
Workshop Overview1
INFECTIOUS DISEASE MOVEMENT IN A BORDERLESS WORLD
Infectious disease is a kind of natural mortar binding one creature to another, one species to another, within the elaborate edifices we call ecosystems.
David Quammen (2007)
The advance of human civilization has brought people, plants, animals, and microbes together in otherwise improbable combinations and locations. While such biological introductions were once rare occurrences, human actions have all but eliminated the spatial and temporal barriers between species and ecosystems (Carlton, 2004). The profound consequences of human-mediated biological introductions include emerging infectious diseases: those caused by pathogens that have increased in incidence, geographic or host range; or that have altered capabilities for pathogenesis; or that have newly evolved; or that have been discovered or newly recognized (Anderson et al., 2004; Daszak et al., 2000; IOM, 1992).
Today, international travel and commerce (most notably the explosive growth of commercial air transportation over the past 50 years) drives the rapid, global distribution of microbial pathogens and the organisms that harbor them (IOM, 2003). These include humans, whose movements have been implicated in the
spread of diseases, including influenza (IOM, 2005); severe acute respiratory syndrome (SARS; IOM, 2004); drug-resistant malaria (IOM, 2003; Martens and Hall, 2000); and chikungunya2 in Europe (Angelini et al., 2007). Indeed, it is possible to travel between most places in the world in less time than the incubation period for many infectious diseases (Wilson, 2003), as was illustrated in spring 2009 by the rapid, global spread of the new, swine origin, influenza A (H1N1) virus (Dawood et al., 2009; Khan et al., 2009).
Travel is not only becoming increasingly rapid and more socially wide-spread, but is also more ubiquitous. Travelers and tourists connect once-remote areas, which serve as both “sources” and “sinks” for emerging infectious diseases, to more developed regions. International trade in food and other agricultural commodities, as well as in wildlife, has also increased markedly among an ever-widening network of producers and markets. Pathogens accompany live animals, plants, and their byproducts across continents and oceans; microbes and vectors also hitch rides in ballast water3 and in shipping crates and containers. Upon arrival in industrialized countries, such as the United States, potentially disease-containing goods can be redistributed nationwide within hours.
Travel and trade have been linked with disease since antiquity. People instinctively feared and isolated ill travelers long before the causative agents of infectious diseases were known or described (Gushulak and MacPherson, 2000). Quarantine laws, established to prevent the importation of plague—without success—in fourteenth-century Venice, were eventually adopted throughout Europe and Asia (Fidler et al., 2007; Markel et al., 2007).
International endeavors to contain infectious diseases commenced more than 150 years ago and are today embodied in the International Health Regulations (IHR), which provide the legal framework for global cooperation on infectious disease surveillance (IOM, 2007; Stern and Markel, 2004). While ideally there are strong incentives for nations to support global efforts to address infectious disease threats, such efforts have from their outset been characterized by a lack of authority for enforcement and weak inducements for participation (Stern and Markel, 2004).
More subtly, but no less importantly, introduced animals, plants, and microbes can disrupt ecosystems in ways that increase the potential for infectious disease outbreaks. Such changes can be more difficult to predict than the movements of pathogens, and more daunting to prevent. The term “invasive species” is widely used to describe plants and animals that spread aggressively when introduced to and established in new environments freed from the constraints found in their native environments (Dybas, 2004). Given both the similarities and characteristics of such invasions with those of pathogenic microbes, it may prove fruitful to view the origins of disease emergence, establishment, and spread through the
larger ecological lens of invasive species, and consider intervention strategies and approaches aimed at preventing and mitigating the far-reaching consequences of biological invasions.
On December 16 and 17, 2008, the Institute of Medicine’s (IOM’s) Forum on Microbial Threats hosted a two-day public workshop in Washington, DC, on Globalization, Movement of Pathogens (and their hosts), and the revised IHRs. Through invited presentations and discussions, participants explored a variety of interrelated topics associated with global infectious disease emergence, detection, and surveillance including the historical role of human migration and mobility in pathogen and vector movements; the complex interrelationship of travel, trade, tourism, and infectious disease emergence; national and international biosecurity policies; and obstacles and opportunities for detecting and containing globalized pathogens, thereby reducing the potential burden of emerging infectious diseases.
Organization of the Workshop Summary
This workshop summary was prepared for the Forum membership in the name of the rapporteurs and includes a collection of individually authored papers and commentary. Sections of the workshop summary not specifically attributed to an individual reflect the views of the rapporteurs and not those of the Forum on Microbial Threats, its sponsors, or the Institute of Medicine. The contents of the unattributed sections are based on the presentations and discussions at the workshop.
The workshop summary is organized into chapters as a topic-by-topic description of the presentations and discussions that took place at the workshop. Its purpose is to present lessons from relevant experience, to delineate a range of pivotal issues and their respective problems, and to offer potential responses as discussed and described by the workshop participants.
Although this workshop summary provides an account of the individual presentations, it also reflects an important aspect of the Forum philosophy. The workshop functions as a dialogue among representatives from different sectors and allows them to present their beliefs about which areas may merit further attention. The reader should be aware, however, that the material presented herein expresses the views and opinions of the individuals participating in the workshop and not the deliberations and conclusions of a formally constituted IOM consensus study committee. These proceedings summarize only the statements of participants in the workshop and are not intended to be an exhaustive exploration of the subject matter or a representation of consensus evaluation.
Globalization: Processes, Patterns, and Impacts
The inexorable migration of the human species has profoundly influenced Earth’s ecology. As our ancestors wandered across the African continent, onward
|
BOX WO-1 Factors Involved in Infectious Disease Emergence
SOURCE: Reprinted from Lancet Infectious Diseases, Morens et al. (2008), with permission from Elsevier. |
to Asia, Australia, Europe, and eventually to the Americas, as we explored the ends of the Earth and beyond the confines of this planet, the vast entourage of animals, plants, and microbes that have accompanied us on our journeys has only amplified the impact of our species on every ecosystem that we have encountered.
Among these “fellow travelers,” pathogens have flourished in new surroundings, while other microbes have colonized incoming migrant host species. Such introductions, abetted by additional genetic, biological, social, and political factors associated with infectious disease emergence (see Box WO-1), have given rise to epidemics throughout recorded history (IOM, 2003; Morens et al., 2008). The current era of “globalization” affords frequent and widespread opportunities for disease emergence, several of which are described in detail in later sections of this overview. This section summarizes two presentations that opened the workshop by exploring the history and ongoing political and public health significance of human migration and mobility.
Human Migration: Past, Present, and Future
In his overview of the history of human migrations, speaker Mark Miller, a professor of comparative politics at the University of Delaware, emphasized migration’s growing political importance (see Miller in Chapter 1). Considering
the present status of global migration as an indicator of future trends, he observed that, “increasingly, the questions of peace and war revolve around migration.”
Highlights of Miller’s whirlwind tour of historic migrations included the fourth-century convergence of a “crazy quilt” of ethic groups to establish the country we now call France; the movement of Celts and Jews into Europe; the travels of Vikings throughout the North Atlantic; and the eastward migration of Germans, counter to other population flows across Europe. He noted that between 8000 B.C.E. and the seventeenth century, four civilizations achieved “a rough kind of equilibrium” on the Eurasian steppe: one was derived from Greece and Europe, one was of Middle Eastern origin, another was Indian, and the last was Chinese.
Following that era, Miller noted, Europeans migrated to the Americas driven by several factors, including:
-
A population explosion in Europe,
-
Development of resistance to diseases of the New World,
-
The advent of capitalism, and
-
The availability of affordable long distance travel.
Despite the fact that this influx of Eastern Europeans at the end of the nineteenth and beginning of the twentieth centuries led to the emergence of the United States as a world power, American suspicion of the “foreign born” greatly restricted immigration between World War I and the 1960s.4,5
A “new age of migration” began in the 1970s, when longstanding migration patterns reversed, rendering Europe a destination for immigrants. Concurrently, Latin America became a net source of new migrants to the United States, and immigration from Asia and Africa also increased. Today, as a result of what Miller called the single most important relationship in the New Age of Migration, approximately 10 percent of Mexico’s population resides in the United States, and Mexicans comprise about 5 percent of the U.S. workforce. These circumstances are “emblematic of the increasing impact of migration around the globe,” he concluded.
Miller predicted that as the global population grows unevenly—faster in developing countries, more slowly and even negatively in developed countries—migration will increase (see also Gushulak and MacPherson in Chapter 1). “Thirty years ago there were two Europeans for every African,” he noted, citing United
Nations population estimates. “Today there are about equal numbers of Africans and Europeans. In 30 years, there will be twice as many Africans as Europeans.” These differences are likely to produce a world of regions that differ greatly from each other, he continued, with “fundamental differences separating the rich countries from the poor countries.”
Population Mobility and Public Health
While migration issues have become increasingly salient in politics and diplomacy, Miller observed that relatively little attention has been paid to the relationship between migration and health.6 Yet as speaker Brian Gushulak, of the Canadian Immigration Department Health Branch, explained, this link is becoming increasingly crucial, as the widening economic gap separating countries and regions both contributes to, and results from, health disparities.
“It is possible to look at migration and population mobility as a metaphor for the evolution of public health and public health security,” Gushulak remarked, as he traced the history of public health through the various means advanced against introduced diseases (see Gushulak and MacPherson in Chapter 1). Echoing Miller’s conclusion that we have reached a new age of unprecedented migration, Gushulak noted that in the mid-1990s, approximately 200 million people—a population exceeding that of all except the worlds’ four largest nations—fit the United Nation’s definition of “migrant.”
Several major changes to immigration ushered in the current era:
-
Post-colonial population flows;
-
Refugee movements and displacements associated with humanitarian emergencies and conflicts;
-
The development of the concept of human capital and employment of international temporary workers; and
-
The increasing ease and declining cost of international transportation.
Together, these factors have produced unprecedented demographic changes in receiving countries, rendering disease control processes and policies based on historical patterns of migration irrelevant, according to Gushulak. “We simply can’t keep up on a policy level as fast as the ground is changing underneath our feet,” he said.
Modern human movements and migration practices have also become increasingly difficult to characterize, due to the diverse origins of migrants,
their often complex journeys, the variety of their experiences upon arrival and resettlement, and the frequency with which many migrants return to their countries of origins for varying lengths of time. Moreover, in addition to migration in the traditional sense (the one-way movement of people from one homeland to another), nonmigratory human travel and trade7 provide pathogens with a wealth of possibilities for relocation. Gushulak employed the more encompassing term “mobility” to describe this collection of processes, all of which contribute to the phenomenon of globalization.
Since pathogens readily cross geopolitical borders, only “functional disease-based borders” matter, Gushulak argued. These boundaries occur between regions that differ not only in terms of disease epidemiology, but also reflect general health disparities due to socioeconomic factors such as poverty, education, housing, nutrition, and access to care (see Figure WO-1). Mobile people (as well as animals and plants) serve as biological bridges between such disparate regions, thwarting attempts to confine infectious diseases within—or exclude them from—national borders. Controlling the spread of infectious diseases across such functional borders will require international cooperation in surveillance and reporting, Gushulak concluded, and mitigation or intervention strategies that focus on mobility as a determinant of global public health, rather than on the containment of specific diseases.
Travel, Conflict, Trade, and Disease
In discussions that focused on the rapid acceleration and expansion of international travel and trade as a catalyst of pathogen movements, workshop participants considered various ways in which the movement of people and goods influences the transmission dynamics of infectious diseases, and how these influences might be better understood in order to reduce the global burden of emerging infectious disease. Workshop presentations examined the role of the traveler as a sentinel—as well as a vector—for disease; the role of armed conflict in increasing infectious disease risks; the complex and multifaceted relationship between trade and disease; and the numerous and diverse risks associated with a globalized food supply.
Traveling Pathogens
Figures WO-2, WO-3, and WO-4 provide graphic illustrations of the current state of global connectivity afforded by planes and ships (as well as cars, trucks, and trains) that transport infected travelers, goods, and disease vectors rapidly across vast distances. They also allow adventurous travelers to enter new
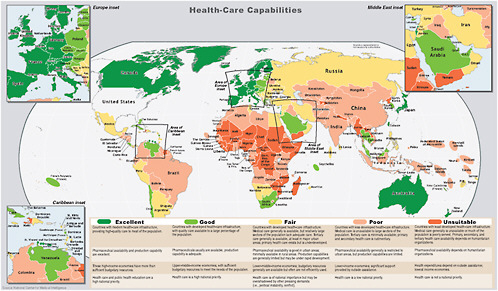

FIGURE WO-2 The rate of globalization has accelerated to the point where we are connected as never before via globalized travel and trade networks.
SOURCE: Reprinted with permission from Hufnagel et al. (2004).
ecosystems and pick up new pathogens, which may then return with the traveler to a new environment and, under appropriate circumstances, persist and spread through new host populations.
The mobility of the global biota is one among many interacting factors that contribute to infectious disease emergence: growing populations of humans and food animals living in increasingly close proximity to each other, climate change and extreme weather events, and changes in land use (IOM, 2003). This upheaval occurs against a backdrop of microbial evolution, remarked Mary Wilson of Harvard University, whose presentation explored the influence of human travel on the geography of infectious diseases, as well as the role of the traveler as a disease sentinel (see Wilson in Chapter 2). She noted that, in addition to enabling pathogens to span vast distances through direct transmission, travel also introduces antimicrobial resistance genes to new populations.
Some pathogens spread quickly upon introduction to a new environment, while others do not survive the transition for lack of an appropriate environment, vector, or host, Wilson observed. Introduced pathogens may meet with vulnerable
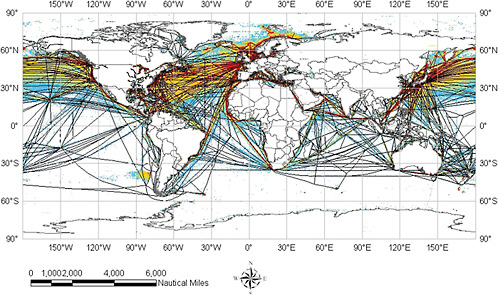
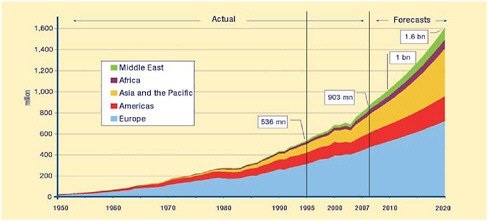
FIGURE WO-4 International tourist arrivals by region (in millions), 1950-2020.
SOURCE: Reprinted with permission from the UNWTO (2008).
hosts—for example, people with low levels of immunity to the pathogen, or those who live in a community with poor housing, water quality, and sanitation—or with resilient ones. If an introduced pathogen produces an epidemic, it may or may not be easy to control. The ease with which spread of infection can be interrupted is determined, to a large extent, by the proportion of transmission that occurs before the onset of symptoms or during asymptomatic infection (Fraser et al., 2004). For this reason, Wilson explained, SARS was relatively easy to control, while HIV/AIDS continues to spread, unabated, as a “silent” pandemic.8
Vector-borne pathogens can travel with relative ease in the blood of viremic hosts, such as human travelers, and upon introduction to a new environment with competent vectors, spread quickly through a new host population, Wilson said. This scenario appears to have occurred in the recent emergence of chikungunya fever in new geographic areas and the expanding distribution of dengue viruses in tropical and subtropical areas. A recent study of trends in emerging infectious diseases finds that emergent events involving vector-borne diseases are occurring with increasing frequency (Figure WO-5; Jones et al., 2008).
Travelers as Sentinels
Travelers represent an important sentinel population for disease emergence, according to Wilson, who added that several surveillance networks have been developed to monitor infectious diseases in travelers. She is involved in the decade-old
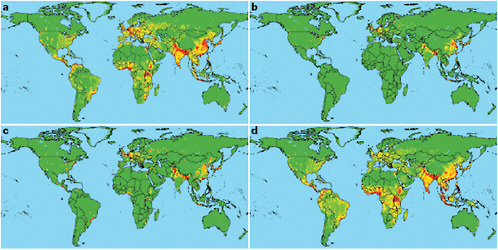
FIGURE WO-5 Global distribution of relative risk of an emerging infectious disease (EID) event. Maps are derived for EID events caused by (a) zoonotic pathogens from wildlife, (b) zoonotic pathogens from nonwildlife, (c) drug-resistant pathogens, and (d) vector-borne pathogens.
SOURCE: Reprinted from Jones et al. (2008) with permission from Macmillan Publishers Ltd. Copyright 2008.
GeoSentinel Surveillance Network, which gathers information on ill international travelers and migrants from 42 travel and tropical medicine clinics on six continents, in order to provide early alerts about unusual infections or infections in unusual locations or populations. Much as Gushulak (see previous section and Gushulak and MacPherson in Chapter 1) noted that contemporary human migrations may be complicated by return visits and exchanges of goods, Wilson recognized that travel frequently consists of multiple stages, each of which—including time in transit—has potential significance to infectious disease transmission. And like Gushulak, Wilson emphasized dramatic differences in the incidences of many infectious diseases (Gushulak referred to these differences as “functional disease-based borders”) between countries and regions. For example, Wilson said, tuberculosis incidence differs by more than 100-fold between some areas of the world. “If we are regularly traveling from one area to another, it becomes very easy to share some of these [infectious diseases],” she observed. Controlling them will require looking beyond local outbreaks to regional and global patterns of transmission, she concluded.
Armed Conflict and Infectious Disease
In wars and other armed conflicts, public health is compromised, increasing the burden of illness, disability, and death. Studies of mortality during the recent civil war in the Democratic Republic of the Congo found that most deaths during that war were due to the breakdown of health-supporting infrastructure of society, including medical care, supply of safe food and water, sanitation and sewage systems, power generation, transportation, and communication (Coghlan et al., 2007; Van Herp et al., 2003).
Certain categories of infectious diseases tend to increase during war, according to speaker Barry Levy of Tufts University, including diarrheal diseases, acute respiratory infections, and tuberculosis (see Levy in Chapter 2). He described the following major causes of wartime infectious diseases:
-
Adverse effects on medical care and public health services,
-
Damage to the health-supporting infrastructure and the environment,
-
Forced migration, and
-
Diversion of resources from health care and health-supporting services.
Measures can be implemented to reduce the frequency of infectious disease during armed conflict. The elimination of infectious disease during armed conflict, however, will require the elimination of armed conflict—the creation of a world without war.
Trading Pathogens
Like travel, globalized trade is vast, rapid, increasing, and a significant risk factor for infectious disease emergence. In her book Risky Trade: Infectious Disease in the Era of Global Trade (2006), speaker Ann Marie Kimball, of the University of Washington, concluded that “market forces in the globalized world are misaligned for microbial safety.” Using examples of diseases including avian influenza, the use of antibiotics in farm animals, and the growing practice of xenotransplantation,9 she demonstrated the profound influence of trade on infectious disease emergence, and vice versa (see Kimball and Hodges in Chapter 2).
Poultry production and H5N1 influenza The rapid expansion of intensive poultry farming10 in Asia, shown in Figure WO-6, immediately preceded the H5N1 outbreak of 2003, which Kimball characterized as an “ecological tipping point,” as well as an economic disaster. Based on this experience, she remarked, “one could question, and certainly should carefully research, whether intensive poultry agriculture is actually safe at all.”
On the other hand, Forum member Michael Osterholm, of the University of Minnesota, argued that in his experience “the best and the safest poultry production in the world right now is occurring in … very large facilities, where biosecurity is actually very high.” In India, 70 percent of all poultry is produced by a single company, which has high standards for biosecurity and an excellent safety record, he asserted. “Our experience, in Asia in particular, has been that all the H5N1, and even the low-pathogenicity [influenza] viruses, have … [been limited to] backyard range production.” This is also true in the United States, Osterholm continued. Migratory birds bring in most influenza viruses, and “we see very, very, very little influenza virus activity in our poultry production, where we have high biosecurity [as] required in large facilities.”11
Kimball responded that, while replacing backyard poultry farming with industrialized poultry production in impoverished areas of Asia might lead to gains in biosecurity, it would compromise the access of poor people to poultry protein because the pricing of poultry from industry is unaffordable compared to the gate price of backyard poultry.
Therefore, she said, she would prefer to better understand how the introduction of intensive poultry facilities into areas with backyard farms contributed to the emergence of H5N1 in humans, and thereby mitigate future risks. Osterholm
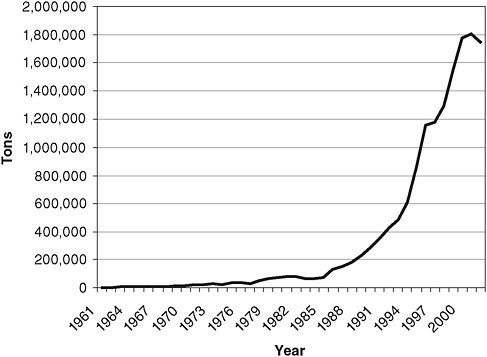
FIGURE WO-6 Poultry exports from Far East Asian countries from 1961 through 2002.
SOURCE: Based on data in FAOSTAT 2003 and reprinted from Kimball (2006) with permission from Ashgate Publishing.
agreed with the importance of such research, in which he participates, but warned that controlling H5N1 in backyard flocks is extraordinarily difficult.
Trade in beef and prion diseases The emergence of two prion diseases, bovine spongiform encephalopathy (BSE) and new-variant Creutzfeldt-Jakob disease (NvCJD), following the entry of the United Kingdom (UK) into the World Trade Organization (WTO), illustrates a similar, but more complex, dynamic relationship between trade and disease. Entry into the WTO required the UK to abandon certain protective tariffs for its beef producers who, due to their resulting need to lower prices, shifted to a less-expensive rendering process that did not deactivate prions. Contrary to popular belief, the practice of feeding sheep offal to cattle as a protein source had been practiced in the UK for decades without incident, Kimball explained. The problems began when processors changed from a batch-rendering process that deactivated prions, to a lower-temperature, continuous vacuum-extraction process that did not. Meat and bone meal produced in this way was used to make animal feed, the vehicle through which prions spread around the world.
While researchers are still discussing the validity of the prion hypothesis and whether prion disease in cattle can be transmitted to beef-eating humans, those debates have long been settled among consumers and commercial interests, Kimball observed. As a result, in 1996, when case-control studies suggested a possible link between BSE and British beef, UK beef exports declined precipitously.
Trade in risky therapies Market forces favoring medical tourism12 and xenotransplantation are also raising the risks for disease emergence, according to Wilson and Kimball. Kimball noted that organ transplantation is becoming increasingly common, and the pig has become a popular, relatively low-cost source for islet cells (to reverse type 1 diabetes that cannot be managed with insulin therapy) and, occasionally, kidneys as well. Kimball noted that in the United States, only heart valves from pigs may be legally transplanted into humans; in India, porcine islet cells and other organs are also transplanted, as well as precursor stem cells from rabbits.
Concern that endogenous animal retroviruses will be introduced into humans through xenotransplantation prompted the World Health Assembly to pass a 2004 resolution urging member states “to allow xenogeneic transplantation only when effective national regulatory control and surveillance mechanisms overseen by national health authorities are in place” (WHA, 2004). Kimball noted that researchers are attempting to address these risks by breeding endogenous retroviruses out of pigs (Scobie and Takeuchi, 2009) and by encapsulating transplanted porcine islet cells within human cells prior to transplantation (Thanos and Elliott, 2009). However, Kimball observed that it would be difficult to find a transplant site so remote (i.e., South Asia) that complications of porcine transplants done at that site will never be seen in U.S. hospitals or clinics.
Responses to Risky Trade
Securing the globalized U.S. food supply A detailed description of infectious disease threats associated with the globalization of the U.S. food supply appears in a recent Forum workshop summary, Addressing Foodborne Theats to Health (IOM, 2006), which featured remarks and a contributed paper from Forum member David Acheson, of the U.S. Food and Drug Administration (FDA). In his presentation to this workshop, Acheson noted several examples of imported threats to food and drug safety recently encountered by the FDA (see Acheson in Chapter 2).
“American consumers want all kinds of food, and they expect it to be available year-round,” Acheson observed. Approximately 15 percent of all food consumed in this country is imported, and food safety standards in many importing nations are far less stringent than in the United States, he reported. Recent experiences, including the 2008 outbreak of Salmonella Saintpaul (and the laborious process by which it was traced to Serrano peppers grown in Mexico), as well as the deliberate contamination of wheat gluten with melamine for economic purposes in China, have compelled the FDA to take a more proactive stance in addressing foodborne threats, Acheson explained. Rather than continue to focus its efforts on reacting after the fact to the importation of tainted raw and processed food items, the FDA is now becoming much more proactive by seeking to understand foodborne threats at the point of origin, to anticipate their potential to spread globally, and to use risk-based inspections to detect these contamination events prior to an outbreak occurring in the United States. In his contribution to Chapter 2, Acheson describes efforts under way to increase the agency’s presence in foreign countries, to develop model systems for risk-based inspections, and to make use of inspection and testing data generated by industry or other “third parties” to increase the breadth and depth of their surveillance.
Partnering with the private sector “The globalization of health … has lagged behind economic globalization and business globalization and commerce globalization, because [the latter processes] … are market-driven and [public health] is not,” Kimball observed. To address this gap, she advocated inclusion of the private sector in efforts to improve the exchange of information on infectious disease threats at all levels, from local to global (see the final section of this summary and Bell in Chapter 5 for further discussion of this topic). Kimball’s work with the Asia Pacific Economic Cooperation (APEC) exemplifies such a private-public partnership.
As part of their effort over the past 14 years to create a “community of interest in health” involving the 21 nations comprising APEC, Kimball and her colleagues have sought to create a platform for rapid communications among member nations as a way to develop working relationships focused on health. The Emerging Infections Network (EINET) affords APEC members enhanced communications, opportunities for collaboration, and improved preparedness for infectious disease events. In so doing, Kimball says, APEC hopes to apply lessons learned from SARS to the threat of avian influenza.
Mobile Animals and Disease
As discussed in the previous section and in a previous workshop summary report of the IOM’s Forum on Microbial Threats—Addressing Foodborne Threats to Health (IOM, 2006)—trade in livestock, poultry, and foodstuffs made from animals has hastened the emergence of several important zoonotic diseases,
including H5N1 influenza and BSE. Here, we consider additional mobile animals, such as pets, wildlife, research animals, and insect vectors (with and without their various hosts). They are also sources and sinks for introducing novel diseases into naïve ecosystems—or changing ecosystems in ways that alter transmission dynamics of existing infectious diseases. Workshop presentations and discussions provided examples of infectious diseases associated with various types of mobile animals, as well as the regulatory and research responses to these evolving threats.
Recognition and Response: The CDC Perspective
According to U.S. Fish and Wildlife Service data, more than 136,000 live mammals (including 29 different species of rodents) were legally imported into the United States in 2006, as well as 243,000 birds, 1.3 million reptiles, 4.6 million amphibians, and 222 million fish (personal communication between Nina Marano, CDC, and Kevin Garlick, U.S. Fish and Wildlife Service, July 10, 2008). Since 2000, more than half a million shipments containing in excess of 1.48 billion live animals have been imported by the United States (Smith et al., 2009). Exotic pets13 are readily available in the United States and other wealthy countries, and their popularity is growing, according to speaker Nina Marano, of the Centers for Disease Control and Prevention (CDC). Animals imported into the United States can be purchased online for home delivery, or bought at local “swap meets,” Marano explained.
Four U.S. government agencies, including the CDC, regulate the importation of animals based on their risk for zoonotic disease; the others are the Department of Homeland Security (Customs and Border Protection), the Department of Agriculture (Animal and Plant Health Inspection Service), and the Department of the Interior (Fish and Wildlife Service). Marano described the CDC’s response in recent years to a series of novel animal disease threats (see Marano et al. in Chapter 3). This effort has included the following:
-
The development of the agency’s non-human primate program in response to an outbreak of Ebola hemorrhagic fever among monkeys destined for
-
medical research that were housed in a quarantine facility in Reston, Virginia, in 1989 (CDC, 1990). This program instituted new requirements for the importation of primates, specifically requiring that the importers isolate and quarantine imported animals in a CDC-approved facility for 31 days upon entering the United States.
-
The prohibition of interstate transportation, sale, distribution, or release into the environment of native prairie dogs and six species of African rodents implicated in a multistate outbreak of monkeypox14 in 2003 (CDC, 2003). This was a joint order issued by the CDC and the FDA; the FDA lifted the ban on interstate movement of prairie dogs in September 2008.
-
Enhanced surveillance and analysis to address the importation of bushmeat,15 a potential source of zoonotic viruses including the human immunodeficiency virus (HIV), simian immunodeficiency virus (SIV), and the Ebola virus.
-
The embargo of birds imported from countries with H5N1 influenza.
To date, the CDC’s regulatory actions to address disease threats from imported animals “have been very reactive … species-specific and very pathogen-specific,” Marano said. Much like the FDA as described by Acheson (see previous section and Chapter 2), the CDC is moving toward more proactive regulation of imports, according to Marano. The agency seeks broader restrictions, such as those proposed in a recent bill introduced in the House of Representatives entitled the Non-native Wildlife Invasion Prevention Act (U.S. Congress, House, 2008). Should this legislation become law it would require that every nonnative wildlife species proposed for importation into the United States receive a risk assessment, including identification to the species level, geographic source, and likelihood that importation could harm other species and habitats in the United States.
“For public health purposes we need a risk-based, proactive approach to preventing the importation of animals and vectors that pose a zoonotic disease risk,” Marano and coauthors conclude in their contribution to Chapter 3. “The risk-based approach should include systematic and targeted surveillance of high-risk animals and animal products and vectors in the countries of origin. Emphasis should be placed on restricting the importation of animals and vectors of diseases not already present in the United States.”
Mosquitoes on the Move
As is noted in the summary of a recent Forum workshop, Vector-Borne Diseases: Understanding the Environmental, Human Health, and Ecological Connections (IOM, 2008a), the rapid expansion of global trade and transportation has been associated with the spread of mosquitoes and mosquito-borne diseases such as dengue and chikungunya. Thanks to today’s globalized economy, these vector-borne diseases—once considered well controlled in industrialized countries—are poised for resurgence, while others, such as West Nile viral fever and chikungunya, have significantly expanded their geographic range (IOM, 2008b).
Speaker Paul Reiter, of the Institut Pasteur, described the distribution pathway that followed from the first U.S. detection of Aedes albopictus, the Asian tiger mosquito, which he captured in Memphis, Tennessee, to his discovery, three years later, that these mosquitoes were being shipped all over the world in used tires (see Reiter in Chapter 3). “There was a world trade in used tires, tens of thousands of used tires being shipped all over the world from Japan particularly,” he recalled. “Japan was shipping at that time to137 different countries.” As a result, he continued, Ae. albopictus is now well established in the United States as far north as Chicago, as well as in 13 European countries, and several African countries. In Africa, Reiter reported, this species has been implicated in the transmission of yellow fever and chikungunya.
These and other diseases described by Reiter in his contribution to Chapter 3 have expanded their geographic range thanks to traveling hosts, vectors, and ease of shipping and transportation. Yellow fever spread to the Americas upon the arrival of slave ships bearing both infected travelers and a highly competent vector, Ae. aegypti, that bred in barrels of potable water, Reiter noted (Crosby, 2006). Chikungunya arrived in Italy—where its vector Ae. albopictus was already present in the environment—in the guise of a viremic traveler from India who visited family members in the small northern town of Castaglione (see Box WO-2). The ensuing outbreak resulted in 205 confirmed cases of the disease (Rezza et al., 2007).
“There has been a quantum leap in the movement of vectors and the movement of pathogens,” Reiter concluded, noting the recent emergence of vector-borne diseases ranging from dengue fever in Hawaii (a small outbreak in a small, relatively isolated community of globe-trotting surfers), to trypanosomiasis in France (brought in by camels), to the arrival of bluetongue virus in Europe (in midges blown in from Africa [IOM, 2008b; Osburn, 2008]), which he predicted would herald “a major tragedy in European agriculture.”
Invasive Species
Introduced animals, plants, and microbes can disrupt ecosystems in ways that increase the potential for infectious disease outbreaks. The term “invasive species” is widely used to describe plants and animals that, when introduced to and
|
BOX WO-2 The Travels of Chikungunya The chikungunya virus, an alphavirus of family Togaviridae, was originally isolated in Tanzania in 1953. The virus circulates among monkey populations in the forests of that country. It is transmitted by mosquitoes of the genus Aedes, particularly Aedes aegyptii (which is widely distributed in the Americas today) and Aedes albopictus. Nosocomial transmission of chikungunya by needle stick has been reported. Chikungunya received relatively little attention until a recent series of explosive outbreaks began in African coastal cities in 2004, and afterward in islands in the Indian Ocean, in mainland India, elsewhere in Asia (most recently, in Thailand and Malaysia), and in Italy (Figure WO-7). There have been thousands of chikungunya infections in travelers, most notably an Indian man whose visit to family members in Castaglione, Italy, in 2007, ignited a localized outbreak of chickungunya fever. The vector in this case was Ae. albopictus, which was introduced to Italy in used tires imported from the United States, which in turn received the species in used tires imported from Japan. Symptoms of chikungunya infection include rash, myalgia,a headache, arthralgiab (which tends to be severe, incapacitating, and persistent), and fever. The virus has a high attack rate, so it can disable entire populations upon its introduction. An apparently recent mutation in the chikungunya virus improved its efficiency of transmission by Ae. albopictus; this may explain the explosiveness of recent outbreaks (Tsetsarkin et al., 2007). Although many cases of chikungunya have been imported to the Americas, to date none of these have resulted in transmission. However, a recent study found that Ae. aegyptii and albopictus strains present in the United States could be infected with, and could subsequently transmit, recent outbreak strains of the virus (Reiskind et al., 2008; Vazeille et al., 2007). 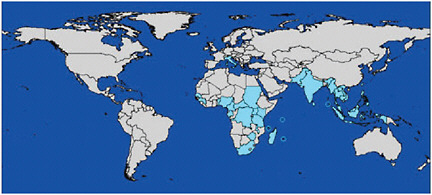 FIGURE WO-7 Approximate global distribution of chikungunya virus, 2008. SOURCE: Modified from Powers and Logue (2007); reprinted from CDC (2008a). |
established in new environments, spread aggressively (Dybas, 2004). Ecologists, including speaker Andrew Dobson of Princeton University, apply the concept of biological invasion to describe pathogen transmission and persistence at the population level.
Dobson’s presentation considered several pathogen-host relationships in this context. A typical invasive species, the European green crab (Figure WO-8), found few of its own host-specific pathogens in its new home on the west coast of the United States, and so can grow to many times the size of its native-born brethren. An atypical invader, the house finch, at first expanded rapidly across the United States in ever-larger flocks; however, flocks that encountered conjunctivitis-causing mycoplasmas in their travels experienced massive, density-dependent population crashes. In general, Dobson said, invasive host species have a major advantage over native ones because the invaders have escaped their parasites (Torchin et al., 2003).
Examining the relative success of various invasive plant species in California, Dobson and colleagues determined that “the things that come in and cause you the biggest problems are going to be similar to the things that are already there” (Seabloom et al., 2006). Applying this principle to emerging diseases, he expressed

FIGURE WO-8 Size comparison of largest green crabs caught from a parasitized population in the crab’s native range (left) and unparasitized population in the crab’s introduced range (right).
SOURCE: Reprinted with permission from the Ecological Society of America from Torchin and Mitchell (2004). Photo credit: Jeff Goddard.
great concern regarding diseases that resemble measles, such as the Nipah and Hendra viruses, for which bats provide a reservoir (see Dobson and Cleaveland in Chapter 3). Because “anything that is like measles that gets into humans [is likely to] stay,” Dobson and colleagues are creating mathematical models that describe Nipah virus behavior at the level of host populations, identifying patterns that could be used to provide early warning of an outbreak.
Dobson also described efforts by his group to apply ecological insights from other biological invasions to predict outbreak risks for the H5N1 influenza A virus. By examining influenza outbreaks in European duck populations, they discovered that the ducks migrate ahead of cold fronts, aggregating in larger and larger groups (in which, presumably, disease could spread quickly) as the weather becomes colder. He also noted that complex models, involving two or more duck species, consistently show that when several possible hosts are available to a pathogen, it becomes persistent (endemic) and relatively stable. An important way to build resilience against zoonoses and non-host-specific infectious diseases, according to Dobson, is to make diverse and abundant host species available to pathogens. For example, Dobson said, if he found himself in one of the several locations in India where 99 percent of mosquito bites occur in cattle, he “would much rather go buy a cow than have a malaria vaccine.”
Some participants questioned the general applicability of Dobson’s influenza model, based on their own research findings. Osterholm remarked that his data from Asia would not suggest that H5N1 outbreaks were associated with cold fronts; instead, he has noticed that feeding opportunities, such as crab breeding seasons, often drive bird crowding. Osterholm warned against the tendency of models to obscure such complexity with “precision and graphic clarity.” Dobson argued that models such as his help researchers to examine problems in an appropriate spatial and temporal scale. “To get at the complexity [of disease emergence] you have got to look at the community level … [and] at the interaction with climate, and on a big enough geographic scale to understand processes on the scale at which they work,” he insisted. “To me the power of the models isn’t what they tell you, it is what they tell you to go and look at next.”
To create more and better predictive population dynamic models of infectious disease emergence, “we need to spend much more money on data collection and surveillance” and in training scientists to analyze the results, Dobson declared. “There are more knee surgeons than we have mathematical epidemiologists who understand how to do these analyses,” he complained, adding that “there is no longer any NIH funding for [the study of] population dynamics in infectious diseases.”
Predicting the consequences of movements of agents, vectors, or pathogens, and preventing the most harmful among them, is likely to require a variety of approaches, observed Forum Chair David Relman, of Stanford University, at the close of the discussion that followed Dobson’s presentation. Progress toward this goal can be made by applying a wide range of scientific tools, drawn from a variety
of disciplines, he added; these include both modeling and measurement in order to acquire “better ground truth data.”
Global Public Health Governance and the Revised IHR
As globalization renders national and geographic boundaries increasingly porous and from an infectious disease standpoint practically meaningless, infectious disease control demands international cooperation and coordination. This became abundantly clear in 2003 when SARS emerged in China and rapidly spread to North America.
The public health response to SARS demonstrated the effectiveness of recently established global information and response networks (see Heymann in Chapter 4). While yet unnamed, SARS was identified in Asia by the Global Public Health Information Network (GPHIN) and other networks such as ProMed; within a week, members of the Global Outbreak Alert and Response Network (GOARN) in 26 institutions and 17 countries, as well as field teams, were exchanging information about the outbreak in real time. Their findings were used by the WHO to make timely travel recommendations in order to contain the global spread of SARS, and recommendations on best practice for clinical management.
The SARS event provided a powerful rationale and catalyst for global public health governance, according to presenter David Heymann, of the World Health Organization (WHO).16 In the months following this workshop, the emergence of swine origin influenza A (H1N1) virus prompted the WHO to take actions authorized under the IHR for the first time since their revision in 2005 and underscored the value of global coordination of infectious disease control (see Chapter 4).
The IHR 2005: A New Era in Global Governance17
Heymann explained that the emergence of SARS in 2003 was a major catalyst toward a fundamental revision of the IHR that had begun in 1995; that process was completed in 2005 and the regulations took effect in 2007. The original IHR, established in 1969, were preceded by a long history of multinational public health measures designed to control the spread of infectious diseases across national borders (see also Gushulak and MacPherson in Chapter 1). The IHR 1969 were intended to monitor and control six diseases—cholera, plague,
smallpox, relapsing fever, typhus, and yellow fever—whose occurrence required WHO notification (WHO, 2005). Following revisions in 1973 and 1981, only three “notifiable” diseases remained: cholera, plague, and yellow fever.
By the mid-1990s, the IHR 1969 appeared obsolete. A vast number of global microbial threats had emerged and reemerged, including many diseases that were not deemed “notifiable,” such as Ebola hemorrhagic fever (IOM, 2007; WHO, 2005). There was also concern that the IHR dependence on “official” country notification, along with a lack of a formal, internationally coordinated mechanism to contain the international spread of disease, might fail to contain a disease with pandemic potential (WHO, 2005). Several resolutions passed by the World Health Assembly (in 1995, 2001, and 2003) encouraged revision of the IHR; the final resolution—WHA58.3—formally adopting IHR 2005, passed on May 23, 2005.
As of June 15, 2007, when revisions to the IHR came into force, member nations of the WHO are required to report all new and reemerging diseases with epidemic or pandemic potential, as well as chemical, radiological, and food-related threats, irrespective of their origin or source (WHO, 2008). Speaker May Chu of the WHO noted that the IHR 2005 provides a specific decision instrument for this purpose, based on the following four questions:
-
Is the public health impact of the event serious?
-
Is the event unusual or unexpected?
-
Is there a significant risk of international spread?
-
Is there a significant risk of international travel or trade restrictions?
If the answer to any two questions is “yes,” the member nation is compelled to notify the WHO of the event, Chu explained. Upon investigation of such a report, the WHO may declare such an event to be a “public health emergency of international concern (PHEIC),” triggering a specific response (see Chu et al. in Chapter 4). This occurred for the first time on April 25, 2009, in the case of swine-origin influenza A (H1N1) virus (see contributions by Chu and Fidler in Chapter 4).
Chu also discussed the second key obligation of signatories to the IHR 2005: to develop the capacity to detect, assess, notify, and report a possible PHEIC. Member nations are required to assess their disease surveillance capacity and develop national action plans by 2009. By 2012, member states must meet standards for national surveillance and response systems, as well as for designated airports, ports, and ground crossings (extensions may be obtained, however).
Chu observed that instructions with regard to capacity-building within the IHR 2005 were flexible, enabling its 194 member nations to build or access (via outsourcing) disease surveillance and investigational capacity. However, she added, the IHR 2005 provide an insufficient basis for evaluating some crucial areas, such as laboratory requirements (e.g., quality assurance). Members of the
public health community, including several workshop participants, have contended that the IHR 2005 insufficiently address economic barriers to reporting infectious outbreaks, and cannot succeed unless supported by funding for public health capacity-building in developing countries (Fidler and Gostin, 2006).
Challenges to IHR 2005
Although preceded by more than a century and a half of international sanitary conventions (Stern and Markel, 2004), the IHR 2005 represent a “radical departure from all previous uses of international law for public health purposes,” according to speaker David Fidler, of Indiana University (Fidler and Gostin, 2007; see also Fidler in Chapter 4). He noted five attributes that set the IHR 2005 apart from their predecessors:
-
Significant expansion of epidemiological and political scope,
-
Obligations for member states to develop and maintain minimum core capabilities for surveillance and response,
-
Empowerment of WHO to collect and use information from nongovernmental sources,
-
Authorization of the WHO Director-General to declare a public health emergency of international concern, and
-
Incorporation of human rights concepts and principles requiring that WHO member states apply public health powers according to principles of international human rights law.
However, Fidler observed, “the mere existence of radical changes in the IHR 2005 does not guarantee that the IHR 2005 will radically change global health.” He noted that global crises—including energy, food, climate change, and most recently, the precipitous downturn of worldwide financial markets—have overshadowed the threat of infectious diseases, causing the effort to implement the IHR 2005 to lose momentum. The emergence of the swine-origin influenza A (H1N1) pandemic briefly raised the priority of health issues in foreign policy, but as Fidler observed in his contribution to Chapter 4, when the outbreak began to resemble seasonal flu rather than the 1918-1919 pandemic, global health faded quickly from political prominence.18 This event and other recent experiences in global health governance, including but not limited to the worldwide campaign to eradicate polio, the issue of “viral sovereignty,” and the global responses to the
swine-origin influenza A (H1N1) virus, described below, highlight the limitations of the IHR 2005 as an instrument for international cooperation and coordination, while revealing the crucial role of global governance instruments in addressing infectious disease threats.
Polio eradication Between 1988 and 2003, efforts to control polio reduced its presence from 125 to only 6 countries, according to Heymann (see Chapter 4). This progress was halted, and then partially reversed, when politicians in northern Nigeria used an Internet rumor that polio vaccine sterilized young girls as a basis for suspension of polio vaccination programs. Heymann described a range of approaches undertaken by the WHO to remedy this situation, including testing vaccines for impurities or hormones that could cause sterility and discussions with a wide range of political, medical, and religious persons and groups of influence, without success. Only after press reports of World Health Assembly resolutions strongly condemning the Nigerian government for suspending polio immunization reached the country’s citizens did their president agree to “do everything humanly possible to ensure that polio is finally and totally eradicated from Nigeria.” Thereafter, polio vaccination programs were resumed in northern Nigeria.
When polio eradication is achieved, the IHR 2005 could be used to ensure the simultaneous, global cessation of oral polio vaccinations, so that no country is put at risk, Heymann said. However, when this measure was recently proposed to the World Health Assembly, it was not accepted, nor was a proposal to address the destruction or consolidation in secure laboratories of wild polioviruses under the IHR. Thus, Heymann observed, although the IHR 2005 were negotiated and established as an international convention, “there is still hesitancy to use these regulations as many in public health had hoped they would be used.”
Viral sovereignty In 2006, Indonesia refused to share samples of the H5N1 avian influenza virus, collected within the country, with the WHO’s H5N1 influenza surveillance team (see contributions by Fidler and Heymann in Chapter 4). Instead, Indonesia claimed “viral sovereignty” over these samples, and announced that it would not share them until the WHO and developed countries established an equitable means of sharing the benefits (e.g., vaccine) derived from viruses collected within its borders. “Indonesia argued that it took these actions because it, and other developing countries, was not gaining benefits in terms of response capabilities from sharing of virus samples for purposes of global surveillance,” Fidler said. Indonesia criticized WHO’s practice of distributing influenza viruses it received for surveillance to pharmaceutical companies, which would make patented vaccines from such samples—vaccines that were often too costly for developing countries to purchase.
Proposals to use IHR 2005 as a means to force Indonesia to share H5N1 virus samples for global surveillance purposes failed, because the IHR 2005 do not require such sharing or address inequitable access to the benefits derived
from such samples, Fidler observed. Instead, all 194 member countries passed a resolution at the World Health Assembly in 2007 to initiate a series of intergovernmental meetings to discuss, debate, and develop a new framework for the sharing of influenza viruses, a move that marginalized the IHR 2005 both legally and politically, Fidler asserted.
Influenza A (H1N1) The emergence of pandemic influenza subsequent to this workshop has highlighted the costs, as well as the benefits, of global information-sharing under the auspices of the IHR 2005. Mexico and the United States complied with their obligations to report outbreaks to the WHO, which declared a PHEIC within 48 hours of laboratory confirmation that the Mexican and U.S. viruses represented a new strain (Condon and Sinha, 2009).
However, despite WHO recommendations to the contrary, a significant number of countries imposed travel and trade restrictions as a result of the outbreak that produced severe economic repercussions, particularly in Mexico (Condon and Sinha, 2009; Editorial, 2009; Gostin, 2009). As Condon and Sinha (2009) observe, the “disproportionate response of several countries to Mexico’s response may well discourage other countries from acting so quickly, effectively and transparently in future disease outbreaks, to the detriment of all countries. The lack of any effective recourse under either the IHR (2005) or the WTO compounds the problem of disproportionate and asymmetrical travel and trade restrictions and creates disincentives to report outbreaks and deal with them in a transparent and decisive manner.”
Intent Versus Reality
The intent of the IHR 2005—to raise the importance of global health as a foreign policy issue and to transform global health governance—contrasts starkly with the reality of multiple barriers to its implementation, several workshop participants observed. They noted that the virus-sharing controversy highlighted several important inequities in public health capacity that exist between developed and developing countries that are not adequately addressed by the IHR 2005. Most daunting among these appears to be the previously mentioned “surveillance gap” that separates global surveillance needs and the resources available to support the development of capacity in resource-poor countries (Fidler and Gostin, 2007).
Divisions between developed and developing countries are further exacerbated by the lack of mechanisms to ensure global equity in response to infectious disease threats. After posing the rhetorical question as to whether a developed country’s national vaccine, antiviral, or antibiotic stockpile will be shared with developing countries in the event of a disease emergency, Fidler and Gostin (2007) observe that despite attempts by the WHO to create global stockpiles of such resources, intervention strategies are largely limited to—and by—national
governments. This situation contributes to the view that the IHR 2005 offer little to developing countries.
“A large proportion of policy makers in resource-constrained countries perceive that the emphasis of the IHR 2005 on the international spread of disease evinces little concern regarding the burden of infectious diseases on the nations in which they occur,” said speaker Oyewale Tomori, of Redeemer’s University in Nigeria (see Tomori in Chapter 4). He added that this perception “is fueled by a longstanding history of selective application and implementation of global health policies in order to support the interests of countries in the developed world,” such as disproportionate international reaction to outbreaks that occur in industrialized countries.
These perceptions can only add to the significant disincentives to reporting infectious disease outbreaks. As speaker David Bell, of the CDC, noted in his contribution to Chapter 5, “countries may perceive substantial economic disincentives to reporting and responding to public health threats as required by the IHR. Economic harm to tourism or export industries could result from public health measures such as travel advisories, quarantine, seizure of hazardous products, or culling of infected livestock—or simply from unjustified public fears. Mounting an emergency response will challenge the health budget of many developing countries, yet the IHR include no provision for financial support or compensation.”
Global Disease Surveillance and Response: Challenges and Opportunities
The IHR 2005, a landmark in the development of a global governance mechanism to respond to global health threats, demonstrate both the promise and the peril of global health governance and, more specifically, of global infectious disease surveillance. Fidler, who characterized surveillance as the “‘center of gravity’ for public health governance,” noted that efforts toward global governance are unlikely to succeed unless the benefits afforded by surveillance are equitably distributed. Workshop participants discussed a range of approaches to support global disease surveillance and response efforts both within and beyond the purview of the IHR 2005.
Addressing Present and Future Challenges to the IHR
In addition to the previously described roadblocks to implementing the IHR 2005—inequity in sharing its costs and benefits, lack of funding for surveillance in developing countries, overcoming sovereignty issues, competition with health and other global agendas—Fidler considered the following four out of five global trends, identified in a recent report from the National Intelligence Council (NIC, 2008a):
-
Overall risks to human life and health are expanding and accelerating,
-
Incentives for political disagreement are increasing,
-
Limitations on governance mechanisms are increasingly apparent, and
-
Vulnerabilities of societies to “pathogen politics”19 are deepening.
While these realities present significant challenges to the implementation and impact of IHR 2005, Fidler said, other international governance mechanisms have proven comparatively weak and ineffective in addressing the many and various drivers of infectious disease emergence and spread (e.g., migration, environmental and climate change, antimicrobial resistance, armed conflict). These failures reinforce the importance of the IHR 2005 to the future of global health, he concluded.
Greater recognition of the potential of the IHR 2005 to promote global security is key to their effective implementation, Heymann added. In the face of the current global recession, he offered two arguments to dissuade those who might favor reducing support for IHR 2005 implementation: its importance to public health security and therefore, to overall global security; and to preserve the foundation of health for economic development and redevelopment.
Bell’s presentation, entitled “Global Trade Security Depends on Implementation of the IHR,” echoed Heymann’s arguments, and explored how trade and tourism stakeholders (e.g., international corporations, industry and trade associations, ministries of trade and tourism) might support various aspects of the implementation of IHR 2005 (see Bell in Chapter 5). For example, Bell envisioned that an international scheme to compensate individuals or countries for economic hardships resulting from infectious disease outbreaks could be created as a public-private partnership involving trade and tourism stakeholders, and structured as a trust fund or insurance product.
“Business, trade, and tourism stakeholders, and those who support them, such as the insurance industry, have a strong vested interest in working with public health authorities to promote global health security,” according to Bell (2008). “The IHR also promote global trade security, which may be provisionally defined as maintenance of a stable trade environment by promotion of safe and unhindered travel and transport, stability of supply and distribution chains, continuity of business operations, and safety of imports and exports…. For businesses, industry associations, and international trade organizations and their member states, promoting IHR implementation is good risk management, since the risk of business and trade disruption is reduced in countries where the IHR are implemented.”
Speaking informally with business leaders, Bell found that most had never
heard of the IHR. However, he added, “they immediately understood its importance to them once the issues were explained. Their question was, what exactly do you want us to do, what might the next steps be?” although their interest was subsequently diverted by the global recession. Revision of the IHR was one of the highest global health priorities of the U.S. government, but it risks sitting on the shelf because support for its global implementation is lacking.
One World, One Health®20
Recognizing the importance of zoonoses as emerging diseases and the economic impact of animal diseases, several workshop participants advocated expanding the purview of surveillance under IHR 2005 by linking its human infectious disease networks with those focused on animal diseases. A similar argument was made to integrate infectious and foodborne disease surveillance by speaker David Nabarro of the United Nations (UN), among others. Nabarro, who serves as the UN’s coordinator for avian and human influenza, as well as for global food security, applauded the advent of such an integrated strategy, known as One World, One Health®, which he characterized as seeking “new ways of aligning action to better address diseases that emerge at the interface between animals and humans in different ecosystems” (Schnirring, 2008).
Speaker Ottorino Cosivi of the WHO described the development of the One World, One Health® strategic framework, which evolved from lessons learned in efforts to address the threat of pandemic avian influenza. Partners in this framework currently include the WHO, the Food and Agriculture Organization of the UN (FAO), the World Organisation for Animal Health (OIE), the UN Children’s Fund (UNICEF), and the World Bank. The concept of One World, One Health® is embodied in projects such as the Global Early Warning and Response System for Major Animal Diseases, Including Zoonoses (GLEWS), which is jointly operated by the FAO, OIE, and the WHO (WHO, 2009a).
Role of the OIE Further alignment of human and animal disease surveillance efforts appears promising based on comparisons between surveillance as
|
20 |
One World, One Health® is a registered trademark of the Wildlife Conservation Society. Health experts from around the world met on September 29, 2004, for a symposium focused on the current and potential movements of diseases among human, domestic animal, and wildlife populations organized by the Wildlife Conservation Society and hosted by The Rockefeller University. Using case studies on Ebola, avian influenza, and chronic wasting disease as examples, the assembled expert panelists delineated priorities for an international, interdisciplinary approach for combating threats to the health of life on Earth. The product—called the “Manhattan Principles” by the organizers of the “One World, One Health®” event—lists 12 recommendations for establishing a more holistic approach to preventing epidemic/epizootic disease and for maintaining ecosystem integrity for the benefit of humans, their domesticated animals, and the foundational biodiversity that supports us all. For more information, see http://www.oneworldonehealth.org/ (accessed July 16, 2009). |
conducted under the IHR 2005, and through the OIE’s World Animal Health Information System (WAHIS), by speaker Alejandro Thiermann of the OIE (see Chapter 5). He described that organization’s efforts to address animal disease to ensure animal health worldwide, food safety and safeguard global trade, which parallel those of the WHO. Member countries are bound to report cases that meet any of the following criteria to the WAHIS: diseases with potential for international spread, apparent emerging diseases, diseases with zoonotic potential, and diseases that show significant spread in naïve populations. OIE reviews and immediately publishes such reports on its World Animal Health Information Database (WAHID), accessible by all member countries. When appropriate, OIE also issues early warnings on a webpage.
Unlike IHR 2005, WAHIS can only publish official information, submitted by its delegates (the chief veterinary officers of its member countries), Thiermann explained. Nevertheless, he added, through collaborations with other surveillance networks, including those operated by the WHO, the OIE searches non-official sources of information for indications of “notifiable” disease events. When evidence of such an event is detected, the information is submitted to that country’s delegate for immediate confirmation or denial. In some cases, the OIE has posted alerts based on such information in the absence of official confirmation, Thiermann said. For example, when Chinese officials did not confirm unofficial reports indicating the presence of avian influenza in ducks in southern China, the OIE nevertheless proceeded to notify its members. Official confirmation was forthcoming from China, but not until 24 hours after this information was posted.
Thiermann noted that when a disease event occurs at the interface of animal and human health, ministries of health and agriculture within the same country often respond differently; in such cases, only the WHO, or only the OIE, may be notified. These situations are best managed through “a close collaboration” that enables the exchange of information between the two organizations, and a joint response to zoonotic threats, he said. Organizations with surveillance and response functions for zoonotic diseases—particularly OIE, FAO, and WHO—need to continually share and collaborate, he concluded.
Role of the WHO A variety of interagency collaborations promote the early detection and control of disease at the animal-human interface, according to Cosivi (see Chapter 5). He described a series of such formal agreements and joint programs involving the WHO, and frequently, the OIE and the FAO as well, dating back to 1948. In addition to the previously described GLEWS and GOARN, these include the following:
-
The International Food Safety Authorities Network (INFOSAN), which disseminates information and fosters international collaboration on food safety (WHO, 2007);
-
Global Salm-Surv, which promotes integrated laboratory- and epidemiology-based foodborne disease surveillance (WHO, 2009c); and
-
The Mediterranean Zoonoses Control Program, which supports the prevention, surveillance, and control of zoonoses and foodborne diseases and serves as a platform for interagency collaboration for country-level capacity building to address these diseases (WHO, 2009b).
Cosivi described the development of the “One World, One Health®” strategy as a paradigm shift in public health, from the “response and rehabilitation mode” characterized by initial attempts to address avian influenza, to prevention and preparedness for all emerging infectious diseases. “To prevent human diseases,” he concluded, “we need to increase attention to prevention, surveillance, and control in wild and domestic animal health, animal production and food systems, and the environment.”
Building Capacity and Trust
In order to build on the foundation provided by the IHR 2005 and the “One World, One Health®” strategic framework, according to Nabarro the following three challenges must be resolved (see Chapter 5):
-
Implementing adequate systems and capacities to conduct global surveillance and respond to global public health emergencies (e.g., animal surveillance for H5N1 influenza);
-
The need to engage all stakeholders, and particularly the private sector, in global disease surveillance and response, recognizing that some key groups do not perceive such action to be in their best interest; and
-
Most importantly, to create the most important incentive for participation in global health initiatives: trust.
Building capacity In addition to previously described workshop discussions that addressed Nabarro’s first point, regarding the need for capacity-building (and for funding to support it), Tomori advocated equal emphasis on the national and international spread of diseases. “The practice of ‘dangling the carrot’ of international resources for responding to a disease outbreak (e.g., vaccines, funding, and foreign expertise) as an incentive for reporting such an outbreak may undermine the determination of resource-constrained countries to develop, strengthen, and maintain national core surveillance and response capabilities,” he contended (see Tomori in Chapter 4). “Moreover, it is far more efficient to contain disease outbreaks than to respond to full-blown epidemics.” Making a similar argument from a global perspective, Forum member Terence Taylor, of the International Council for the Life Sciences, observed that in an age of mobile populations such as those described by Gushulak (see Chapter 1), border
biosecurity “is less important than building … national core infectious disease surveillance capacity.”
Tomori stated that countries should be encouraged to develop the capacities to report, detect, and investigate suspected disease outbreaks and thus prevent sporadic cases from escalating to epidemics, and that more resources be provided for establishing and maintaining disease surveillance systems at the national level. He described the establishment of the acute flaccid paralysis (AFP) surveillance system, backed by an African region-wide laboratory network, as a model for such national surveillance systems.
The only way to make progress on global health governance is to empower countries to develop their own surveillance capacities, Nabarro said. Developing countries must be encouraged to work with other countries in their subregions to develop networking and common approaches across nearby borders, but such efforts have to originate within countries, he insisted.
Engaging all stakeholders Nabarro, whose remarks focused on the issue of conducting effective global disease surveillance and response in an atmosphere of increasing suspicion toward the value of globalized initiatives, recalled that, for a time, the threat of pandemic avian influenza generated “unity of purpose and synergy of action.” Although occasional discord arose, coordination between donors, foundations, national governments, regional bodies, and international nongovernmental groups was strong.
“What was the incentive that brought so many disparate groups to work together as if in a strong magnetic field, and not to lose their separateness? Answer: It certainly wasn’t cash,” Nabarro said, because although money was available, it moved slowly, and little of it made it to those organizations that were working in concert. Instead, he observed, these groups were motivated to join a global movement. “They found it both attractive and at the same time comforting … to be coherent, to be together, to be joint stakeholders within a movement,” he concluded, adding that the same force has motivated recent collaborations to address HIV/AIDS, and to eradicate polio (as described by Heymann; see Chapter 1). “I believe that the best incentive for working together on surveillance, on reporting, on response, is the creation of a movement that is open enough, strong enough, inclusive enough, to enable hundreds of different stakeholders to feel at home inside it,” he concluded.
Two Forum members—Gail Cassell, of Eli Lilly, and Phil Hosbach, of Sanofi Pasteur—urged that such collaborations include another stakeholder in global disease control not mentioned specifically by Nabarro: the pharmaceutical industry. For example, Hosbach said, pharmaceutical companies represent the solution to one of the critical challenges to influenza surveillance. “The benefits-sharing that these countries are looking for is … [protection] from influenza, and what better way to do that than with vaccine?” he asked. Heymann agreed that industry had served as “a faithful partner in the influenza pandemic and vaccine
production,” but he maintained that pharmaceutical companies have not “brought to the table any solutions to make vaccines available.” Resolving this impasse would require dialogue between global public health and industry groups, focused on solving this critical problem, he observed.
Building trust “You can’t get results on control of H5N1 or other diseases through compulsion,” Nabarro continued. “If you compel, then people start to hide, they fail to explain, they don’t involve themselves. So it is absolutely essential to build the necessary trust so that the work can progress.” Moreover, he said, mistrust among stakeholders in a common enterprise, such as global disease surveillance and response, must be anticipated, insured against, and addressed as soon as it arises.
The United States has been the strongest and most consistent leader in promoting global collaborations to address H5N1 influenza over the past three years, Nabarro said. While he encouraged the United States to continue this leadership, despite the risks involved, he also encouraged inclusiveness. Likening the role of the United States as the builder of a tent to be occupied by a host of stakeholders in global health, he advised the country to “make the tent so it is big enough, but also so that it is open enough … [and] exciting enough to bring people in.”
Toward Resilience
Workshop participants were compelled to discuss the unfolding worldwide economic crisis and its possible repercussions for global public health. Nabarro suggested that any among a range of potential shocks—including pandemic disease, climate change, food crisis, and recession—would have similar effects on a given community or individual household, depending upon its overall resilience. “The stronger, most resilient households will survive,” he said, and “in many cases … resilience can be surprising.” Less resilient households, particularly those that have recently moved from a subsistence into the market economy, will not be so fortunate, he continued, and are likely to decline into subsistence; this will be especially likely for women-headed households and those in which a breadwinner becomes ill or disabled.
Therefore, in the context of global recession, and in order to prepare people, communities, and countries to withstand any of the various threats looming on the horizon, Nabarro advocated the promotion of resilience. He noted that the World Bank has taken a leadership role in this effort, but this effort will require a multifaceted approach that includes public health. He also advocated continued support, led by the United States, for development assistance “geared toward efficient action, leverage, and [the] empowerment of local communities to do more for themselves.”
Reflecting on workshop presentations and discussions that encompassed history, public health policy, ecology, and medical science, Relman considered the
relationship between diversity and resilience. “Is there an aspect of diversity that predicts resistance to perturbation?” he asked. “One might look for this feature in patterns of diversity amongst susceptible host species or in diversity amongst local response mechanisms, or both, to mention a few possibilities.”
“It sounds to me as though many people are suggesting that there is no one global fix for the kinds of problems we are talking about,” Relman continued. Rather, he concluded, we are presented with a set of possible local solutions, based on common principles, which can be adapted and strengthened to support specific ecosystems, communities, and public health capacities.
OVERVIEW REFERENCES
Anderson, P. K., A. A. Cunningham, N. G. Patel, F. J. Morales, P. R. Epstein, and P. Daszak. 2004. Emerging infectious diseases of plants: pathogen pollution, climate change and agrotechnology drivers. Trends in Ecology and Evolution 19(10):535-544.
Angelini, R., A. C. Finarelli, P. Angelini, C. Po, K. Petropulacos, G. Silvi, P. Macini, C. Fortuna, G. Venturi, F. Magurano, C. Fiorentini, A. Marchi, E. Benedetti, P. Bucci, S. Boros, R. Romi, G. Majori, M. G. Ciufolini, L. Nicoletti, G. Rezza, and A. Cassone. 2007. Chikungunya in northeastern Italy: a summing up of the outbreak. Eurosurveillance 12(11):E071122.2.
Bell, D. M. 2008. Of milk, health and trade security. Far Eastern Economic Review 178(8):34-37.
Bertozzi, S., A. Kelso, M. Tashiro, V. Savy, J. Farrar, M. Osterholm, S. Jameel, and C. P. Muller. 2009. Pandemic flu: from the front lines. Nature 461(7260):20-21.
Carlton, J. 2004. Invasions in the world’s oceans: how much do we know, and what does the future hold? Presentation given at the American Institute of Biological Sciences annual meeting, March.
CDC (Centers for Disease Control and Prevention). 1990. Update: Ebola-related Filovirus infection in nonhuman primates and interim guidelines for handling nonhuman primates during transit and quarantine. Morbidity and Mortality Weekly Report 39(2):22-24, 29-30.
———. 2003. Multistate outbreak of monkeypox—Illinois, Indiana, and Wisconsin, 2003. Morbidity and Mortality Weekly Report 52(23):537-540.
———. 2008a. Chikungunya distribution and global map, http://www.cdc.gov/ncidod/dvbid/Chikungunya/CH_GlobalMap.html (accessed July 17, 2009).
———. 2008b. Questions and answers about monkeypox, http://www.cdc.gov/ncidod/monkeypox/qa.htm (accessed October 21, 2009).
Coghlan, B., V. N. Bemo, P. Ngoy, T. Stewart, F. Mulmba, J. Lewis, C. Hardy, and R. Brennan. 2007. Mortality in the Democratic Republic of Congo: an ongoing crisis. New York and Australia: International Rescue Committee and Burnet Institute.
Condon, B. J., and T. Sinha. 2009. Chronicle of a pandemic foretold: lessons from the 2009 influenza epidemic, http://papers.ssrn.com/sol3/papers.cfm?abstract_id=1398445 (accessed July 16, 2009).
Crosby, M. C. 2006. The American plague: the untold story of yellow fever, the epidemic that shaped our history. New York: Berkley.
Daszak, P., A. A. Cunningham, and A. D. Hyatt. 2000. Emerging infectious diseases of wildlife—threats to biodiversity and human health. Science 287(5452):443-449.
Dawood, F. S., S. Jain, L. Finelli, M. W. Shaw, S. Lindstrom, R. J. Garten, L. V. Gubareva, X. Xu, C. B. Bridges, and T. M. Uyeki. 2009. Emergence of a novel swine-origin influenza A (H1N1) virus in humans. New England Journal of Medicine 360(25):2605-2615.
Deloitte Center for Health Solutions. 2008. Medical tourism: consumers in search of value. Washington, DC: Deloitte LLP.
Dybas, C. L. 2004. Invasive species: the search for solutions. BioScience 54(7):615-621.
Editorial. 2009 (May 9). Of pigs, planes and protectionism. New York Times.
Fairchild, A. L. 2003. Science at the borders: immigrant medical inspection and the shaping of the modern industrial labor force. Baltimore, MD: The Johns Hopkins University Press.
FDA (Food and Drug Administration). 2009. Xenotransplantation, http://www.fda.gov/BiologicsBloodVaccines/Xenotransplantation/default.htm# (accessed October 21, 2009).
Fidler, D. P., and L. O. Gostin. 2006. The new International Health Regulations: an historic development for international law and public health. The Journal of Law, Medicine, and Ethics 34(1):85-94, 4.
———. 2007. Biosecurity in the global age: biological weapons, public health, and the rule of law. Stanford, CA: Stanford University Press.
Fidler, D. P., L. O. Gostin, and H. Markel. 2007. Through the quarantine looking glass: drug-resistant tuberculosis and public health governance, law, and ethics. The Journal of Law, Medicine, and Ethics 35(4):616-628, 512.
Fraser, C., S. Riley, R. M. Anderson, and N. M. Ferguson. 2004. Factors that make an infectious disease outbreak controllable. Proceedings of the National Academy of Sciences 101(16):6146-6151.
Gostin, L. O. 2009. Influenza A (H1N1) and pandemic preparedness under the rule of international law. Journal of the American Medical Association 301(22):2376-2378.
Graham, J. P., J. H. Leibler, L. B. Price, J. M. Otte, D. U. Pfeiffer, T. Tiensin, and E. K. Silbergeld. 2008. The animal-human interface and infectious disease in industrial food animal production: rethinking biosecurity and biocontainment. Public Health Reports 123(3):282-299.
Gushulak, B. D., and D. W. MacPherson. 2000. Population mobility and infectious diseases: the diminishing impact of classical infectious diseases and new approaches for the 21st century. Clinical Infectious Diseases 31(3):776-780.
Hufnagel, L., D. Brockmann, and T. Geisel. 2004. Forecast and control of epidemics in a globalized world. Proceedings of the National Academy of Sciences 101(42):15124-15129.
IOM (Institute of Medicine). 1992. Emerging infections: microbial threats to health in the United States. Washington, DC: National Academy Press.
———. 2003. Microbial threats to health: emergence, detection, and response. Washington, DC: The National Academies Press.
———. 2004. Learning from SARS. Washington, DC: The National Academies Press.
———. 2005. The threat of pandemic influenza: are we ready? Washington, DC: The National Academies Press.
———. 2006. Addressing foodborne threats to health: policies, practices, and global coordination. Washington DC: The National Academies Press.
———. 2007. Ethical and legal considerations in mitigating pandemic disease. Washington, DC: The National Academies Press.
———. 2008a. Vector-borne diseases: understanding the environment, human health, and ecological connections. Washington, DC: The National Academies Press.
———. 2008b. Global climate change and extreme weather events: understanding the contribution to infectious disease emergence. Washington, DC: The National Academies Press.
Jones, K. E., N. G. Patel, M. A. Levy, A. Storeygard, D. Balk, J. L. Gittleman, and P. Daszak. 2008. Global trends in emerging infectious diseases. Nature 451(7181):990-993.
Khan, K., J. Arino, W. Hu, P. Raposo, J. Sears, F. Calderon, C. Heidebrecht, M. Macdonald, J. Liauw, A. Chan, and M. Gardam. 2009. Spread of a novel influenza A (H1N1) virus via global airline transportation. New England Journal of Medicine 361(2):212-214.
Kimball, A. M. 2006. Risky trade: infectious disease in the era of global trade. Surrey, UK: Ashgate. P. 59.
Kraut, A. M. 1995. Silent travelers: germs, genes, and the immigrant menace. Baltimore, MD: The Johns Hopkins University Press.
Markel, H. 1997. Quarantine! Baltimore, MD: The Johns Hopkins University Press.
———. 2004. When germs travel: six major epidemics that have invaded America and the fears they have unleashed. New York: Vintage.
Markel, H., D. Fidler, and L. O. Gostin. 2007. Extensively drug-resistant tuberculosis: an isolation order, public health powers, and a global crisis. Journal of the American Medical Association 298(1):83-86.
Martens, P., and L. Hall. 2000. Malaria on the move: human population movement and malarial transmission. Emerging Infectious Diseases 6(2):103-109.
Morens, D. M., G. K. Folkers, and A. S. Fauci. 2008. Emerging infections: a perpetual challenge. Lancet Infectious Diseases 8(11):710-719.
NIC (National Intelligence Council). 2008a. Global trends 2025: a transformed world. Washington, DC: U.S. Government Printing Office.
———. 2008b. Strategic implications of global health. Washington, DC: U.S. Government Printing Office.
Osburn, B. I. 2008. Vector-borne zoonotic diseases and their ecological and economic implications: bluetongue disease in Europe. In IOM, Vector-borne diseases: understanding the environmental, human health, and ecological connections. Washington, DC: The National Academies Press.
PCAST (President’s Council of Advisors on Science and Technology). 2009. Report to the President on U.S. Preparations for 2009-H1N1 influenza. Washington, DC: Office of Science and Technology Policy.
Powers, A. M., and C. H. Logue. 2007. Changing patterns of chikungunya virus: re-emergence of a zoonotic arbovirus. Journal of General Virology 88(pt. 9):2363-2377.
Quammen, D. 2007 (October). Deadly contact: how animals and humans exchange disease. National Geographic:78-105.
Reiskind, M. H., K. Pesko, C. J. Westbrook, and C. N. Mores. 2008. Susceptibility of Florida mosquitoes to infection with chikungunya virus. American Journal of Tropical Medicine and Hygiene 78(3):422-425.
Rezza, G., L. Nicoletti, R. Angelini, R. Romi, A. C. Finarelli, M. Panning, P. Cordioli, C. Fortuna, S. Boros, F. Magurano, G. Silvi, P. Angelini, M. Dottori, M. G. Ciufolini, G. C. Majori, and A. Cassone. 2007. Infection with chikungunya virus in Italy: an outbreak in a temperate region. Lancet 370(9602):1840-1846.
Schnirring, L. 2008. FAO: Momentum builds for “One World, One Health” concept. Center for Infectious Disease Research and Policy, November 26, http://www.cidrap.umn.edu/cidrap/content/influenza/panflu/news/nov2608fao-jw.html (accessed April 4, 2009).
Scobie, L., and Y. Takeuchi. 2009. Porcine endogenous retrovirus and other viruses in xenotransplantation. Current Opinion in Organ Transplantation 14(2):175-179.
Seabloom, E. W., J. W. Williams, D. Slayback, D. M. Stoms, J. H. Viers, and A. P. Dobson. 2006. Human impacts, plant invasion, and imperiled plant species in California. Ecological Applications 16(4):1338-1350.
Smith, K. F., M. Behrens, L. M. Schloegel, N. Marano, S. Burgiel, and P. Daszak. 2009. Ecology: reducing the risks of the wildlife trade. Science 324(5927):594-595.
Stern, A. M., and H. Markel. 2004. International efforts to control infectious diseases, 1851 to the present. Journal of the American Medical Association 292(12):1474-1479.
Thanos, C. G., and R. B. Elliott. 2009. Encapsulated porcine islet transplantation: an evolving therapy for the treatment of type I diabetes. Expert Opinion on Biological Therapy 9(1):29-44.
Torchin, M. E., and C. E. Mitchell. 2004. Parasites, pathogens, and invasions by plants and animals. Frontiers in Ecology and the Environment 2(4):183-190.
Torchin, M. E., K. D. Lafferty, A. P. Dobson, V. J. McKenzie, and A. M. Kuris. 2003. Introduced species and their missing parasites. Nature 421(6923):628-630.
Tsetsarkin, K. A., D. L. Vanlandingham, C. E. McGee, and S. Higgs. 2007. A single mutation in chikungunya virus affects vector specificity and epidemic potential. PLoS Pathogens 3(12):e201.
Tutton, M. 2009. Medical tourism: have illness, will travel, http://www.cnn.com/2009/HEALTH/03/26/medical.tourism/ (accessed October 14, 2009).
UNWTO (United Nations World Tourism Organization). 2008. UNWTO World Tourism Barometer 6(1), http://www.world-tourism.org/facts/menu.html (accessed February 8, 2008).
U.S. Congress, House. 2008. The Nonnative Wildlife Invasion Prevention Act. H. R. 6311 (introduced). 100th Congress, 2nd session.
USDA (U.S. Department of Agriculture). 2009. Intensive farming, http://agclass.nal.usda.gov/agt/mtwdk.exe?s=1&n=1&y=0&l=60&k=glossary&t=2&w=intensive+farming (accessed October 21, 2009).
Van Herp, M., V. Parque, E. Rackley, and N. Ford. 2003. Mortality, violence and lack of access to health-care in the Democratic Republic of Congo. Disasters 27(2):141-153.
Vazeille, M., S. Moutailler, D. Coudrier, C. Rousseaux, H. Khun, M. Huerre, J. Thiria, J. S. Dehecq, D. Fontenille, I. Schuffenecker, P. Despres, and A. B. Failloux. 2007. Two chikungunya isolates from the outbreak of La Réunion (Indian Ocean) exhibit different patterns of infection in the mosquito, Aedes albopictus. PLoS One 2(11):e1168.
Wang, C. 2006. A study of geographical characterization of ship traffic and emissions and a cost-effectiveness analysis of reducing sulfur emissions from foreign waterborne commerce for the U.S. west coast. Newark, DE: University of Delaware.
Wang, C., J. J. Corbett, and J. Firestone. 2007. Modeling energy use and emissions from North American shipping: application of the ship traffic, energy, and environment model. Environmental Science and Technology 41(9):3226-3232.
WCS (Wildlife Conservation Society). 2009. What is bushmeat? http://www.wcs-congo.org/01ecosystemthreats/02bushmeat/104whatisbushmeat.html (accessed October 21, 2009).
WHA (World Health Assembly). 2004. Human organ and tissue transplantation. Geneva: World Health Organization.
WHO (World Health Organization). 2005. Frequently asked questions about the International Health Regulations (2005), http://www.who.int/csr/ihr/howtheywork/faq/en/index.html (accessed November 26, 2008).
———. 2007. International Food Safety Authorities Network (INFOSAN), http://www.who.int/foodsafety/fs_management/infosan_1007_en.pdf (accessed April 10, 2009).
———. 2008. International Health Regulations, http://www.who.int/csr/ihr/en/ (accessed January 28, 2009).
———. 2009a. Global Early Warning System for Major Animal Diseases, Including Zoonoses (GLEWS), http://www.who.int/zoonoses/outbreaks/glews/en/ (accessed April 5, 2009).
———. 2009b. Mediterranean Zoonoses Control Programme (MZCP) of the World Health Organization, http://www.who.int/zoonoses/institutions/mzcp/en/ (accessed April 5, 2009).
———. 2009c. WHO Global Salm-Surv, http://www.who.int/salmsurv/en/ (accessed April 5, 2009).
Wilson, M. E. 2003. The traveler and emerging infections: sentinel, courier, transmitter. Journal of Applied Microbiology 94(Supp):1S-11S.








































