
2
Food Safety Oversight
OVERVIEW
In the United States, the oversight of food safety at the national level presently involves at least 12 agencies,1 of which 4 predominate: the U.S. Department of Agriculture (USDA), the Food and Drug Administration (FDA), the Environmental Protection Agency (EPA), and the National Marine Fisheries Service. Many of the more than 70 agreements intended to coordinate food safety activities among federal agencies are not fully implemented or enforced, resulting in considerable waste, confusion, and inefficiency. Therefore, it is not surprising that over the past six decades more than 20 proposals have advocated a reorganization of the federal food safety system. Prominent among these calls for reform was a 1998 report of the Institute of Medicine (IOM) and National Research Council (NRC), entitled Ensuring Safe Food from Production to Consumption that recommended the integration of food safety oversight into a single, independent agency (IOM/NRC, 1998). In the first paper in this chapter, Dr. John Bailar, chairman of the study committee, discusses the committee’s findings and considers why little progress has been made toward implementing the report’s recommendations in the seven years since its publication.
The subsequent contribution by Dr. Jørgen Schlundt, director of the food safety program of the World Health Organization (WHO), offers a global perspective on the burden of foodborne illness and progress toward the development of international systems to respond to foodborne outbreaks. WHO has assumed a central role in global food safety through its organization of Global Salm-Surv, a network linking Salmonella surveillance efforts in 141 countries, and the International Food Safety Authorities Network (INFOSAN), which disseminates information related to food safety. Pending forthcoming revisions to the international health regulations due to take effect in 2007, WHO will serve as the hub of a global system for reporting public health emergencies including foodborne illness.
Although each country needs to defend its food supply from deliberate contamination, Schlundt maintains that these efforts should be undertaken as part of a comprehensive food safety agenda that extends to the international level. The WHO Global Strategy for Food Safety takes a largely preventive approach, combining surveillance, communication among all stakeholders, and rapid response to foodborne outbreaks. Rather than rely on food testing to intercept contaminated products, the inherent inefficiency of which Schlundt demonstrates, WHO seeks to build capacity for safe food production and outbreak detection and alert, particularly in developing countries in recognition of their increasing contribution to global food trade.
THE U.S. FOOD SAFETY SYSTEM
John Bailar, M.D., Ph.D.2
Professor Emeritus, University of Chicago
The focus of my remarks to the Forum on Microbial Threats was the 1998 report entitled Ensuring Safe Food from Production to Consumption (IOM/NRC, 1998). That report was issued by a committee assembled jointly by the Institute of Medicine and the National Research Council, which I chaired, and which included at least three participants in this workshop: Lonnie King, Sanford Miller, and Michael Osterholm. My brief presentation, summarized below, described the long-recognized need for a complete overhaul of the U.S. food safety system, including the integration of widely scattered responsibilities for food safety oversight into a single, independent federal agency.
How the System Falls Short
The problems that must be addressed by the U.S. food safety system were discussed in detail in several workshop presentations (see Summary and Assessment,
as well as Osterholm in Chapter 1, Tauxe in Chapter 3). Briefly, they include the tens of millions of cases, the thousands of deaths, and the billions of dollars lost every year because of foodborne illness, as well as the possibility of deliberate harm to our food system. To address these challenges, we have a food safety system that involves at least 12 different agencies (of which four have major responsibilities) that conduct monitoring, surveillance, inspection, enforcement, outbreak management, research, and education. These agencies work under a total of 35 food safety-related statutes and more than 50 interagency agreements and working groups; they report to a total of 28 House and Senate committees. A variety of federal-state programs, international treaties and agreements, and voluntary programs are also involved in ensuring food safety.
Clearly, there is an absence of focused leadership in food safety oversight. The federal agencies that share responsibility for food safety are poorly integrated, as are federal, state, and local food safety agencies. Moreover, each federal agency with food safety responsibilities has other missions that are generally regarded as more important. This situation has numerous and serious repercussions: surveillance of known, existing problems is inadequate; food safety standards are inconsistent, uneven, and archaic; resources available for food safety are lacking; consumers have limited knowledge about food safety; and there is poor adherence to even the minimum food safety standards currently in place.
The lack of integration and clear leadership among federal agencies responsible for food safety is demonstrated in Table 2-1, which lists the various offices and agencies involved in ensuring the safety of various food categories and contaminants through monitoring and surveillance, risk assessment, research, inspection and enforcement, and education. None of the four major elements of food safety—type of hazard, food category, nature of activity, or program responsibility—lines up with any of the others. Is anyone surprised that foodborne illness remains so common? Overlap occurs for every specific function listed in the table (e.g., four offices and three different agencies are responsible for risk assessment in seafood). Inconsistencies appear in each column; for example, in several cases, agencies responsible for monitoring and surveillance for a given commodity are not responsible for risk assessment, and some of these agencies in turn differ from those involved in research, inspection, enforcement, and education. Looking across the rows in Table 2-1, the group of agencies sharing responsibility for a function in one commodity (e.g., inspection of fruits and vegetables) does not match the agencies responsible for the same function in another commodity (e.g., inspection of seafood).
Reorganizing the U.S. Food Safety System
Prominent among the recommendations made in Ensuring Safe Food from Production to Consumption seven years ago is the following statement:
TABLE 2-1 Overlap in Federal Food Safety Oversight
|
Selected Food Products |
Food Contaminants |
|||||||
|
Fruits and Vegetables |
Dairy Products |
Eggs & Egg Products |
Meat & Poultry |
Seafood |
Grain, Rice & Related Commodities |
Imported Foods |
Animal Drugs & Feeds |
Pesticide Residues |
|
CDC; CFSAN/FDA |
CDC; CFSAN & CVM/FDA |
CDC; CFSAN/FDA; AMS/USDA |
CDC; CFSAN/FDA; USDA: FSIS, ERS |
CDC; CFSAN/FDA; NMFS/NOAA |
CDC; CFSAN/FDA |
CDC, CFSAN & ORA/FDA; FSIS/USDA |
CDC; CVM/FDA; FSIS/USDA; APHIS |
CDC; FSIS/USDA; CFSAN/FDA |
|
CFSAN/FDA; ARS/USDA |
CFSAN; CVM/FDA; ARS/USDA |
ARS & FSIS/USDA; ORACBA; CFSAN/FDA |
USDA: ARS, CSREES, FSIS, ERS, ORACBA; CFSAN/FDA |
CFSAN/FDA; NMFS/NOAA; ARS/USDA |
ARS/USDA; CFSAN/FDA |
Same as domestic food products |
CVM/FDA; ARS/USDA/APHIS |
OPPTS/EPA; USDA: AMS, ARS, ERS, NASS |
|
CFSAN, NCTR/FDA; ARS, CSREES/USDA |
CFSAN; CVM/FDA, CSREES & ARS/USDA |
CFSAN/FDA; ARS/USDA CSREES |
USDA: ARS, CSREES |
CVM & CFSAN/FDA; NMFS/NOAA; CSREES & ARS/USDA |
ARS, CSREES/USDA; CFSAN/FDA |
Same as domestic food products |
CFSAN & CVM/FDA; ARS & CSREES/USDA |
ORD/EPA; CSREES & ARS/USDA; CFSAN/FDA |
|
CFSAN & ORA/FDA |
CFSAN, ORA, & CVM/FDA |
FSIS/USDA; FDA: CVM, CFSAN & ORA |
FSIS/USDA; CFSAN & CVM/FDA |
ORA & CFSAN/FDA; NMFS/NOAA |
GIPSA/USDA; ORA & CFSAN/FDA |
FSIS/USDA; CFSAN & ORA/FDA |
ORA & CVM/FDA; FSIS/USDA; APHIS |
USDA: FSIS, AMS/FDA: CFSAN, CVM, & ORA; OECA/EPA |
|
CFSAN/FDA; CSREES, ARS/USDA |
CFSAN/FDA; CSREES, ARS/USDA |
CFSAN/FDA; FSIS & CSREES, ARS/USDA |
USDA: FSIS, CSREES, ARS, ERS, ORACBA; CFSAN/FDA |
CFSAN/FDA; CSREES, ARS/USDA; NMFS/NOAA |
CSREES, ARS/USDA; CFSAN/FDA |
CSREES, ARS/FDA; CFSAN/FDA |
CSREES, ARS/USDA; CVM/FDA |
CFSAN/FDA; FSIS & CSREES, ARS/USDA |
|
NOTE: Acronym list is provided in Appendix B. SOURCE: IOM/NRC (1998). |
||||||||
Congress should establish, by statute, a unified and central framework for managing food safety programs, one that is headed by a single official and which has the responsibility and control of resources for all federal food safety activities, including outbreak management, standard-setting, inspection, monitoring, surveillance, risk assessment, enforcement, research, and education (IOM/NRC, 1998).
This committee was not the first body to call for such reform. At that time, we knew of nearly 20 commissions, committees, and studies dating back to 1949 that had made similar recommendations (Vogt, 1998); more recently, the Government Accountability Office (GAO) has taken up this issue (GAO, 2004, 2005a,b). However, I would like to emphasize one of the important points that came out of our report: the need to have an independent agency, one that will not be influenced by competing priorities within agencies where the work of ensuring food safety is currently carried out.
I will conclude with a personal observation as to why, despite the many calls for reorganization, our food safety system remains fragmented and inadequate. I believe that the following three reasons lie at the heart of this problem:
-
Bureaucratic inertia—It will take time, effort, and money to implement the major reorganization that has been recommended.
-
Turf battles—Federal agencies and congressional committees that currently oversee various aspects of food safety do not want to give up funds, personnel positions, authorities, and responsibilities.
-
Industrial inertia—Regulated industries have adapted to the present system and its constraints. Companies do not welcome change, even when it is in the public interest.
Although none of these obstacles constitutes an acceptable excuse for postponing needed reform, they clearly must be overcome in order to create the unified, independent federal program that is needed to truly ensure the safety of the U.S. food supply.
FOOD SAFETY THREATS—INTERNATIONAL COORDINATION
Jørgen Schlundt, Ph.D.3
World Health Organization
Summary
Food safety relates to both human health and economic development. Countries all over the world are affected by a range of diseases related to food, in effect
causing a very significant disease burden that seems to have been on the rise in both developed and developing countries over the most recent decades. Outbreaks of foodborne diseases most often originate in natural or accidental contamination events, but the potential for intentional contamination of the food chain is present, as documented by previously recorded—although relatively minor—such outbreaks. The developments towards a more global food market underlines that it is in the best interest of all countries to strengthen the international capacity for foodborne outbreak alert and response. Such capacity is built most efficiently through unified systems dealing with all forms of outbreak—intentional as well as unintentional. The role of the WHO is to provide advice on strengthening national systems to prevent and respond to foodborne outbreaks, including intentional contamination events. The WHO is in a unique position to coordinate existing international systems for public health disease surveillance and emergency response. The revised WHO International Health Regulations provides the legal platform for all countries to declare public health emergencies of international concern. The WHO INFOSAN offers a system for alert action and response to public health emergencies involving food, related to both intentional and unintentional contamination events.
Existing Foodborne Disease Burden
Food safety is an important public health problem that relates to both human health and economic development (WHO, 2002a). Countries all over the world are affected by a range of diseases related to food, in effect causing a very significant disease burden that seems to be increasing both in developed and developing countries.
Food safety problems can cause a number of different diseases, from relatively mild cases of food poisoning to deadly infections and cancer. Diarrheal diseases—almost all caused by food- or waterborne microbial pathogens—are leading causes of illness and death in less developed countries, killing an estimated 1.8 million people annually at the global level (WHO, 2005). Even in developed countries it is estimated that up to one-third of the population is affected by microbiological foodborne disease each year (Mead et al., 1999). The majority of the pathogens causing this significant disease burden are now considered to be zoonotic pathogens. The occurrence of some of these zoonotic pathogens seems to have increased significantly over recent years.
Although a significant fraction of diarrhea is caused by food, this still only constitutes part of the total foodborne disease burden. Other parts of the burden relate to a number of important, and often more chronic, diseases caused by not only microorganisms but also chemical contaminants in our food. The disease burden related to chemical contaminants and chemical constituents in our food is very difficult to estimate, but it is likely that this part of the total burden could be as big as the microbiological burden.
The reporting of foodborne disease is typically based on the number of laboratory confirmed cases, only representing a fraction of the real cases. The factor between reported and real cases is called the underreporting factor. Few thorough epidemiological estimations of the national underreporting factor have been made, but there are significant variations in the factor presented. One example of such variation is that for salmonellosis the factors can vary from 3.2 fold from a study in the United Kingdom (Wheeler et al., 1999) to 38 fold from a study in the United States (Mead et al., 1999). It is not easily evaluated whether differences in the underreporting factor between countries is a reflection of real differences in the performance of health systems or a reflection of differences in methodology used to estimate the factor.
Although some national foodborne disease surveillance systems mainly collect information on the number of outbreaks and the number of cases involved in the outbreaks, for most foodborne diseases the majority of cases are sporadic. Surveillance systems must include measures to estimate also the sporadic part of the foodborne disease burden. New, active surveillance systems are likely in the future to blur the difference between what has traditionally been referred to as outbreaks and sporadic cases. The possibility of comparing types of pathogens (e.g., pulsed-field gel electrophoresis typing) isolated from human cases in a broad national system enables the linking of cases, previously considered single or sporadic in nature, and present them as part of an outbreak spread over a larger geographical area (Gerner-Smidt et al., 2005). It is thus likely that our understanding of the relative importance of outbreaks and sporadic cases will change in the near future.
As a result of the increased global trade in food it is also likely that outbreaks covering larger areas and affecting several countries will be recognized in larger numbers in the future. Surveillance of foodborne diseases provides information for action. The use of laboratory data in surveillance enables the identification of pathogens and the potential sources of infection. In the future, integrated surveillance including human data as well as animal- and food-monitoring data can also provide the basis for preventive action along the entire food chain. In 2000, WHO initiated the Global Salm-Surv, which provides targeted efforts to national typing laboratories, and the sharing and analysis of such results has recently lead to the recognition of trade and foreign travel as factors related to the international emergence of certain Salmonella serotypes as well as to multicountry outbreaks of Salmonella (WHO, 2006).
The Global Salm-Surv network builds laboratory and epidemiological capacity for integrated laboratory-based foodborne disease surveillance. The network presently has almost 900 members from 141 countries. The Global Salm-Surv maintains a database that in its first five-year period (2000–2004) recorded 565,042 isolates from humans and 102,113 nonhuman isolates (mainly from food).
As an integral part of foodborne disease surveillance there is a need to enable precise and timely information sharing between countries of outbreak-related data. At the global level such systems do not yet exist, but WHO efforts related to the new International Health Regulations and the newly formed INFOSAN should be seen in this light. These initiatives will be described further in Chapter 4.
Deliberate Contamination of Food: Recent Concern—Old Problem
The “deliberate contamination of food” is sometimes used synonymously with food terrorism or food bioterrorism. Food terrorism is defined as an act or threat of deliberate contamination of food for human consumption with chemical, biological, or radionuclear agents for the purpose of causing injury or death to civilian populations and/or disrupting social, economic, or political stability. Threats from terrorists, criminals, and other antisocial groups who target the safety of the food supply are already a reality. During the past two decades, WHO member states have expressed concern about the possibility that chemical and biological agents and radionuclear materials might deliberately be used to harm civilian populations. In May 2002, the 55th World Health Assembly (WHA) adopted a resolution that expressed serious concern about threats against civilian populations by deliberate use of biological, chemical, or radionuclear agents (WHO, 2002b). It noted that such agents can be disseminated via food, and the WHA requested the Director General to provide tools and support to member states, particularly developing countries, in strengthening their national systems.
In the past food supplies have often been contaminated deliberately, historically during military campaigns and, more recently, to terrorize or otherwise intimidate civilian populations (Khan et al., 2001). Deliberate contamination of food by chemical, biological, or radionuclear agents can occur at any vulnerable point along the food chain, from farm to table, depending on both the food and the agent. For example, in 1984, members of a religious cult contaminated salad bars in the United States with Salmonella typhimurium, causing 751 cases of salmonellosis. The attack appeared to be a trial run for a more extensive attack intended to disrupt local elections. The cult was also in possession of strains of Salmonella typhi, the causative organism of typhoid fever, a severe invasive illness (Torok et al., 1997).
The impact on human health of the future deliberate contamination of food can be estimated by extrapolation from the many documented examples of unintentional outbreaks of foodborne disease. The largest, best-documented incidents include an outbreak of S. typhimurium infection in 1985, affecting 170,000 people, caused by contamination of pasteurized milk from a dairy plant in the United States (Ryan et al., 1987). An outbreak of hepatitis A associated with consumption of clams in Shanghai, China, in 1991 affected nearly 300,000 people and may be the largest foodborne disease incident in history (Halliday et al., 1991). In 1994, an outbreak of S. enteritidis infection from contaminated pasteurized liquid
ice cream that was transported as a premix in tanker trucks caused illness in 224,000 people in 41 states in the United States (Hennesy et al., 1996). In 1996, about 8,000 children in Japan became ill, including some deaths, with Escherichia coli O157:H7 infection from contaminated radish sprouts served in school lunches (Mermin and Griffin, 1999).
Episodes of foodborne illness caused by chemicals have also been reported in the published literature. The chemicals that can contaminate food include pesticides, mycotoxins, heavy metals, and other acutely toxic chemicals. In perhaps one of the most deadly incidents, over 800 people died and about 20,000 were injured, many permanently, by a chemical agent present in cooking oil sold in Spain in 1981 (WHO, 1983). In 1985, 1,373 people in the United States reported becoming ill after eating watermelon grown in soil treated with aldicarb (Green et al., 1987).
There are also many examples of outbreaks resulting from imported foods. In 1989, staphylococcal food poisoning in the United States was associated with eating mushrooms that had been canned in China (Levine et al., 1996). Outbreaks of cyclosporiasis in the United States in 1996 and 1997 were linked to consumption of Guatemalan raspberries (Herwaldt and Ackers, 1997). In the early 1990s epidemiological investigations of an increased human incidence of Salmonella berta in England and Wales was traced to chicken imported from Denmark (Threlfall et al., 1992).
In general, contamination of food may also have enormous economic implications. In an effort to damage Israel’s economy in 1978, some citrus fruit exported to several European countries was contaminated with mercury, leading to significant trade disruption. In 1998, a company in the United States recalled 14 million kilograms of frankfurters and luncheon meats potentially contaminated with Listeria, resulting in a total cost of approximately US$50–70 million (CDC, 1999). An outbreak of E. coli O157:H7 infection in the United States in 1997 resulted in the recall of 11 million kilograms of ground beef (CDC, 1997). The crisis in Belgium in which dioxin-contaminated meat and dairy products were recalled around the world demonstrates not only the extensive costs to individual countries, but also the extent of disruption of global trade that can be caused by this type of incident (WHO, 2004a). From October 1996 to November 2002, 139 cases of variant Creutzfeldt-Jakob Disease have been reported globally, mainly in the United Kingdom, and most likely linked to exposure through food to the causative “agent” of bovine spongiform encephalopathy (BSE) in cattle (WHO, 2002c). Consequent consumer concern about consumption of meat has had a significant long-term impact on meat production in many countries.
In less developed countries, the economic consequences of major food contamination events could—in addition to human suffering and costs—also affect development and exacerbate poverty as well as food availability. Likewise the loss of export earnings can be very substantial both as a result of substantiated as well as unsubstantiated import restrictions. The lost revenues from food (espe-
cially fish) exports as a result of the 1991 cholera epidemic in Peru has been estimated to be US$700 million (Motarjemi, 1993). In a less well documented case, fish import restrictions in the European Union were upheld for a significant period of time following the publication of reports of cholera in East Africa, resulting in significant economic losses.
Prevention and Response Systems
All countries must have basic systems to prevent or deter deliberate contamination of their food supplies and, if attacked, to respond rapidly to minimize the health, economic, and other effects of such contamination.
However, counterterrorism should be seen as only one aspect of a broader, comprehensive food safety program in national and global contexts. WHO and a number of member states have addressed this issue with strategies to reduce the increasing burden of foodborne illness. The WHO Global Strategy for Food Safety, endorsed in January 2002 by the WHO executive board, comprises a preventive approach to food safety, with increased surveillance and more rapid response to outbreaks of foodborne illness. This approach could substantially expand the abilities of member states to protect the safety of their food supplies against natural and accidental threats and provides a framework for addressing terrorist threats to food.
Food production systems have become longer and more complicated over the latest decades. These changes in the way food is produced, processed, distributed, and sold have occurred at the same time as rapidly expanding international trade, the emergence of new transboundary food scares, greater international travel, and changing consumer preferences—all serving to draw new attention to the importance and challenge of ensuring food safety at the international level.
The recognition of the source and potential intention behind an outbreak or contamination event will in many cases only be possible at a very late stage. Although deliberate contamination presents a special set of issues, the same detection and response systems need to tackle outbreaks or contamination events whether the event is intentional or unintentional. Sensible precautions, coupled with strong surveillance and response capacity, constitute the most efficient and effective way of countering all such emergencies, including deliberate contamination of food.
For both developed and developing countries, guidance is needed to strengthen surveillance, preparedness, and response systems to meet the threat of any food safety emergency. Unfortunately, the tragic events in the United States on September 11, 2001, have focused a new angle to the debate of food safety: the issue of bioterrorism or other forms of intentional contamination of food. Agricultural production systems and food-processing facilities are potentially at risk. Efforts towards prevention should be integrated in existing systems, for ex-
ample critical points for control should be defined within existing Hazard Analysis and Critical Control Point (HACCP) systems. Likewise existing surveillance and monitoring systems for foodborne disease and food contamination should be expanded to include the threats related to potential intentional contamination. This integrated approach would result in activities supporting the general food safety efforts instead of detracting from them.
Strengthening of such integrated systems and programs will both increase a country’s capacity to reduce the increasing burden of foodborne illness and help to address the threat of intentional food contamination. It is important to reiterate that any intentional contamination event would probably always initially be considered as a natural or unintentional event, and that such events must therefore be managed on the food side through one, coherent system with relevant links to other authorities (police, intelligence services, etc.) in case of suspicious events.
Prevention, although never completely effective, is the first line of defense. The key to preventing food terrorism is establishment and enhancement of existing food safety management programs and implementation of reasonable security measures—not the setting up of new separate systems potentially detracting from existing efforts and scarce resources.
Prevention is best achieved through a cooperative effort between government and industry, given that the primary means for minimizing food risks lie with the food industry. Policy advice should be aimed at strengthening existing emergency alert and response systems by improving links with all the relevant agencies and with the food industry. This multistakeholder approach will strengthen disease outbreak surveillance, investigation capacity, preparedness planning, effective communication, and response (WHO, 2002d).
There is a growing realization that existing systems for food animal production in many countries do not correspond to the prevalent food control systems that are often centered around efforts at the slaughter house. The importance of small-holder production systems and animal markets has been clearly outlined, especially in an Asian context and in relation to recent outbreaks of highly pathogenic H5N1 avian influenza. A recent WHO report underlines the need for WHO and countries to improve current regulatory frameworks related to the marketing of live birds and other animals for food, including guidance applicable in developing countries (WHO, 2004b). Again the links between countries through increased food trade should be recognized, as should the need for timely international information sharing and coordinated response.
A growing share of the food consumed in industrialized countries today comes from developing and transition countries, and this trend is likely to intensify in the future. Clearly, it is in the best interest of us all to strengthen the capacity of the public and private sector in developing countries to produce food that meets international safety and quality standards. Consumers and importers in industrialized countries stand to benefit from increased access to an affordable, diverse, and safe supply of food products. Developing countries will benefit from access to new markets and greater foreign exchange earnings through trade.
International Preparedness
Contrary to popular beliefs the effect of food control systems based on testing is not very efficient. The reason for this relates to the fact that for many food types the prevalence of pathogens potentially causing disease can be very low. Salmonella in eggs causes a very large proportion of the human salmonellosis cases in most countries. Nevertheless, the prevalence of Salmonella-positive eggs is often 1:1,000 or even down to 1:10,000. In effect, you would therefore have to test a very large number of eggs to have any chance to find positive eggs, and the effect of removing such (few) eggs from the market is negligible. Even for foods with higher prevalence of pathogens, control based on testing is inefficient, and the main positive effect of such systems lies in a potential for (economic) punishment leading to changes in the production systems. For example, it is likely that the classification of enterohemorrhagic Escherichia coli as an adulterant in the United States and the resulting economic disasters for certain producers found to be in violation could have resulted in changes in the production systems leading to the avoidance of some of the previous problems. However, in many of these cases it is difficult to measure objectively the effect of such strategies as these problems are often affected by many different factors at the same time.
Since test-and-eliminate strategies are often not very efficient, it follows that prevention of outbreaks solely based on border control in most cases will not provide the level of protection sought after. New—and more efficient—food safety systems try to focus on preventative efforts as close to the source as possible, such as in industrial production settings through the introduction of HACCP systems. Because many food contamination events have international implications and because a significant fraction of food for consumption in many countries are imported, it follows that the most efficient way for any country to prevent intentional or unintentional foodborne outbreaks is to strengthen food safety in the country of origin and to ensure efficient international systems for outbreak alert and necessary response. A result of the global food market is that we now have a joint interest in building capacity to prevent and detect foodborne outbreaks in all countries through relevant international mechanisms.
In general, the need for international exchange of experience and scientific information in the food safety area is evident. The recent 2nd Global Forum for Food Safety Regulators in Bangkok, Thailand, is an example of such exchange of experience with a view of building efficient food safety capacity in all countries (FAO/WHO, 2004). Based on the outcome of this meeting the newly established INFOSAN, hosted by WHO, will continue a real-time interaction between the food safety authorities of the world (WHO, 2004c).
INFOSAN is intended to be an information network for the dissemination of important information about global food safety issues. INFOSAN members (of which each country can have several) receive information notes on current issues of interest for food safety authorities. Recent examples of information note sub-
jects include avian influenza, Enterobacter sakazakii in powdered infant formula, acrylamide in food, antimicrobial-resistant Salmonella, and evaluation of genetically modified food. The INFOSAN focal points are expected to disseminate INFOSAN information to interested parties and stakeholders in their country, as appropriate. INFOSAN focal points may be located in several ministries, such as ministries of health, commerce, agriculture, and trade (see Figure 2-1).
A new emergency arm of the INFOSAN network (INFOSAN Emergency) will enable timely sharing of information and coordinated response in the case of major international foodborne outbreaks or food contamination events (WHO, 2004c). INFOSAN Emergency contact points are expected to function as two-way action points for emergency information. They should alert relevant food safety authorities within their country to foodborne disease outbreaks or food contamination events of international public health significance as reported to them by INFOSAN Emergency. And they should convey to the network information of national outbreaks or contamination events with a potential to become international events. Only one INFOSAN Emergency contact point has been requested per country in order to facilitate rapid and reliable communication with governments in cases where timeliness is critical. Potential future incidents involving deliberate contamination with international implications would likely be communicated through INFOSAN Emergency.
Relevant past examples of international food-related events that could have benefited from an international system for information sharing include the Chernobyl accident in the former Soviet Union (1986), the BSE outbreak and ban
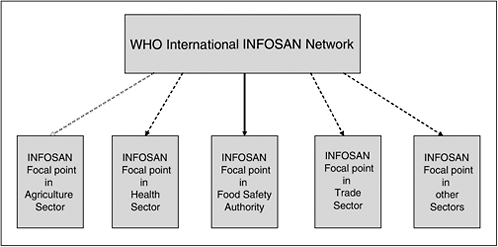
FIGURE 2-1 The WHO International Food Safety Authorities Network (INFOSAN): Set-up of focal points for information sharing.
SOURCE: INFOSAN (2005).
on feeding materials in the United Kingdom (1996), and the dioxin contamination of animal-derived food in Belgium (1997).
Since its inception in October 2004, INFOSAN Emergency has been involved in 11 verification events and sent out 3 notifications alerting from 5 to 32 countries on issues of potential international importance. These issues include powdered infant formula contaminated with Salmonella, orange juice contaminated with Salmonella, and pork contaminated with Streptococcus.
Clear, rapid, reliable, and authoritative information on food emergencies is the essential basis not only for prevention and response measures but also maintaining consumer confidence in the food supply. INFOSAN Emergency will be activated only during major international incidents involving the imminent risk of serious injury or death to consumers. INFOSAN Emergency contact points will be expected to accept some notification and response responsibility and to facilitate the communication of urgent messages during food safety emergencies. Figure 2-2 presents an example of how this may be structured in a country. Because of the potential sensitivity of the information exchanged, communication on this network would be considered confidential.
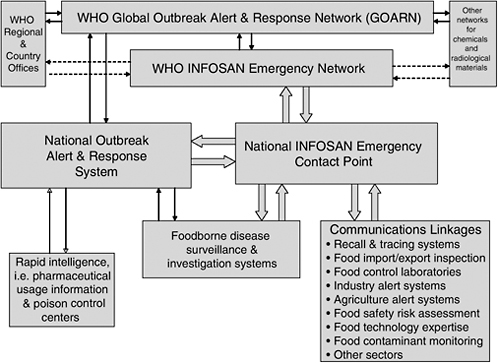
FIGURE 2-2 The WHO International Food Safety Authorities Network (INFOSAN): Potential communication lines for national INFOSAN Emergency Contact Points.
SOURCE: INFOSAN (2005).
INFOSAN Emergency will be closely linked to the alert-and-response activities of WHO and will be—to the extent necessary—functioning in support of the new international health regulations (WHO, 2004d). These regulations stipulate the international rules for sharing information on certain infectious diseases. The existing rules have up until now only covered yellow fever, cholera, and plague, enabling (and demanding) international exchange of information of outbreaks of such diseases. Responding to a realization that many internationally important disease incidents involve other responsible agents, including new agents such as the SARS virus, the need for a revision of international health rules was formulated in the WHA several years ago. The new rules propose the extension of the WHO coordinated public health emergency system to include all public health emergencies of international concern, which has been defined to also include foodborne emergencies or emergencies involving zoonotic diseases. Because of the legal framework of the regulations, there is no need for national ratification, and they will enter into force for all 192 WHO member states in June 2007.4 All WHO member states will be obliged to declare public health emergencies of international concern to the WHO.
WHO’s international systems to minimize impact on public health of international incidents, including the international health rules, INFOSAN, and other networks related to chemical and radiological incidents basically exist to do the following:
-
Rapidly detect any international incident;
-
Respond in a timely fashion to international emergencies; and
-
Decide and inform on the termination of emergency situations.
The systems therefore require:
-
Capacity for efficient information gathering and rapid communication;
-
Capacity to verify and make decisions;
-
Procedures to respond and capacity to assist; and
-
Basic platforms of national preparedness with international links.
REFERENCES
CDC (Centers for Disease Control and Prevention). 1997. Escherichia coli O157:H7 infections associated with eating a nationally distributed commercial brand of frozen ground beef patties and hamburgers: Colorado, 1997. Morbidity and Mortality Weekly Report 46(33):777–778.
CDC. 1999. Update: Multi-state outbreak of listeriosis—United States, 1998–1999. Morbidity and Mortality Weekly Report 47(51/52):1117–1118.
FAO/WHO (Food and Agriculture Association and the World Health Organization). 2004. Second FAO/WHO Global Forum of Food Safety Regulators—A Forum Dedicated to Sharing Experiences in Management of Food Safety. [Online]. Available: http://www.foodsafetyforum.org/global2/index_en.asp [accessed April 10, 2006].
GAO (Government Accountability Office). 2004. Federal Food Safety and Security System: Fundamental Restructuring is Needed to Address Fragmentation and Overlap. GAO-04-588T. Washington, D.C.: GAO.
GAO. 2005a. Overseeing the U.S. Food Supply: Steps Should be Taken to Reduce Overlapping Inspections and Related Activities. GAO-05-549T. Washington, D.C.: GAO.
GAO. 2005b. Oversight of Food Safety Activities: Federal Agencies Should Pursue Opportunities to Reduce Overlap and Better Leverage Resources. GAO-05-213. Washington, D.C.: GAO.
Gerner-Smidt P, Kincaid J, Kubota K, Hise K, Hunter SB, Fair MA, Norton D, Woo-Ming A, Kurzynski T, Sotir MJ, Head M, Holt K, Swaminathan B. 2005. Molecular surveillance of shiga toxigenic Escherichia coli O157 by PulseNet USA. Journal of Food Protection 68(9):1926– 1931.
Green MA, Heumann MA, Wehr HM, Foster LR, Williams LP Jr, Polder JA, Morgan CL, Wagner SL, Wanke LA, Witt JM. 1987. An outbreak of watermelon-borne pesticide toxicity. American Journal of Public Health 77(11):1431–1434.
Halliday ML, Kang LY, Zhou TK, Hu MD, Pan QC, Fu TY, Huang YS, Hu SL. 1991. An epidemic of hepatitis A attributable to the ingestion of raw clams in Shanghai, China. Journal of Infectious Diseases 164(5):852–859.
Hennesy TW, Hedberg CW, Slutsker L, White KE, Besser-Wiek JM, Moen ME, Feldman J, Coleman WW, Edmonson LM, MacDonald KL, Osterholm MT. 1996. National outbreak of Salmonella enteritidis infections from ice cream. New England Journal of Medicine 334(20):1281–1286.
Herwaldt BL, Ackers ML. 1997. An outbreak in 1996 of cyclosporiasis associated with imported raspberries. Cyclospora Working Group. New England Journal of Medicine 336(22):1548–1556.
INFOSAN (International Food Safety Authorities Network). 2005. International Food Safety Authorities Network. [Online]. Available: http://www.who.int/foodsafety/fs_management/infosan_0705_en.pdf [accessed April 20, 2006].
IOM/NRC (Institute of Medicine/National Research Council). 1998. Ensuring Safe Food from Production to Consumption. Washington, D.C.: National Academy Press.
Khan AS, Swerdlow DL, Juranek DD. 2001. Precautions against biological and chemical terrorism directed at food and water supplies. Public Health Reports 116(1):3–14.
Levine WC, Bennet RW, Choi Y, Henning KJ, Rager JR, Hendricks KA, Hopkins DP, Gunn RA, Griffin PM. 1996. Staphylococcal food poisoning caused by imported canned mushrooms. Journal of Infectious Diseases 173(5):1263–1267.
Mead PS, Slutsker L, Dietz V, McCaig LF, Bresee JS, Shapiro C, Griffin PM, Tauxe RV. 1999. Food-related illness and death in the United States. Emerging Infectious Diseases 5(5):607–625.
Mermin JH, Griffin PM. 1999. Public health in crisis: Outbreaks of Escherichia coli O157:H7 in Japan. American Journal of Epidemiology 150(8):797–803.
Motarjemi Y. 1993. Health and development aspects of food safety. Archiv für Lebensmittelhygiene 44(2):35–41.
Ryan CA, Nickels MK, Hargrett-Bean NT, Potter ME, Endo T, Mayer L, Langkop CW, Gibson C, McDonald RC, Kenney RT, Puhr ND, McDonnell PJ, Martin RJ, Cohen ML, Blake PA. 1987. Massive outbreak of antimicrobial-resistant salmonellosis traced to pasteurized milk. Journal of the American Medical Association 258(22):3269–3274.
Threlfall EJ, Hall ML, Ward LR, Rowe B. 1992. Plasmid profiles demonstrate that an upsurge in Salmonella berta in humans in England and Wales is associated with imported poultry meat. European Journal of Epidemiology 8(1):27–33.
Torok T, Tauxe RV, Wise RP, Livengood JR, Sokolow R, Mauvais S, Birkness KA, Skeels MR, Horan JM, Foster LR. 1997. A large community outbreak of Salmonella caused by intentional
contamination of restaurant salad bars. Journal of the American Medical Association 278(5): 389–395.
Vogt DU. 1998. Food Safety: Recommendations for Changes in the Organization of Federal Food Safety Responsibilities, 1949–1997. CRS Report 93-955. Washington, D.C.: Library of Congress.
Wheeler JG, Sehti D, Cowden JM, Wall PG, Rodrigues LC, Tompkins DS, Hudson MJ, Roderirick PJ. 1999. Study of infectious intestinal disease in England: Rates in the community, presenting to general practice, and reported to national surveillance. The Infectious Intestinal Disease Study Executive. British Medical Journal 318(7190):1046–1050.
WHO (World Health Organization). 1983. Toxic Oil Syndrome: Mass Food Poisoning in Pain. Report of a WHO meeting, Madrid, Spain, May 21–25, 1983. Copenhagen: WHO Regional Office for Europe.
WHO. 2002a. WHO Global Strategy for Food Safety: Safer Food for Better Health. Food Safety Issues Series. [Online]. Available: http://www.who/int/foodsafety/publications/general/global_strategy/en/ [accessed April 10, 2006].
WHO. 2002b. World Health Assembly Resolution (WHA55.16): Global Public Health Response to Natural Occurrence, Accidental Release or Deliberate Use of Biological and Chemical Agents or Radionuclear Material That Affect Health. [Online]. Available: http://www.who.int/gb/ebwha/pdf_files/WHA55/ewha5516.pdf [accessed April 10, 2006].
WHO. 2002c. Fact Sheet No. 180 on variant Creutzfeldt-Jakob Disease (Rev. November 2002). Geneva: WHO.
WHO. 2002d. Terrorist Threats to Food: Guidance for Establishing and Strengthening Prevention and Response Systems, Food Safety Issues Series. Geneva: WHO.
WHO. 2004a. Sixth Futures Forum on Crisis Communication. Report of a WHO meeting, Reykjavik, Iceland, May 10–11, 2004. Copenhagen: WHO Regional Office for Europe.
WHO. 2004b. Food safety. In: The Work of WHO in the Western Pacific Region, Report of the Regional Director, 1 July 2003–30 June 2004. Manila, Philippines: WHO. Pp. 80–83.
WHO. 2004c. INFOSAN: International Food Safety Authorities Network. [Online]. Available: http://www.who/int/foodsafety/fs_management/infosan/en/ [accessed April 10, 2006].
WHO. 2004d. IHR: International Health Regulations. [Online]. Available: http://www.who.int/csr/ihr/en/ [accessed April 10, 2006].
WHO. 2005. World Health Report 2005. Annexes by Country. [Online]. Available: http://www.who.int/whr/2005/en/ [accessed April 10, 2006].
WHO. 2006. WHO Global Salm-Surv Progress Report (2000–2005): Building Capacity for Laboratory-Based Foodborne Disease Surveillance and Outbreak Detection and Response. Geneva: WHO.

















