
1
Introduction
Reducing Americans’ intake of sodium has been an important but elusive public health goal for many years. The U.S. population consumes far more sodium than is recommended, placing individuals at risk for diseases related to elevated blood pressure. Since 1969, initiatives to reduce sodium intake have driven an array of public health interventions and national dietary guidance recommendations. To date, these activities have failed to meet their goal. Americans’ intake of sodium remains at best unchanged and has even trended upward since the early 1970s. Meanwhile, the incidence of hypertension has not decreased.
The major federal nutrition policy guidance, Dietary Guidelines for Americans, specified quantitative limits for dietary sodium intake for the first time in 2005. It recommends consuming < 2,300 mg/d of sodium for the general population 2 or more years of age. The Dietary Guidelines for Americans further identifies at-risk subgroups within the general population—persons with hypertension, African Americans, and middle-aged and older adults—and recommends a sodium intake of no more than 1,500 mg/d for these individuals. New analysis of National Health and Nutrition Examination Survey (NHANES) data shows that this lower recommendation would apply to 69 percent of U.S. adults (CDC, 2009). The Dietary Guidelines for Americans also indicates that measures of salt use at the table and during cooking have remained fairly stable and relatively small compared to other sources of sodium, suggesting that programs for decreasing the salt intake of a population may be most successful if they are designed to concentrate on reducing salt added during food processing and on changes in food selection.
The Dietary Guidelines for Americans quantitative recommendation of < 2,300 mg/d is consistent with the Institute of Medicine’s (IOM’s) Tolerable Upper Intake Level for sodium for adults as established by the report Dietary Reference Intakes for Water, Potassium, Sodium, Chloride, and Sulfate (IOM, 2005). Further, the IOM report identifies the need for public health strategies to reduce sodium intake as well as the development of alternative processing technologies to reduce the sodium content of foods. The report suggests that special attention be given to maintaining flavor, texture, consumer acceptability, and low cost.
The Consolidated Appropriations Act of 20081 targeted to the Departments of Labor, Health and Human Services, and Education and related agencies directs the Centers for Disease Control and Prevention (CDC) to undertake a study through the IOM of the National Academies “to examine and make recommendations regarding various means that could be employed to reduce dietary sodium intake to levels recommended by the Dietary Guidelines for Americans.” CDC was joined by several other federal agencies in supporting this study, including the Food and Drug Administration; the National Heart, Lung, and Blood Institute; and the Office of Disease Prevention and Health Promotion.
THE TASK
The statement of task for the committee charged with carrying out this study is found in Box 1-1.
As part of its general task, the committee was requested to address
-
dietary intake of sodium and the primary sources of sodium for the U.S. population overall;
-
understandings about the physiology of taste and sensitivity, and their interface with consumer behavior and taste preferences;
-
functions of sodium in foods and how these functions relate to product development, consumer preferences, and health;
-
factors that could affect sodium reduction strategies;
-
potential of food technology to develop innovative alternatives to current sodium use in processed foods, taking into account the physiology of taste as well as consumer behaviors and preferences;
-
potential unanticipated consequences;
-
sodium reduction efforts in other countries;
-
policy levers such as regulation (including labeling), investment of public monies, education, incentives, support for local capac-
|
BOX 1-1 Statement of Task The committee will review and make recommendations about various means that could be employed to reduce dietary sodium intake to levels recommended by the Dietary Guidelines for Americans. The committee will consider a variety of options. These may include, but are not limited to, government approaches (regulatory and legislative actions), food supply approaches (new product development, food reformulation), and information/education strategies for the public and professionals. Attention will be given to opportunities for government and industry collaboration, along with input from health professionals, for the purposes of fostering innovation in this area. The committee will prepare a consensus report that (1) describes the state of actions to reduce sodium intake and factors to consider in sodium reduction strategies as learned from the committee’s review and considerations and (2) recommends actions (with rationale) for public and private stakeholders in order to achieve sodium intake consistent with the Dietary Guidelines for Americans. The report will recommend options for long-term monitoring and identify research needs. |
-
ity, health professional role, industry codes of conduct, research, monitoring progress (accountability), and leadership; and
-
options for public-private partnerships in the context of fostering creative and innovative approaches and programs ranging from basic and consumer research to planning for and implementing sodium reduction in diverse populations.
It should be noted that the tasks assigned to this committee did not include reviewing the scientific evidence on the relationship between sodium intake and health or reevaluating dietary guidance on the levels of sodium that should be consumed. Instead, the committee relied upon conclusions from authoritative bodies to support the health benefits related to sodium reduction.
THE APPROACH
Scientific Rationale for Strategy-Setting Decisions
Consideration of the scientific basis for establishing the relationship between high sodium intake and elevated blood pressure is not within this committee’s task and was not specifically reviewed or addressed. The charge to the committee is to make recommendations about means to reduce dietary sodium intake to levels recommended by the Dietary Guidelines
for Americans. The charge reflects the conclusions of the widespread and numerous public health initiatives that began in the early 1970s and have continued through the present time, as discussed in Chapter 2. Overall, these initiatives, many of which relied on expert advisory committees for scientific expertise, concluded that there is strong scientific support for a direct and progressive relationship between sodium intake and blood pressure. They also voiced long-standing concerns about unacceptably high incidence of hypertension among U.S. adults and the associated increased risk for cardiovascular disease (e.g., stroke and coronary heart disease) and the persistence of high intake of sodium among the general U.S. population. All recommended reduced sodium intake as a public health strategy.
Although a primary scientific review to document the relationship between sodium intake and disease risk was not within the committee’s mandate, the study required an understanding of the science relative to two key questions if the committee’s strategy decisions were to be adequately informed. The first question relates to the seriousness and nature of the public health problem. The nature of the recommended strategies should be commensurate with the seriousness and extent of that problem. The second question relates to the nature of the target population—specifically, whether the strategies should focus on the general population or be limited to specified subpopulations.
To understand the nature of the scientific consensus among qualified experts on these two questions, it was deemed useful to review the scientific conclusions from the most current major authoritative consensus bodies, including the 2005 Dietary Guidelines Advisory Committee (DGAC, 2005), the IOM (2005), and the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (NHLBI, 2004), and to update these reports, where applicable and necessary, with other relevant evidence.
Seriousness of the Public Health Problem
The prevalence of hypertension is common and increasing among American adults. It is a condition associated with several factors including obesity, genetics, and food- and physical activity-related behaviors, some of which may be related to culture/ethnicity. While the definition of hypertension has changed over time, rates of hypertension have remained high. The age-standardized prevalence rate of hypertension was 24 percent in NHANES III (1988–1994) (Cutler et al., 2008) and increased to 28–30 percent during the continuous NHANES from 1999 to 2006 (Ostchega et al., 2008). More than half of persons 60–69 years of age, and approximately three-fourths of those 70 years and older, have hypertension (NHLBI, 2004). The number of adults with hypertension in 1988–1994 was approxi-
mately 50 million and is estimated to be 65 million in 1999–2000 (Cutler et al., 2008). Blood pressure levels among children and adolescents also increased between 1988 and 2000 (Muntner et al., 2004).
Although increases in the prevalence of hypertension in both adults and children were partially explained by increases in body mass index (BMI)—an indirect measure of body fat—over the corresponding periods of comparison, adjusting for increasing BMI levels cannot completely explain the increasing prevalences (Cutler et al., 2008; Muntner et al., 2004). This suggests that, separate from the issue of obesity, the overconsumption of calories (and the concomitant overconsumption of sodium) is problematic. Moreover, while the measurement of short-term absolute risk for hypertension is determined by incidence rates, the long-term risk for hypertension can be reported by using the lifetime risk statistic, defined as the probability of developing hypertension during the remaining years of life (NHLBI, 2004). The lifetime risk of hypertension is approximately 86–90 percent for women and 81–83 percent for men after adjusting for competing mortality (Vasan et al., 2002).
In assessing the nature of the public health problem associated with elevated blood pressure levels, it is also important to consider its major consequences—heart disease, stroke, and kidney disease. Heart disease is the largest cause of death in the United States (26 percent of deaths in 2006), and stroke is the third-largest underlying cause of death (5.7 percent of deaths in 2006) (Xu et al., 2009). Furthermore, available data from cross-sectional studies in hypertensive individuals have consistently documented a progressive, direct relationship between sodium intake and left ventricular mass (a powerful predictor of stroke and other forms of cardiovascular disease). Sodium may have a direct effect apart from an indirect effect mediated through blood pressure (IOM, 2005). While one controlled trial (Jula and Karanko, 1994) suggests that the association between sodium intake and left ventricular mass is causal, additional trials are needed (IOM, 2005).
Given the direct causal relationship between sodium intake, blood pressure, and associated cardiovascular disease risk, several analyses of cost effectiveness have assessed the health effects and costs of population-wide reductions in salt intake of the U.S. population. Danaei et al. (2009) concluded that smoking and high blood pressure are the risk factors responsible for the greatest number of deaths in the United States, with high blood pressure responsible for 395,000 deaths annually. They estimated that population-wide reductions in sodium intake could prevent more than 100,000 deaths annually (Danaei et al., 2009). High dietary sodium intake, compared to the other dietary risk factors examined (i.e., low omega-3 fatty acids, high trans fatty acids, alcohol use, low intake of fruits and vegetables, low polyunsaturated fatty acids as an indicator of high saturated
fat intake), was associated with more attributable deaths than any of the other single dietary factors.
The potential societal and medical savings of reducing hypertension and related cardiovascular disease by way of a reduction in population-level sodium intake have been demonstrated in recent analyses (Bibbons-Domingo et al., 2010; Palar and Sturm, 2009; Smith-Spangler et al., 2010). Reducing the average population sodium intake to 2,300 mg/d from current intake levels was estimated to reduce cases of hypertension by 11 million, to save $18 billion in health-care dollars, and to gain 312,000 quality-adjusted life-years that are worth $32 billion annually (Palar and Sturm, 2009). Bibbons-Domingo et al. (2010) developed a projection model that showed a benefit for all population groups from a reduction of salt intake by 3 g (equal to 1,200 mg sodium) per day. This decrease was projected to reduce the number of new cases of coronary heart disease by 60,000, stroke by 32,000, and myocardial infarction by 54,000 per year. Smith-Spangler et al. (2010) estimated that decreasing mean population sodium intake by 9.5 percent would prevent 513,885 strokes and 480,358 myocardial infarctions over the lifetime of adults currently aged 40–85 years, saving $32.1 billion in medical costs.
In summary, the nature of the public health problem associated with excessive sodium intake is serious, directly affects large numbers of people, and is associated with high health-care and quality-of-life costs. Therefore, strong solutions are warranted if it is to be addressed effectively. Because sodium intake is causally related to high blood pressure, an established risk factor for cardiovascular disease, reductions in sodium intake have been seen as an essential component of national public health policy for the past several decades (Loria et al., 2001; USDA/HHS, 2005). Newer data document that this requires continued priority and attention; furthermore, the IOM committee on Public Health Priorities to Reduce and Control Hypertension in the U.S. Population found the evidence base to reduce dietary sodium as a means to shift the population distribution of blood pressure levels convincing (IOM, 2010).
Target Population for Sodium Intake Reduction
Initially, reduction of sodium intake focused on persons considered to be at high risk, such as those with hypertension and older adults. For this report, the committee considered the general population when making recommendations because as new science has emerged, the focus of public health policy has expanded to include the general population as well as high-risk subgroups (Loria et al., 2001). In addition, the lifetime risk of becoming hypertensive for adults is greater than 80 percent (after adjusting for competing causes of mortality) (Vasan et al., 2002), but currently there
is no method for determining which individuals fall within the 20 percent of the population that will not become hypertensive. Furthermore, because excess sodium intake can gradually increase blood pressure throughout life, before individuals develop clinically defined hypertension, and taste preferences for salty foods may be established early in life, long before individuals are aware of their risk for hypertension, a focus on at-risk subgroups could potentially fail to reach individuals who would benefit from a reduced sodium intake.
Although the extension of recommendations from high-risk groups to the general population has engendered controversy (Alderman, 2010; Cohen et al., 2006; Loria et al., 2001; McCarron, 2000, 2008; McCarron et al., 2009), numerous expert advisory panels (see Appendix B), including the most recent Dietary Guidelines Advisory Committee (DGAC, 2005), have consistently and repeatedly concluded, after careful evaluation of stakeholder concerns and the available scientific evidence, that the evidence and public health concerns warrant extending recommendations for sodium intake reduction to members of the general population across the lifespan. Recent data, including results of a clinical trial that documented the long-term benefits of sodium reduction in terms of cardiovascular events (Cook et al., 2007), have only strengthened the scientific rationale for population-wide sodium reduction (Bibbons-Domingo et al., 2010).
While the clinical problem of hypertension most commonly affects middle-aged and older adults in developed countries such as the United States, the genesis of elevated blood pressure is a lifelong process in which blood pressure rises gradually with age. There is a progressive dose-response relationship, without an apparent threshold, between salt intake and increased blood pressure across a range of salt intakes (DGAC, 2005). Published findings indicate that the genesis of hypertension begins in childhood and that blood pressure-related vascular disease is already evident at early ages (Cutler and Roccella, 2006). Specifically, in autopsy studies of children and young adults, elevated blood pressure in children is directly associated with fatty streaks and fibrous plaques in the aorta and coronary arteries (Berenson et al., 1998). In young adults, there is a direct relationship between blood pressure and coronary artery calcium scores (Loria et al., 2007; Mahoney et al., 1996).
As in adults, sodium reduction during childhood lowers blood pressure. Therefore, decreases in sodium intake during childhood and early adulthood are thought to help blunt the well-documented increases in blood pressure that occur with age among the U.S. population and thereby prevent the development, or delay the onset, of clinical hypertension (Cutler and Roccella, 2006; Ellison et al., 1989; He and MacGregor, 2006).
In addition to the progressive nature of increasing blood pressure levels and associated cardiovascular disease risks throughout life as noted above,
the most recent Dietary Guidelines Advisory Committee (DGAC, 2005) also noted that inclusion of children beginning at 2 years of age is based partly on concerns about the development of taste preferences for foods with added salt at young ages. As discussed in Chapter 3, preferences for salt taste begin as early as 4 months of age and are shaped by experiences with foods. Moreover, throughout the lifespan, adaptation to lower sodium intake can occur if introduced gradually.
An additional point of controversy concerning extension of the reduction of sodium intake to the general population is the issue of salt sensitivity. This concept refers to differences between individuals in the way that their blood pressure responds to changes in dietary salt intake (Strazzullo, 2009). Although some argue that if salt sensitivity were taken into account as part of dietary recommendations, such recommendations would not need to be expanded to the general population, the major national authoritative consensus bodies have not supported the conclusion that salt sensitivity mitigates the concern for a general population approach (DGAC, 2005; IOM, 2005). There is variation in responses to changes in salt intake (IOM, 2005). However, such changes do not reflect a threshold effect, but rather have a continuous distribution (DGAC, 2005). There are no established standardized diagnostic criteria or tests, and there is no biological basis for deriving meaningful cut-points (Cutler et al., 2003; DGAC, 2005). Further, the responses are modifiable by factors such as potassium and other dietary intakes. For these reasons, there is no validated or scientifically defensible basis on which persons could be identified as “salt sensitive” or “salt resistant.” As such, the concept of salt sensitivity does not provide a basis to identify a subgroup of the total population as a target group (IOM, 2005).
Based on the consensus reports from expert advisory committees and relevant published literature, the strategies to be developed are to be targeted to the general population and consistent with the statement of task. The goal is an overall population-wide intake of sodium consistent with the levels specified by the Dietary Guidelines for Americans.
Development of Recommended Strategies
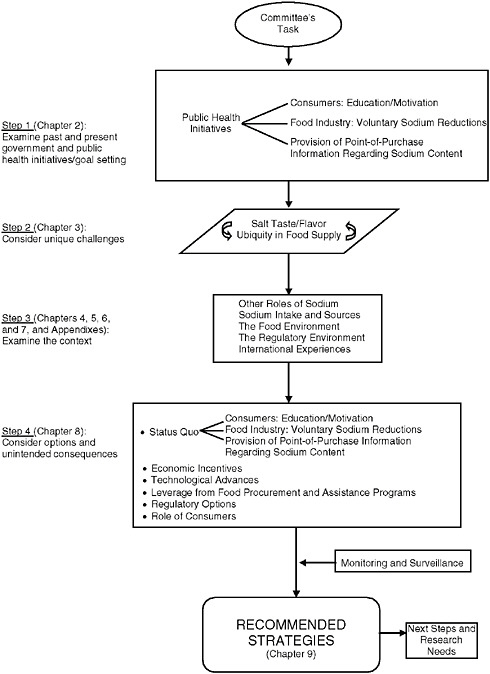
The steps followed by the committee in recommending strategies to reduce sodium intake are illustrated in Figure 1-1. At the outset, it is important to clarify key terminology. Although the term “salt” (sodium chloride) is not interchangeable with the term “sodium,” many reports use them synonymously because the most significant contributor to dietary sodium is salt. This report uses the term “salt” when the intended reference is to sodium chloride, and the term “sodium” when the intended reference is to sodium. Further, the term “food industry” is meant to encompass
both processed food manufacturers and restaurant/foodservice operations. “Salt taste preference” is used to mean the preference for foods to which salt has been added. Terms used in this report are defined in the Glossary (Appendix A).
The committee began its work by reviewing the past and current major national public health initiatives and international efforts (see Appendix C) targeted to the reduction of sodium intake, and integrated summaries of the key outcomes so as to provide an overall but focused picture of the current situation. This effort, as presented in Chapter 2, along with considerations of the special nature of salt taste and flavor (Chapter 3), sets the stage for the committee’s more in-depth examination of factors important to recommending strategies to reduce sodium intake
Importantly, these long-standing public health activities have been oriented primarily toward affecting the behaviors of consumers through consumer education and motivating consumers to alter food behaviors. However, these initiatives included calls for supporting activities in the form of (1) efforts by members of the food industry to voluntarily reduce sodium in their products and (2) information about the sodium content of foods to be made available at the point of purchase. As a sequel to its initial consideration of past and current initiatives, the committee next examined the taste and flavor effects of salt, as well as the nature of salt taste and the preference for foods to which salt has been added, notably in the context of the high levels of salt in the food supply and the role that preference for foods to which salt has been added may play in impacting the success of strategies to reduce sodium intake. In this way, Chapters 2 and 3 served as stage-setting activities for the committee.
The committee next turned to an in-depth review of the data underlying the outcomes, as well as additional background information, reviewing the following topics: the nature of the roles of sodium in food beyond taste and flavor effects (Chapter 4); current estimates of sodium intake and characterization of dietary sources of sodium (Chapter 5); the food environment as it relates to the processed food and restaurant/foodservice industries and consumers (Chapter 6); and the regulatory environment and legal provisions that pertain to the addition of salt to foods and related labeling information (Chapter 7). The committee also considered international experiences related to the reduction of sodium intake, compiled in Appendix C.
This information allowed the committee to fully consider the lessons learned and provided a basis upon which to consider relevant strategies (Chapter 8). The committee targeted this integrative discussion to focus first on the status quo and then on the potential for economic incentives, technological advances, and for leverages from large-scale government procurement and assistance programs. Regulatory options were considered as were potential roles for consumers. Recommendations are presented in
Chapter 9, and Chapter 10 discusses activities for the implementation of the recommended strategies and research needs. Chapter 11 contains the committee member biographical sketches.
REFERENCES
Alderman, M. H. 2010. Reducing dietary sodium: The case for caution. Journal of the American Medical Association 303(5):448-449.
Berenson, G. S., S. R. Srinivasan, W. Bao, W. P. Newman III, R. E. Tracy, and W. A. Wattigney. 1998. Association between multiple cardiovascular risk factors and atherosclerosis in children and young adults. New England Journal of Medicine 338(23):1650-1656.
Bibbins-Domingo, K., G. M. Chertow, P. G. Coxson, A. Moran, J. M. Lightwood, M. J. Pletcher, and L. Goldman. 2010. Projected effect of dietary salt reductions on future cardiovascular disease. New England Journal of Medicine 362(7):590-599.
CDC (Centers for Disease Control and Prevention). 2009. Application of lower sodium intake recommendations to adults—United States, 1999–2006. Morbidity and Mortality Weekly Report 58(11):281-283.
Cohen, H. W., S. M. Hailpern, J. Fang, and M. H. Alderman. 2006. Sodium intake and mortality in the NHANES II follow-up study. The American Journal of Medicine 119(3): 275.e7-275.e214.
Cook, N. R., J. A. Cutler, E. Obarzanek, J. E. Buring, K. M. Rexrode, S. K. Kumanyika, L. J. Appel, and P. K. Whelton. 2007. Long term effects of dietary sodium reduction on cardiovascular disease outcomes: Observational follow-up of the trials of hypertension prevention (TOHP). British Medical Journal 334(7599):885-888.
Cutler, J. A., and E. J. Roccella. 2006. Salt reduction for preventing hypertension and cardiovascular disease: A population approach should include children. Hypertension 48(5): 818-819.
Cutler, J., E. Obarzanek, and E. Roccella. 2003. Dietary salt reduction. In Lifestyle modification for the prevention and treatment of hypertension, edited by P. K. Whelton, J. He, and G. T. Louis. New York: Marcel Dekker. Pp. 139-159.
Cutler, J. A., P. D. Sorlie, M. Wolz, T. Thom, L. E. Fields, and E. J. Roccella. 2008. Trends in hypertension prevalence, awareness, treatment, and control rates in United States adults between 1988–1994 and 1999–2004. Hypertension 52(5):818-827.
Danaei, G., E. L. Ding, D. Mozaffarian, B. Taylor, J. Rehm, C. J. L. Murray, and M. Ezzati. 2009. The preventable causes of death in the United States: Comparative risk assessment of dietary, lifestyle, and metabolic risk factors. PLoS Medicine 6(4).
DGAC (Dietary Guidelines Advisory Committee). 2005. Report of the Dietary Guidelines Advisory Committee on the Dietary Guidelines for Americans, 2005. A Report to the Secretary of Health and Human Services and the Secretary of Agriculture. Washington, DC: U.S. Department of Agriculture and U.S. Department of Health and Human Services.
Ellison, R. C., A. L. Capper, W. P. Stephenson, R. J. Goldberg, D. W. Hosmer Jr., K. F. Humphrey, J. K. Ockene, W. J. Gamble, J. C. Witschi, and F. J. Stare. 1989. Effects on blood pressure of a decrease in sodium use in institutional food preparation: The Exeter-Andover project. Journal of Clinical Epidemiology 42(3):201-208.
He, F. J., and G. A. MacGregor. 2006. Importance of salt in determining blood pressure in children: Meta-analysis of controlled trials. Hypertension 48(5):861-869.
IOM (Institute of Medicine). 2005. Dietary Reference Intakes for water, potassium, sodium, chloride, and sulfate. Washington, DC: The National Academies Press. Pp. 269-423.
IOM. 2010. A population-based policy and systems change approach to prevent and control hypertension. Washington, DC: The National Academies Press.
Jula, A. M., and H. M. Karanko. 1994. Effects on left ventricular hypertrophy of long-term nonpharmacological treatment with sodium restriction in mild-to-moderate essential hypertension. Circulation 89(3):1023-1031.
Loria, C. M., K. Liu, C. E. Lewis, S. B. Hulley, S. Sidney, P. J. Schreiner, O. D. Williams, D. E. Bild, and R. Detrano. 2007. Early adult risk factor levels and subsequent coronary artery calcification: The CARDIA study. Journal of the American College of Cardiology 49(20):2013-2020.
Loria, C. M., E. Obarzanek, and N. D. Ernst. 2001. Choose and prepare foods with less salt: Dietary advice for all Americans. Journal of Nutrition 131(2, Supplement 1): 536S-551S.
Mahoney, L. T., T. L. Burns, W. Stanford, B. H. Thompson, J. D. Witt, C. A. Rost, and R. M. Lauer. 1996. Coronary risk factors measured in childhood and young adult life are associated with coronary artery calcification in young adults: The Muscatine study. Journal of the American College of Cardiology 27(2):277-284.
McCarron, D. A. 2000. The dietary guideline for sodium: Should we shake it up? Yes! American Journal of Clinical Nutrition 71(5):1013-1019.
McCarron, D. A. 2008. Dietary sodium and cardiovascular and renal disease risk factors: Dark horse or phantom entry? Nephrology Dialysis Transplantation 23(7):2133-2137.
McCarron, D. A., J. C. Geerling, A. Kazaks, and J. S. Stern. 2009. Can dietary sodium intake be modified by public policy? Clinical Journal of the American Society of Nephrology 4(1):1878-1882.
Muntner, P., J. He, J. A. Cutler, R. P. Wildman, and P. K. Whelton. 2004. Trends in blood pressure among children and adolescents. Journal of the American Medical Association 291(17):2107-2113.
NHLBI (National Heart, Lung, and Blood Institute). 2004. The seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and the Treatment of High Blood Pressure. NIH Publication No. 04-5230. Bethesda, MD: National Heart, Lung, and Blood Institute.
Ostchega, Y., S. S. Yoon, J. Hughes, and T. Louis. 2008. Hypertension awareness, treatment, and control—Continued disparities in adults: United States, 2005–2006. NCHS Data Brief No. 3. Hyattsville, MD: National Center for Health Statistics.
Palar, K., and R. Sturm. 2009. Potential societal savings from reduced sodium consumption in the U.S. adult population. American Journal of Health Promotion 24(1):49-57.
Smith-Spangler, C. M., J. L. Juusola, E. A. Enns, D. K. Owens, and A. M. Garber. 2010. Population strategies to decrease sodium intake and the burden of cardiovascular disease. Annals of Internal Medicine 152(8):481-487.
Strazzullo, P. 2009. Compelling evidence for salt-dependence of blood pressure from GENSALT. Journal of Hypertension 27:22-23.
USDA/HHS (U.S. Department of Agriculture/U.S. Department of Health and Human Services). 2005. Dietary Guidelines for Americans. 6th ed., Home and Garden Bulletin No. 232. Washington, DC: U.S. Government Printing Office.
Vasan, R. S., A. Beiser, S. Seshadri, M. G. Larson, W. B. Kannel, R. B. D’Agostino, and D. Levy. 2002. Residual lifetime risk for developing hypertension in middle-aged women and men: The Framingham Heart Study. Journal of the American Medical Association 287(8):1003-1010.
Xu, J., K. D. Kochanek, and B. Tejada-Vera. 2009. Deaths: Preliminary data for 2007. National Vital Statistics Reports 58(1).












