
5
Medical and Pregnancy Conditions Associated with Preterm Birth
ABSTRACT
A number of maternal medical conditions are associated with an increased risk of indicated or spontaneous preterm birth, including, for example, chronic hypertension, prepregnancy diabetes mellitus, and systemic lupus erythematosus. Maternal illnesses can alter or limit the placental delivery of oxygen and nutrients to the developing fetus, possibly resulting in fetal growth restriction. In addition, they can increase the risk of preeclampsia and, thus, the risk of indicated preterm birth. Therefore, acute maternal medical conditions might lead to preterm birth. Other risk factors for preterm birth are underweight and obesity. A family history of preterm birth can also be an indicator of higher risk, as can a short interpregnancy interval. Finally, the number of American women using assisted reproductive technologies to achieve pregnancies has increased, and the use of such technologies is associated with multiple gestations and the increased risk for preterm delivery. The existence of any of these risk factors for preterm birth provides a focus for understanding their causative effects and developing interventions.
A number of maternal illnesses, conditions, and medical treatments are associated with indicated or spontaneous preterm birth. Spontaneous
preterm birth naturally occurs as a result of preterm labor or preterm premature rupture of fetal membranes. In contrast, indicated preterm occurs when labor is initiated by medical intervention because of dangerous pregnancy complications. This chapter discusses several medical illnesses and conditions, such as low prepregnancy weight, obesity, a family history of spontaneous preterm birth, and short interpregnancy interval, and their relationships to preterm birth. The chapter also provides an overview of infertility treatments and the resulting risk of multiple gestations, which place women at a greater risk for preterm delivery.
MEDICAL ILLNESSES AND CONDITIONS
Indicated preterm birth appears to share a number of risk factors with spontaneous preterm birth. In a cohort of more than 2,900 pregnant women, Meis and colleagues (1998) noted a relation between indicated preterm birth and müllerian duct abnormality (OR 7.02; 95% CI 1.69– 29.15, proteinuria at less than 24 weeks of gestation (OR 5.85; 95% CI 2.66–12.89), a history of chronic hypertension (OR 4.06; 95% CI 2.29– 7.55), a history of indicated preterm birth (OR 2.79; 95% CI 1.45–5.40), a history of lung disease (OR 2.52; 95% CI 1.32–4.80), previous spontaneous preterm birth (OR 2.45; 95% CI 1.55–3.89), age greater than 30 years (OR 2.42; 95% CI 1.57–3.74), being African American (OR 1.56; 95% CI 1.02–2.40), and working during pregnancy (OR 1.49; 95% CI 1.02–2.19). With the possibility of a significant heterogeneity of risk factors and etiologic overlap, studies of preterm birth should consider indicated and spontaneous preterm births both together and separately as outcomes of interest (Savitz et al., 2005).
A number of maternal medical conditions are associated with an increased risk of indicated preterm birth (Table 5-1). Maternal medical ill-
TABLE 5-1 Examples of Maternal Medical Problems That May Lead to Indicated Preterm Birth
|
Chronic hypertension Systemic lupus erythematosus Restrictive lung disease Hyperthyroidism Pregestational diabetes mellitus Maternal cardiac disease Asthma Gestational diabetes mellitus Pregestational renal disorders Hypertensive disorders of pregnancy |
nesses such as chronic hypertension, prepregnancy diabetes mellitus, or systemic lupus erythematosus can alter or limit the placental delivery of oxygen and nutrients to the developing fetus, possibly resulting in fetal growth restriction. These same maternal medical illnesses also increase the risk of preeclampsia and, thus, the risk of indicated preterm birth. The mechanism(s) that place a woman at increased risk for preeclampsia are unknown. Acute maternal medical conditions may also result in preterm birth. For example, severe trauma and shock are acute conditions that could create a nonreassuring fetal status or placental abruption and thus lead to indicated preterm birth. The progressive course of some medical illnesses could mandate indicated preterm birth to preserve the health and well-being of the mother. Functional or structural maternal cardiac disease is an example of one such illness. Fetal conditions, such as red cell alloimmunization or a twin-to-twin transfusion sequence, might also progress to require indicated preterm birth in an effort to prevent stillbirth.
There is some evidence for a relationship between birth defects and preterm birth. Rasmussen and colleagues (2001) examined more than 250,000 infants with known gestational ages born between 1989 and 1995 in the Atlanta, Georgia, metropolitan area. Infants born at less than 37 weeks of gestation were more than twice as likely to have a range of birth defects than infants born at term, between 37 and 41 weeks of gestation (RR 2.43; 95% CI 2.30–2.56). The risk of preterm birth in infants with birth defects was 21.5 percent, whereas it was 9.3 percent in infants without birth defects. The relationship between preterm birth and birth defects was also analyzed by smaller gestational age categories (20 to 28 weeks, 29 to 32 weeks, 33 to 34 weeks, and 35 to 36 weeks). Compared to infants born at term, the risk of preterm birth was the highest for those born at between 29 and 32 weeks of gestation (RR 3.37; 95% CI 3.04–3.73). Similar results were found when the analysis was stratified by maternal age, race, and the infant’s gender. Data were not specifically provided on the proportion of births that were spontaneous versus indicated. However, the authors note that while some deliveries of babies with birth defects may have been indicated it is unlikely that these deliveries would have performed among infants in the 29 to 32 week gestational age category, unless survival of the fetus was not anticipated. In another study of 2,761 infants born alive with spina bifida between 1995 and 2001 in selected states, approximately 22 percent were born preterm and accounted for more than half of the deaths of infants with spina bifida (Bol, 2006).
In analyses provided to the Committee from the Utah Birth Defects Prevention Network, between 1999 and 2004, about 20 percent of the infants born alive with birth defects in the state of Utah were born preterm. These results are consistent with those reported by Rasmussen et al. (2001) and Bol et al. (2006). It may be that some birth defects increase the risk for
preterm birth, that some sociodemographic factors that are associated with preterm birth are also associated with some birth defects, or that the two conditions may share other maternal risk factors or medical conditions (Rasmussen et al., 2001). Further investigation is needed to understand this association.
Underweight and Spontaneous Preterm Birth
Low maternal prepregnancy weight and body mass index (BMI) have consistently been associated with preterm birth. After adjusting for confounders (previous preterm labor, previous low birth weight, standing at work >2 hours, abruptio placentae, urinary tract infection and stress score >5), Moutquin (2003) noted that women with BMIs of less than 20 were nearly four times as likely as heavier women to have a spontaneous preterm birth (OR 3.96; 95% CI 2.61–7.09). Indeed, the relationship between low prepregnancy BMI and spontaneous preterm birth is consistent (OR 1.7– 3.9) among North American caucasians (Moutquin, 2003), blacks (Johnson et al., 1994), and urban Latinas (Siega-Riz et al., 1994, 1996).
A low BMI also modifies the contribution of low pregnancy weight gain to the risk of preterm birth (Schieve et al., 2000). Compared with normal-weight women (BMI 19.8–26.0) with adequate weight gain during pregnancy (0.5–1.5 kg/week), the risk of spontaneous preterm birth at less than 37 weeks of gestation is sixfold greater for underweight women (BMI < 19.8) with poor pregnancy weight gain (< 0.5 kg/week) and threefold greater for normal-weight women with poor pregnancy weight gain.
A randomized trial of treatment for bacterial vaginosis (BV) examined the incidence of preterm delivery in at-risk women, including those who were underweight (Hauth et al., 1995). Women who had a previous spontaneous preterm birth or a prepregnancy weight of less than 50 kilograms (N = 624) were randomly assigned to metronidazole and erythromycin antibiotic therapy or placebo. Among the 258 women with BV, a lower rate of preterm delivery in those assigned to the treatment group was observed for women who weighed less than 50 kilograms (N = 81). The incidence of preterm birth was 33 percent in the placebo group and 14 percent in the antibiotic-treated group (p = 0.04). This is in contrast to the findings of several investigators who demonstrated that treatment of BV in a general obstetric population is ineffective (Carey et al., 2000).
Obesity and Spontaneous Preterm Birth
In a cohort of more than 70 percent white women, Sebire and colleagues (2001) noted a decreased frequency of delivery at less than 32 weeks of gestation among women with BMIs greater than or equal to 30 (OR
0.73; 95% CI 0.65–0.82) compared with that among women with BMIs less than 30. Those investigators did not differentiate spontaneous from indicated preterm birth.
In a recent secondary analysis from the National Institute of Child Health and Human Development MFM Units Network Preterm Prediction study, in which 65 percent of the sample was African American, Hendler and colleagues (2005) found a decreased odds of spontaneous preterm birth at less than 37 weeks of gestation among women with prepregnancy BMIs greater than or equal to 30 (OR 0.57; 95% CI 0.39–0.83) compared with that among women with BMIs less than 30.
Even though obesity is detrimental for numerous aspects of human health and disease, high BMIs are associated with better outcomes of both congestive heart failure and atherosclerotic heart disease among people with chronic renal disease (Beddhu, 2004; Kalantar-Zadeh et al., 2004). It has been hypothesized that these epidemiological paradoxes may be the result of obesity-related changes in systemic inflammation (Beddhu, 2004; Kalantar-Zadeh et al., 2004).
Family History and Spontaneous Preterm Birth
Several observations support the hypothesis that spontaneous preterm birth is influenced by a family history of preterm birth. First, evidence from two studies performed with twins suggests a genetic predisposition for preterm birth with estimates of the proportion of preterm births among women with a family history of preterm birth ranging from 20 to 40 percent (Blackmore-Prince et al., 2000; Fuentes-Afflick and Hessol, 2000). Other observations support the idea that genetic factors affect the risk of preterm birth: (1) the leading risk factor for preterm birth is a previous preterm birth (James et al., 1999; Klerman et al., 1998; Shults et al., 1999); (2) an association between race-ethnicity and preterm birth persists in some instances, even if it is corrected for socioeconomic condition (Ekwo and Moawad, 1998); and (3) mothers who were preterm themselves (Basso et al., 1998) or who have a sister who had delivered an infant preterm (Kallan, 1997) have an increased risk of delivering their infants preterm.
Short Interpregnancy Interval and Preterm Birth
Interpregnancy interval is defined as that interval between the termination of one pregnancy and the conception of another. Numerous investigators have found a univariate association between short interpregnancy interval and a number of adverse perinatal outcomes, including preterm birth, low birth weight, and stillbirth (Adams et al., 1997; Al-Jasmi et al., 2002; Basso et al., 1998; Blackmore-Prince et al., 2000; Brody and Bracken, 1987; Conde-Agudelo et al., 2005; Dafopoulos et al., 2002; Ekwo and Moawad,
1998; Erickson and Bjerkedal, 1978; Ferraz et al., 1988; Fuentes-Afflick and Hessol, 2000; Hsieh et al., 2005; Kallan, 1992, 1997; Klebanoff, 1988; Lang et al., 1990; Miller, 1994; Rawlings et al., 1995; Shults et al., 1999; Smith et al., 2003; Zhu and Le, 2003; Zhu et al., 2001). These published reports did not distinguish spontaneous from indicated preterm birth, however. The definition of short interpregnancy interval varies widely across studies; the most common definition is less than or equal to 6 months.
Impacts of Ethnicity and Geography
The relationships between short interpregnancy interval and preterm birth, low birth weight, and small-for-gestational age birth have been noted to be similar in magnitude and significance for African American and white women (James et al., 1999; Kallan, 1992, 1997; Zhu et al., 2001). Most studies have found that the prevalence of short interpregnancy intervals is higher among African American women than white women (James et al., 1999; Kallan, 1992, 1997; Zhu et al., 2001), but others have not found such a higher prevalence (Kallan, 1992; Klerman et al., 1998). International studies have shown that a short interpregnancy interval has been associated with preterm birth in rural Greece, the Philippines, the United Arab Emirates, and Latin America (Blackmore-Prince et al., 2000; Conde-Agudelo et al., 2005; Lang et al., 1990; Zhu et al., 2001).
Magnitude of Effect
The magnitude of the increased risk for preterm birth with an interpregnancy interval of less than 6 months is estimated to be 30 to 60 percent (Kallan, 1997). A single report has suggested that the magnitude and the significance of a short interpregnancy interval are the greatest when the index pregnancy was a preterm birth rather than a term birth (Hsieh et al., 2005).
Role for Intervention
Klebanoff (1988) notes that a short interpregnancy interval is primarily a marker for a woman who is otherwise at high risk of delivering her infant preterm and that modification of that interval alone may be unlikely to have a major impact on low birth weight. Other investigators also support the notion that a short interpregnancy interval may function as a marker of other risk factors rather than exerting an independent effect on preterm birth (Brody and Braken, 1987; Erickson and Bjerkedal, 1978). This concept may be extended to the impact of a short interpregnancy interval on low birth weight. In a Brazilian study, the effect of a short interpregnancy
interval on low birth weight was explained by an increased prevalence of underweight among women with short interpregnancy intervals (Ferraz et al., 1988). In the general obstetric population at low risk for adverse pregnancy outcomes, Adams et al. (1997) found that short interpregnancy intervals are rare and are weak risk factors among low-risk women, and thus, efforts to lengthen interpregnancy intervals are unlikely to reduce substantially the rates of adverse pregnancy outcomes among these women. Smith et al. (2003) estimated the attributable risk fractions of a short interpregnancy interval of less than 6 months to preterm birth at 24 to 32 weeks and 33 to 36 weeks of gestation to be 6 and 4 percent, respectively. In a largely African American cohort of women, Blackmore-Prince et al. (2000) found that the median interpregnancy interval was 15 months (range, 1 to 207 months), with 19 (4 percent) of the women having interpregnancy intervals of less than 3 months. After adjustment for parity, gestational age (in weeks), and smoking status, the mean birth weight associated with an interpregnancy interval of 3 or more months was 3,106 grams, 215 grams greater than that for an interpregnancy interval of less than 3 months (p = 0.06).
INFERTILITY TREATMENTS AND PRETERM BIRTH
Infertility treatments have allowed thousands of couples who have difficulty conceiving to fulfill their desire to have children. In the United States in 2002, 7.3 million women, or 12 percent of women ages 15 to 44, had physical difficulty becoming pregnant or carrying a baby to term. Approximately 2.1 million of these women, or 7 percent of all women between the ages of 15 and 44, were infertile, defined as not becoming pregnant after 12 months when the couple is not using contraception (CDC, 2002b). Two percent of women had had an infertility-related medical appointment within the previous year, and an additional 10 percent reported that they had received services for infertility at some point in their lives.
The use of infertility treatments has risen dramatically in the past 20 years and has been associated with the trend to delay childbearing (see Chapter 1). In 2002, 33,000 American women delivered babies as a result of the use of infertility procedures; this is more than twice the number who had done so in 1996 (Meis et al., 1998). More than 50 percent of these women were 35 years of age or older. In recent years, an unintended consequence of the use of these technologies, multiple gestations and the increased risk for preterm delivery, has become a focus of attention. There is also evidence that a portion of the reported association between infertility treatments and preterm birth may be attributable to the underlying biological reasons for infertility and subfecundity (long time to becoming pregnant) (Basso and Baird, 2003; Henriksen et al, 1997; Joffe and Li, 1994).
Henriksen and colleagues (1997) examined pregnancy outcomes for two cohorts of approximately 13,000 deliveries in Denmark. The analyses excluded women with chronic illness, multiple fetuses, and unplanned pregnancies. Compared to women who took 6 or less months to conceive before becoming pregnant, women who tried for 7 to 12 months to conceive had a higher adjusted risk (1.3 times) for preterm delivery (95% CI .8–2.1) in both cohorts. Those who tried for 12 months or longer had an adjusted risk of 1.6 (95% CI 1.1–2.2) in the first cohort and 1.7 in the second (95% CI 1.1–2.6). Results held after controlling for infertility treatments.
This section provides an overview of infertility treatments, including Assisted Reproductive Technologies (ARTs) and ovulation promotion procedures, trends in their use and the resulting pregnancies, maternal and child outcomes, and current regulations on the use of these treatments.
Types of ART-Related Treatments and Incidence of Pregnancies Conceived by Use of ART
The Centers for Disease Control and Prevention (CDC) defines ARTs as procedures in which the egg and the sperm are handled in the laboratory, including in vitro fertilization (IVF) as well as related procedures, such as intracytoplasmic sperm injection (ICSI) and gamete intrafallopian transfer (GIFT) or zygote intrafallopian transfer (ZIFT) (Table 5-2). Since 1996, the federal government has mandated that all clinics performing procedures involving ARTs report their outcomes to the CDC (Meis et al., 1998).
TABLE 5-2 Procedures Involving ARTs Defined by the CDC
|
Treatment |
Procedure |
|
In vitro fertilization (IVF) |
Extraction of the woman’s eggs, fertilization of the eggs in the laboratory, and transfer of the resulting embryos into the woman’s uterus; may include intracytoplasmic sperm injection (ICSI), in which a single sperm is injected directly into the egg |
|
Gamete intrafallopian transfer (GIFT) |
Use of laparoscope to guide the transfer of unfertilized eggs and sperm into the fallopian tubes through incisions in the abdomen |
|
Zygote intrafallopian transfer (ZIFT) |
Fertilization of an egg in the laboratory and use of a laparoscope to guide the transfer of the fertilized eggs into the fallopian tubes |
|
SOURCE: CDC (2003d). |
|
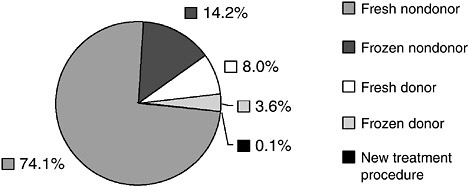
FIGURE 5-1 Types of ART procedures used in the United States, 2003.
SOURCE: CDC (2005f).
ARTs can use a woman’s own egg (nondonor egg) or another woman’s egg (donor egg). Some eggs are newly fertilized (fresh eggs) or previously fertilized, frozen, and then thawed (frozen eggs). Figure 5-1 depicts the frequency with which procedures involving ARTs were used in the United States in 2003. The majority of the procedures (nearly three-quarters of the cycles of ART) used fresh nondonor eggs. Of those procedures involving fresh nondonor eggs, approximately 44 percent used traditional IVF and another 56 percent used IVF with ICSI. Concern has been raised about the use of ICSI (see section below on Maternal and Child Risks). A small proportion of procedures used GIFT, ZIFT, or a combination of procedures (Figure 5-2).
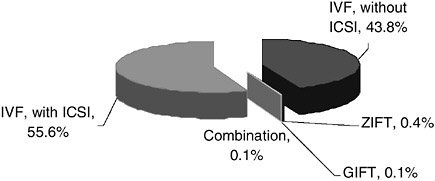
FIGURE 5-2 Types of ART procedures performed with fresh nondonor eggs or embryos, 2003.
SOURCE: CDC (2005f).
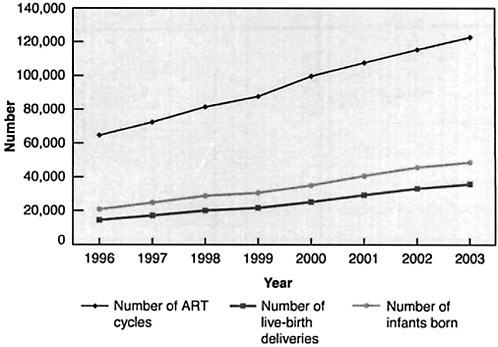
FIGURE 5-3 Numbers of ART cycles performed, live-birth deliveries, and infants born as a result of the use of ARTs, 1996 to 2003.
SOURCE: CDC (2005f).
The rate of use of ARTs has increased significantly in the past several years (Figure 5-3). Between 1996 and 2003, the number of cycles of ART nearly doubled from 64,681 to 122,872. The number of live births resulting from conceptions achieved by the use of ARTs more than doubled from 14,507 to 35,785. Because of the number of multiple births per delivery, the actual number of infants born is greater than the number of deliveries. In 2003, 48,756 infants were born as a result of the use of ARTs, whereas 20,840 were born in 1996.
Although the use of ARTs must be reported, this is not the case with other fertility treatments not classified as ARTs. The CDC definition of an ART does not include treatments in which only sperm are handled (i.e., intrauterine insemination, which is also known as artificial insemination) or procedures in which a woman takes medication to stimulate egg production without the intention of having the eggs retrieved. Superovulation with or without intrauterine insemination is used to improve fertility, but the frequency of use of this technique and the number of births attributable to the use of this technique are unknown. This is an important gap in current knowledge.
Disparities in Infertility Treatment
As discussed in Chapter 4, socioeconomic differences in multiple gestations have not been well studied (Kramer et al., 2000). The literature on infertility, utilization of treatment, and outcomes of treatment has been focused on white and socieconomically advantaged populations. While the extent to which various racial-ethnic minority populations and subpopulations experience fertility problems is not precisely known, a series of recent reports developed from a workshop, Health Disparities in Infertility, began to shed light on infertility problems among racial-ethnic minority populations (Berkowitz and Davis, 2006). This workshop was sponsored by the National Institute of Child Health and Human Development, Office of Behavioral and Social Sciences Research, and Office of Research on Women’s Health of the National Institutes of Health, and Agency for Healthcare Research and Quality.
In an effort to assess whether racial-ethnic or socioeconomic disparities exist in infertility, impaired fecundity, or infertility treatment, Bitler and Schmidt (2006) analyzed data from the National Survey of Family Growth. The authors reported that infertility was more common for Hispanic, non-Hispanic black, and non-Hispanic women of other races than for non-Hispanic white women. In addition, results suggested disparities by educational attainment. Non-college educated women were more likely to experience problems with infertility and impaired fecundity than women with 4-year college degrees. Despite a higher likelihood of fertility problems for minority and socioeconomically disadvantaged women, these women were less likely to have ever received infertility treatment. Further, state-level infertility insurance mandates (currently in place in 15 states) did not ameliorate these disparities. Within a population of women receiving ART services in the military health care system, clinically significant differences in the live birth rate and statistically significant differences in spontaneous abortions were observed between African American and white women (Feinberg et al., 2006). The authors speculate that this may be due, in part, to higher prevalence of leiomyomas (benign uterine tumors) in the African American women. Other investigations also revealed delayed time to seeking treatment in African American women (Jain, 2006), and economic barriers to care seeking in Arab American (Inhorn and Fakih, 2006) and Latinas women (Becker et al., 2006).
The study by Becker and colleagues also suggests that Latino women raised in the United States may be more likely to seek care, compared with Latino women raised elsewhere. Continued research to understand disparities in infertility, infertility treatment, and outcomes of treatment including multiple gestations and preterm birth is needed.
RISK FOR MULTIPLE GESTATIONS ARTs
Multiple gestations are more common as a result of assisted reproduction than as a result of natural conception because of the transfer of multiple embryos and a higher incidence of spontaneous twinning with any single embryo. The risk of monozygotic twinning after implantation of a single embryo appears to be increased in pregnancies conceived by IVF compared with the rate during spontaneous conceptions; however, this risk is relatively low, with only a 1 to 2 percent chance of having twins with implantation of a single embryo (Adashi et al., 2004). Therefore, the major cause underlying the increased risk of multiple births as a result of the use of ARTs is the number of embryos transferred. Results from a recent study suggest that IVF with a single blastocyst-stage embryo (at 5 days) versus the typical transfer with an embryo at the cleavage stage (3 days) in women under age 36 results in a higher rate of pregnancy and delivery. Of the two cases of multiple pregnancies, both occurred in the cleavage stage group (Papanikolaou et al., 2006).
National data indicate that in the United States, the majority of ART cycles involve the transfer of more than one embryo, with more embryos transferred as maternal age increases. In 2003, for women under age 35, an average of 2.6 fresh nondonor eggs were transferred per cycle (CDC, 2003d). For women ages 35 to 37, 38 to 40, and 41 to 42, the average numbers of embryos transferred were 2.9, 3.1, and 3.5, respectively. As the techniques involving ARTs have improved, the relationship between the number of embryos transferred and the achievement of a successful live birth is less clear. With the exception of women older than 40 years of age, there appears to be no improvement in the rates of live births when two or more embryos are transferred. Evidence suggests that for women under age 35, the transfer of more than two embryos is not associated with an increased likelihood of conception (Filicori et al., 2005). The transfer of more than two embryos in women over age 40, however, may prove beneficial, as it may result in a successful pregnancy, with fewer risks of multiple gestations (Filicori et al., 2005).
There is a direct relationship between the rise in the use of assisted reproduction and the increase in the numbers of multiple gestations. Fiftythree percent of 45,751 infants born in the United States as a result of the use of ART in 2002 were part of multiple gestations. Although approximately 1 percent of the infants born were conceived through the use of ARTs, these infants represented 0.5 percent of all singleton births and 17 percent of all multiple births. Sixteen percent of twins and 44 percent of
higher-order multiple births were conceived by the use of ARTs (CDC, 2005g).
Ovulation Promotion
Much of the focus on the causes of multiple gestations has been placed on the role of ARTs, particularly IVF. Much less attention has been paid to the role of ovulation promotion (superovulation or intrauterine insemination and conventional ovulation induction), which is equally important in terms of its contribution to multiple gestations. The risk of multiple gestations secondary to infertility treatments such as ovulation stimulation with injectable hormones is less well documented, as the collection of data on the frequency of use of these treatments is not mandated. Nonetheless, limited data suggest that these treatments may be associated with an even higher risk of multiple gestations than IVF and ICSI, particularly if the number of developing oocytes is not monitored during the cycle (Adashi et al., 2004).
In 2000, ovulation promotion accounted for 21 percent of twin births, whereas IVF accounted for 12 percent (Figure 5-4) (Reynolds et al., 2003). Ovulation promotion was implicated in 40 percent of higher-order multiple births (Figure 5-5). Forty-two percent of these higher-order multiple births were the result of IVF, whereas 18 percent occurred spontaneously.
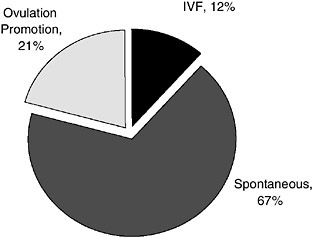
FIGURE 5-4 Contributions (percent) of IVF and ovulation promotion to twin births: 2000.
SOURCE: Reynolds et al. (2003). Reprinted from American Journal of Obstetrics and Gynecology, Vol. 190, Pg. 887, © 2004, with permission from Elsevier.
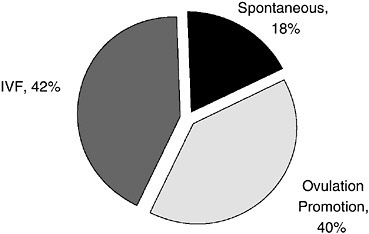
FIGURE 5-5 Contributions (percent) of IVF and ovulation promotion to higherorder multiple births: 2000.
SOURCE: Reynolds et al. (2003). Reprinted from American Journal of Obstetrics and Gynecology, Vol. 190, Pg. 887, © 2004, with permission from Elsevier.
Finding 5-1: The prevalence of the use of superovulation with or without artificial insemination is unknown, and no systematic mechanisms are in place to collect these data.
ARTs and Preterm Birth
The primary concern regarding the use of ARTs and ovulation promotion is the risk of preterm delivery that is associated with multiple gestations. For twins, the average gestational age at delivery is approximately 35 weeks, with 58 percent of these deliveries occurring before term (37 weeks of gestation) and with more than 12 percent occurring before 32 weeks of gestation (CDC, 2003d) (Figure 5-6). The risks are even greater for higherorder multiple births. The mean gestational ages of triplets, quadruplets, and quintuplets and higher-order multiples were 32.2, 29.9, and 28.5 weeks, respectively. More than 90 percent of triplets were born at less than 37 weeks of gestation, and approximately 36 percent were born at less than 32 weeks of gestation.
Among the infants conceived through the use of ARTs specifically, 14.5 percent of singleton births, 61.7 percent of twin births, and 97.2 percent of higher-order multiple births were born at gestational ages of less than 37 weeks (CDC, 2005f).
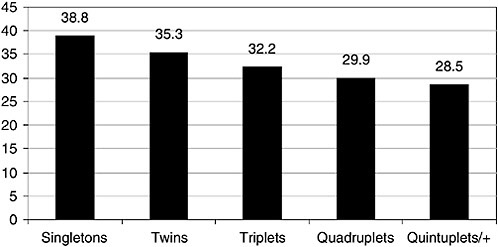
FIGURE 5-6 Mean gestational age (weeks) by number of infants born, United States, 2002.
SOURCE: CDC (2003d).
Singletons Conceived Through ARTs and Preterm Birth
Singletons conceived through the use of IVF are twice as likely to be born preterm and die within 1 week of birth than those not conceived through IVF and 2.7 times more likely to have a low birth weight (Hampton, 2004). A meta-analysis that compiled information from 12,283 singleton births conceived through the use of IVF and 1.9 million spontaneously conceived singleton births noted a twofold increase in the risk of preterm delivery (Jackson et al., 2004). Similarly, the results of a meta-analysis conducted by McGovern and colleagues (2004) found that singleton pregnancies resulting from IVF (embryo transfer) and GIFT were twice as likely as naturally conceived singletons to be delivered preterm. The etiology of this type of preterm birth remains unknown. Recent evidence suggests the possibility of placentation problems in ART pregnancies. A study from the First And Second Trimester Evaluation of Risk trial examined whether the use of ART was associated with an increased risk of chromosomal abnormalities, fetal malformations, or adverse pregnancy outcomes among singleton births (Shevell et al., 2005). Approximately 95 percent of patients did not use any form of ART, 3.4 percent used ovulation induction, and 1.5 percent received IVF treatment. Results indicate that patients who used ovulation induction had an increased risk of placental abruption (OR 2.4; 95% CI 1.3–4.2) and fetal loss after 24 weeks (OR 2.1; 95% CI 1.3–3.6) compared to women who did not receive ART. Patients who used IVF were more likely to develop preeclampsia (OR 2.7; 95% CI 1.7–4.4) have a placental
abruption (OR 2.4; 95% CI 1.1–5.2), placenta previa (OR 6.0; 95% CI 3.4–10.7), and undergo a cesarean delivery (OR 2.3; 95% CI 1.8–2.9) compared to women who did not undergo ART. There was no association between ART and fetal growth restriction, aneuploidy, or fetal anomalies after adjusting for a number of sociodemographic and health variables.
Finding 5-2: Fertility treatments are a significant contributor to preterm birth among both multiple and singleton pregnancies.
Finding 5-3: The mechanisms by which conditions of infertility, subfertility, and fertility treatments increase the risk of preterm birth, particularly among singleton pregnancies, are unknown. The mechanisms may be markedly different from the mechanisms suggested when racial and socioeconomic causes of preterm birth are considered.
Maternal and Child Risks
The use of ARTs and ovulation promotion has raised concern about potential risks to the women who undergo these procedures and the children who are conceived as a result. Some investigators have speculated about the effects of fertility drugs on the risk of breast cancer and cancers of the reproductive system. A study by Klip and colleagues (2000), in which a cohort of women in the Netherlands was monitored for 5 to 8 years, found no increase in the risk of breast cancer or ovarian cancer in women who underwent IVF compared with that in subfertile women who had not undergone IVF. The study also found that both women who had undergone IVF and subfertile women did not have an increased risk for endometrial cancer. The authors suggest a potential link between endometrial cancer and subfertility.
Other risks associated with hormonal ovulation stimulation include ovarian hyperstimulation syndrome, in which fluid imbalances and ovary enlargement become problematic; rupture of the ovaries is also a possibility (for a review of the well-being of women during the use of ARTs, see The President’s Council on Bioethics [2004]). Multiple pregnancies pose higher risks of mortality and morbidity to the mothers than singleton pregnancies. Mothers with multiple pregnancies are more likely to experience high blood pressure, anemia, preeclampsia, and gestational diabetes and to require delivery by cesarean (Sebire et al., 2001; Wen et al., 2004).
Of central interest in the discussion of the unintended consequences of the use of ARTs is the well-being of the children conceived through the use of these procedures. Although large-scale and long-term followup studies of these children are lacking, recent evidence associates some
ART procedures with certain birth defects as a result of defects in DNA methylation, such as Beckwith-Wiedemann syndrome, retinoblastoma, and Angelman syndrome (Jacob and Moley, 2005; Niemitz and Feinberg, 2004). However, the prevalence of these conditions is extremely low. Concern has been raised about the use of intracytoplasmic sperm injection, as this procedure impedes the ovum’s natural ability to resist fertilization by a sperm that would otherwise not have the ability to fertilize the egg. However, these risks are considered small, and the greater risk from the use of these procedures results from the consequences of multiple gestations.
Reducing Rates of Multiple Gestation
Nationally, the rate of birth of live twins has continued to increase (Figure 5-7), whereas the rate of birth of live triplets has leveled off since 1998 (Figure 5-8). For births that specifically result from the use of ARTs, the percentage of twin deliveries per ART cycle with fresh nondonor eggs or embryos remained essentially unchanged from 1996 to 2003 (31.4 to 31.0 percent). During this period, the percentage of triplets decreased from 7.0 to 3.2 percent (CDC, 2005f). Despite this trend, the number of multiple deliveries in the United States continues to be a problem and is of concern.
The oversight of ART practices currently occurs at both the governmental (federal and state) and nongovernmental levels, and both govern-
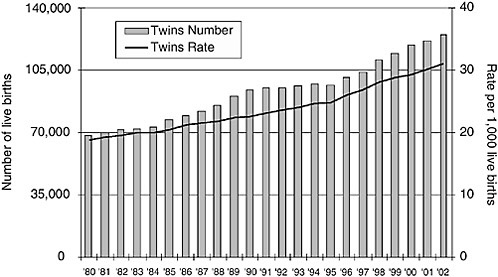
FIGURE 5-7 Trends in live twins births, 1980 to 2002, United States.
SOURCES: CDC (1999a,b, 2002a, 2003b).
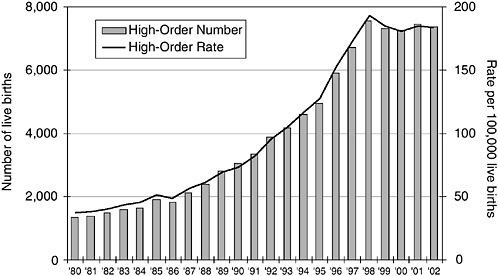
FIGURE 5-8 Trends in live high-order births, 1980 to 2002, United States.
SOURCES: CDC (1999a,b, 2002a, 2003b).
mental and nongovernmental entities also provide the public with guidance on such practices. For a more detailed overview of the goals, scope, requirements, mechanisms, and efficacy of ART-related policies, the reader is referred to Reproduction and Responsibility: The Regulation of New Biotechnologies (The President’s Council on Bioethics, 2004). The Fertility Clinic Success Rate and Certification Act of 1992 was designed to provide consumers with reliable information about the services provided by and the success rates of fertility clinics throughout the United States. Data are reported by the Society for Assisted Reproductive Technology (SART) and are published by the CDC. This act also provides states with a standard process for the accreditation of embryo laboratories. In most states, the states oversee access to services and determine whether and to what extent those services are covered by health insurance. Other states address the prevention of abuse by practitioners and regulate gamete and embryo donations.
Nongovernmental guidance on the practice of ART has come primarily from the American Society for Reproductive Medicine (ASRM) in conjunction with SART. In 1999, ASRM issued guidelines that recommended limiting the number of embryos transferred to no more than two in young women in their first cycle of IVF if sufficient embryos were available for cryopreservation (Barbieri, 2005). A demonstrable drop in the rate of triplet gestations from 7 to 3.8 percent from 1996 to 2002 has been cited as
evidence of the success of these practice guidelines (Barbieri, 2005). It is noted that a decrease in the number of triplet live births may be due to factors other than reducing the number of embryos transferred. For example, a distinction should be made between triplet live births and the percent of triplets detected with heart beats since a discordance may exists as a consequence of the use of multifetal reduction. ASRM further refined these guidelines in 2004, recommending the transfer of a single embryo for young women less than 35 years of age with favorable prognoses (PC of SART and ASRM, 2004). The recommendations become less restrictive as maternal age advances and suggest the transfer of no more than two embryos to women with favorable prognoses between the ages of 35 and 37 years and no more than three embryos in women with favorable prognoses between the ages of 38 and 40 years. Transfer of an additional embryo is suggested if an unfavorable prognosis exists. For women over age 40, the recommended limit to the numbers of embryos transferred is no more than five.
Despite the successes in reducing the rates of higher-order multiple births, the United States does not fare as well as European countries in minimizing the risk of multiple gestations (Anderson et al., 2005). The most recent figures released by the European Society of Human Reproduction and Embryology (ESHRE) reported an overall multiple gestation rate of 25.5 percent among pregnancies conceived by the use of ARTs in 2001, when the U.S. ART-related multiple gestation rate was twice that level. Twenty-four percent of European pregnancies conceived by the use of ARTs resulted in twins, and only 1.5 percent resulted in triplets or higher-order multiple births. By 2001, the United States halved its rate of higher-order multiple births to 3.8 percent, but Europe reduced the rate by nearly 60 percent to a low of 1.5 percent. Furthermore, whereas over half of all U.S. ART cycles involve the transfer of three or more embryos, in Europe over 60 percent involve the transfer of only one embryo (12 percent) or two embryos (51.7 percent). A lower number of embryos transferred may result in lower success rate per cycle, especially in women over 40 years. However, continued progress is being made toward addressing the problem of multiple gestations. A recent study examined the results of approximately 200 IVF cycles in which patients had either one or two embryos transferred. Results revealed similar implantation and live birth rates and a significant reduction in the number of twins conceived with single embryo transfer (Criniti et al., 2005).
The international difference in the rates of multiple gestations may reflect the more stringent guidelines regarding the number of embryos transferred. As early as 1993, the Swedish health organizations recommended reductions in the number of embryos transferred from three to two per cycle (Källén et al., 2005). Subsequent voluntary reduction on the part of ART providers virtually eliminated the risk of triplets without low-
ering the rate of live births (NBHW, 2006). Currently, public funding of ART cycles in Sweden covers only the transfer of single embryos, which has resulted in an even further reduction in multiple gestations. ESHRE guidelines on the recommended number of embryos to be transferred emphasize the elective transfer of a single embryo for women up to 36 years of age if at least one good-quality embryo has been produced. However, there is no scientifically-based definition of what a good quality embryo is and how this can be measured objectively, which affects decisions about which and how many embryos to transfer.
Additional support for single-embryo transfer (SET) comes from a recently published randomized controlled trial comparing two cycles of SET with one cycle of double-embryo transfer (DET) (Lukassen et al., 2005). Two cycles of SET were equally effective in achieving a live birth as a single cycle of DET, with similar costs through 6 weeks postpartum. The investigators estimated that if the lifetime costs of caring for handicapped preterm survivors are included, SET will result in a savings of 7,000 pounds per live birth. The investigators noted that in countries where ART regulation is the strictest, the fee structure supports the use of SET (Ombelet et al., 2005; Papanikolau et al., 2006; Thurin et al., 2004).
The challenge of reducing multiple gestations is also a sensitive and personal issue. The rights and autonomy of patients, the autonomy of providers, and the public good are forces that must be considered (Adashi et al., 2004). Patients may not be rigorously apprised of the risks of multiple gestations or may accept the risks in their desire to conceive. Ovulation enhancement has proceeded without formal guidelines, and advanced training and certification is not required for its practice. With IVF, providers must weigh the goal of a successful singleton pregnancy outcome with the inability to predict the success of implantation of any given embryo. Payers are largely uninvolved in the discussion of the challenge of the risk of multiple gestations. Although some payers underwrite ovulation enhancement, most do not underwrite IVF, the outcome of which is more predictable than that of ovulation enhancement and which results in a lower rate of multiple births. This may be because payers have not been thoroughly informed about the financial consequences of higher-order multiple births.
In an effort to decrease the number of multiple births related to IVF, the Belgian government, in 2003, agreed to reimburse laboratory expenses for the first six IVF trials in women up to age 42. In exchange, restrictions are placed on the number of embryos transferred, depending on the age of the woman (Gordts et al., 2005; Ombelet et al., 2005). For example, in women under 36, single embryo transfer is performed in the first trial and in the second (if high quality embryos are available). Thereafter a maximum of two embryos are transferred. Data reveal that after this policy was instituted, the percentage of singe embryo transfers increased, and overall preg-
nancy rates did not differ. Twin pregnancies were reduced from 19 percent to 3 percent (Gordts et al., 2005).
Stricter guidelines on the number of embryos transferred should be emphasized by a number of U.S. professional organizations and not just ASRM. Similar best-practice guidelines should be outlined for other infertility treatments that use ARTs, such as ovulation induction. Such guidelines should recommend the use of strict ultrasound guidance and abandonment of a cycle if too many follicles develop. Policy makers should mandate the more systematic collection of data on such procedures and should also consider recommending the use of medication to stimulate egg production. Professional organizations and surveillance activities should redefine success as singleton live births (rather than pregnancy rates). Efforts to reeducate ART consumers on the risks of multiple gestation and preterm birth must transpire simultaneously. Other policies regarding access to assisted reproduction should also be further explored.
Access to reproductive health care and reproductive technology may be a double-edged sword when it comes to ARTs. States with legally mandated coverage for infertility treatment, including ARTs, were the states with the highest rates of ART procedures per million population (Massachusetts, New Jersey, Maryland, the District of Columbia, and Rhode Island) (CDC, 2002b). In Massachusetts, a rise in the state’s rate of multiple births can be directly linked to mandated insurance coverage of infertility services (CDC, 1999a). Sweden and Belgium exemplify a contrasting approach, with public funding limited to the coverage of only SET cycles, thus freeing infertile couples from the financial pressure to transfer as many embryos as possible.





















