 2002; White and Peterson, 2003), suggesting that ongoing research (or educational) collaborations have been hampered (Alberts, Wulf, and Fineberg, 2003). Hence, foreign workers with unique skill sets that are not
available in the existing labour pool in a country might require consideration. Although the application of stringent geographical criteria that delay visa clearance of “foreign” scientists are for rigorous applicant screening rather than policies to exclude, the outcomes and impact on research remain unaltered.
Conclusions
Many infectious diseases could be prevented or cured with known public health measures. As part of a wider public health movement, the founding of the HPA was a significant step to addressing microbial-related threats. The World Health Organisation recommendations propose that, in the face of terrorism and emerging infections, a country’s best defence is a high-quality public health service (Gates, 2003). There is an immense need for national and international societies to embrace this specialty. There is also a need to address the deficiencies in this discipline by motivating funding agencies and training institutions to redirect resources to strengthen the health professional’s capacity to deal with infectious diseases adequately throughout the world (Carlson and El Ansari, 2000). It is hoped that the courses described in this paper are a step forward to accomplishing these aims.
Acknowledgements
The authors would like to thank Dr. Richard Mayon-White for constructive comments on earlier drafts of the manuscript.
References
Alberts B, Wulf Wm A, and Fineberg H. 2003. Current Visa Restrictions Interfere with U.S. Science and Engineering Contributions to Important National Needs. The National Academies: Office of News and Public Information. Available at www4.nationalacademies.org/news.nsf/isbn/s12132002?OpenDocument [accessed December 8, 2005].
Anonymous. 2003. Health Protection Agency: Introductory Course in Epidemiology and Surveillance of Infectious Diseases (Advertisement). Public Health News 8 December:16.
Begg N, Ramsay M, White J, and Bozoky Z. 1998. Media Dents Confidence in MMR Vaccine. BMJ 316:561.
Blackwell D, Holden K, and Tregoning D. 2002. An Interim Report of Health Needs Assessment of Asylum Seekers in Sunderland and North Tyneside. Public Health 116:221–226.
Carlson CL and El Ansari W. 2000. Squaring the Circle: Developing Public Health Competencies in Primary Care. Nurs Times Res 5:2–14.
Chief Medical Officer. 2002. Getting Ahead of the Curve, a Strategy for Combating Infectious Diseases (including other aspects of health protection). London:
Ciofi Degli Atti ML, Fabi F, Salmaso S, Pizzuti R, and de Campora E. 2003. Measles Epidemic Attributed to Inadequate Vaccination Coverage, Campania, Italy. MMWR 52: 1044–1047.
Communicable Disease Report Weekly. 1999. MMR Vaccine Coverage Falls in the United Kingdom. (London: Public Health Laboratory Service).
Crowcroft NS and Britto J. 2002. Whooping Cough—A Continuing Problem. BMJ 324:1537–1538.
Croxson B, Allen P, Roberts JA, Archibald K, Crawshaw S, and Taylor L. 2003. The Funding and Organisation of Infection Control in NHS Hospital Trusts: A Study of Infection Control Professionals’ Views. Health Serv Manag Res 16:71–84.
Department of Health; available at www.dh.gov.uk/assetRoot/04/06/03/38/04060338.pdf [accessed December 8, 2005].
Dobson R. 2002. Asylum Seekers Have Low Rates of Vaccination and Screening. BMJ 325:182.
El Ansari W. 2002. Student Nurse Satisfaction Levels with their Courses: Part II—Effects of Academic Variables. Nurse Educ Today 22:171–180.
El Ansari W. 2003. Educational Partnerships for Health: do Stakeholders Perceive Similar Outcomes? J Public Health Manag Prac 9:136–156.
El Ansari W and Phillips CJ. 2001. Interprofessional Collaboration: A Stakeholder Approach to Evaluation of Voluntary Participation in Community Partnerships. J Interprof Care 15:351–368.
El Ansari W and Phillips CJ. 2004. The Costs and Benefits of Participants in Community Partnerships. A Paradox? Health Promot Prac 5:35–548.
El Ansari W, Pearson D, and Davis T. 2002. Satisfaction with Interprofessional Multidisciplinary Education? Influences of Learners’ Demographic and Academic Characteristics. J Interprof Care 16:174–175.
El Ansari W, Russell J, and Wills J. 2003a. Education for Health: Case Studies of Two Multidisciplinary MPH/MSc Public Health Programmes in the UK. Public Health 117:366–76.
El Ansari W, Russell J, Spence W, Ryder E, and Chambers C. 2003b. New Skills for a New Age: Leading the Introduction of Public Health Concepts in Health Care Curricula. Public Health 117:77–87.
Frankel S. 2003. The Faculty of Public Health, and Future Standards in Public Health. http://www.fphm.org.uk/publications_press_and_communications/Publications/March2001phcom/Future_standards_in_publichealth.shtml [Accessed October 12].
Fauci AS. 2001. Infectious Diseases: Considerations for the 21st Century. Clin InfectDis 32:675–685.
Friedman C, Barnette M, Buck AS, Ham R, Harris JA, Hoffman P, Johnson D, Manian F, Nicolle L, Pearson ML, Perl TM, and Solomon SL. 1999. Requirements for Infrastructure and Essential Activities of Infection Control and Epidemiology in Out-of-Hospital Settings: A Consensus Panel Report. Am J Infect Control 27:418–430.
Gates E. 2003. Under a Microscope. Public Health News, November 3. Available at www.publichealthnews.com/features/showcontent.asp?id={73C65DAA-92E2-4BE8-99A5-6C7095DDE7F9} [accessed December 8, 2005].
Gebbie K, Merrill J, and Tilson HH. 2002. The Public Health Workforce. Health Affairs 21:57–67.
Goede H and El Ansari W, editors. 2002. Partnership Work: The Health Service-Community Interface for the Prevention, Care and Treatment of HIV/AIDS. Report of a WHO Consultation, 5–6 December. (Geneva: WHO). Available at www.who.int/entity/hiv/pub/prev_care/en/37564_OMS_interieur.pdf [accessed May 15, 2004].
Glen S and Leiba T, editors. 2002. Multi-Professional Learning for Nurses: Breaking the Boundaries. (Basingstoke, UK: Palgrave).
Institute of Medicine (IOM), the National Academies/Forum on Emerging Infections, Board on Global Health. 2003. Ensuring an Infectious Disease Workforce: Education and Training Needs for the 21st Century,Workshop, 12–13 June, Washington, DC.
King L and Khabbaz R. 2003. Converging Issues in Veterinary and Public Health. Emerg Infect Dis 9:210–1.
Lightfoot N, Wale M, Spencer R, and Nicoll A. 2001. Appropriate Responses to Bioterrorist Threats. BMJ 323:877–878.
Lincoln YS and Guba EG. 1985. Naturalistic Inquiry. (Newbury Park, CA: Sage).
London School of Hygiene and Tropical Medicine. 2004. Diploma in Hospital Infection Control 2004. Available at PERLINK www.lshtm.ac.uk/prospectus/short/shic.html [Accessed May 14, 2004).
London South Bank University. 2004. Diploma in Infection Control Nursing 2004 Available at www.courses.lsbu.ac.uk/undergrad/u3IndCourse.asp?v1Z7&v2Z57&v3Z183 [Accessed May 12, 2004].
Lovinger SP. 2003. Emerging Infections and Bioterrorism Raise Profile of Schools of Public Health. JAMA 290:1306–1307.
Mayor S. 2003. UK Doctors Warned After Ricin Poison Found in Police Raid. BMJ 326:126.
McGarry J. 2003. The Essence of “Community” Within Community Nursing: A District Nursing Pperspective. Health Soc Care Commun 11:423–30.
Nicoll A and Murray V. 2002. Health protection—a strategy and a national agency. Public Health 116:129–137.
Northumbria University. 2004. Master of public health 2004. Available at online. northumbria.ac.uk/prospectus/coursedetailasp?CourseIDZ664 [Accessed May 12, 2004].
Oxford Brookes University. 2001. Infection control in practice. Module handbook. (Oxford: Oxford Brookes University).
Oxford Brookes University. 2002. Communicable diseases and public health. Module handbook. (Oxford: Oxford Brookes University).
Pennington H. 2003. Trends in Infection and Microbial Exposure. Health Hygiene, March: 5–6.
Pratt R, Loveday H, Harper P, Mulhall A, Pellowe C, Howard J, and MacRae E. 2002. Informing the Future: A Review of the Roles and Responsibilities of Community Infection Control and Communicable Disease Control Nurses in England. London: Department of Health and Richard Wells Research Centre.
Public Health Laboratory Service. 2001. Annual Review 1999–2000. Communicable Disease Surveillance Centre, December. Available at www.hpa.org.uk/hpa/publications/publications.htm [accessed December 8, 2005].
Public Health Laboratory Service. 2002. Infection Control in the Community Study. London: Communicable Disease Surveillance Centre.
Regan M. 1999. Health Protection in the Next Millennium: From Tactics to Strategy? J. Epidemiol Commun Health 53:517–518.
Ronald A and Memish Z. 2001. Infectious Diseases: Career Preparation. J Chemother 13(Suppl. 1):50–53.
Skrowronski DM, De Serres G, MacDonald D, Wu W, Shaw C, Macnabb J, Champagne S, Patrick DM, and Halperin SA. 2002. The Changing Age and Seasonal Profile of Pertussis in Canada. J Infect Dis 185:1448–1453.
Somerville L and Cornish Y. 2001. Multidisciplinary Public Health. Available at www.fphm.org.uk/INTERNETPAGES/ph.com-Sept2001.htm.
Spira AM. 2003. Preparing the traveller. Lancet 361:1368–1381.
Steenbergen G and El Ansari W. 2003. The Power of Partnership. WHO/HTM/STB/2003.24. Geneva: WHO. Available at www.stoptb.org/documents/WHO-HTM-STB-2003.24PocketG-2colorsfin.pdf [Accessed May 15, 2004].
Torok TJ, Tauxe RV, Wise RP, Livengood JR, Sokolow R, Mauvais S, Birkness KA, Skeels MR, Horan JM, and Foster LR. 1997. A Large Community Outbreak of Salmonellosis Caused by Intentional Contamination of Restaurant Salad Bars. JAMA 278:389–395.
UHI Millennium Institute. 2003. UHI Course Helps Medical Professionals With Infection Control 2003 www.uhi.ac.uk/news/press/030917professionalsbeatsuperbug.shtm [Accessed December 10, 2003].
University of Bristol. 2003. Department of social medicine. Short Course Programme 2003. Available at www.epi.bris.ac.uk/shortc/shortc.htm [Accessed December 10, 2003].
University of Essex. 2003. MSc community infection control 2003. www.essex.ac.uk/hhs/pg/pgt/msc_cic.htm [Accessed December 10, 2003].
University of Hertfordshire. 2003. Post-Registration Nursing, Infection Control 2003 Available at www.health.herts.ac.uk/depts/postreg/infectionControl/ [Accessed December 10, 2003].
University of Leeds. 2003. The Certificate in Infection Control 2003. Available at www.leeds.ac.uk/healthcare/courses/CPD/Courseinfo/ShortPInfecControl.htm [Accessed December 10, 2003).
Weiss G. 2003. European Union Plans for its Own CDC. Science 301:581.
White WD and Peterson L. 2003. Visas for Visiting Scientists and Students: Current Situation. Physiologist 46:47–50.
Yin R. 1994. Case Study Research: Design and Methods Applied Social Research Methods Series 5. (Thousand Oaks, CA: Sage).
ADDRESSING THE HEALTH WORKFORCE CRISIS IN THE DEVELOPING WORLD
A. Edward Elmendorf, M.A., M.P.H.
World Bank
Washington, D.C.
Data are limited and largely anecdotal on the health workforce crisis in the developing world.3 In considering this issue, it is important to bear in mind the limits of international and developing countries financial and institutional capacity. For example, while the World Bank is the largest external financier of health, nutrition, and population programs in the developing countries, its annual commitments for health in developing countries amount to only around $1 billion, and its work on health involves employment of only about 250 professional staff in Washington, D.C., and around the world. According to one estimate, the United States spends $2.22 per capita per annum on infectious disease epidemiology alone—a figure that may be contrasted with the fact that a number of low-income developing countries, such as Bangladesh, spend about this amount per capita per annum overall on health.
It was proposed at the Institute of Medicine (IOM) Forum that emphasis should be placed on a global perspective in addressing health workforce issues, rather than one of international health. A global perspective might, for example, call for financing of U.S. participation in the fight against polio from U.S. domestic resources devoted to polio prevention and control, rather than from development “assistance” funds. The Millennium Development Goals should be seen as a commitment of the global community, rather than solely as an aspiration. The Severe Acute Respiratory Syndrome (SARS) outbreak made it abundantly clear—if proof still were needed after September 11, 2001—that there are no more walls. A global perspective would see American engagement in health human resources issues of other countries less in terms of our defining the problem and sending American personnel into poor countries to deliver services than in terms of a collaborative effort to solve jointly defined problems. Such a joint problem definition might result in temporary use of American health workers in particular poor countries, but that use would be decided jointly in the context of a collaborative long-term program, involving a wide range of domestic and external stakeholders, for resolution of the country’s human resources for health problems.
|
3 |
For a recent synthesis of available evidence, see Lincoln Chen et al., Human Resources for Health: Overcoming the Crisis (2005), Harvard University Press, available on the web at www.globalhealthtrust.org/Report.html. |
The IOM Forum was warned against the risks of pursuing a parochial, non-global health workforce agenda. The ease with which one could lose a global perspective was illustrated in the case of the American Public Health Association (APHA). While the APHA has assigned itself a global concern, its executive director publicly endorsed a proposal to ease U.S. visa restrictions for foreign medical graduates willing to be deployed in underserved areas of the United States. There seemed to have been no consideration of the impact of such incentives for foreign medical graduates to remain in the United States, from the standpoint of their participation in the foreign and U.S. labor markets. In effect, this reduction of visa restrictions constituted an incentive for developing country health care providers needed critically in their own countries to emigrate to the United States.
Solutions to health workforce issues, whether in developing countries or in the United States, need to take into account the full complexity of the issues and the many stakeholders concerned. Parties that need to be brought to the table include not only ministries of health and others directly responsible for health policies. Also to be included must be ministries and senior academic administrators responsible for higher education (because of their responsibility for universities and medical schools) and for civil service and public employment policies and practices (because such a large share of the health workforce is employed in the public sector), as well as the organized health professions (who have frequently been ignored in developing country policy making). Finally, ministries of finance and treasuries, which hold the purse of public spending, need to be brought into the dialogue.
Internationally, it should not be expected that the World Health Organization alone can handle health workforce issues in their much-needed global context. The World Trade Organization should be involved because of its growing concern with trade in services, which inevitably will include the services of health care personnel. International financial institutions, such as the World Bank and the International Monetary Fund, should be involved because of their engagement with developing country macroeconomic and sectoral policies. The Organisation for Economic Co-operation and Development should have a role because it is deeply involved as a forum for coordination and cooperation on industrial country economic and social policies, including health and labor policies. Bringing all of these actors together internationally, along with their many domestic counterparts, constitutes a formidable challenge. Finally, the work of the Global Commission on International Migration should be brought to bear.4
|
4 |
The Commission presented its report, Migration in an interconnected world: New directions for action, to the UN Secretary-General, UN member states, and other stakeholders on October 5, 2005. Additional information is available at its website: www.gcim.org/en/. |
ENSURING AN ADEQUATE INFECTIOUS DISEASES PHYSICIAN RESPONSE TO EMERGING INFECTIONS
Gary L. Gorby, M.D.
Department of Medical Microbiology and Immunology
Creighton University School of Medicine
Omaha VA Medical Center
Omaha, NE
There is a limited amount of quality data regarding the number of infectious diseases (ID) physicians in the United States or worldwide. So, this report subscribes to the goal of the Health Resources and Services Administration (HRSA) Public Health Work Force Enumeration of 2000 (Gebbie, 2000), which was to arrive at a current best estimate: “the perfect was not allowed to become the enemy of the good.”
Infectious Diseases Physician Training Programs/Status
Table A-5 displays the demographic changes in infectious diseases training programs between 1994 and 2002 (Joiner et al., 1998; Personal communication, A.C. Mucha, Director of Organizational Affairs, Infectious Diseases Society of America, June 2, 2003). During this period, there has been a slight reduction in the number of programs that participate in the national resident matching program, but the overall number of positions offered is about the same now as it was in 1994. The number of filled positions has risen from 60 percent to around 80 percent, and the percentage of positions filled with U.S. graduates has risen from 34.6 percent to 51 percent. Evaluating this latter statistic is somewhat like evaluating a new software product. Viewed from one perspective (national), the trend could be considered a feature, as we are training more ID experts who are United States citizens and likely to remain in this country. However, viewed from another perspective (international), the trend could be considered a “bug.” Emerging infectious disease challenges may appear anywhere on the globe, and a smaller proportion of experts may enter the global community if the trend continues.
Adequacy of Infectious Diseases Training
Within the past decade, there have been two published surveys that addressed the adequacy of ID fellowship training (Slama et al., 2000; Joiner et al., 2001). In 1998, an informal Infectious Disease Society of America (IDSA) survey of all members determined that over 85 percent of ID spe-
TABLE A-5 Infectious diseases fellowships 1994–2002
cialists felt their research, basic science, clinical microbiology, HIV, and clinical infectious disease training was adequate (Slama et al., 2000). However, only 35 percent of them felt that their training in public health was adequate, and less than 31 percent felt that their infection control training was adequate. A more formal survey was done of recent ID fellowship graduates who had passed their infectious diseases board certification between 1992 and 1999 (Joiner et al., 2001). Around 80 percent of the respondents were IDSA members. Findings were similar to the IDSA membership survey in the sense that similar areas of training were felt to be inadequate. For example, only 51 percent of respondents felt that their training in infection control was adequate. Interestingly, 52 percent were providing infection control services in their practice, and about half of these individuals indicated that they were compensated for this activity. Those who were actually providing these infection control services were more confident of their training, as two-thirds of them believed that their fellowship provided them with sufficient skills with which to conduct such work. Ninety-one percent felt that didactic teaching of infection control was a necessary component of fellowship programs. The authors concluded that a Web site-based training program for infection control should be jointly developed by the Infectious Disease Society of America and others, including the Society for Healthcare Epidemiology of America (SHEA), the Association for Professionals in Infection Control and Epidemiology (APIC), and the Centers for Disease Control and Prevention (CDC).
Demographics of IDSA Members
To ensure an adequate infectious diseases workforce, one must first know the nature of existing ID expertise and how their professional effort is distributed. Assuming that roughly four out of five recent fellowship graduates are IDSA members (Joiner et al., 2001), the society’s member demographics hold some validity in estimating these parameters. More than 83 percent of its members belong to the categories of Adult or Pediatric Infectious Diseases, with Internal Medicine being the next most common specialty (see Table A-6). Over 50 percent of members listed patient care as their primary professional activity, and another 22 percent identified with clinical or basic research (see Table A-7). Only a little over 4 percent listed public health or hospital epidemiology as their primary activity (Personal communication, A.C. Mucha, Director of Organizational Affairs, Infectious Diseases Society of America, June 2, 2003). Thus, only a small minority of ID specialists are responsible for formally responding to an emerging infectious disease agent within their jurisdiction or hospital.
TABLE A-6 IDSA Members by Specialty (2003)
|
Specialty |
Percent |
|
Adult ID |
71.55 |
|
Pediatric ID |
12.62 |
|
Internal Medicine |
07.50 |
|
Other |
06.62 |
|
Family Practice |
01.31 |
|
Ob/Gyn |
00.39 |
TABLE A-7 IDSA Members by Professional Activity (2003)
|
Activity |
Percent |
|
Patient Care |
50.30 |
|
Clinical Research |
13.97 |
|
Basic Research |
08.88 |
|
Administration |
08.50 |
|
Teaching/Educ. |
07.35 |
|
Public Health |
04.18 |
|
Hospital Epi. |
02.77 |
|
Clinical Micro. |
02.54 |
|
Other |
01.51 |
Infectious Diseases Job Market
Two studies have examined the infectious diseases job market by evaluating advertisements in widely circulated journals covering internal medicine. Preheim found that the number of advertisements for ID jobs in the New England Journal of Medicine declined significantly from 1990 to 1995. Only a small, and decreasing, minority of positions listed hospital epidemiology or infection control as a major component of the position (Preheim, 1998). A second study by Tice et al. confirmed the earlier study, but found that job opportunities increased 140 percent from 1995 to 2002 (Tice et al., 2002). Most of the increase was in private practice opportunities. This study did not enumerate epidemiology or public health jobs, presumably because they made up a small proportion of the total. The authors also commented that many medical communities do not have a specialist trained in infectious diseases and do not advertise for one. This is an unstudied need. In addition, there is no information on which to rely
regarding changes to the job market since the terrorist events of 2001. In general, it seems reasonable to assume that overall job opportunities in the ID private-practice sector have been increasing.
Infectious Diseases/Public Health Physicians
A survey study by the Council of State and Territorial Epidemiologists conducted in 2001–2002 identified a significant deficiency in infectious disease and all other areas of epidemiology (CSTE, 2003). In 1992, there were about 1,700 “full-time equivalent” positions in epidemiology surveillance. By the time the survey was conducted, this number had decreased to less than 1,400. Of these professionals, 152 were physicians. Ninety-nine of these worked in an infectious disease or bioterrorism (BT) capacity. Most state/territorial epidemiologists reported a shortage of staff and resources. The study concluded that increased capacity was urgently needed. The study argued for increased federal funding in the face of shrinking state budgets, despite the fact that about 60 percent of the funding for epidemiology and surveillance already came from the federal government.
It is even more difficult to measure the job market for public health (PH) physicians. In epidemiology circles, a popular monthly newsletter entitled “Epi Monitor” is the “best resource” for identifying epidemiology jobs (personal communication, A. Mardis, Medical Epidemiologist, Nebraska Health and Human Services System, May 29, 2003). Although they had done no formal enumeration, the newsletter publishers reported a general sense that the number of available jobs had increased. They noted that many positions were being advertised due to turnover and that many recent positions had been reposted because of a lack of qualified applicants.
Resources to Develop Infectious Diseases/Public Health Physician Expertise
Funding sources to develop ID/PH expertise are diverse, with ID fellowships traditionally financed through hospitals, medical schools, and some research training grants. New funding sources to augment ID/PH expertise mainly fall under the guise of bioterrorism preparedness. Two of the largest BT financial resources are the Health Resources and Services Administration and the Centers for Disease Control and Prevention. The HRSA provided $275 million in 2002 and budgeted $542 million in 2003. The CDC provided $918 million in 2002 and $870 million in 2003. In 2000, the CDC established a national system of Centers for Public Health Preparedness, with the purpose of improving the capacity of frontline public health and health care workers to respond to bioterrorism, other infectious diseases outbreaks, and other PH threats and emergencies, primarily
through education and training. There are three types of centers: academic, specialty, and advanced practice sites. Academic centers link schools of public health with state, local, and regional needs. Specialty centers, which are established in colleges or universities, may address unique content, discipline-specific, or technology needs. Advanced practice sites, which have been established in local public health departments, focus on operational readiness, communications, and/or information technology and training applications. Although these resources broadly target ID/PH expertise, they are not specifically designed to increase the ID or PH physician workforce. While the influx of funds for bioterrorism preparedness is welcome, one must recognize that these funds are at risk if the threat of BT is perceived to decrease. As shown by the outbreak of severe acute respiratory syndrome (SARS) and the recent outbreak of monkeypox, Mother Nature can masquerade as a terrorist. So, the enhancement of ID/PH physician expertise is essential regardless of the relative threat of bioterrorism.
Nebraska: An Example of Demand and Change
Nebraska has 93 counties. On September 11, 2001, there were 72 counties that were not covered by local health departments (see Figure A-3). At the time there were 16 health departments that covered the remaining 21 counties. By using tobacco settlement dollars through The Healthcare Funding Act (LB692), Nebraska funded 16 new health districts. To receive the funds, districts had to identify a region that served at least 30,000 individuals. Only one county currently is not part of a local health district (see Figure A-4). Sixteen new districts were formed, and new health directors were hired. A minority of these directors had preexisting public health backgrounds or training, and they were not physicians. Local health district boards have physician membership, but in general they are not trained in infectious diseases or public health (Personal Communication, A. Mardis, Medical Epidemiologist, Nebraska Health and Human Services System, June 6, 2003). Nebraska’s need and response to improve its public health infrastructure anecdotally supports the notion that there is a growing need for ID/PH expertise in the country that has been recognized since September 11, 2001.
Large Private–Public Partnership
As discussed above, there is a relatively small cadre of physicians whose primary function lies in the public health or infection control fields, and there are many other physicians and health care workers whom we rely on to activate a public health or infection control response in the event of an infectious disease outbreak, through passive reporting of unusual events.
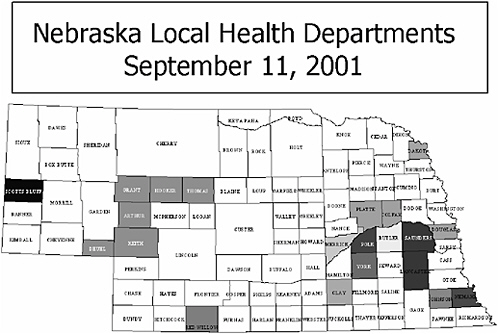
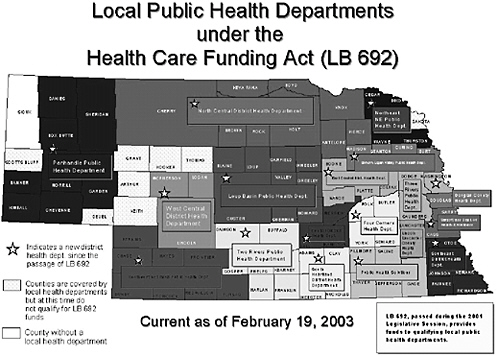
FIGURE A-5 Homunculus illustrating the “small body” of full-time ID/PH physicians.
The situation is somewhat analogous to the concept of a homunculus, which is a man with body parts in proportion to the relative amount of brain substance devoted to innervating each part (see Figure A-5). In this analogy, “official” public health/infection control physicians make up the very small torso of the public health homunculus, while a larger “unofficial” group fulfills the disproportionately large part of the peripheral nervous system of public health functionality as the oversized eyes, ears, nose, hands, etc. These physicians are largely in private practice and are not necessarily ID specialists. Some of them may serve on their local health district boards, yet lack adequate training and knowledge about public health, epidemiology, and infectious diseases. This is not surprising, because even among infectious disease specialists, there is a relative lack of confidence in their own infectious disease epidemiology and infection control training. Together, these unofficial providers are the disproportionately large private part of this critical private–public partnership that makes up the sum total of the nation’s public health response pool. Members of this large private portion have a keen interest in the intended function, but often lack knowledge of public health as a discipline. To function optimally they are in need of formal, practical training.
Deterrents to Infectious Diseases/Public Health Physician Careers
Why don’t more physicians enter careers in infectious diseases and public health? One reason is the significant financial disincentive. The average medical student graduates with a debt of about $100,000 (AAMC Databook, 2002), and public health physicians fall into the low-earner category. According to an American Medical Association (AMA) Physician Marketplace Report from 1996, low earners were those who earned less than the 25th percentile, or $120,000 (AMA, 1997). In 2000, the median net income for general internists was $144,000. According to the IDSA Web site, in 1998 the median salary for ID private practice was $151,000, but starting salaries in academia were around $109,000 (IDSA, 2000). The Council of State and Territorial Epidemiologists (CSTE) survey, which was published 6 years after the AMA study that defined the low earners’ salary mark as $120,000, identified the median salary scale for PH physicians at $87,190 to $120,000 (CSTE, 2003). Clearly, one would find it difficult to choose a career path that would involve additional training for lower wages following the accumulation of a sizeable educational debt. In addition, few students are exposed to an ID/PH career path prior to the accrual of this debt. In general, medical students and residents have a lack of familiarity with PH career options. According to a 1998 Institute of Medicine report, only 56 out of 125 medical schools required courses on public health, epidemiology, or biostatistics. Lastly, the job environment may be a deterrent. Understaffing, limited resources, and relatively frequent turnover of political appointee state chief medical officers may detract from job satisfaction (CSTE, 2003; personal communication, R. Raymond, Chief Medical Officer, Nebraska Health and Human Services System, May 21, 2003). The average term of office for state chief medical officers is about 2.5 years, and only 12 of the current officers have held that position for more than 4 years (personal communication, R. Raymond, Chief Medical Officer, Nebraska Health and Human Services System, May 21, 2003).
Models for Enhanced ID/PH Physician Capacity
There are numerous ways to address the need for enhanced ID/PH physician competence and capacity. Some of the lessons learned from the recent efforts at bolstering bioterrorism preparedness should be applied to the problem of ensuring an adequate infectious diseases workforce both in quantity and quality. As an anecdotal example, the diagram in Figure A-6 depicts the initiatives of the Center for Biopreparedness Education (CBE, 2003). This is a consortium with over 30 members, including codirection by faculty members from both medical schools in Nebraska. It is supported by CDC and HRSA funds provided through the state of Nebraska. The center’s initiatives grew out of a needs and resource assessment, which
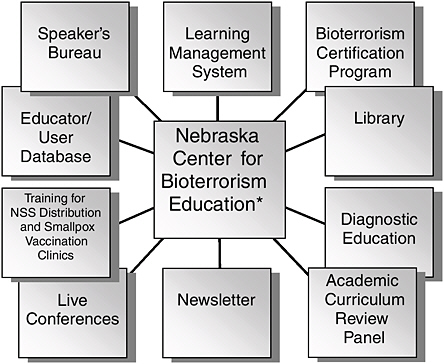
FIGURE A-6 Schematic organization of BT Education Consortium. *Renamed Center for Biopreparedness Education 1/02/2005. NSS, National Strategic Stockpile.
enabled the development of an educator database, in addition to identifying educational needs. A notable feature is the center’s participation in a learning management system. Through this system, users will be able to access distance education courses from any one of the more than 20 participating states. The system will maintain individual user educational profiles while tracking their participation in live on-site conferences or on-line instructional modules. A certification program has been conceived. This certification is not like board certification of medical specialties, but is more analogous to Basic Cardiac Life Support that crosses disciplines. Among the live conferences, the center cosponsors the military-derived Medical Management of Chemical and Biological Casualties Course (Chemcare) and the Medical Effects of Ionizing Radiation Course (MEIR) in a unique joint effort with the Collaborative Training Center at Offut Air Force Base. Participants receive training certificates upon completion of the course. This joint approach enables the development of a database of expertise that can be called on should the need arise, and enables effective integration of civilian and military expertise in an actual event because of similar preparative training. A bioterrorism library with full-time librarian has been established. From this resource, providers across the state can request BT-related
publications in a variety of formats (e.g., hardcopy, video, CD-ROM, electronic document). In addition, a teledermatology system is being implemented to enable distant evaluation of unique visual signs of illness, and academic curriculum review panels are being organized to aid health sciences professional schools to develop appropriate BT curricula. While this consortium is designed for BT education, a similar model could be adapted to enhance the training of the infectious diseases workforce.
Assessment and Recommendations
There clearly is a current demand for more infectious diseases expertise both in the private sector and in an official public health capacity, yet the number of ID fellowship training slots is slightly lower than in 1994. However, the number of slots filled has increased from 60 percent up to 79 percent, with an increasing number of U.S. medical school graduates. If one examines these data from the opposite point of view, more than 20 percent of training slots remain unfilled, despite the increased demand for ID specialists. Clearly, market demand is not having a maximal input on funneling trainees into fellowships. Student awareness of the demand for ID expertise must be raised, and deterrents to an ID/PH career must be eliminated to better utilize existing slots to meet the increased need. Moreover, the ability of experts to respond adequately to emerging infectious disease threats must be augmented through changes in educational curricula and organized response infrastructure. The following challenges must be met to accomplish these goals:
-
About half of ID physicians feel their training provides an inadequate skill set to respond to intentional or natural emerging microbial threats.
-
A very small minority of ID physicians serve in an official capacity in positions whose purpose is to identify and control infectious disease outbreaks.
-
In the past decade, job opportunities for ID physicians have been increasing primarily in the private sector. More recently, positions in the public health sector may have been increasing as well, but the evidence for this is not as well documented.
-
There is an identified need for enhanced infectious disease expertise in state and territorial health departments, but there is high job turnover and a lack of qualified applicants.
-
Major recent funding pools for developing ID/PH physician expertise, which have been in the guise of bioterrorism preparedness and have helped bolster public health infrastructure, also show how the nation’s ID response capacity could be at risk should the perceived risk of bioterrorism diminish.
-
There are significant deterrents to choosing an ID/PH career path, including financial disincentives, inadequate marketing of opportunities to potential trainees, and limited resources within the PH job environment.
-
The current public health system is reliant on the large private portion of the public–private partnership for activating and providing surge capacity for the public health response to emerging infections.
-
The lack of uniform standards for PH certification competency has resulted in a wide variation in the level of public health and private-sector preparedness for emerging infections.
What are some potential solutions to these challenges?
ID training programs need to ensure that formal didactic training in public health, epidemiology, and infection control practices is included in every fellowship experience. This could be accomplished through formal month-long rotations, participation in the SHEA epidemiology course, or participation in a website-based course. For the latter, Joiner et al. suggested that such a program should be jointly developed by IDSA, CDC, SHEA, and APIC. Both basic and advanced components should be included in a modular design (Joiner et al., 2001; Note: since this document was drafted, the IDSA began development on a web-based infection control/epidemiology course). Medical schools also must do a better job of including these topics in their curriculums.
Closer links need to be cultivated between private practice ID physicians and the relatively small group of ID physicians who work full time in an infection control/public health capacity. These links should be grown primarily at the local level and to a lesser degree at the state/territorial health department level to strengthen the necessary “nuts and bolts” local response network. Mechanisms for rapidly educating existing local ID/PH resources need to be developed. Even with best efforts at continuing education, sudden demands for training may arise in unforeseen outbreaks of emerging infectious diseases. The large unofficial private part of the public health workforce needs to be targeted through multimodal training. Novel technologies for on-demand interactive training should be explored. An example of this would be a natural language engine paired with a text-to-speech software application or animated virtual teaching assistant. This type of solution would enable conversation-like interactions of users with a relatively low bandwidth educational website that could be accessed simultaneously by many users (VTA, 2003).
A more formal updated assessment of the recently changed ID/PH job landscape is in order to determine how significant the lack of qualified individuals may be. It is possible that the ID job market in the public health/infection control arena has opened up significantly following the large
influx of funds in 2002 to states and territories for bioterrorism preparedness and the increased importance of hospital response capacity. However, documentation of this is lacking. Moreover, the documented increase in ID private practice opportunities may be siphoning even more ID physicians away from PH careers. It is important to determine how many new positions are being supported by these funds to find out how much of the PH infectious disease response capacity is at risk if this funding were to decrease in the future.
Incentives to encourage individuals to pursue infectious diseases training and careers in public health/infection control activities must be developed. Marketing of PH careers should take place prior to the accumulation of a large educational debt while students are still in an “undifferentiated” career state, because large economic pressures clearly play a role in career choices. An unusual but possible approach to raise public awareness of ID/PH careers might employ “edutainment” venues analogous to recent television series about forensic pathology. However, in this case the programming would be slanted toward the detective work of the epidemiologist. Premed or high school students who were previously unaware of the career path might give some consideration to the option. Forgiveness of educational loan debts for individuals who elect to undergo infectious diseases/public health training would remove a major deterrent to the pursuit of an ID or PH career. In exchange, these individuals would have to agree to work in a PH capacity for several years after their training. One would expect that many of these individuals would remain in the public health field even after their obligation was met.
Consideration should be given to the development of multilevel PH competence certification and the development of a Public Health Medical Reserve Force analogous to military reservists. Such a program would significantly bolster the surge capacity now provided by the large private part of the largely informal public–private partnership that currently exists. The need for this was crystallized by the recent SARS experience in Canada, and the point was driven home by an e-mail sent on June 5, 2003, by W. Michael Scheld, M.D., the president of IDSA. In this message, he solicited the membership on behalf of the Ontario Ministry of Health and Long Term Care to try to find ID physicians who were willing to go to Toronto to help, because the resources of the ID physicians in that city had been stretched to the limit. While well-intentioned people often say they would be willing to help in an emergency, it is extremely important that potential respondents have the right expertise for the problem being encountered and that they actually show up when called on. A Medical Reserve Force that could be formally and selectively activated would have an obligation to respond, thus ensuring an adequate and competent response team. Membership on the Medical Reserve Force should carry an obligation for recurring
training certification for which the reservist would be compensated. As of April 2005, some cities have community-based Medical Reserve Corp (MRC) units that function as a specialized component of Citizen Corps, a national network of volunteers that are organized under the President’s USA Freedom Corps. While this is a step in the right direction, the existing volunteer MRC falls below the level of formal training and mandated obligation to deploy that this document is advocating. Because a serious natural or intentional emerging ID threat would likely involve a response by private, public health, and military medical personnel, it would be wise to develop any PH certification program (and BT certification as well) in concert with the military. This would facilitate effective integration of civilian and military medical responses, because both groups would be operating under the same knowledge base and with the same vocabulary. Levels of certification should be tiered from basic to advanced. Although this solution has been raised in the context of the ID physician, a Public Health Medical Reserve Force and public health certification should not be limited to physician participation only.
References
AAMC Databook. 2002. Washington, DC: Association of American Medical Colleges.
AMA (American Medical Association). 1997. Center for Health Policy Research; Physician Marketplace Report. An Analysis of Physician Net Income: A Comparison of High and Low Earners.
CBE (Center for Biopreparedness Education). 2003. [Online]. Available: www.bioprepare.org/ [accessed January 10, 2005].
CSTE (Council of State and Territorial Epidemiologists). 2003, March. National Assessment of Epidemiologic Capacity in Public Health: Findings and Recommendations. Available: www.cste.org/pdffiles/ecacover1.pdf [accessed December 8, 2005].
Gebbie K. 2000. December. The Public Health Work Force Enumeration 2000. New York: Center for Health Policy, Columbia University School of Nursing.
IDSA (Infectious Diseases Society of America). 2000. Career Opportunities in Infectious Diseases. [Online]. Available: http://www.idsociety.org/PD/IDCareerBrochure.htm [accessed January 10, 2005].
Joiner KA, Dismukes WE, Britigan BE, Cohen MS, Johnson WD, Karchmer AW, Mandell GI, and Stamm WE. 2001. Adequacy of Fellowship Training: Results of a Survey of Recently Graduated Fellows. Clin Infect Dis 32:255-262.
Joiner, KA, Powderly WG, Blaser MJ, Klempner MS, Locksley RM, Mandell GI, Preheim LC, Remington JS, Slama TG, Steigbigel NH, and Bartlett JG. 1998. Fellowship Training in Infectious Diseases: A Report from the Regional and National Meetings of Infectious Diseases Division Chiefs and Program Directors. Clin Infect Dis 26:1060-1065.
Preheim LC. 1998. Career Opportunities for Infectious Diseases Subspecialists. Clin Infect Dis 26:277–281.
Slama TG, Sexton DJ, Ingram CW, Petrak RM, Joseph WP. 2000. Findings of the 1998 Infectious Diseases Society of America Membership Survey. Clin Infect Dis 31:1396-1402.
Tice AD, Strait K, and Tice ACC. 2002. The Market for Infectious Diseases Specialists. Infectious Diseases in Clinical Practice 11:193–197.
VTA (Virtual Teaching Assistant). 2003. Test Site. [Online]. Available: http://gsquared.creighton.edu/smallpoxeval/detectplatform.html [accessed January 10, 2005].
ADDRESSING THE MICROBIAL THREAT TO HEALTH: TRAINING Ph.D. SCIENTISTS TO HELP LEAD THE WAY
Martha L. Gray, Ph.D.
Division of Health Sciences and Technology
Massachusetts Institute of Technology
Harvard University
Cambridge, MA
“The United States has shown leadership in the past by strengthening its own and others’ capacities to deal with infectious diseases, but the present reality nevertheless is that public health and medical communities are inadequately prepared. We must do more to improve our ability to prevent, detect, and control emerging—as well as resurging—microbial threats to health,” notes a 2003 Institute of Medicine report (IOM, 2003). The report goes on to outline the multiple factors, illustrated in Figure A-7, that account for new or enhanced emergence of microbial threats, emphasizing that it is the convergence of one or more of these factors that poses the greatest risks and challenges.
Recognizing the magnitude of the challenge and the fact that dealing with infectious disease threats is going to be an ongoing, evolving challenge for many generations to come, a key issue relates to how we educate the next generation to grapple effectively with the complex social, scientific, environmental, and human factors that conspire to promote the emergence and spread of disease.
Generally speaking, the present educational paradigms provide outstanding grounding in relevant, highly specialized disciplines. And, generally speaking, our nation’s approach to infectious disease has apportioned work and responsibility accordingly to these specialized disciplines, with the physicians serving the primary role of translating and delivering advances in science and technology to the care of patients and to the shaping of public health policies. While these educational strategies should be credited for the dramatic advances in our ability to detect, control, and prevent infectious disease, it is also apparent that they do not presently train individuals to have the broad perspective and context consistent with the complex challenges attendant to the global infectious disease challenges that lay ahead.
In short, the premise here is two-fold: (1) there is a critical need to establish a multidisciplinary, multiprofessional model for graduate training in the area of infectious diseases, and (2) appropriately trained Ph.D. scientists can have a direct role in translating science and technology to advancing our ability to deal with microbial threats to health. Experience with
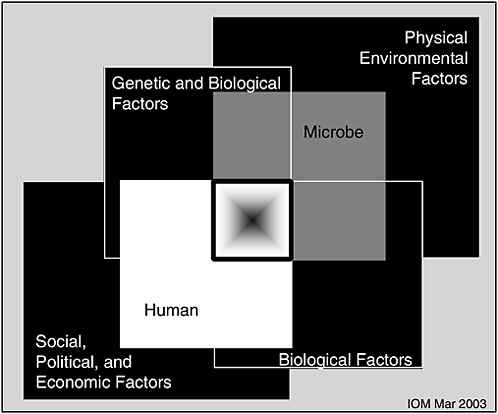
FIGURE A-7 The Convergence Model, illustrating that the microbe-host interaction is influenced by determinants from multiple domains. Each box represents a domain. The center box represents the convergence of factors that could result in a particularly high-risk situation. From the standpoint of education, this convergence model suggests that these multiple domains should be represented (from IOM, 2003).
multidisciplinary, multiprofessional Ph.D. training programs in different biomedical areas clearly illustrates that such training paradigms can be enormously successful and attract exceptional students. The formulation of these training modules recognizes the complex, multidisciplinary factors associated with unmet medical needs (see Figure A-8). Much of this report is therefore devoted to describing these educational models. As one might surmise from the similarity of Figures A-7 and A-8, it should be straightforward, in principle, to adapt these models to establish the kind of training suggested by the complex multifactorial nature of the infectious disease threat.
The notion of multidisciplinary education (or research) in the biomedical arena is one that can generate passionate responses—for and against. Those people opposed typically cite one of two objections: (1) that the
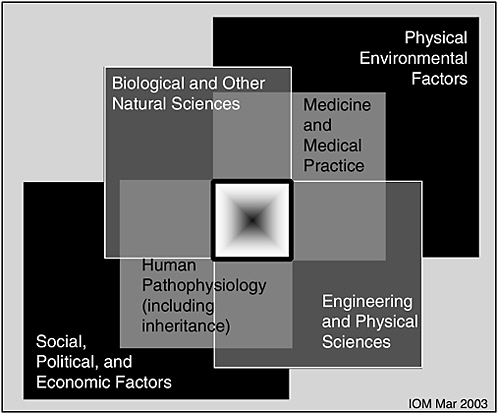
FIGURE A-8 Adapted from the concept of Figure A-7, this diagram illustrates the multiple domains intrinsic to most unmet medical needs. Each box represents a broad domain. The center box represents the convergence of factors that play a role in a health or medical problem, and presumably would play a role in developing a solution. The educational models described here are designed to provide the student with the context and, in some cases, experience, represented by this diagram.
increased breadth incurs an unacceptable loss of depth, and/or (2) why mess with success, as our institutions are very well honed and have a good track record in handing off new biomedical science and technology to the industries that can translate and deliver them to the benefit of humans and human health. The outcome data from the training models described below largely refute those two objections. The argument in favor of multidisciplinary, multiprofessional training in biomedically related areas (including infectious disease) focuses on the following realities:
-
Identifying areas of unmet need requires understanding the multiple associated contexts.
-
Solutions require contributions from multiple disciplines and professions.
-
Solutions are rarely typified by a clean sequence of compartmentalized progress.
-
Organizational structures (and educational programs) are normally unidisciplinary and highly focused on a single facet of an area or problem.
Is it possible to train Ph.D. scientists to increase the likelihood of their impacting infectious disease medicine and public health? And if so, how? Would such training attract the very best scientists? To our knowledge, there is no direct evidence in the specific area of infectious disease. There is, however, increasing evidence from programs that seek to train Ph.D.’s broadly to be at the forefront of advancing clinical medicine. The overarching philosophy of these programs is essentially the same as that for M.D.–Ph.D. training programs; that is, if someone is going to be in a position to translate bench research to the bedside, then that person needs to have substantial training in both domains.
We focus particularly here on two prototypical training models established over the past 15–25 years—models that could be suitably adapted to focus on infectious disease in accordance with the 2003 IOM report (IOM, 2003). We presume here that we have well-established and effective training models for basic biological research, so the issue becomes the mechanism and degree to which we augment that training in light of the realities enumerated above and suggested by Figure A-8. We also include comments about the nature of the training environment, something that we feel to be as important to a successful outcome as the specific curricular components of training.
HST-MEMP Model: In-depth Pathophysiology and Clinical Training for Ph.D. Students
The Harvard–MIT Division of Health Sciences and Technology (HST) was established in 1970 as a joint effort between the Massachusetts Institute of Technology and Harvard University to bring engineering and the physical sciences to biology and medicine. The first academic program that HST offered was a unique M.D. program, steeped in basic science and geared to the education of physician–scientists (Abelmann et al., 1997; Wilkerson and Abelmann, 1993). In 1978, the Medical Engineering Medical Physics (MEMP) Ph.D. program was launched. This program was designed specifically to equip graduate students at the interdisciplinary foci of engineering and the physical sciences and biology and medicine so that the students would be prepared to solve critical problems in medicine. This program was, and remains, unique in providing a clinical experience that is very similar to one that a second- or third-year medical student would have. Central to the mission of this program is the training of Ph.D. scientists
both in their chosen subspecialty of engineering and the physical sciences and in the fundamentals of clinical medicine so that they can identify unmet medical needs and ultimately make contributions that will impact health care. Although MEMP has an engineering and physical science focus, the model is equally applicable to trainees who might have a natural science focus. We describe it in some detail here so that the differences from more traditional Ph.D. training can be appreciated and to aid those who wish to adapt this model to focus on other multidisciplinary educational goals, such as is needed for infectious disease.
The MEMP Ph.D. program carries out its multidisciplinary mission via a flexible structure that permits exploration of all the intersections of those disciplines. Students are jointly admitted by HST and a collaborating department selected from any of the “traditional” engineering or physical science departments at MIT or Harvard. Presently, we accept about 10 percent of applicants, yielding a class of approximately 18–22 students each year (the number has varied from 10 to 22, depending on available fellowship funding). The program accepts students with quantitative backgrounds (usually with undergraduate degrees in engineering or physics) who want to solve problems in human health. We attract people who are very comfortable in multidisciplinary environments and who are eager to have full access to the rich environments of Harvard and MIT (including the teaching hospitals) in deciding on mentors, collaborators, and courses. The applicants also are attracted to the concept of learning and working alongside medical students. The most compelling evidence we have that this program attracts the very best students (beyond the high selectivity) is that HST-MEMP is generally the first choice of our applicants, with more than 75 percent of admitted students selecting this program over others at MIT, Harvard, and other top-ranked institutions.
Depending on their interests and career goals, students follow diverse curricular paths. With guidance from HST and collaborating department faculty, the student begins with an intensive grounding in a subdiscipline of engineering or physical science at MIT or Harvard. The student then passes a doctoral qualifying examination in the collaborating department. At that point, HST becomes the student’s primary institutional association. In addition to their thesis research, students are required to complete seven preclinical courses in one of two tracks: a systems physiology track or a cellular/molecular track. Ph.D. students take these courses with the HST M.D. and M.D.–Ph.D. students, thus providing a rich environment for cross-fertilization between the Ph.D. students and physician–scientist trainees. It should be noted that the content in these courses is structured much like a graduate school subject to include basic science foundations, cuttingedge science, and clinical correlates in recognition of the goals of the students, whether they are pursuing an M.D. or Ph.D. degree, to ultimately
have research as an important part of their career. It should also be noted that most students do not segment their training into the “engineering/physical sciences” piece followed by the medical piece; rather, they integrate some medical subjects early in their training, and may take a few engineering subjects later in their training. Indeed, the semester format of the medical courses permits this kind of integration with regular graduate courses by all HST students (M.D., Ph.D., or M.D.–Ph.D.).
After completing the set of preclinical courses, students then complete a three-part clinical experience over a total of 4 months. This opportunity to participate in clinical training, through coursework with medical students and hands-on experience, is a distinctive hallmark of the MEMP program. The first 6-week period is an intensive introduction to clinical medicine. Students develop skills in patient interviewing and physical examination, become proficient in the organization and communication of clinical information, and work on correlations of clinical issues with basic pathophysiology. Finally, the students become familiar with the multiple components of clinical decision making and the broad economic, ethical, and sociological factors that impact this decision-making process.
In the second 6 weeks, they enhance their clinical skills by working with a hospital ward team in the same manner as would be expected for a third-year medical student. They are directly involved in acute and longitudinal patient care, participate in patient management decisions with the house staff and attending staff, and attend regularly scheduled teaching conferences. Students take call in turn with their fellow students, including night call. They are involved in the assessment and medical management of many common diseases seen on a medical ward, such as chronic obstructive lung disease, atherosclerosis, congestive heart failure, renal failure, and hepatitis, and in this way they are exposed to what is largely adult medicine.
This frontline clinical experience has a profound influence on the student, who comes away from it with an insight into the health care system and how physicians make decisions. Students witness the successes and failures of modern medicine’s diagnostic and therapeutic approaches and often formulate their goals for how their future research can impact individual patient care. Attending physicians often comment that the performance of the Ph.D. students is indistinguishable from third-year M.D. candidates.
A third bout of clinical experience comes later in the Ph.D. training. At this point, the student constructs, with faculty advice, a 1-month preceptorship that is conducted in a clinical environment. In some cases, students use this preceptorship to design or launch a pilot clinical study; in others, they seek to understand the medical management of a particular class of diseases; in still others, they seek to define how an emerging science or technology might impact clinical medicine. The experience involves patient contact, and a term paper is required.
Record of Success
The program works. As described in more detail elsewhere (Gray and Bonventre, 2002; Mark, 2002), outcomes of this HST model for Ph.D. training are very similar to outcomes from M.D.–Ph.D. programs. The total time from matriculation to awarding of the Ph.D. degree has been a mean of 6.1 years—a duration similar to the time-to-degree for most Ph.D. training programs in engineering and physical sciences.
In terms of career choices, of those students who had completed training as of summer 2001, 98 percent have remained in biomedically related careers, with 67 percent in academic positions and 26 percent in business positions. Virtually all of the academic positions are in top-ranked institutions, and they are about evenly split between engineering/physical science departments in a university-based setting and clinical departments in a medical-center setting. Notably, a substantial fraction (36 percent) of graduates in the 1981–1995 cohort are already in influential leadership positions.
Those graduates in academia have been successful in garnering grant support. In a study done in 2001, we found that of our graduates in U.S. academic institutions, 60 percent of those who had graduated before 1990 had currently active grants from the National Institutes of Health (NIH). This compares very favorably to graduates of Medical Scientist Training Program (MSTP)-funded M.D.–Ph.D. programs, where approximately 50 percent of those who received their Ph.D. roughly 10 years prior to the study had ever held an NIH grant (NIGMS Medical Scientist Training Program, 1998). Although we do not have direct comparative data, one would expect only a very small proportion of graduates from engineering programs (e.g., graduates of the departments that collaborate with MEMP) to be supported by the NIH.
The scope of research of our graduates encompasses the spectrum from basic science to clinical research, as reflected by their publications. Although we do not have complete data from all of our alumni, we have ample evidence that MEMP alumni publish in leading basic and clinical journals, with the top 20 including more general publications such as Nature Medicine, Proceedings of the National Academy of Sciences, and Science, as well as specialty publications, such as Circulation and J. Orthopaedic Research, and basic science publications, such as Biophysical Journal (Gray and Bonventre, 2002).
Thus, while MEMP is still a relatively young program, its graduates have been very successful in careers that reflect their training at the boundaries of science, engineering, and clinical medicine. The impact that MEMP grads have had on medicine is more difficult to assess quantitatively. The success in NIH funding tells part of the story. The publication record tells another part. The final part of the story lies in direct evidence of transla-
tion. We do know that at least 17 of the 59 alumni (26 percent) with known positions in the 1981–1995 cohort are directly involved in moving their scientific accomplishments to clinical-level investigation and implementation. This is likely a marked underestimate of the numbers involved in translation. These data clearly support the notion that investigators who do not have an M.D. can, nevertheless, become actively and integrally involved in bringing their discoveries to the bedside. More generally, these data indicate an ability of MEMP graduates to navigate and adapt to changes in biology, engineering, and medicine, identifying and making primary contributions to critical unmet needs. Interestingly, in describing their own successes, MEMP alumni consistently credit the in-depth biomedical and clinical experiences and the multiprofessional community of HST as the most important factors (Mark, 2002).
Targeted Exposure Model: Pathophysiology/Pathobiology Training for Ph.D. Students
An alternative to the HST-type model with in-depth biomedical training model is a targeted exposure model where pathophysiology, pathobiology, or medical concepts are offered to graduate students. This alternative has been used in a variety of training programs for decades. Since their inception in the early 1960s, most formal biomedical engineering (BME) doctoral programs have embraced (patho)physiology as a core requirement. In some cases, such as the program at Johns Hopkins University and the joint program at the University of California, San Francisco, and the University of California, Davis, the required or optional courses are taken together with medical students. However, in many cases the courses are specifically created for BME students and do not include medical students. (A reasonable summary of these curricula can be gleaned from the Whitaker Foundation Web site [www.whitaker.org].) Although most BME programs use a targeted exposure model to provide a medical perspective, to our knowledge the new BME program at Purdue University (where students have a summer clinical internship) is the only one other than HST-MEMP to require both substantial coursework and an extended in-depth clinical experience. It is interesting to note that with the rapid growth in the number of bioengineering programs, some of them are expanding the medical science opportunities while others are moving away from the notion of embracing medical science, in favor of refining (or defining) the discipline of bioengineering—as distinct from the application of engineering to medical problems—and these curricula do not include courses like pathophysiology or pathobiology.
In a somewhat similar but independent trend, several Ph.D. programs in the biological sciences have introduced targeted medically relevant mate-
rial into their curriculum. To our knowledge, the most long-standing of these is the program introduced in 1983 by Irwin Arias at Tufts University, in which selected Ph.D. students take a one-semester subject in pathobiology, in which they interact with patients, handle pathological specimens, and see major diagnostic and therapeutic facilities, as a basis for delving into pathobiological mechanisms (Arias, 1989). Washington University launched a similar program in 1992 in which students have a two-semester experience in human pathology that focuses on the clinical and basic science aspects of important disease states. In addition, the interactions initiated in the course are sustained through a clinical mentor program that continues throughout the graduate experience. We are aware of a number of other relatively brief efforts to address this need and the substantial student interest in biomedical training; many of these efforts were abandoned due to lack of funds. At Harvard Medical School, in the late 1970s Morris Karnovsky offered a pathobiology course that served roughly 50 Boston-area graduate students. In 1992, this effort was renewed in a more extended format. Sixteen students each year were selected after admission to the Division of Medical Sciences. These students took a number of preclinical courses with the Harvard medical students, and they had regular visits to hospitals where they would meet with investigators doing research at the interface of basic science and clinical medicine, talk with patients, and see clinical procedures (Bunn and Casey, 1995). Eight programs were funded between 1992 and 1996 by the Markey Charitable Trust to enhance the knowledge of clinical medicine of Ph.D. students through one or more additional courses (NRC, 2004). Each of these programs appears to be viewed as extremely attractive and successful by their students, but the only program for which outcome data are known to be available is the one at Tufts University (Arias, 2002), where, in particular, career decisions were appreciably influenced, with substantially more participants selecting academic positions, especially in medical centers, compared with the otherwise-similar graduate cohort reported in the MSTP study (NIGMS Medical Scientist Training Program, 1998).
Application to Future Ph.D. Training in Infectious Disease
Several key conclusions can be drawn from these graduate programs with experiences in medical science. These programs attract exceptional candidates and are consistently oversubscribed. Although outcome data are incomplete, alumni of these programs are overwhelmingly retained and are successful in biomedical careers, and many are in positions where they can connect with the patient-care enterprise during the course of their research and thus have the potential to create a vibrant link between the clinic and basic research. That is, they appear to be bridging the traditional gap
between basic science (and engineering) and medicine, an objective that attracted them to these special training programs and a success for which alumni credit their training program as having laid the foundation. Anecdotally, what draws these exceptional students to these programs is an excitement about the problem domain—problems that are challenging, important to the human endeavor, and for which solutions have enormous implications. Certainly the problem domain encompassed by the global infectious disease challenge shares all of those attributes, and so, if framed in the large context typified by Figure A-7, could be expected to attract exceptional talent.
In framing the training program as typified by Figure A-7 (or Figure A-8), it is worth emphasizing the fundamental difference between these training approaches and the more classical approaches. What in particular has distinguished the HST graduate (and medical) training programs is that there is adequate flexibility for students to establish a broad and deep background in their field of interest, and, in addition, to have substantial experiences in both research and clinical practice within a multiprofessional training community where they develop knowledge and social networks. Consequently, students come to understand and appreciate the domain knowledge, the culture, and the value systems of both biomedical discovery and medicine. By getting the “best of both worlds” (without getting separate degrees in both), graduates are well positioned to create scientific and technological innovation, since they can more easily identify the important needs and establish the path for translation from concept to implementation. The contrast between this approach and the more traditional approaches is considerable. Generally speaking, the more traditional training programs exist in uniprofessional communities, have highly specified core curricula, and have limited multidisciplinary experiences. Although these traditional training programs have been undeniably successful in many respects, they satisfy only part of the training need suggested by Figures A-7 and A-8.
In applying the principles underlying the HST-type training model (or the targeted exposure model) to a focus on infectious disease, we offer the following guide:
-
Establish the overarching goal of the training effort.
-
Begin with the best elements of traditional programs.
-
Splice those elements together by establishing a few multidisciplinary courses or experiences.
-
Ensure trainees have an opportunity for hands-on, real-world learning outside the core areas of expertise.
-
Absolutely ensure students become part of a vibrant multidisciplinary/multiprofessional community.
This implementation strategy is one that can create an informed workforce now and can evolve naturally and appropriately over time.
The principle implementation challenges relate to establishing a truly multiprofessional community and to “institutionalizing” a program that cuts across the classical organizational structures. As an aid to overcoming those challenges, we offer here several important “lessons learned” that are not obvious and that we have learned, in part, through trial and error.
First, exposing students to human disease through direct interactions with patients is extremely important. This can happen in a more passive fashion, such as by bringing patients into classes in graduate courses, or more actively by bringing students to the clinical setting. Such experiences lack the power of a period of total immersion in the clinical milieu, but in our experience certainly have had positive effects in decreasing the gulf between the bench and the bedside.
Second, having both M.D. and Ph.D. students together in the same course helps all students to better appreciate the vastly different cultures encompassing the practice of medicine and the practice of science.
Third, there are benefits to teaching graduate students clinical medicine and medical science in the same way that one teaches medical students. In other words, it is not necessary (and is, in fact, not desirable) to ask instructors to modify what and how they teach to accommodate the fact that these students are not medical students.
Fourth, as any student making the transition from preclinical to clinical work will attest, there is a world of difference between learning something in the classroom and having to implement it on the wards. The opportunities, limitations, and constraints of the clinical environment are far more difficult to appreciate by students who have not had to function in that environment.
Finally, one of the most important lessons has come through our organizational structure. We have had the benefit of training M.D.’s, Ph.D.’s, and M.D.–Ph.D.’s—with about 120 of each enrolled at any given time—under the auspices of a single academic unit. By contrast, M.D. and Ph.D. students are usually in wholly separate departments and even institutions, and there are many pressures to maintain that segregation. This multidisciplinary, multiprofessional organization greatly reduces the inevitable barriers that exist between departments and institutions and helps students and faculty to better understand the value system, perspectives, and key questions of each other—and it is this understanding that forms the foundation for the necessarily collaborative work that is required to bring the proverbial bench to the bedside. Furthermore, by electing not to create a virtual construct, but instead by formally establishing a multidisciplinary, multiprofessional organization comprised of students, faculty, and admin-
istrative infrastructure, it becomes easier to resist the inevitable pulls and pushes that aim to make these programs “fit” and seek to elevate one domain in favor of another domain.
The value in undertaking the considerable effort involved in establishing and maintaining such training programs and the associated organizational structure lies in the significant impact that graduates are likely to have on infectious disease. The documented success of both the HST-type in-depth model and the targeted model supports our contention that such training could have comparable success in the infectious disease domain. Furthermore, there is increasing evidence that part of the scientific and technological innovation process requires a sharing and translation of knowledge from one domain to another (Grant, 1996; Hanson, 2002; Hargadon and Sutton, 1997; Sole and Edmondson, 2002). It is not clear how individuals learn to build such communities and to identify and access needed domain knowledge, but it is reasonable to assume that there are advantages to training programs that explicitly place the students in such multidisciplinary, multiprofessional communities.
In summary, outcome data from the in-depth HST-type and targeted exposure training models provide compelling evidence that Ph.D. scientists can play a huge role in advancing clinical medicine. Given the similar complexity of the infectious disease problem domain, it is reasonable to believe that such training models can be and should be implemented to train the infectious disease workforce of the future. The magnitude of the infectious disease problem requires a renewed commitment to education (IOM, 2003). The multidisciplinary, multiprofessional training models described here offer a principled approach to creating training programs in infectious diseases to build a cadre of individuals who have a deep appreciation of the complex multifactorial (multidisciplinary and multiprofessional) issues that conspire to make infectious disease a continuing burden around the world. Furthermore, these training models create “adaptive experts” who can lead change by adapting to the myriad advances and changes in science, technology, and the world.
Thus, in view of the importance of the infectious disease threat, and the reality that addressing the infectious disease threat will involve multiple disciplines and professions, coupled with compelling data indicating that multidisciplinary, multiprofessional educational approaches can be very successful and tend to attract the very best people, it is time for a deep commitment to train the next generation of infectious disease specialists positioned to take the lead in improving our ability to prevent and control microbial threats to health.
References
Abelmann WH, Nave BD, and Wilkerson L. 1997. Generation of physician-scientists manpower: A follow-up study of the first 294 graduates of the Harvard-MIT Program of Health Sciences and Technology. J Investigative Medicine 45:272–275.
Arias IM. 1989. Training basic scientists to bridge the gap between basic science and its application to human disease. N Engl J Med 321:972–974.
Arias I. 2000. Bridge Building between Medicine and Basic Science. National Research Council. Washington, DC: National Academy Press.
Bunn HF and Casey CG. 1995. Educating the biomedical scientist. FASEB J 9:1392–1395.
Grant R. 1996. Prospering in dynamically competitive environments: Organizational capability as knowledge integration. Organization Science 7:375–387.
Gray ML, and Bonventre JV. 2002. Training Ph.D. researchers to translate science to clinical medicine: Closing the gap from the other side. Nature Med 8:433–436.
Hanson MT. 2002. Knowledge networks: Explaining effective knowledge sharing in multiunit companies. Organization Science 13:232–248.
Hargadon A and Sutton R. 1997. Technology brokering and innovation in a product development firm. Administrative Science Quarterly 42:716–749.
IOM (Institute of Medicine). 2003. Microbial Threats to Health: Emergence, Detection, and Response. Washington, DC: The National Academies Press.
Mark RG. 2002. Evaluation of the medical engineering and medical physics doctoral program. In: Abelman WH, ed. The Harvard-MIT Division of Health Sciences and Technology: The First 25 Years 1970–1995. Cambridge, MA: Harvard University Press.
National Research Council. 2004. Bridging the Bed-Bench Gap: Contributions of the Markey Trust. Report of the Committee on the Evaluation of the Lucille P. Markey Charitable Trust Programs in Biomedical Sciences. Washington, DC: The National Academies Press. Available at www.books.nap.edu/catalog/10920.html [accessed May 30, 2005].
NIGMS Medical Scientist Training Program. 1998. The Careers and Professional Activities of Graduates of the NIGMS Medical Scientist Training Program. Bethesda: NIGMS. [Online]. Available: www.nigms.nih.gov/news/reports/mstpstudy/mstp-print.html [accessed December 8, 2005].
Sole D and Edmondson A. 2002. Bridging knowledge gaps: Learning in geographically dispersed crossfunctional teams. In: Choo CW, and Bontis N, eds. Strategic Management of Intellectual Capital and Organizational Knowledge. New York: Oxford University Press.
Wilkerson L and Abelmann WH. 1993. Producing physician–scientists: A survey of graduates from the Harvard-MIT Program in Health Sciences and Technology. Academic Medicine 68:214–218.
WHAT KINDS OF SCIENTISTS DO WE NEED TO TRAIN, AND HOW?
Victoria McGovern, Ph.D.
Burroughs Wellcome Fund
Research Triangle Park, North Carolina
We are moving into a future that incorporates a more systematic view of infectious disease—a future in which, as Joshua Lederberg has said, we consider the life and times of the microbiome, the system of organisms that live within and upon us, rather than focusing on any “war” between “us” and “them.” This shift already is changing, and will continue to change, who infectious disease researchers work with at the bench, who they talk to, and who they train. Now is the time for considering what kinds of thinkers we need to be attracting to this field, and about how we invite and integrate new people into our research culture.
Doing this brings us to the intersection of two large issues: how the scientific boundaries of the infectious diseases are changing, and how the workforce is changing. This report will first share some insights from a recent Banbury Conference that asked, how can we move toward a more unified understanding of infectious disease? Who do we need at the table? How can we lower barriers that keep fields apart? How can we bring critical fields together in hopes that we can move ahead, farther and faster, toward understanding the bones of the problem of how the creatures in, among, and around us live, and harm us, and help us. After laying out those ideas, this report will switch gears to talk not about who does research but about how we train those people. Is the Ph.D. degree the best model? For some scientific work, yes, but for many of the tasks at hand, no.
Bringing new approaches into the infectious diseases will require:
-
Bringing people (and ideas) together better.
-
Valuing emerging fields.
-
Protecting the time and promotability of the people who do it.
Anthony Fauci’s early 2001 “roadmap” paper discussed the need to bring new kinds of expertise into the study of infectious disease. He highlighted the need for expertise in genomics and proteomics, which will have many applications in our field. Synthetic chemistry and mathematical modeling need to be brought in, especially for drug design. Epidemiological approaches, both at the molecular and macro levels, will be more and more important. Also, there is a need to draw in people with skills for developing robotics and high-throughput approaches. And we need experts in informa-
TABLE A-8 Science base for infectious diseases research in 21st century
|
Field |
Research applications |
|
Genomics and proteomics |
Host immunity Diagnostics New drug targets Vaccines Drug resistance Pathogenesis |
|
Synthetic chemistry/robotics |
Drug design High-throughput screening |
|
Computer/mathematical modeling |
Drug design Predictive models of transmission |
|
Molecular epidemiology |
Pathogen virulence Transmission patterns |
|
Genetic epidemiology |
Host susceptibility |
|
Information technology |
All encompassing |
tion technology—people whose skills are in demand not only across the life sciences but across the whole of the economic and intellectual spectrum (see Table A-8).
Physical, computational, and mathematical approaches to life science research are only going to become more important as the field turns rich new data toward application. As a field, we need to be recruiting people with appropriately numerate backgrounds, not only from other kinds of attractive life science areas, but also from the many areas outside of human health where they could turn their attention. At the same time, we need to do a better job of pulling people in from other traditional life science disciplines if we are going to understand how we and our microbes interact, and especially if we are to understand how, why, and when a given bug becomes a “pathogen,” causing disease, rather than living quietly near us, a microbial face in the crowd.
Infectious disease research needs to attract immunology back into its microbiology roots. The field needs insights, language, and people from ecology, evolution, and development to lay the groundwork for understanding the human–microbe interface. And the researchers focusing on human diseases need to look, closer and more often, at plant biology, at the infectious diseases of plants, and at that rich literature of those fields, as well as at veterinary science.
TABLE A-9 Mechanisms to promote more productive interactions at the interfaces between fields
|
Mechanism |
Advantages |
|
Convening Activities |
Enhance local collaboration and help build nearby peer connections; advance integrated approaches; provide opportunities for cross-talk among pathogen systems, scientific approaches, or fields. |
|
Training and Retraining: Courses, Sabbaticals, and Level-Peer Mentoring |
Bring groups of scientists to a common level of competency in a field or approach; help spread new ideas and competencies. |
|
Network Development |
Provide mechanism for focusing on defined problems; attract targeted expertise to the field. |
|
Support of “No points” Science |
Encourage more directed development of critical tools; provide a safety net for those opening new systems. |
There are so many ways of doing science that would be remarkable additions to the field: pages could be spent on listing them. The hurdle is not pointing at the science that needs to be brought in to the infectious diseases, but the practical matter of doing it. How can we promote greater and more productive interactions at the interfaces between fields (see Table A-9)?
Locally, there are seminars, and series of them. Researchers could interact better in their own backyards by using these venues to bring a department or mixed group up to a common speed on new approaches. Crossing departments or crossing colleges—bringing together researchers from medicine, engineering, or agricultural schools within a university—would certainly stir in new ideas. There are plenty of ways to use meetings to reach the goal of finding more unified ways of looking at disease. The Midwest Microbial Pathogenesis meeting is an excellent example of how to do it. This is an excellent but regional meeting that mixes researchers—and, importantly, mixes many young scientists, from across the spectrum of disease. Keystone meetings, the American Society of Microbiology small meetings office’s conferences, and other existing venues are places where there are straightforward ways to build excellent small meetings in the kind of intimate conditions where new perspectives can be mixed together and let to stew.
From these kinds of events, which nucleate researchers around problems, you can start to build networks, and when funders get involved in building and supporting networks, as the MacArthur Foundation has in vector biology, the effects can be dramatic. That kind of problem-focus can do great things. Another approach is to try to identify the people who will be leading the field in a decade or two, and to build networks to bring them along faster, an approach that the Burroughs Wellcome Fund, the Life Sciences Research Foundation, the Searle Scholars program, and others have taken.
While we are on funders, there is what Nina Agabian has called “no points” science—the thankless scientific exploration that opens fields. Too often, funders do not have the right mechanisms in place to encourage the high-effort, low-yield work needed to break a system open. Researchers work on critical tool development with support and time cribbed here and there, and proposals for discovery science, the critical early steps into new directions, are devalued as “fishing expeditions.” Funders need to fix this. We need to encourage risk and to reward skilled and serious pioneers. We should demonstrate clearly to the communities we serve—especially the academic world—that this kind of work is important and should be graded high in both the research and service categories at tenure time.
We need to encourage the spread and cross-pollination of knowledge. Training courses and workshops work. They bring a cadre of people together, inoculate them with a shared knowledge, frame new ways of thinking about that knowledge, and then turn them loose on the world to spread it. Courses are aimed, usually, at young researchers—students and postdocs. Sabbaticals and lateral mentoring can spread ideas across the more senior population. But in both course and sabbatical support there is a funding gap that needs to be addressed.
The professional societies concerned with infectious diseases—the American Society of Microbiology, the Infectious Disease Society of America, and several others—are important parts of the field’s infrastructure and have roles to play in bringing in new approaches. Their oldest and most central roles are convening researchers and publishing journals. Societies can give new ideas and new connections a boost by playing a part in bringing people together around emerging issues. More importantly, through their publishing operations they help define the field. Their publishing choices can give a kind of imprimatur that legitimizes, enhances, and encourages nascent approaches to the scientific problems that hold their organizations together.
Finally, universities need to prepare themselves for the coming wave of more connected, more collaborative science. They have to value good work, even when that work is team driven. The tenure system is a huge barrier to young scientists’ reaching out. Universities should value this kind of work
and actively support it by protecting time for it and making resources available when strong faculty want to move in new directions.
Looking at a related issue, the scientific workforce, in general, and how it is trained, we need to understand what kind of workers are needed at the bench and how we can best train them. An obvious place to start is to ask, “Is there a problem, or are we already doing what we should?”
The RAND Corporation recently released a report titled “Is There a Shortage of Scientists and Engineers? How Would We Know?” The answer to the first question depends, according to the report, on what “shortage” means. When we ask if there is a scientist shortage, we could be asking any of a number of questions: Are we making fewer scientists than before? Are our competitors getting more of their scientists into the marketplace? Do the producers of scientists want to make more scientists? Are we under-supplying the nation’s needs? Is the lack of production driving up the cost of hiring scientists?
The first four problems—if they are, indeed, problems—can be addressed by changing the number of scientists produced and put into the system. But the fifth is self-solving: “if you pay them, they will come” is a principle that has been demonstrated over and over again in labor markets. The salaries expected by our finishing graduate students are not skyrocketing. Although postdoctoral salaries are increasing, they are rising because of changes imposed by funding agencies, such as the National Institutes of Health (NIH), and they are increasing to levels that stem despair. The entering salaries of trained scientists are not rising to levels that will encourage our best and brightest 18-year-olds to focus on research as a career rather than choose other, higher paying, intellectually challenging professions.
There is more to life than money, of course, but early career scientists, those in training, in graduate school, and postdoctoral positions, defer more than earning while they train. They put off building other important stabilizers of happiness, health, and wealth, such as starting families, buying homes, and saving for retirement. It is taking longer and longer to get through the system. A 6-year Ph.D. was the norm 30 years ago, turning out new Ph.D.’s at an average age of 29.5 years. Now, the average new Ph.D.’s are 32 years old, finishing up their degrees in 8 years (see Figure A-9). This is very discouraging to people entering the system. And on top of this, the period spent in postdoctoral work is getting longer as well, but that is not as easy to quantitate because postdocs are not as well tracked as graduate students.
A 35-year-old should have his or her career well launched. In most of the fields that compete with science for bright young people, a 35-year-old is professionally mature. But if we look at NIH grant dollars, it is clear this is not true in health science research (see Figure A-10). Twenty years ago, young people comprised 20 percent of the grant pool. Today, they com-
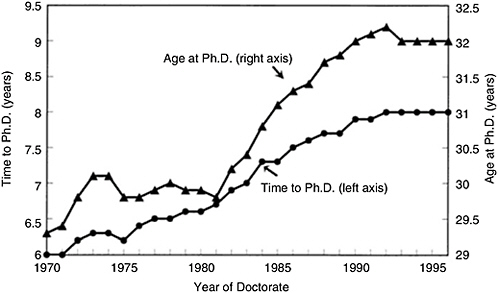
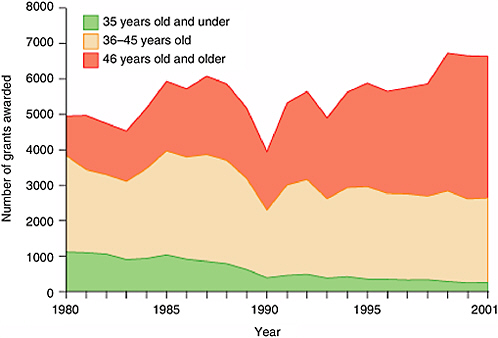
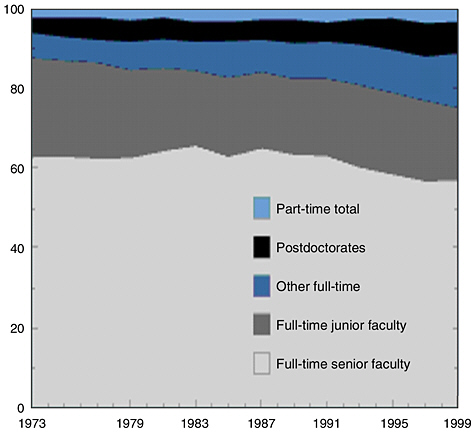
FIGURE A-11 More researchers are in non-faculty academic jobs.
SOURCE: Derived from Science and Engineering Indicators 2002.
prise less than 5 percent—and worse in clinical research. Why? It is not that we discriminate against the young. The bigger factor is that they are just not in the pool of researchers in a position to submit grants. So we are getting top-heavy, with more of our dollars in older people, while our “new blood,” our young researchers, are left in an extended professional adolescence.
Thirty years ago, about 10 percent of the people in the system were postdocs or in other positions where they were fully trained but not yet stable (see Figure A-11). That population had more than doubled by the end of the century, largely because of growth in non-postdoctoral, non-tenure-track, non-stable research-track positions. As the young crowd into these unstable positions, the professoriate is graying. Reaping the intellectual and material rewards of independent science is less and less a young person’s game.
The numbers are discouraging to us, the people already in the system.
But how much more discouraging they are to the 15-year-old who has just caught the excitement that brought us into this field, or to the 19-year-old premed who is driven toward a career bridging the bench and the clinic. These numbers are not hidden from students. Increasingly, American students vote with their feet. They are lost to us.
But we need them. And science is bigger than academe. Industry needs people. And there may be problems coming if we cannot get enough scientific workers abroad, as we have been able to do so far.
Industry does not necessarily need the same things as academe. In academic science, innovation is the big thing, and producing one’s first important, innovative work is the centerpiece of the Ph.D. Industry needs innovation. But companies also need praxis. Industry is driven by people who go in and get the job done. Companies need team players with multi-valent skills.
RAND suggests, then, creating a “professional doctorate,” akin to the way medical schools train a cadre of people to readiness for practicing medicine. In this case, graduates would be ready for industry and would be fed into jobs. But are doctorates what are needed?
Most people degreed in the life sciences do not even work in science and engineering. How can we better tap into this pool of people, who are clearly interested, in some level, in the life sciences? If we look at who stays in, it is primarily those individuals with Ph.D. and master’s degrees. How can we catch more of those students who receive bachelor’s degrees before they go into other things?
If we look outside academe, it is not a Ph.D. life sciences workforce. In fact, more than 70 percent of the workforce does not have an advanced degree (see Figure A-12). Many of those people have specific, practical education. Practical education, preparation for real day-to-day work, matters.
How can we attract people into the practical, professional jobs industry needs to fill? In 1997, the Sloan Foundation began one experimental approach, the Professional Science Masters program (www.sciencemasters.com). The foundation is supporting 30 programs, developed by academe in concert with industry, to produce professional skilled people in 2 years. These programs aim to deepen student knowledge; fuse and integrate fields; and integrate science with law, management, and other professional bodies of knowledge.
One example of such a program is the Master’s in Microbial Biotechnology at North Carolina State University, which is one of the three “corner” universities for which the Research Triangle is named. North Carolina’s Research Triangle Park is the largest research park, or area set aside for scientific and technical innovation and development, in the United States. The area’s needs for a well-trained high-tech workforce are considerable.
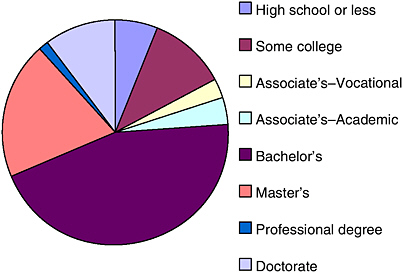
FIGURE A-12 Education levels of science and engineering (S&E) employees outside academe.
SOURCE: Derived from Science and Engineering Indicators 2002.
The N.C. State Microbial Biotechnology program mixes training in microbiology, business, and process biotechnology. Along with laying the educational groundwork and providing research experience, the program prepares its students for careers, including by actively creating professional networks that the students can step into. A dedicated 22-year-old entering a program like this emerges with a real job, a professional job, 2 years later. This is a real draw.
Evaluations of these programs are only now coming in, but one program has looked at how its graduates are doing in the job market. The average master’s holder makes about $33,000 a year. Two thirds of the graduates of the Professional Science Master’s programs are earning more than $50,000 a year, and a good number of them start out making more than $70,000. For most of these graduates, their compensation also includes additional incentives, such as signing bonuses, stock options, and tuition benefits. So their compensation compares well enough with the 2002 lawyerly average of $60,000 across specialties, since students know that law, itself, has many jobs that leave law school graduates underpaid and deep in debt. Clarifying and popularizing the track to professional master’s level jobs could, potentially, let smart, ambitious 18-year-olds see a future for themselves in science again. Some of the students who choose to go this route will find themselves more interested in the long view of research and will move off the master’s track and toward a Ph.D. But for
these students, advanced study will be a real choice, not the default it is for so many doctoral students today. Some students who enter science thinking of a good payday, or simply a stable future, will find themselves wrapped up in the excitement and joy of basic science, and they will be excellent Ph.D. students—the kind we would all like to see more of. When those students come to us, we can do great things for them, and look to them for our future.
Background
Butz W, Bloom G, Gross M, Kelly T, Kofner A, and Rippen H. 2003. Is There a Shortage of Scientists and Engineers? How Would We Know? RAND Science and Technology Issue Paper.
Committee on Dimensions, Causes, and Implications of Recent Trends in Careers of Life Scientists, National Research Council. 1998. Trends in the Early Careers of Life Scientists. Washington, DC: National Academy Press.
Fauci A. 2001. Infectious Diseases: Considerations for the 21st Century. Clinical Infectious Diseases 32:675–685.
Goldman E and Marshall Eliot. 2002. NIH Grantees: Where Have All the Young Ones Gone? Science 298:40–41.
National Science Board. 2002. “Science and Engineering Workforce,” chapter 3 of Science and Engineering Indicators—2002. National Science Foundation publication NSB-02-01.
Simmons C. 2003, March. Creating the Scientific Equivalent of the MBA. Executive Action 46.
Simmons C. 2003. New Career Paths for Science-Trained Professionals—A Progress Report on the Alfred P. Sloan Foundation’s Professional Science Master’s Degree Program. The Conference Board Report #E-0002-03, 2003.
VACCINES IN THE 21ST CENTURY
Stanley Plotkin, M.D.
University of Pennsylvania and Aventis Pasteur Vaccines
Vaccines are an essential element in the success of modern medical science, and they have played a central role in providing people around the world with longer and better lives. Indeed, it is difficult to exaggerate the impact of vaccination on the world’s population. With the exception of providing safe water, no other modality, not even antibiotics, has had such a large effect on mortality reduction and population growth. However, despite the remarkable advances that have been made in basic knowledge of immunology and microbiology, proportional translation of these findings into new vaccines has not occurred, and many diseases that need to be controlled by vaccines remain throughout all regions of the globe (see Table A-10). The evolution of a new field of microbiology and immunology—called “vaccinology,” and comprising not only vaccine development but also the use of vaccines and their effects on public health (Bendelac and Medzhitov, 2002; Plotkin, 2003)—has led to the lack of an adequately trained workforce to develop vaccines. The need for people to work on vaccines to control these pathogens is critical. An increased commitment to research and to the recruitment and training of more scientists in the field is necessary to ensure the development of vaccines for the numerous infectious diseases that threaten the world’s human population.
TABLE A-10 Some Major Infectious Diseases Uncontrolled by Vaccination
|
Chlamydia |
Influenza |
|
Cytomegalovirus |
Parainfluenza |
|
Dengue |
Malaria |
|
EBV |
Meningococcus B |
|
E. coli 0157 |
Nosocomial (Staph, enterococcus) |
|
Helicobacter pylori |
Shigella |
|
Hepatitis C |
Strep, GpA + B |
|
Herpes simplex |
Tuberculosis |
|
HIV |
Urinary tract infection |
|
Human papillomavirus |
Zoster |
Changing Vaccine Development Strategies
The technical complexity of vaccine development has increased over the years. In the past, attenuation and inactivation have been the primary paths to vaccine development (Plotkin and Plotkin, 1999). Only recently have additional methods come into play, including live recombinants, alpha virus replicons, reverse genetics, and prime-boost strategies, to name a few. So, what might have been characterized as relatively straightforward, technical work in the past has now become extremely complex, requiring a great range of expertise. For any agent of interest these days, at least four or five strategies, all different, are being explored. These strategies include:
Attenuation
Heat, oxygenation, chemical agents, and aging were the first methods of attenuation used, notably by Pasteur for rabies and anthrax vaccines. Passage in animal hosts, such as the embryonated hen’s egg, was the next method, as practiced by Theiler for yellow fever vaccine. After the development of cell culture in the 1940s, attenuation in vitro was accomplished by a variety of means, including selection of chance mutants, adaptation to growth at low temperatures, chemical mutation to induce inability to grow at high temperature (temperature sensitivity), or induction to auxotrophy in bacteria.
Inactivation
The second set of strategies is the inactivated organism or subunit path. In the late 19th century, Theobald Smith in the United States and Pasteur’s colleagues independently showed that whole organisms could be killed without losing immunogenicity, and this approach soon became the basis of vaccines for typhoid and cholera, and later for pertussis, influenza, and hepatitis A. In the 1920s, the exotoxins of Corynebacterium diphtheriae and Clostridium tetani were inactivated by formalin to provide antigens for immunization against diphtheria and tetanus. Later, influenza vaccine progressed from viral soup to the extracted proteins that are used today in acellular vaccines.
Reassortment
For viruses with segmented genomes, such as influenza virus and rotavirus, reassortment has been used to combine genetic material coding for protective antigens of pathogens with genes coding for attenuated behavior in the host. The resultant reassortants can immunize without caus-
ing illness. Reassortants have been fundamental to the preparation of both killed and live virus influenza vaccines.
Peptides
Extracted native polysaccharides from the capsules of Haemophilus influenzae type b, pneumococci, meningococci, and typhoid bacilli proved useful in immunizing older children and adults, and, more recently, the conjugation of these polysaccharides with proteins has provided us with immunogens that generate T cell memory and are effective even in young infants. Although peptide subunits of proteins have not thus far been successful against infectious diseases, they do offer hope for vaccines against melanoma and other cancers, and both lipidated and multiepitope peptides show greater immunogenicity against microbes (BenMohamed et al., 2002; Meloen et al., 2001).
Live Recombinants
To develop live recombinants, genes from heterotypic viruses can be inserted into an attenuated virus. As examples, the envelope genes from three dengue virus serotypes have been inserted into a fourth attenuated serotype to produce a candidate dengue vaccine. Dengue virus genes have also been inserted into the attenuated 17D yellow fever virus as a carrier; a candidate West Nile virus vaccine is also based on this carrier (Guirakhoo et al., 2002; Monath, 2001).
Alphavirus Replicons
Splitting cDNA copies of alpha virus RNA genomes makes it possible to insert a gene for a foreign protein into a segment that also codes for replicase enzymes, whereas the genes for the viral structural proteins are contained in another helper construct from which the packaging signal for RNA is deleted. Co-transfection enables the replicon to be incorporated into an alpha virus particle that can enter cells, in which the foreign gene is then expressed. The particle is immunogenic but unable to replicate (Liljestrom and Garoff, 1991; Rayner et al., 2002).
Reverse Genetics
Reverse genetics, the technique of inducing specific genetic lesions and then observing the phenotypic changes, is being applied to several viruses, particularly to negative stranded RNA respiratory viruses such as influenza virus, parainfluenza virus, and respiratory syncytial virus (Murphy and
Collins, 2002; Neumann et al., 1999; Fodor et al., 1999; Palese and Garcia-Sastre, 2002). This technique depends on inducing mutations at specific sites in cDNA and reconstituting a new virus by furnishing nonstructural enzymes, in a co-transfection with the modified genome segments. This rescued virus can then be examined for its phenotypic qualities.
Prime-Boost Strategies
Although immune responses and protection afforded by DNA vaccines or vectors alone are often insufficient, the combination of modalities in a prime-boost configuration is more promising (Excler and Plotkin, 1997). The prime-boost approach works both for generating antibodies and for generating cell-mediated immunity. For example, one of the earliest trials of the prime-boost concept involved priming with canarypox vectors containing human immunodeficiency virus (HIV) genes and boosting with injections of the envelope glycoprotein 120 of the virus (Pialoux et al., 1995). This approach may work for other diseases as well; in fact, clinical trials of a malaria vaccine that uses DNA priming followed by boosting with modified vaccinia Ankara (MVA) are now in progress (Moorthy and Hill, 2002).
Expanding Targets of Vaccination
Targets for vaccination are expanding (see Table A-11). Vaccination has traditionally been considered a pediatric task, aimed at improving the health of children, and pediatricians have been in the forefront of promoting and developing vaccines. As vaccine development progresses, the target diseases and populations are broadening to include adults in specific risk groups (e.g., hospitalized patients) and adults in general (e.g., for pertussis). Noninfectious diseases also will become targets of immunization strategies (Frenkel and Solomon, 2001). Cancer prevention is already provided by hepatitis B vaccine, which is reducing the incidence of hepatic neoplasms, and the recent preliminary success of a human papillomavirus vaccine in preventing infection and dysplasia is promising for cervical cancer. In addition, the isolation of antigens specific for transformed cells allows for the possible development of vaccine prevention and therapy for cancer. Immunization may also be useful in situations in which infection plays no role, such as to prevent conception or to neutralize drugs in the bloodstream to treat addiction (Singh et al., 1998; Kantak et al., 2000).
The application of vaccines to pregnant women has been inhibited by medicolegal concerns. The primary goal of vaccination in pregnancy is to either protect the newborn (e.g., group B streptococcal disease) or to protect the woman herself (e.g., influenza). Candidate vaccines that might be used late in pregnancy to protect the neonate during the early months of life
TABLE A-11 New Targets for Vaccination
|
Targets |
Examples |
|
Adolescents |
Human papillomavirus, cytomegalovirus, pertussis |
|
Adults |
Herpes simplex virus, zoster, pertussis |
|
Hospital patients |
Staphylococcus, pseudomonas, Candida |
|
Pregnant women |
Group B streptococcus, respiratory syncytial virus, parainfluenza virus 3, H. influenzae type b, pneumococcal polysaccharide, pertussis |
|
Bioterror threats |
New smallpox, anthrax, plague |
|
Noninfectious diseases |
Cancer, diabetes, Alzheimer dementia |
include those against respiratory syncytial virus, pertussis, pneumococcal polysaccharide, and group B streptococcus.
Vaccines for herpes simplex and zoster are being developed for adults. Nosocomial infections are now being targeted as well, and a staphylococcal vaccine is far advanced in development. Extending vaccination of pregnant women beyond tetanus and influenza to other diseases is being seriously considered, and efforts are being blocked only by the large legal establishment in this country. Most importantly, immunology is being extended to noninfectious diseases, to include immunization against so-called cancer antigens, antigens on neoplastic cells, diabetes, and even against amyloid for Alzheimer’s disease.
Not only is vaccinology moving ahead in those areas, but it is also moving toward therapeutic vaccination, something that has not been considered largely before (Vandepapeliere, 2002). Therapeutic vaccination against chronic infections is an entirely new field of vaccinology. Therapeutic immunization protocols are currently being tested in at least four viral diseases—hepatitis B, HIV, herpes simplex, and papilloma—based on the idea that whereas in chronic infection the host is unable to mount an effective immune response, external administration of antigens may induce cellular responses that suppress viral replication (Peters, 2001). Therapeutic immunization may also be useful in chronic bacterial infections, such as that due to Helicobacter pylori.
Workforce Issues
The new strategies and expanding targets of vaccines have led to a demand for more scientists trained to conduct research and develop vaccines. The changing nature of vaccine development has led to a need for expanded training and education of scientists in the field. Students must be educated on vaccines, vaccination, and vaccinology in medical school, so that they will consider this a realistic career path. Currently, little time and
attention is spent on the study of vaccines, and more should be done to integrate this into the current medical school curriculum.
A number of areas exist in which physicians and scientists are needed. These areas include pathogenesis and the development of animal models that shed light on pathogenesis; choice of antigens, which in turn depends on understanding of immunology of the disease; and the large area of clinical trials, which range from small trials to very large and complex trials that require a tremendous amount of preparation and knowledge of epidemiology. Safety assessments also have become important in this climate, particularly in developed countries, and people with a broad understanding of diseases are needed so analysis of an immune reaction can be performed in both the clinical and laboratory settings. Postlicensure studies on safety, effectiveness, risk groups, and persistence are necessary as well.
The study of pathogenesis is critical to vaccine development, and more young investigators are needed in this field. Molecular biology permits us to construct just about any antigen; however, there have been relatively few vaccines brought to market as a result of efforts in the area, primarily because too little is known about pathogenesis, and as a result, the target antigen remains unknown. For example, the genomic sequence is known for cytomegalovirus (CMV), but a major issue that has recently developed is that many immunoevasive genes exist in the virus. To develop a live vaccine, these genes may need to be deleted.
Education and Training
The need for scientists in vaccinology is considerable. When companies look to hire people in this area, they are having problems finding qualified candidates who have the right education and background in the sciences. This is one of the reasons why the vaccine industry is small—there are not enough people who are properly trained in the science of vaccines to comprise an adequate and well-trained workforce. Although it would be a good idea to have more than the four major companies that now currently manufacture vaccines, expanding the field is difficult, because each new company will be competing with the larger companies to hire the few trained personnel that exist. It is vital that on-the-job training opportunities, especially for students, be further developed to ensure that professionals are exposed to career paths in vaccinology. Training programs in vaccinology are critical for the development of a strong workforce.
Another problem is the trivial amount of time in medical school that is devoted to disease prevention via vaccines. A practical solution to this would be to change the curricula to emphasize prevention rather than treatment. Currently, some postgraduate vaccinology courses and programs are in place both domestically and internationally. These programs may
provide a solid foundation on which present programs can be expanded and future epidemiology training programs modeled.
Since 2000, the Marcel Merieux Foundation, headquartered in France, has offered an annual course in advanced vaccinology, which aims to introduce participants to the different aspects of vaccinology, and, in particular, the development of vaccines, the conduct of clinical trials, and the safety issues involved in the administration of vaccines. This course, delivered in English, is intended for scientists of both the public and private sectors who are responsible for vaccine development, the implementation of vaccine strategies, or the introduction of new vaccines in public health programs. The course also covers selecting appropriate vaccination strategies, integrating new vaccines into public health programs, the side effects of vaccines, perfecting new vaccines, and therapeutic vaccines. This course is open to people from all over the world, and developing countries have shown great interest. Surprisingly, few Americans apply for the course, even though there is scholarship money available to pay their expenses. This is astonishing, but there is not a large pool of people in training who are interested in vaccine development. So, academia and the vaccine industry should partner to discuss and develop such a program. While the 2-week course in France is exactly this type of program, there is a paucity of other courses (Fondation Marcel Merieux, 2003).
Infectious diseases are complex, a fact that has led to a focus on multidisciplinary and multicultural training. This is true for the vaccine industry as well. It is very clear that a microbiologist can work in the laboratory and move into the world of vaccinology by trial and tribulation. However, to encourage more people to go into this field, it would be useful to develop a multidisciplinary program that includes training in a number of core areas, including microbial immunology, safety regulations, scale-up technology, clinical development, and investigational new drug formulations. A multidisciplinary approach in education would enable students to learn about vaccine development, and much could be gained by this approach. The question that then arises is who will teach these courses? The majority of qualified people are in industry. Trials often cannot be done too many times if they are not done correctly the first time; there are not too many second chances when it comes to clinical trials. It is also possible to learn from academics who have been through clinical trials, but again, most of the people with such experience are in industry.
People who have conducted phase III trials outside of industry do in fact exist, but there is no formal training available in that type of complex operation—and the complexity of such trials is ever increasing as regulations increase. So, those people who have mastered the necessary skills are rare, and they are solicited for their expertise. Although these skills are specialized, it is possible to teach them. For example, a vaccinology fellow
|
Box A-1 The National Institutes of Health funds a training grant in vaccinology at the University of Maryland Center for Vaccine Development. This program enables individuals with M.D. or Ph.D. degrees to be prepared specifically for careers in vaccinology, either to pursue basic vaccine development research or to conduct investigative clinical trials. The program offers all trainees a broad exposure to both the laboratory and clinical trial phases of vaccinology, but is set up as two tracks so that trainees can select whether to concentrate in either the laboratory or the clinical aspects of vaccinology. The laboratory track provides for training basic scientists and physician–scientists in vaccine development laboratory research, particularly in the use of recombinant DNA technology to prepare new vaccine candidates and the use of modern immunological techniques to study the human humoral and cellular immune response to different vaccines. The clinical track trains clinicians (internists or pediatricians) in clinical trial design, protocol preparation, procurement of administrative and ethical clearances, and performance of clinical trials and analysis of data. The ultimate goal of this program is to provide a well-trained cadre of individuals who can fully exploit the unprecedented opportunities now available in vaccine development. SOURCE: University of Maryland School of Medicine, 2003. |
from a university participating in the development of a phase III trial would learn from this experience. A number of formal courses in vaccinology are taught in schools of public health throughout the United States and abroad. For example, courses are offered at the University of Maryland, Johns Hopkins University, the University of Geneva, and the University of Texas at Galveston. The University of Maryland Center for Vaccine Development provides formal training in all aspects of vaccinology, through a training grant from the National Institutes of Health (see Box A-1).
Getting skilled people in industry engaged at the level of training scientists when they are in their predoctoral and early postdoctoral period is a challenge that needs to be addressed—but solutions should be possible. Confidentiality issues may be involved, but they could be worked out. Other issues to be addressed extend beyond the science underlying development and the practical aspects of development to marketing issues and to the policy issues related to utilization and acceptance.
The development of vaccines is a delicate fabric. The makeup of this fabric consists of academia and biotechnology companies developing ideas and passing them to industry, which then develops the products. The government then comes in, developing and enforcing regulations and making
recommendations, and then academe again becomes involved in testing the vaccines. This process is working fairly well at the moment, but vaccine shortages have recently become apparent. In order to expand on what we have now, shortages of people will be encountered along the way.
References
Bendelac A and Medzhitov R. 2002. Adjuvants of Immunity: Harnessing Innate Immunity to Promote Adaptive Immunity. J Exp Med 195:F19–F23.
BenMohamed L, Wechsler SL, and Nesburn AB. 2002. Lipopeptide Vaccines: Yesterday, Today, and Tomorrow. Lancet Infect Dis 2:425–431.
Excler JL and Plotkin SA. 1997. The Prime-Boost Concept Applied to HIV Preventive Vaccines. AIDS 11:S127–S137.
Fodor E, Devenish L, Englehardt OG, PAlese P, Brownlee GG, and Garcia-Sastre A. 1999. Rescue of Influenza A Virus from Recombinant DNA. J Virol 73:9679–9682.
Fondation Marcel Merieux. 2003. Advanced Vaccinology Course. [Online] Available: http://fond-merieux.org/eng/enseignement/indexnew.htm [accessed August 19, 2003].
Frenkel D and Solomon B. 2001. Towards Alzheimer’s Beta-Amyloid Vaccination. Biologicals 29:243–247.
Guirakhoo F, Pugachev K, Arroyo J, Miller C, Zhang ZX, Weltzin R, Georgakopoulos K, Catalan J, Ocran S, Draper K, and Monath TP. 2002. Viremia and Immunogenicity in Nonhuman Primates of a Tetravalent Yellow Fever-Dengue Chimeric Vaccine: Genetic Reconstructions, Dose Adjustment, and Antibody Responses Against Wild-Type Dengue Virus Isolates. Virology 298: 146–159.
Kantak KM, Collins SL, Lipman EG, Bond J, Giovanoni K, and Fox BS. 2000. Evaluation of Anti-Cocaine Antibodies and a Cocaine Vacine in a Rat Self-Administration Model. Psychopharmacology (Berl) 148:251–262.
Liljestrom P and Garoff H. 1991. A New Generation of Animal Cell Expression Vectors Based on the Semliki Forest Virus Replicon. Biotechnology (NY) 9:1356–1361.
Meloen RH, Langeveld JP, Schaaper WM, and Slootstra JW. 2001. Synthetic Peptide Vaccines: Unexpected Fulfillment of Discarded Hope? Biologicals 29:233–236.
Monath TP. 2001. Prospects for Development of a Vaccine Against the West Nile Virus. Ann NY Acad Sci 951:1–12.
Moorthy V and Hill AV. 2002. Malaria Vaccines. Br Med Bull 62:59–72.
Murphy BR and Collins PL. 2002. Live-Attenuated Virus Vaccines for Respiratory Syncytial and Parainfluenza Viruses: Applications of Reverse Genetics. J Clin Invest 110:21–27.
Neumann G, Watanabe T, Ito H, Watanabe S, Goto H, Gao P, Hughes M, Perez DR, Donis R, Hoffmann E, Hobom G, and Kawaoka Y. 1999. Generation of Influenza A Viruses Entirely from Cloned cDNAs. Proc Natl Acad Sci USA 96:9345–9350.
Palese P and Garcia-Sastre A. 2002. Influenza Vaccines: Present and Future. J Clin Invest 110:9–13.
Peters BS. 2001. The Basis for HIV Immunotherapeutic Vaccines. Vaccine 20:688–705.
Pialoux G, Excler JL, Riviere Y, Gonzalez-Canali G, Feuillie V, Coulaud P, Gluckman JC, Matthews TJ, Meignier B, Kieny MP, et al. 1995. A Prime-Boost Approach to HIV Preventive Vaccine Using a Recombinant Canarypox Virus Expressing Glycoprotein 160 (MN) Followed by a Recombinant Glycoprotein 160 (MN/LAI). AGIS Group, and l’Agence Nationale de Recherche sur le SIDA. AIDS Res Hum Retroviruses 11:373–381.
Plotkin S. 2003. Vaccines, Vaccination, and Vaccinology. JID 187:1349–1357.
Plotkin SL and Plotkin SA. 1999. The History of Vaccination. In: Plotkin SA, Orenstein WO, eds. Vaccines. 3rd ed. Philadelphia: W. B. Saunders. Pp. 1–12.
Rayner JO, Dryga SA, and Kamrud KI. 2002. Alphavirus Vectors and Vaccination. Rev Med Virol 12:279–296.
Singh M, Das SK, Suri S, Singh O, and Talwar GP. 1998. Regain of Fertility and Normality of Progeny Born During Below Protective Threshold Antibody Titers in Women Immunized with the HSD-hCG Vaccine. Am J Reprod Immunol 39:395–398.
University of Maryland School of Medicine. 2003. Center for Vaccine Development. [Online]. Available: http://medschool.umaryland.edu/cvd/training.htm [accessed August 19, 2003].
Vandepapeliere P. 2002. Therapeutic vaccination against chronic viral infections. Lancet Infect Dis 2:353–367.
SCHOOLS OF PUBLIC HEALTH: MEETING THE WORKFORCE CHALLENGE OF EMERGING INFECTIONS
Margaret A. Potter, J.D.
Associate Dean and Director
Center for Public Health Practice
University of Pittsburgh Graduate School of Public Health
Pittsburgh, PA
Schools of public health contribute to meeting the challenge of emerging infections. Faculties at these schools conduct research and teach current and future working professionals. However, for a number of reasons, measuring the need for and the impact of these contributions is problematic. We have reliable estimates on the current supply of professionals trained in epidemiology and disease investigation, but we lack standards and methods for determining demand, that is, the appropriate number needed for optimal surveillance, detection, and response. Nor do we yet know how well the schools are meeting the task of educating those in the workforce, since performance capacity studies are lacking.
The experience with anthrax-contaminated mail in the fall of 2001 and winter of 2002 raised concern about the lack of good information and illustrated the fact that state and local public health agencies could quickly become overwhelmed by the intentional dispersion of an infectious agent. The federal Government Accounting Office estimated that authorities had received 70,000 samples containing white powder suspected of being anthrax during that 3-month period; and it identified gaps in disease surveillance systems, inadequate laboratory facilities, and workforce shortages (Heinrich, 2003).
This report presents a summary of recent and ongoing efforts within and outside of public health schools to address some of the demand and supply issues concerning public health professionals. It begins with an overview of workforce information that is specific to the infectious disease challenge, examines some of the current and future contributions by the schools to meeting the demand, and concludes with recommendations for research and education focused on assuring that schools contribute optimally to the task of protecting the public from emerging infections.
Current Supply of Public Health Infectious-Disease Workers
Gebbie et al. (Gebbie et al., 2000) have recently reported a job-classified enumeration of the approximately 448,254 individuals who constitute the nation’s paid public health workforce. The classifications most relevant to meeting the challenge of emerging infections are “epidemiolo-
gist” and “infection control/disease investigator.” Together, these two classifications contribute less than 0.47 percent of the total enumerated workforce. This percentage may underrepresent or overcount the actual number of relevant workers, for several reasons. First, not all epidemiologists work on infectious diseases for all or most of their time; some of them, for example, work on chronic diseases and injuries. Second, workers who function in these job classifications might hold otherwise-titled positions or might work in agencies not included in the count (e.g., state environmental health departments). Third, some professional classifications (e.g., physicians and nurses) that are included in the enumeration might function as infectious disease specialists, but the enumeration data failed to capture the functional roles of individual workers. Fourth, since the year-2000 enumeration, staffing for the detection and containment of infectious diseases in state and local health departments has probably increased due to federal bioterrorism funding. Despite these limitations, given that epidemiology is the core science of infectious disease monitoring and that infection control/investigation is the front-line defense against outbreaks, the fact that these positions comprise such a low percentage of the public health workforce is startling.
The “Demand” Side: Currently Employed Infectious-Disease Workers
There is no good information about how large a professional workforce is needed to combat emerging infections, how specifically to educate people for this work, or what the rate of turnover in the relevant positions might be. These are quite clearly important questions for educators and policy makers. Systematic studies of public health capacity—particularly research on the number, types, and distribution of professionals needed to confront emerging infections—do not exist. Without such information, schools cannot target education and training programs, state and local governments lack standards for staffing of public agencies, and policy makers cannot rationally allocate resources for achieving this important public health function.
At least one professional collaboration attempted to quantify public health workforce needs for its own strategic planning purposes, using the professional judgment and experience of a committee comprised of local and state health officials and legislative staff. This committee estimated that minimum staffing should include 1.1 full-time-equivalent (FTE) epidemiologists and 0.55 FTE disease investigators per 50,000 people (Libbey, 1998). As fully acknowledged by its contributors, this method was subjective and not validated by systematic performance-capacity research. The staffing numbers projected by these FTE-to-population ratios are limited by the fact that actual staffing patterns must adapt to available resources and be suited to jurisdictional size, population, political organization, population-
specific health risks, and other factors. Nevertheless, if projected to the entire U.S. population (more than 280 million) and compared with the workforce enumeration data, then this method suggests that there are fewer than 20 percent of epidemiologists and about 30 percent of disease investigators actually on the job, as compared with the need. The disparity between projected need and current actual staffing patterns would vary widely among regions of the country, between neighboring states, and even among areas within states. Even if the “correct” FTE projections for any jurisdiction were half of those cited here, then the conclusion would remain that the functions of epidemiology and disease control/investigation should probably be staffed with more professionals than are currently in place.
The “Supply” Side: Research and Teaching
Schools of public health contribute to the supply of infectious disease specialists in the public health workforce by conducting research that informs professional judgment and programming and by educating the workforce both current and future. Both sets of functions have been undergoing significant change within these schools over the past decade, and continued developments are foreseeable.
Research
Practice-oriented research is needed to answer the questions about how many students and workers are needed to meet the challenges of emerging infectious diseases, and schools of public health have a special role here. Scientists in these schools contribute to the pursuit of research into communicable diseases, their vectors, their incidence and prevalence, their prevention, and their treatments, along with scientists in other schools as well as with those in public-sector agencies and private-sector institutions. The foci of this research span a continuum from basic, laboratory-based studies and clinical trials on the one end all the way to experiential, practice-based studies at the opposite end. Academic scientists in public health, like their counterparts in other schools, often have greater support and incentives to work on problems at the basic science/clinical end of the research continuum. But public health schools have special reasons to encourage the attention of their faculties to topics at the practice end of the research continuum. Two sequential reports by the Institute of Medicine concerning the future of public health, one in 1988 (IOM, 1988) and the other in 2003 (IOM, 2003), pointedly recommended that schools of public health should conduct research on improving the capacities and performance of public health agencies and on the health of groups, communities, and populations.
Since 1993, accreditation criteria for these schools have included specific encouragement for practice-oriented research (CEPH, 2002).5
Recent developments provide further incentives for practice-oriented public health research by drawing attention to the scholarly importance of this field. In 2002, Academy Health (a national organization of scientists focusing on health research and policy) authorized the formation of a Public Health Systems Research Affiliate, and in 2003 the organization added public health as a major session within the agenda for its annual research meeting. The Council on Linkages Between Public Health Practice and Academia, whose leaders and membership include academicians in public health and preventive medicine, is developing an agenda and soliciting funding commitments for public health systems research. While the topics on this agenda (workforce, infrastructure, and performance standards) are not restricted to infectious disease alone, they are highly relevant to the capacities and effectiveness of public health systems to face the challenge of emerging infections.The Association of Schools of Public Health (ASPH), the membership organization of fully accredited institutions in the United States, has provided leadership for the development of practice-oriented research. In 2000, the ASPH Council of Public Health Practice Coordinators (faculty and administrators appointed by their deans to advise and to manage academic-practice programs) issued a white paper that articulated a comprehensive rationale for practice-oriented scholarship, including research (ASPH, 2000). Planning to further this work, the council in September 2003 convened a 2-day workshop to initiate the writing of another white paper that will examine, among other issues, the academic policies that affect faculty members’ incentives to conduct practice-based research.6
Teaching
There are currently 36 accredited schools of public health, with the number of schools increasing by six during the past decade. The schools’ accreditation criteria mandate that they sponsor degree programs in five core disciplines, including epidemiology (CEPH, 2002b).
In 2002, ASPH-member schools produced more than 1,000 graduates in epidemiology (ASPH, 2003), but this number has limited relevance to the
actual supply of epidemiologists who enter the public health workforce. Little is known about the specific educational backgrounds of public health workers, except that formal training for such careers is unusual rather than typical (Public Health Functions Project, 1995). According to the federal Health Resources and Services Administration (HRSA), in 1989 only 44 percent of the then-estimated 500,000 public health workers had any formal, academic training in public health, and those with graduate public health degrees were an even smaller fraction (HRSA, 1991). Even less is known about career paths among graduates of public health degree programs. The educational requirements for employment in epidemiology positions (e.g., master’s versus doctor’s degree) differ among state and local jurisdictions. Not all individuals who hold the title “epidemiologist” necessarily have formal education specific to their work, and many who do attain such education do not go to work in public health agencies. Furthermore, some institutions that are not public health schools also contribute to the supply of these workers. There are currently 41 accredited Master of Public Health (MPH) programs in community-health and preventive-medicine departments of medical schools, and there are 16 accredited MPH programs in other schools (CEPH, 2005).
Given that most public health workers are not formally educated in this particular field, the schools are directing practical training programs to them in their work sites, by distance-communication media, and in special on-campus programs. Two federal training programs are currently administered through cooperative agreement grants available exclusively to ASPH-member schools of public health. The Health Resources and Services Administration launched its Public Health Training Centers in 2000 and now funds 14 of these centers in schools of public health (U.S. Health Resources and Services Administration). The federal Centers for Disease Control and Prevention (CDC) created Centers for Public Health Preparedness in 2001 and now sponsors 22 such centers in the schools (CDC, 2003). The training provided through these centers includes crosscutting topics of relevance to public health practice as well as specialized topics relevant to emerging infectious diseases.
However, the continued effectiveness and commitment of schools to train working professionals depends in part on funding from the public sector. Since public health as a discipline does not have credentialing or continuing-education requirements (as do some related disciplines such as medicine, health education, and nursing), its workers have little reason for, and no expectation of, paying out-of-pocket for post-degree training. Currently, grant programs of the CDC and HRSA heavily subsidize the cost of training to the agencies that employ these professionals, and the school-based centers function as nonprofit organizations under the terms of their cooperative agreement contracts. Without this funding mechanism, profes-
sionals employed in state and local health departments would lack both incentives and resources to pursue training.
Recommendations
The foregoing overview of demand and supply issues for the nation’s infectious disease workforce brings into sharp relief several major concerns that call for attention.
First, the numbers, actual jobs, characteristics, and qualifications for members of the public health and infectious disease workforce are not sufficiently well documented. The year-2000 enumeration study was a very important and well-executed effort to begin this documentation, and it should be repeated on a regular basis over time. However, a limitation of that study was the lack of correspondence between its standardized set of universal job classifications (as recommended by a national blue-ribbon panel (Public Health Functions Project, 1995)) and the position descriptions actually used by the states and local health agencies whose workers were counted. For the future, a better approach might be to base workforce enumeration on the essential public health services or on important crosscutting functions. The staffing of work needed to carry out surveillance, detection, and response to emerging infections is indeed one of those functions. Future studies of the public health workforce should also include demographics and educational backgrounds, information that will help to guide both educators in designing programs and students in selecting them. Schools of public health should systematically track the career paths of their graduates and assess the incentives that draw some of them into public service. This information will help to inform hiring and compensation decisions among public agencies and policy makers.
Second, there is an inadequate base of evidence on which to guide policy making for targeting education and training programs, for specifying qualifications and numbers of public agency staffs, and for allocating resources for workforce development. Public health systems research is needed to assess the performance capacity of public health agencies. The training of workers should be planned and directed to achieve strategic improvements in the worker competencies needed to assure infectious-disease surveillance, detection, and response. Schools should consider the review of academic policies that create disincentives for faculty members to contribute to this research.
Third, research and education to assure an effective infectious disease workforce cannot be sustained without federal and state funding commitments. Practice-oriented research, including public health systems research, lacks current earmarks in the major federal health-research budgets of the National Institutes of Health and the Centers for Disease Control and
Prevention. The authorizing legislation for both the CDC and the HRSA workforce training programs will soon expire. For the HRSA training centers, appropriations have been eliminated from federal administration budgets in each fiscal year since they were first authorized, making their ongoing operations repeatedly subject to special action by Congress during each of the past 3 years.
References
ASPH (Association of Schools of Public Health), Council of Practice Coordinators. 2000. Demonstrating Excellence in Academic Public Health Practice. J Public Health Management Practice 6(1). [Online]. Available: http://www.asph.org/uploads/demon.pdf [accessed March 23, 2005].
ASPH. 2003. 2002 Annual Data Report. [Online]. Available: www.asph.org/uploads/adr2002.pdf [accessed March 23, 2005].
CDC (Centers for Disease Control and Prevention), Office of Workforce Policy and Planning. 2003. Centers for Public Health Preparedness Program. [Online]. Available: www.phppo.cdc.gov/owpp/CPHPLocations.asp [accessed March 22, 2005].
CEPH (Council on Education for Public Health). 2002. Accreditation Criteria, Graduate Schools of Public Health. [Online]. Available: www.ceph.org [accessed September 15, 2003].
CEPH. 2002b. Accreditation Criteria, Graduate Schools of Public Health. [Online]. Available: www.ceph.org [accessed March 22, 2005]. See Criterion V-A.
CEPH. 2005. Accredited Schools and Programs. [Online]. Available: www.ceph.org. [accessed March 22, 2005].
Gebbie K, Merrill J, Biloush R, Cortazal M, Gebbie E, Gupta M, Hrvang I, King M, and Wagner M. 2000, December. The Public Health Workforce: Enumeration 2000. Rockville, MD: U.S. Health Resources and Service Administration, Bureau of Health Professions, National Center for Health Workforce Information and Analysis.
Heinrich J, Director, Health Care–Public Issues. 2003, May 7. SARS Outbreak. Improvements to Public Health Capacity Are Needed for Responding to Bioterrorism and Emerging Infectious Diseases. Government Accounting Office Report 03-769T.
HRSA (Health Resources and Services Administration), Bureau of Health Manpower. 1991. A Report to President and Congress on the Status of Health Professions Personnel in the United States. Manpower Analysis Branch 1978–1990.
HRSA. Bureau of Health Professions. Public Health Training Centers Program. [Online]. Available: http://bhpr.hrsa.gov/publichealth/phtc.htm [accessed March 23, 2005].
IOM (Institute of Medicine). 1988. The Future of Public Health. Washington DC: National Academy Press. P. 16.
IOM. 2003. Who Will Keep the Public Healthy? Educating Public Health Professionals for the 21st Century. Washington, DC: The National Academies Press. P. 12.
Libbey P. 1998, October. Correspondence and unpublished draft report on staffing estimates in relation to public health capacity standards for Washington State.
Public Health Functions Project. 1995. The Public Health Workforce: An Agenda for the 21st Century. Washington, DC: U.S. Department of Health and Human Services.
U.S. CAPACITY TO CONFRONT EMERGING VECTOR-BORNE PATHOGENS
Andrew Spielman, Sc.D.
School of Public Health
and
Center for International Development
Harvard University
The discipline of public health entomology began to assume its present form during the 1960s with the development of the concept of vectorial capacity and the abandonment of hope that malaria could be eradicated. The National Institutes of Health (NIH) system of funding investigator-initiated grant proposals soon became the main source of support for research in tropical medicine and parasitology (TMP) in the United States. Insect physiology came to be considered relevant to tropical medicine and parasitology following a Woods Hole Conference in 1978. Within 4 years, so many proposals of this kind were received that a separate ad hoc study section was formed to consider entomological proposals. Insect transgenesis came to be considered relevant to TMP following a Keystone Symposium in 1993. In 1994, the four main U.S. societies dealing with vector-borne pathogens passed resolutions requesting a narrower definition of TMP. The broadened definition held, however, and the ad hoc study section was divided once again in 2003 such that proposals containing a field component were excluded. Vector biology, thereafter, would be removed from TMP and considered in an epidemiological context. A Coolfont Symposium in 1982 distinguished public health entomology as taught in health-related institutions from that taught in departments of entomology in land-grant institutions and enumerated the faculty engaged in this work. Another survey, conducted in 2002, indicated that about half of these programs had been discontinued. An Institute of Medicine (IOM) conference in 2003 recommended that the U.S. “human resource capacity” in vector biology should be “rebuilt.” Although the NIH system of investigator-initiated grants largely determines the characteristics of the faculty employed in health-related institutions, private donors and foundations may also influence hiring practices. The reemerging discipline of public health entomology should rest heavily on vector ecology, epidemiology, and microbiology. (This report summarizes a more detailed account published in the Journal of Experimental Biology [Spielman, 2003].)
Introduction
Malaria and dengue remain as major health burdens and as obstacles to economic development throughout much of the world’s tropics, while Lyme disease and West Nile fever continue to emerge in many temperate regions. The growing level of annoyance caused by many diverse insects and ticks, of course, adds to the need for effective entomological interventions. The research activities that are appropriate for dealing with these problems focus primarily on vector ecology, but they also include epidemiology and population genetics, as well as aspects of insect physiology. Vector transgenics may, in the future, provide useful modalities. The research interests of the faculty serving in U.S. universities largely determine the characteristics of our scientific workforce, and the discussion that follows is designed to identify the forces that influence hiring practices for faculty engaged in public health entomology.
Discussion
Source of U.S. Research Funding
In teaching institutions in the United States, health-related positions for junior faculty are allocated largely on the basis of external funding. Such “soft” funding less critically defines faculty profiles in universities whose appointees receive their salaries from the various states. During the second half of the 20th century, therefore, the administrations of schools of public health and of medicine increasingly designed their faculties around the “investigator-initiated” system of research grants awarded by the National Institutes of Health, and the “RO1” system of grants served largely as the engine of faculty growth. Today, job descriptions continue to be composed mainly around this perception. Before 1982, proposals relating to vector-associated disease were reviewed by the members of the Tropical Medicine and Parasitology Study Section of the National Institute of Allergy and Infectious Disease (NIAID). The entire gamut of relevant disciplines was considered by this group of experts in entomology, microbiology, vaccinology, and other disciplines.
Developments Following the Woods Hole Conference of 1978
Entomological review was separated from the regular TMP Study Section in 1982, in the wake of the development of the first hormonomimetic insecticides and the landmark meeting of this committee in 1978 in Woods Hole, MA. The meeting was inspired by the research accomplishments of the noted insect physiologist Carroll Williams, who spoke of the “third
generation of insecticides” that was then being developed. The sense of this meeting held that although funding for insect physiology had previously derived largely from the National Science Foundation, any research effort pertaining to the physiology of insects should now be considered relevant to tropical medicine or parasitology. The NIAID accepted this recommendation and agreed to consider such proposals. Many proposals subsequently were submitted, and they were reviewed by the TMP Study Section as a whole. Some of the proposals in insect physiology were funded, and this encouraged additional submissions, which, in turn, required the assignment of reviewers who specialized in insect physiology. Within 4 years, so many basic physiological proposals were submitted that a new ad hoc committee was formed to evaluate all proposals requiring entomological attention. Epidemiological and parasitological applications of entomology, as well as certain arbovirological proposals, were thereupon separated from the health-related sciences and placed in a context that included basic insect physiology. The composition of this standing committee thereafter evolved to match the proposals that were submitted, a situation that would necessarily tend to favor subjects familiar to the members of the committee.
By 1994, the effect of this separation of entomology from health was such that the community of public health entomologists in the United States became alarmed. Led by George Craig, the various societies that were most directly concerned with tropical health addressed resolutions to the NIH director, requesting corrective action. These societies included the American Society of Tropical Medicine and Hygiene, the Entomological Society of America, the Society of Vector Ecology, and the American Mosquito Control Association. The societies pointed out that 93 percent of the 56 grants in vector biology that were funded in 1993 dealt with fundamental insect physiology or molecular genetics, and that their principle investigators mainly were associated with experimental research rather than with tropical medicine or medical entomology. Within a decade after this ad hoc study section became a separate unit, virtually all NIAID-funded work on vector-associated disease would then have been conducted entirely at the bench. No analysis of previous funding patterns was provided.
Developments Following the Keystone Conference of 1998
American scientists concerned with vector-associated infections began to employ molecular techniques during the late 1980s; the first symposium on that subject was held at the annual meeting of the American Society of Tropical Medicine and Hygiene in 1986. It examined the idea that the pathogen competence of a vector population might be reduced by releasing transposon-favored, transgenically incompetent mosquitoes. None of the speakers were, themselves, engaged in work on vector arthropods. That
situation soon changed. Numerous vector-related projects soon focused largely on molecular genetics. Indeed, 22 of the 53 titles that comprised the 1998 Keystone Symposium on transgenesis, titled “Toward the Genetic Manipulation of Insects,” dealt with mosquitoes or kissing bugs (James et al., 1998). The expertise of three of the five conference organizers derived largely from their research accomplishments with mosquitoes. This influential symposium was the second in a continuing series of such events that were funded by the John D. and Catherine T. MacArthur Foundation and attended by members of various granting agencies. The sequencing of the genomes of Plasmodium falciparum (Gardner et al., 2002) and Anopheles gambiae (Holt et al., 2002) and the ongoing NIAID-funded effort to sequence that of Aedes aegypti have greatly facilitated such work. The creation of an insect that might be released in nature and that would transmit particular useful genes to a disproportionate fraction of its offspring became the goal of many research efforts.
The self-generating dynamic that followed the acceptance of insect physiology by the TMP Study Section in 1978 operated once again in 1998. The many proposals relating to molecular genetics that were submitted to the ad hoc medical entomology panel, soon designated as an “Ad Hoc Special Emphasis Panel,” required appropriate reviewers’ expertise. Members of a review panel would naturally tend to favor proposals in their own discipline. Such a shift in membership encouraged the submission of more proposals of this nature, and the more molecular proposals that were submitted and funded, the more the membership shifted. In a session held in 2002, for example, 17 of the 20 members were themselves engaged exclusively in experimental research performed in the laboratory. This process accelerated into 2003 when the Ad Hoc Special Emphasis Panel was divided, much as the original Tropical Medicine and Parasitology Study Section was divided in 1982. All entomological proposals that included a field component were thereupon removed to an epidemiological study section, then operating within the NIAID.
Sources of Research Funding
The NIAID program of investigator-initiated grants in tropical medicine and parasitology was augmented in 1980 by a system of tropical disease research units that originally was designed to support overseas work on the five parasitoses selected by the World Health Organization (WHO) and expanded in 1995. These “program grants” include several discrete “projects,” and they generally are based in a tropical site. Although few in number, these university-based programs continue to provide first-rate employment and training opportunities for people engaged in research on vector-borne infections.
Supplemental funding opportunities have been provided since 1982 by the Small Business Innovation Research Program (SBIR), which is designed to encourage small U.S. businesses to develop innovative products in conjunction with the academic scientific community. Various governmental agencies contributed more than $1 billion during 2002 to this program. A complementary program, known as the Small Business Technology Transfer Program (STTR), expanded support for these academic–entrepreneurial links, and contributed nearly $100 million more during 2002. Although health expenditures would have comprised only a fraction of these totals, the financial incentives would be considerable. Except for efforts devoted to bioterrorism, it seems unlikely that these programs would be sufficiently reliable to serve as stimuli for the creation of academic appointments.
The NIH’s system of training grants has long provided crucial support to many generations of students interested in vector-associated disease. The NIAID program is designated mainly for U.S. nationals, and the program conducted by the Fogarty International Institute is mainly for foreign scientists. Although both programs support students, neither provides faculty salaries. The federal Centers for Disease Control and Prevention (CDC) recently initiated a system of training grant awards in public health entomology, and it now awards research contracts in response to particular emerging infections. These training programs and occasional research efforts do little to stimulate faculty hiring.
The United States military was an important source of extramural funding for research in vector-associated disease during the 1970s. The military-funded, investigator-initiated proposals, much as those considered under NIH’s RO1 system, supplied funds according to the opinions of an Ad Hoc Study Group on Medical Entomology of the Walter Reed Army Institute of Research. This panel operated in the pattern of an NIH study section. That program, however, was too small to influence staffing patterns in the U.S. university system, and it ended during the middle 1980s. Particular projects on such vector-borne “select agents” as those responsible for tularemia and eastern equine encephalitis have been funded by the Defense Advanced Research Projects Agency. But this source of funding, too, is small and potentially short-lived and may not influence university hiring practices. The various Naval Medical Research Units also maintain overseas laboratories that conduct research projects devoted to vector-borne infection. Grants from the National Oceanic and Atmospheric Administration support faculty engaged in research on the distribution of these infections.
The U.S. Agency for International Development (USAID) became a major granting agency in 1963, in the wake of the failure of the worldwide effort to eradicate malaria. Although malariological research was discouraged during the eradication effort, 5 percent of all operational funds were designated for research after the effort was abandoned. An audit of the
program, conducted in 1983, described a $125 million general research fund that had been awarded since 1963 (GAO, 1982). Of this, the $26.5 million that had been spent was devoted mainly to academic research on drug and vaccine development. Robert Desowitz’s book Malaria Capers (1993), however, described the sadly disappointing nature of this research effort. USAID’s subsequent program of “environmental impact evaluation” provided opportunity for numerous university faculty to gain important experience in the epidemiology of infectious disease, but provided little salary support. Such “nonacademic” units as Harvard University’s Institute for International Development once devoted important resources to the central administration of that institution, but generated few new teaching faculty. The personnel were recently transferred to Boston University. The National Science Foundation also awards relevant funds. Although certain of the non-health-related U.S. governmental agencies provide some support for university faculty, their impact on university hiring practices seems slight.
Funds from the U.S. Department of Agriculture (USDA) largely shape the faculties of U.S. land-grant institutions. Faculty at these state universities draw their salaries as a line item in each state’s budget, and many of them also acquire research funding from federal “Hatch” funds. Until recently, these universities produced many of the medical entomologists employed by public health agencies and universities. The entomological orientation of the land-grant programs has been uniquely strong, and the departments of entomology in the United States tend to be located in such institutions. This element of financial permanence largely insulates the faculties of land-grant colleges from peer-generated pressures on their faculty profiles. Although NIAID funding supplements their basic agriculture-oriented sources, the faculty profiles of the land-grant schools tend to respond less directly to public health requirements than do those of schools of medicine or of public health.
Various foundations have long played an important part in funding research efforts relevant to vector-borne infection. The Rockefeller Foundation, of course, contributed much fundamental knowledge during the early part of the 20th century. The MacArthur Foundation’s program has focused narrowly on molecular biology, as has the program of the Burroughs Wellcome Fund. The Bill & Melinda Gates Foundation has entered this field of endeavor with a system of unusually large donations. A multimillion-dollar gift to the London School of Tropical Medicine has permitted that institution to transform its malaria activities with a multifaceted program of research. An even larger gift to the Johns Hopkins Bloomberg School of Public Health, from another anonymous source, permitted that school to expand its malaria program. New faculty members appear to have been recruited in response to both of these gifts. The Gates Foundation has
recently requested suggestions for a grand malariological challenge, and we await the result. This effort, too, seems likely to increase the number of scientists engaged in research on vector-borne infection. Although foundation support now tends to be directed toward narrow “cutting-edge” goals, such funds have been sufficiently generous and sustained since the early 1990s to influence faculty hiring patterns.
Antimalaria interventions recommended by the Roll Back Malaria program of the WHO and its partner agencies seek to halve the burden of malaria during the first decade of the millennium, and to halve it once again by 2015, by “scaling up” the application of these techniques. Only limited operational research is conducted, and progress has not yet been reported. The United Nations recently launched a Millennium Development Goals program for reducing poverty in the developing world, and one component of this program is concerned with developing antimalaria strategies. The role of research in this developing strategic formulation is yet to be defined.
Changes in Vector-Related Activities in U.S. Universities
A comprehensive review of the status of training and research in public health entomology was conducted in 1982 as part of the Coolfont Symposium, which was organized by the National Research Council and included participants from various universities, diverse laboratories, the military, federal and multilateral granting agencies, and various foundations. Questionnaires were submitted to 28 schools of medicine, schools of public health, departments of biology, and departments of entomology that were identified as potential sources of training in disciplines that pertained to the transmission of vector-associated disease. The 24 institutions that responded listed 63 relevant faculty, and about half of the respondents had only 1 faculty member. Of those responding, 17 had teaching programs that included some field-related component; but only 7 had overseas components.
Characteristics of the different programs that were identified are instructive. Because faculty in the seven land-grant institutions draw their salaries from their state coffers, they tend to design their research and teaching programs around local needs. The training programs of these institutions focused on the biology of the vectors themselves, and none included course work in epidemiology or pathogenesis. A few programs included virological components. Conversely, the seven health-oriented institutions emphasized course work pertinent to the burden of human disease while downplaying entomological subjects. The salaries of these health-related faculty were then, as now, notoriously soft, deriving mainly from external sources, a fact that induces the faculty to cast a broad net in their search for grant support. Overseas activities play a large part in their endeavors. The three responding departments of biology were housed in pri-
vate institutions. Their programs and research orientation differed. One department, at Notre Dame University, trained a large fraction of the medical entomologists of the time and focused on the biology and genetics of mosquitoes. Some seven doctoral-level vector biologists had been graduating from these diverse U.S. institutions each year. In general, the respondents suggested that the growth of their programs was less dynamic than in the recent past.
A smaller but comparable survey of U.S. training opportunities in public health entomology was conducted in 2002 by Walter Tabachnick at the request of the American Mosquito Control Association (personal communication). He found that 12 universities had active doctoral-level programs in the subject and that they employed 33 relevant faculty. These instructors had been producing some nine doctoral graduates in vector biology per year since 1998. A simple comparison of the Coolfont and Tabachnick surveys suggests that nearly half of the relevant programs may have been discontinued during the past 2 decades, and that the extant programs employed only half as many faculty as in 1982. Surprisingly, no diminution in doctoral graduates was evident.
Transgenesis came to dominate vector-oriented studies beginning in 1993, when a series of notable research findings was published (Aldhous, 1993). As practiced, these research efforts generally include no field component. The Special Program for Research and Training in Tropical Diseases (jointly supported by the United Nations and several other international organizations), the MacArthur Foundation, and the Burroughs Wellcome Fund, modified their funding policies in 1993 such that future grants in this discipline would be devoted to attempts to create transgenic vector insects. Although the public health usefulness of such a mosquito was then controversial (Spielman, 1994) and still remains in doubt, an aura of excitement has increasingly come to surround vector transgenesis. The proportion of the faculty that Tabachnick surveyed who were engaged in this narrowly focused aspect of the study of vector-associated disease may be quite large. In general, then, fewer university faculty in the United States appear to be prepared to investigate the transmission of vector-borne pathogens than in the recent past. The magnitude of the investment in research in vector transgenics will affect this trend.
Conclusions
A panel recently convened by the Institute of Medicine recognized that the United States now lacks the capacity to confront the health threats posed by vector-borne pathogens (Institute of Medicine, 2003). The panel concluded that the Centers for Disease Control and Prevention, the Department of Defense (DOD), the National Institutes of Health, and the
Department of Agriculture “should work with academia, private organizations, and foundations to support efforts at rebuilding the human resource capacity at both academic centers and public health agencies in the relevant sciences—such as medical entomology, vector and reservoir biology, vector and reservoir ecology, and zoonoses—necessary to control vector-borne and zoonotic diseases.”
These diverse federal agencies differ in their faculty-enhancing policies. In the past, only the NIH had sufficient resources and a commitment to investigator-initiated research to affect staffing decisions at health-related and private U.S. institutions. The influence of the USDA mainly affects land-grant institutions, and staffing decisions there respond largely to the interests of their respective state legislatures. The departments of entomology in these institutions, therefore, tend to be shaped by local interests. Funding by the CDC and the DOD has been much lower than that of the NIH, and their funds have been directed toward narrowly defined goals that have changed as the perceived need has changed. The National Science Foundation, which was not included in the IOM recommendation, at least until recently, has tended to fund basic rather than health-related research. The CDC, the DOD, and the USDA employ vector-related health scientists, but without stimulating the faculty appointments that result in their production. Therefore, the human resource capacity at U.S. universities that might be capable of dealing with vector-related issues in health would depend largely on the system of generous investigator-initiated research that resides at the NIH.
The IOM recommendation cited above omits reference to the contribution of private foundations to the human resource capacity of U.S. academe. The Gates Foundation and the Burroughs Wellcome Fund seem likely to play an important role in this dynamic. The funding policies that they pursue in the immediate future may encourage faculty to engage in insect transgenesis, insect physiology, or research relating to transmission of pathogens.
Changes in the NIH system of proposal review may impose novel constraints on health-related research on vectors conducted by the faculty of U.S. universities in the immediate future. Investigator-initiated proposals might be evaluated at the NIH in an epidemiological context in place of the biological milieu that pertained in the recent past, and the research tradition of at least some of the authors of these proposals will differ fundamentally from that of their reviewers. Faculty working in land-grant institutions, in particular, may not readily be able to address reviewers whose research tradition focuses on numerical rather than experimental applications. In addition, many of the reviewers of proposals dealing with vector transgenics will, themselves, be practitioners of that discipline. Authors of research proposals that pursue aspects of insect physiology may also find
themselves at a disadvantage. These developments seem likely to increase the numbers of funded research proposals that approach vector biology from the tradition of molecular biology. The administrators of U.S. schools of public health and of medicine, therefore, would feel constrained to plan their staffing policies accordingly.
A cohort of scientists is required who can usefully produce the next generation of public health entomologists and whose research activities will promote that goal. Their programs will strike some balance between the three entomological interests that have vied for support during the past half century—vector biology, insect physiology, and molecular biology—and their work should incorporate strong epidemiological features. Because faculty-hiring priorities are determined so strongly by the NIH system of investigator-initiated grants, a major responsibility in this regard falls on that federal agency. Participation by foundations and private donors may contribute powerfully to the outcome of this process. The characteristics of the evolving discipline of public health entomology remain to be defined.
References
Aldhous P. 1993. Malaria: Focus on mosquito genes. Science 30:605–608.
Desowitz RS. 1993. Malaria Capers: Tales of Parasites and People. New York: W.W. Norton & Company, Inc.
GAO (General Accounting Office). 1982. Malaria Control in Developing Countries: Where Does it Stand? What is the U.S. Role? Report to the Administrator for International Development, Agency for International Development, 26 April 1982. ID-82-27. Washington, DC: General Accounting Office.
Gardner MJ, Hall N, Fung E, White O, Berriman M, Hyman RW, Carlton JM, Pain A, Nelson KE, Bowman S, Paulsen IT, James K, Eisen JA, Rutherford K, Salzberg SL, Craig A, Kyes S, Chan MS, Nene V, Shallom SJ, Suh B, Peterson J, Angiuoli S, Pertea M, Allen J, Selengut J, Haft D, Mather MW, Vaidya AB, Martin DM, Fairlamb AH, Fraunholz MJ, Roos DS, Ralph SA, McFadden GI, Cummings LM, Subramanian GM, Mungall C, Venter JC, Carucci DJ, Hoffman SL, Newbold C, Davis RW, Fraser CM, and Barrell B. 2002. Genome sequence of the human malaria parasite Plasmodium falciparum. Nature 419:498–511.
Holt RA, Subramanian GM, Halpern A, Sutton GG, Charlab R, Nusskern DR, Wincker P, Clark AG, Ribeiro JM, Wides R, Salzberg SL, Loftus B, Yandell M, Majoros WH, Rusch DB, Lai Z, Kraft CL, Abril JF, Anthouard V, Arensburger P, Atkinson PW, Baden H, de Berardinis V, Baldwin D, Benes V, Biedler J, Blass C, Bolanos R, Boscus D, Barnstead M, Cai S, Center A, Chaturverdi K, Christohides GK, Chrystal MA, Clamp M, Cravchik A, Curwen V, Dana A, Delcher A, Dew I, Evans CA, Flanigan M, Grundschober-Freimoser A, Friedli L, Gu Z, Guan P, Guigo R, Hillenmeyer ME, Hladun SL, Hogan JR, Hong YS, Hoover J, Jaillon O, Ke Z, Kodira C, Kokoza E, Koutsos A, Letunic I, Levitsky A, Liang Y, Lin JJ, Lobo NF, Lopez JR, Malek JA, McIntosh TC, Meister S, Miller J, Mobarry C, Mogin E, Murphy SD, O’Brochta DA, Pfannkoch C, Qi R, Regier MA, Remington K, Shao H, Sharakhova MV, Sitter CD, Shetty J, Smith TJ, Strong R, Sun J, Thomasova D, Ton LQ, Topalis P, Tu Z, Unger MF, Walenz B, Wang A, Wang J, Wang M, Wang X, Woodford KJ, Wortman JR, Wu M, Yao A, Zdobnov EM, Zhang H, Zhao Q, Zhao X, Zhu SC, Zhimulev I, Coluzzi M, della Torre A, Roth CW, Louis C,
Kalush F, Mural RJ, Myers EW, Adams MD, Smith HO, Broder S, Gardner MJ, Fraser CM, Birney E, Bork P, Brey PT, Venter JC, Weissenbach J, Kafatos FC, Collins FH, and Hoffman SL. 2002. The genome sequence of the malaria mosquito Anopheles gambiae. Science 298:129–149.
Institute of Medicine. 2003. Microbial Threats to Health: Emergence, Detection, and Response. The National Academies Press: Washington, DC.
James AA, Beckage NE, Christensen B, Ffrench-Constant R, and Raikhel AS. 1998. Toward the Genetic Manipulation of Insects. Taos, New Mexico. Keystone Symposium, Sponsored by The John D. and Catherine T. MacArthur Foundation.
Spielman A. 1994. Why entomological antimalaria research should not focus on transgenic mosquitoes. Parasitol Today 10:374–376.
Spielman A. 2003. Research approaches in the development of interventions against vector-borne infection. J Exp Biol 206:3727–3734.
















































































































































