
1
INTRODUCTION
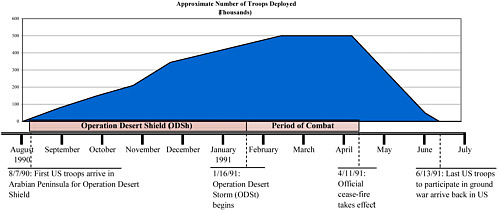
Five days after the Iraqi invasion of Kuwait on August 2, 1990, the United States deployed troops to Operation Desert Shield (ODSh). The United States attacked Iraqi armed forces by air on January 16, 1991, and this marked the beginning of Operation Desert Storm (ODSt). The ground war began on February 24, 1991, and ended 4 days later. The official ceasefire took effect on April 11, 1991, and the last troops to participate in the ground war arrived back in the United States on June 13, 1991. In this report, ODSh and ODSt are also referred to collectively as the Gulf War.
About 697,000 US troops were deployed to the Persian Gulf during ODSh and ODSt. Figure 1.1 depicts the size of the US military presence in the Persian Gulf from August 1990 through June 1991. The war was considered to be a successful military operation, and there were few injuries and deaths.
Shortly after returning to the United States, a number of veterans started reporting a variety of symptoms—fatigue, headache, muscle and joint pain, sleep disturbances, and cognitive difficulties (Persian Gulf Veterans Coordinating Board 1995). The veterans were concerned that they might have been exposed to chemical, biologic, or physical agents during their deployment to the Persian Gulf and that those exposures might be responsible for their unexplained illnesses.
In response to the concerns of the Gulf War veterans about their unexplained illnesses, the US Department of Veterans Affairs (VA) asked the Institute of Medicine (IOM) to conduct a study to evaluate the scientific literature on chemical, biologic, and physical agents to which military personnel in the gulf were potentially exposed and possible long-term adverse health outcomes. In addition, Congress passed two laws in 1998—the Persian Gulf War Veterans Act (PL 105-277) and the Veterans Programs Enhancement Act (PL 105-368)—that called for the review of the scientific literature on specified agents with regard to long-term adverse health outcomes. That legislation directs IOM to study a number of diverse chemical, biologic, and physical agents (listed in Box 1.1). IOM divided the task into several reviews. It has completed four reports: Gulf War and Health, Volume 1: Depleted Uranium, Pyridostigmine Bromide, Sarin, Vaccines (IOM 2000); Gulf War and Health, Volume 2: Insecticides and Solvents (IOM 2003); Gulf War and Health Volume 3: Fuels, Combustion Products, and Propellants (IOM 2005); and Gulf War and Health, Volume 4: Health Effects of Serving in the Gulf War (IOM 2006). The present report is the fifth volume in the series. An additional, related report has also been published: Gulf War and Health: Updated Literature Review of Sarin (IOM 2004).
Since VA asked IOM to conduct the above-mentioned study and PL 105-277 and PL 105-368 were enacted, the United States has again entered into military conflicts in southwest and south-central Asia—Operation Enduring Freedom (OEF) and Operation Iraqi Freedom (OIF). Therefore, VA has asked IOM to make this report relevant to the military personnel serving in OEF and OIF in addition to those who served in the 1991 Gulf War.
|
BOX 1-1 Agents Specified in PL 105-277 and PL 105-368
|
IDENTIFYING THE INFECTIOUS DISEASES TO STUDY
In accordance with PL 105-277 and PL 105-368, IOM appointed the Committee on Gulf War and Health: Infectious Diseases and tasked it to review, evaluate, and summarize the peer-reviewed scientific and medical literature on long-term adverse health outcomes associated with selected infectious diseases pertinent to service in the Gulf War. The infectious diseases can include, but are not limited to, pathogenic Escherichia coli infection, shigellosis, leishmaniasis, and sand fly fever.
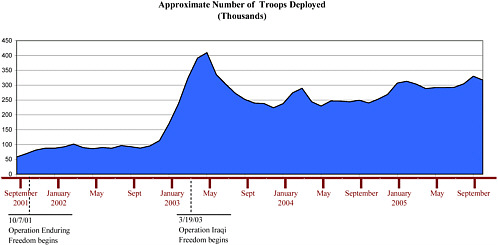
VA is also concerned about potential long-term adverse health outcomes of infectious diseases in veterans of OEF and OIF. As of October 2005, about 1.2 million US troops have been deployed to OEF or OIF (see Figure 1.2). VA asked IOM to evaluate infectious diseases pertinent to service in OEF and OIF.
It should be noted that the charge to IOM was not to determine whether a unique Gulf War syndrome or Gulf War illness exists or to make judgments about whether individual veterans were exposed to specific pathogens. Nor was the charge to focus on broader issues, such as the potential costs of compensation for veterans or policy regarding compensation; such decisions are the responsibility of the secretary of veterans affairs.
THE COMMITTEE’S APPROACH TO ITS CHARGE
A brief overview of how the committee approached its charge is presented here. A more comprehensive explanation is provided in Chapter 2.
The committee identified numerous infectious diseases to which Gulf War, OIF, and OEF military personnel might have been exposed during their deployment. Dozens of infectious diseases are endemic to southwest and south-central Asia, which includes Iraq, Kuwait, and Afghanistan. The committee then determined which of the endemic infectious diseases are known to have long-term adverse health outcomes. To determine which infectious diseases to review in depth, the committee took several factors into account, including which ones were diagnosed in military personnel who served in the Gulf War, OEF, or OIF and in veterans after they returned home, as well as the prevalence of the infectious diseases in southwest and south-central Asia compared with their prevalence in the United States.
Overall, the incidence of infectious diseases among Gulf War military personnel was low (Hyams et al. 1995). Acute diarrheal and acute respiratory diseases were the major causes of morbidity from infectious diseases (Hyams et al. 1995; Hyams et al. 2001). The outbreaks of diarrhea were due primarily to enterotoxigenic Escherichia coli and Shigella sonnei. Some 12 cases of viscerotropic leishmaniasis and 20 cases of cutaneous leishmaniasis were diagnosed in Gulf War military personnel (Hyams et al. 1995; Hyams et al. 2001). Other reported infectious diseases included Q fever (three cases), West Nile fever (one case), and malaria (seven cases) (Hyams et al. 1995; Hyams et al. 2001).
Infectious diseases reported in troops who served in OEF and OIF as of December 2005 are visceral and cutaneous leishmaniasis, malaria, diarrheal disease, respiratory disease, tuberculosis infection (but not active tuberculosis), Q fever, brucellosis, and Acinetobacter baumannii infection (Kilpatrick 2005). Chapter 4 reviews the literature on infectious diseases that have been diagnosed in military personnel during or shortly after returning from the Gulf War, OIF, or OEF.
The committee identified for comprehensive evaluation nine infectious diseases known to have long-term adverse health outcomes that were diagnosed in military personnel who served in the Gulf War, OEF, or OIF. Some information is presented on a number of other infectious diseases as well because they are endemic to southwest and south-central Asia, although there have been no reported cases in military personnel through December 2005. It is possible that military personnel have become infected but that no diagnosis was made either because no acute symptoms were present or because the symptoms were mild and the soldier who had them did not seek medical care. We also present information on diseases and agents of special concern to veterans of the Gulf War, OEF, and OIF (Al Eskan disease, acute eosinophilic pneumonia, Acinetobacter baumannii infection, mycoplasmas, and biological warfare agents).
After determining which infectious diseases it would evaluate, the committee had to identify the relevant literature for review. The committee relied primarily on peer-reviewed published literature in developing its conclusions. It also consulted other material, such as surveillance reports, technical reports, and textbooks, and it obtained additional information from experts in infectious diseases of southwest and south-central Asia, from Deployment Health Support at the Department of Defense (DOD), from Walter Reed Army Institute of Research, from the VA Occupational and Environmental Health Strategic Healthcare Group, and from veteran service organizations and Gulf War veterans. The committee focused on medical and
scientific data on long-term adverse health outcomes related to the infectious diseases it selected for study.
The final step in the committee’s evaluation process was to weigh the evidence on the infectious diseases and their long-term adverse health outcomes and to develop conclusions about the strength of the evidence. The conclusions are assigned to categories of association, which range from sufficient evidence of a causal relationship to insufficient or inadequate evidence of an association.
This report includes discussion of acute diseases with potential long-term adverse health outcomes caused by known pathogens. The committee acknowledges that there might be clinically important pathogens that cannot be detected with available cultivation techniques (Relman 2002). Because the extent to which such pathogens might contribute to acute illnesses in military personnel is unknown, it is not possible to define a relationship between them and an acute illness or long-term adverse health outcome.
ORGANIZATION OF THE REPORT
Chapter 2 lays out the committee’s process for selecting the infectious diseases to study and reviewing and evaluating the evidence on them. Chapter 3 presents, in tabular format, the endemic infectious diseases of southwest and south-central Asia that are known to have long-term adverse health outcomes. Chapter 4 summarizes the body of literature on infectious diseases that have been diagnosed in military personnel serving in the Gulf War, OIF, and OEF. The committee’s comprehensive evaluations of selected infectious diseases are presented in Chapter 5, which also contains the committee’s conclusions. The final chapter, Chapter 6, presents information about diseases and agents of special concern to veterans of the Gulf War, OIF, and OEF that have an infectious component or have been implicated as a cause of “Gulf War illness”.
REFERENCES
DOD (Department of Defense). 2006. US Department of Defense Official Website. [Online]. Available: http://www.defenselink.mil/ [accessed March 2006].
Hyams KC, Hanson K, Wignall FS, Escamilla J, Oldfield EC, 3rd. 1995. The impact of infectious diseases on the health of US troops deployed to the Persian Gulf during operations Desert Shield and Desert Storm. Clinical Infectious Diseases 20(6):1497-1504.
Hyams KC, Riddle J, Trump DH, Graham JT. 2001. Endemic infectious diseases and biological warfare during the Gulf War: A decade of analysis and final concerns. American Journal of Tropical Medicine and Hygiene 65(5):664-670.
IOM (Institute of Medicine). 2000. Gulf War and Health, Volume 1: Depleted Uranium, Sarin, Pyridostigmine Bromide, Vaccines. Washington, DC: National Academy Press.
IOM. 2003. Gulf War and Health, Volume 2: Insecticides and Solvents. Washington, DC: The National Academies Press.
IOM. 2004. Gulf War and Health: Updated Literature Review of Sarin. Washington, DC: The National Academies Press.
IOM. 2005. Gulf War and Health, Volume 3: Fuels, Combustion Products, and Propellants. Washington, DC: The National Academies Press.
IOM. 2006. Gulf War and Health, Volume 4: Health Effects of Serving in the Gulf War. Washington, DC: The National Academies Press.
Kilpatrick ME. 2005. Presentation to IOM Committee on Gulf War and Health: Infectious Diseases. Washington, DC.
PAC (Presidential Advisory Committee). 1996. Presidential Advisory Committee on Gulf War Veterans’ Illnesses: Final Report. Washington, DC: US Government Printing Office.
Persian Gulf Veterans Coordinating Board. 1995. Unexplained illnesses among Desert Storm veterans. A search for causes, treatment, and cooperation. Persian Gulf Veterans Coordinating Board. Archives of Internal Medicine 155(3):262-268.
Relman DA. 2002. New technologies, human-microbe interactions, and the search for previously unrecognized pathogens. Journal of Infectious Diseases 186(2 Suppl):S254-S258.










