
9
Incentives Aligned with Value and Learning
INTRODUCTION
The present structure of the American healthcare system rewards volume over value and performing procedures over achieving the best outcomes. Transforming the health system will require a radical change in key precepts—including incentive schemes—and has the potential to elevate national healthcare statistics from mediocre to excellent. If this is to occur, commitments must be made by all stakeholders, and incentives will need to encompass both monetary and professional rewards. Incentive programs already are scattered across the country, but the system as a whole should be reengineered so that all stakeholders—for example, physicians, patients, health systems, payers, advocacy groups, and insurers—provide incentives for constant improvement, science-driven care, and value.
Papers in this chapter illustrate approaches to realign incentives to reward value and learning over volume and excess. In the first paper, Michael E. Chernew of Harvard University argues that cost containment and payment for value, not volume, should rank high in strategies to effect transformative change. He shows how global payment models offer promise for building a system based on science and value. Integral to realigning the health system are comprehensive performance measures that are based on solid evidence and observability as well as incentives that reward positive health outcomes.
The second paper, presented by Richard Gilfillan, formerly of Geisinger Health System, makes a business case for practicing evidence-based, integrated care rather than the high-volume, fragmented care typical in much of the United States. He notes that the business model for providers and hos-
pitals should be the main focus as it can trump à la carte incentives in determining whether individuals or organizations focus on volume vs. value. Additionally, Gilfillan highlights how systems approaches can produce reliable processes that minimize errors and how systems can be designed to put evidence-based knowledge in the real-time care workflow.
Anne F. Weiss and Bianca M. Freda of The Robert Wood Johnson Foundation describe the Aligning Forces for Quality (AF4Q) initiative. Active in 17 regions around the country, leadership teams of multiple stakeholders are involved in crafting performance measures, building quality improvement infrastructure, and assessing ways to better engage the public in the concept of a learning health system. The authors state that through the AF4Q initiative, the Foundation hopes to learn how to improve messaging, encourage community participation, and stimulate a learning culture.
PAYING FOR VALUE AND SCIENCE-DRIVEN CARE
Michael E. Chernew, M.D.
Harvard University
All stakeholders agree that the healthcare system should promote value: the amount of benefits received per dollar spent. Clinical improvements are likely the most significant benefit, but nonclinical benefits, such as reassurance, are important as well. Admittedly, benefit is in the eye of the beholder, but it is useful in this context to define benefits from a patient-centric perspective. Value calculations should use a broad definition of costs, including medical and nonmedical costs associated with care. Many tools can be used to promote value, including the design of provider payment and benefits, the focus of this paper.
The general theory of how value is created in competitive markets is straightforward. Consumers know their preferences. They face prices. They make choices. In a perfectly competitive setting, economists define the outcomes of those choices as reflecting value. This model is subject to extensions and caveats as markets deviate from perfect competition, but for the most part, it captures how market economies work.
In imperfect markets, consumers may not be making the right choices (in their diet, for example), but solutions often require more paternalism than economists typically prefer. When problems arise within such markets, private or public information is often provided to improve choice, or markets are regulated to prevent the most serious problems. But in most markets, interventions are modest, and market forces are the benchmark strategy used to generate value. The problem in health care is that for a number of reasons related to imperfect markets and the salience of health, the problems are more severe.
A key problem is that consumers do not observe quality in health care. Quality measurement and communication in health care may be improved, but for the foreseeable future, the information available will be woefully inadequate to support a perfect market. Moreover, in part because of poor information, providers have weak incentives to improve quality. For example, if a provider works in a hospital and is paid per admission, he/she has little incentive to improve quality and prevent readmissions. On the patient side, apart from the information problem, insurance distorts the choices because incentives to avoid high-cost treatments and providers are typically very weak.
The issue of obtaining value on the provider’s side generally focuses on changing provider incentives and combining those incentives with information. Payment reform, including value-based purchasing, is largely a provider-centric way of promoting value. This is in contrast with value-based benefit design, which is patient-centered. The two are not mutually exclusive, and they should be synergistic. For example, it would be problematic if all services were free for patients but providers were discouraged from providing those services. Recognizing where to use patient versus provider incentives and how to integrate them is important.
Despite the focus on value, the overarching concern of the healthcare system must be spending growth. In the President’s budget, the ratio of debt to gross domestic product (GDP) becomes 90 percent by 2020 (Figure 9-1) (CBO, 2010). That ratio is not good, and it also is on an upward trajectory,
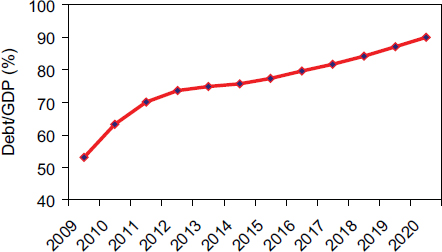
FIGURE 9-1 Expected trajectory of ratio of U.S. debt to gross domestic product (GDP). Payment must do more than promote value; it must also control costs.
NOTE: Cited from CBO Analysis of the President’s 2011 Budget.
SOURCE: CBO, 2010.
which is even more concerning. Much of the forecast is based on projected healthcare spending. This fiscal imbalance must be resolved, the mechanisms used will define the healthcare system of the future, ideally promoting value while constraining spending.
Alternate Payment Systems
Incentives and payment for promoting value must be designed to control aggregate spending. This is important when considering payment systems because they must be evaluated not simply on the basis of whether they promote value (which is important), but also on the basis of whether they contribute to a fiscally sustainable healthcare system.
One prominent payment strategy for promoting value is pay for performance (P4P). It is almost cliché to observe that one will get what one pays for. Currently, because value is not being paid for, value is not being delivered. The idea behind P4P is that high-value services can be defined and paid for. P4P raises several concerns. One example is the comprehensiveness of measures. Everything cannot be measured. Current measure sets can be expanded, but they will remain incomplete. The result is a multitasking problem. If one thing is paid for, providers may stop doing other things, even if some of those things are high-value. Another concern is the size of the reward. How big a reward is needed to change behavior meaningfully? There are also issues of design. Should providers be paid for relative or absolute performance? Existing evidence for the success of P4P programs is limited, much more limited than the proponents of P4P would have thought 5 to 10 years ago. Richard Frank and Kathleen Mullen conclude an evaluation of a P4P program in California by noting, “Our results cast doubt on the promise of pay for performance as a transformative mechanism for improving the general quality of the healthcare system” (Mullen et al., 2010). Overall, P4P should be considered a tool to be used in the context of broader payment reform. The fundamental concern in health care is the spending trajectory, and it is unlikely that P4P programs alone will be able to change that trajectory sufficiently. Moreover, the technical concerns are sufficiently great that P4P is unlikely to be the foundation of an incentive program designed to promote value.
Another payment approach involves bundling payments. One bundling strategy is episode-based payment. The idea behind episode-based payment is that payment should be made for episodes of care, bundled across as many services and providers as possible. This approach contrasts with fee-for-service, which encourages fragmented care. Hospitals and their physicians should be included in the bundle, and in many cases, other services, such as post–acute care, should be bundled in as well. Payment should be defined based on what consumers care about (care for a particular ailment
or collection of ailments), as opposed to the detailed services that are part of that care.
Episode payment requires good performance standards to ensure that people are actually receiving good-quality care. Obviously, the least costly way to provide care is not to provide it. As with P4P, technical issues arise about how to implement episode payment. Episodes must be defined, and it must be recognized that people have multiple episodes. Establishing payment rates is problematic if a patient has multiple episodes concurrently. Another concern is who controls the payment (who is the residual claimant). Finally, it remains to be seen how much of health care is amendable to episode definition and how payments would be updated over time. Episode-based payment has been implemented, at least on a limited scale, demonstrating its feasibility. For the reasons cited above (comprehensiveness, dealing with multiple episodes), however, it is probably best to view episode-based payment as a tool, as opposed to the fundamental way of solving cost and quality problems.
Another bundled payment approach is global payment, which entails a single risk-adjusted payment to providers (or a provider group). This approach should be defined to include performance standards, which address the incentive to provide less care and distinguishes this strategy from past capitation approaches. Global payment also must deal with the risk faced by providers. Doing so may require a transformation of practice organization, which, while challenging, is feasible. Many accountable care organization models, which use gain sharing, are a form of this approach. Implementation issues, such as how the money flows and who is the residual claimant, would have to be considered carefully. As with episode-based payment, the process for updating fees over time is important. Nevertheless, because of its global nature, this approach is a much more likely starting point for solving the fundamental cost problem than some of the other payment strategies.
One example is the Alternative Quality Contract that is offered by Blue Cross Blue Shield of Massachusetts. A global payment is made to a physician organization that assumes accountability for the full continuum of care—from preventive to end-of-life care and everything between. The global budget is updated over 5 years, in general by the consumer price index, so providers agree to a global payment trajectory for 5 years. This is not a 1-year capitation. Providers can receive performance bonuses, and there is a comprehensive set of ambulatory and inpatient performance measures. Payment flows to providers just as in a fee-for-service system, but it is oriented to the primary care physician group (which could be a multispecialty group), which is the residual claimant (and bearer of the risk). This makes the approach consistent with medical home models.
Performance Measures in a Learning Health System
All of the new payment models require performance measurement which will need to be able to identify bad performers; be supported and informed by a strong clinical research base; and adjust for risk. Meeting many of these requirements is facilitated by larger care systems and better information systems, suggesting that care systems are likely to become larger.
The question at hand is how to deal with this issue in a learning environment, especially in a healthcare system that is constantly evolving with new evidence being generated. New approaches are good, but quality measures are unlikely to incorporate cutting-edge care directly. Evidence takes time to develop and to be accepted. Some outcome measures, however, such as patient satisfaction, complications, and readmission rates, hold potential for capturing innovation. A set of outcome measures may be broad enough to capture providers who significantly underutilize high-value, cutting-edge care.
Updating measures for innovative care will be a particular challenge. New measures will have to be incorporated as new data emerge. The measure set will always lag. A core set of measures that are transparent and developed through some public or quasi-public process will be necessary. Additionally, some expansion and experimentation by purchasers will have to be allowed as they devise new measures. This will be an ongoing process among purchasers and other quality-focused entities.
Updating bundled payment for new services will be a particular challenge that will require considerable clinical knowledge. Payers will have to develop a system for increasing payments if particularly valuable services are developed, but the system will need to maintain overall fiscal restraint.
In the context of any fiscally sensible system, maintaining quality will require ongoing effort. However, if the concern is not to diminish quality in any way and thus to pay for whatever people (or their doctors) want, the system will collapse by its own weight, and quality will suffer.
Conclusion
In summary, the economy is the goose that lays the golden egg (the healthcare system). If spending increases enough that it destroys the economy, the healthcare system will be degraded. A quick recipe for going forward is to (1) start with cost containment, probably moving to global payment; (2) build as comprehensive a performance system as possible; (3) incentivize patients appropriately; (4) provide as much information as possible to everyone in a manageable way; and (5) encourage organizational reform. Taking these steps will entail a great deal of work, but we may have no choice but to start the journey.
GENERATING EVIDENCE TO GUIDE CARE
Richard Gilfillan, M.D.
Geisinger Health System (former)
Center for Medicare and Medicaid Innovation
America’s healthcare industry is highly innovative in sectors that reward innovation. The development of electronic health records (EHRs) and other data management innovations will speed learning and innovation, but these innovations could produce either more or less value for patients depending on the industry’s business model. The current business model focuses learning and innovation on increasing the volume of and revenue for services provided. To focus learning on innovation and produce more value for patients, new business models are needed that reward patient-centered value. There are ample opportunities to improve the value produced by the healthcare system, and there is much to be learned. The recent healthcare reform legislation includes a number of alternative reimbursement approaches for Medicare and Medicaid. Private payers could work closely with the Centers for Medicare & Medicaid Services (CMS) to develop robust partnerships with providers committed to learning to deliver higher-value care. Such organizations, with a preponderance of their business dependent on delivering high-value outcomes, will demonstrate how much more value the healthcare system can deliver.
Patient-Centered Value as the Vision
The good news is that the United States already spends $2.6 trillion annually on health care. That amount should be more than enough to cover everyone. Yet the nation has 40 million people uninsured, experiences frequent medical expense–driven personal bankruptcies, and is characterized by highly variable clinical outcomes. From a patient perspective, we have a low-value system. The problem is that too much of the value produced by the system flows to producers, including insurers, hospitals, physicians, and other providers of care.
The Institute of Medicine’s (IOM’s) learning health system, the Institute for Healthcare Improvement’s (IHI) triple aim framework (population health, experience of care, per capita costs), and The Commonwealth Fund’s high-performance delivery system constitute alternative visions of a system that would optimize the quality, affordability, and experience of care for patients (Berwick et al., 2008; Commonwealth Fund, 2010; IOM, 2007). All are based on a patient-centered, value-driven healthcare system. The Affordable Care Act (ACA) of 2010 assumes that higher-value care would help finance coverage for millions of uninsured Americans. These
visions all rely on increased innovation and knowledge to create higher-value care.
But are innovation and knowledge necessarily drivers of value? Should we press for more innovation and systems of learning without addressing the business context in which they occur?
The Healthcare Industry Business Model
Businesses produce what is rewarded. Industries evolve from business models that align incentives with desired outcomes. The healthcare industry’s fee-for-service business model is perfectly aligned with the rewarded outcomes: more revenue from more services. The dictum “no margin, no mission” recognizes that not-for-profit healthcare organizations operate within the same context and generally produce the same high-cost outcomes.
In policy discussions, the U.S. healthcare system is expected to produce efficient, high-quality care and is referred to as broken because it does not. Yet no rewards are provided for high-value care, and no one is held accountable for producing it. By rewarding piecework, the current business model encourages fragmentation of care. If no one is in charge, no one can be accountable for the outcomes that occur. The automobile industry is more accountable for health outcomes than is the healthcare industry. When accelerator problems in its cars were found to cause 3.5 deaths per year, Toyota was forced to recall and fix 8.5 million cars. When the IOM identified 90,000 unnecessary deaths per year caused by medical errors, there was no one to call (IOM, 1999). Ten years later, despite a great deal of work and attention, medical errors continue to cause thousands of deaths annually (Sebelius, 2010).
If high-value outcomes are desired, business models that reward providers for delivering those outcomes are needed. The right business models to produce high-value care are unknown, although proposals abound. Congress has included a variety of new payment initiatives in the healthcare reform legislation so that different models can be evaluated. One thing is certain: if we are going to achieve the visions of the IOM, IHI, and The Commonwealth Fund, the primary challenge for policy makers and healthcare managers over the next decade will be driving and managing the transition of the healthcare business model from producer-centered volume to patient-centered value. Key attributes of these models are listed in Box 9-1.
The Role of Innovation and Learning
Policy makers have identified a lack of innovation and knowledge of what treatments work as reasons for the current low-value system. But
BOX 9-1
A Choice of Healthcare Business Models
| Producer-Centered Volume | vs. | Patient-Centered Value |
| • Uncoordinated | • Coordinated | |
| • Fragmented | • Integrated | |
| • High-cost | • Lower-cost | |
| • Fair quality | • High quality | |
| • Minimal accountability | • Triple aim accountability |
innovation and learning do not occur in a vacuum. Dynamic industries learn because innovative business practices are rewarded. Moore’s law for the semiconductor industry states that the number of transistors that can efficiently be placed on an integrated circuit board doubles every 2 years. This law has held true for 45 years because faster, smaller processing chips produce large margins for Intel and other focused producers. Learning and innovation follow the business model.
Producer-Centered Volume Innovation and Learning
The current healthcare business model directs innovation in three ways. Businesses proactively select innovation and learning opportunities based on the expected business development opportunity. An example is the focus on new drugs to treat chronic diseases that are prevalent in developed countries. Businesses typically do not invest in learning that offers no return. Businesses also avoid innovations that might compromise their success. Hospitals traditionally have not invested in programs to decrease readmissions.
Rapid innovation occurs in health care. I recently heard a presentation by a medical device sales representative who proudly displayed four iterative versions of her company’s spinal fusion screws. The cycle time was 9 months. The speaker had no information demonstrating improved outcomes for patients.
Case mix adjustment for Medicare Advantage (MA) plans provides another example. CMS began the rollout of Hierarchical Condition Categories (HCC) coding for case mix adjustment in 2004. Over the next 3 years, an entire new industry segment of HCC coding optimization erupted. The innovation was driven by a fundamental change in the business model for MA plans. When revenue became a direct function of population risk, investments in systems to fully identify the burden of patient risk became a necessity.
Innovation in the pharmaceutical industry continues to produce important advances in specialty drugs. Unfortunately, the pace of value-adding discoveries in the more traditional pharmaceutical sector has slowed. Much of the learning and innovation has produced “me too” drugs that provide high margins for producers but little incremental value for patients.
Why does the healthcare system invest in non-value-added medical devices, coding systems, and purple pills, but not programs for care transitions? The obvious answer is that the former are driven by strong business cases, while the latter are not. In the current business model, innovation is much more likely to decrease than to increase patient-centered value. The United States does not have low-value health care because it lacks knowledge about delivering high-value care, but because the healthcare business model rewards and thereby drives low-value care. Innovation and learning need to be focused on patient-centered value business models that reward them.
Patient-Centered Value Innovations
Geisinger Health System (GHS) includes a Clinical Enterprise with 800 physicians and three hospitals and a 240,000-member Geisinger Health Plan (GHP). The system has EHRs that connect all sites of care and GHP. Neither entity works exclusively with its GHS partner. Both rely on non-Geisinger relationships for the majority of their business. GHS physicians do provide primary care for 40 percent of GHP members. This shared population provides an opportunity for joint pursuit of innovative care delivery and financing initiatives.
Five years ago, the GHS board of directors and leadership made “Geisinger Quality” the central strategic goal. There were four reasons for this approach:
- It is the right thing for our patients and our community.
- It inspires our staff.
- Our integrated system is well positioned to create knowledge about higher-value care.
- The current model is not sustainable.
Quality was broadly defined to include the IOM’s six aims for quality improvement (IOM, 2001) and several other dimensions. Generally, the goal was to deliver high-value patient-centered care.
To execute this strategy, we developed a series of care transformation initiatives as joint projects of our Clinical Enterprise and GHP teams. These initiatives target care models of high frequency and costs that also demonstrate high variance in care and outcomes—models that could be significantly improved to deliver higher-value outcomes for patients.
Once care models have been identified for improvement, evidence-based best practices are researched, agreed upon, and implemented. The EHR is used to enable this reengineered care and to collect data with which to document results. A new GHP contractual arrangement also is put in place to align reimbursement with the expected higher-value outcomes. The payment approaches are aligned with the nature of the clinical process of care. Global, bundled payments are used for patient-based episodic care, while pay for performance and shared savings incentives are used for population-based improvements. Each care model innovation, then, is accompanied by a new business model that rewards high-value outcomes.
Each initiative typically tracks process, outcome, efficiency, and patient satisfaction metrics. Process metrics demonstrate compliance with evidence-based care. Outcome metrics show the impact of the new care pathways on patients’ health status. Efficiency metrics track improvements in the total payer cost or in the cost of delivering a service. Patient satisfaction metrics monitor the patient experience of care.
Improvement in these measures of success leads to better financial results for the Clinical Enterprise. Physicians and operational managers are directly impacted as well because their performance evaluations and incentive payments are based on the same outcomes. The effect of these changes in clinical and reimbursement models, then, is to bring the value dimensions of patient experience, health status, and efficiency into the managerial mainstream. Clinical managers and physicians are directly accountable for, and therefore attentive to, outcomes. Outcome measures for the population are the measures of operational success tracked directly by managers. Value garners managerial attention.
The standard reimbursement arrangement between the parties is a straightforward fee-for-service contract. For the clinical enterprise, these programs move the business model from volume toward value. For GHP, the better outcomes, more satisfied patients, and lower costs provide an opportunity for growth in market share. Accordingly, GHP provides additional payments to help the physicians and practices finance the care transformation. The revised business models establish a “virtuous cycle” that drives a provider–payer partnership to deliver better patient outcomes and higher-value health care.
Examples of this approach include the following:
ProvenCare Acute:
- Population—those undergoing acute surgical and medical procedures
- Care model innovation—evidence-based redesigned care pathways for acute hospital services
- Business model innovation—bundled payment for an episode of care
- Measures of success—outcome metrics, compliance with guidelines, patient satisfaction, cost of services
- Result—improved outcomes and cost of services (Table 9-1)
Chronic Disease Care Optimization:
- Population—primary care office patients with chronic diseases
- Care model innovation—evidence-based care pathways and EHR-based registries and reminders for patients with diabetes, high blood pressure, and hyperlipidemia
- Business model innovation—pay-for-performance incentives
- Measures of success—bundled metrics for diabetes, hypertension, cholesterol and preventive services, patient satisfaction
- Results—marked improvement in all metrics (Table 9-2)
ProvenHealth Navigator:
- Population—all Medicare beneficiaries seen in primary care offices
- Care innovation—value-driven medical home model based on partnership between primary care providers and GHP
- Business model innovation—fee for service supplemented with stipends and a quality-driven shared savings model
- Measures of success—triple aim outcome metrics for health status, patient experience of care, cost of care
- Results—improvements in Healthcare Effectiveness Data and Information Set, patient satisfaction, and cost metrics (Table 9-3)
Patient-Centered Value Learning
This patient-centered value business model focuses learning on systems to improve outcomes. This is best seen in our ProvenHealth Navigator medical home model. The measures of success for this model are improvements in the dimensions of health status, patient experience of care, and total cost of care. Physicians are rewarded explicitly for improvements along these dimensions. As a result, the practices and GHP are tightly focused on monitoring outcomes together. The entire practice team, including GHP in-office case managers, reviews outcome results at monthly meetings. The practice managers produce monthly reports demonstrating the results of chronic disease care and patient satisfaction for each physician. GHP staff report on patients admitted to the hospital, all readmissions, and the total cost of care. Admissions, readmissions, and concerns for specific patients or care systems are discussed with the entire staff. The whole team, including office staff and GHP payer staff, is engaged in conversations about what could be done
TABLE 9-1 Value Learning: ProvenCare
|
|
|
| Results | Improvement (%) |
|
|
|
| Patients with more than one complication | 28 |
| Atrial fibrillation | 17 |
| Any pulmonary complication | 43 |
| Deep sternal wound infection | 25 |
| Readmission within 30 days | 44 |
|
Innovation: Evidence-based best practice surgical case redesign |
|
|
Evidence Development: Process and outcome metrics for surgical care |
|
|
Incentive: 90 global payment, including complications |
|
|
|
|
TABLE 9-2 Value Learning: Chronic Disease Care Optimization
|
|
|
| Results | Improvement (%) |
|
|
|
| Diabetes bundle | 30 |
| Coronary disease bundle | 20 |
| Preventive care bundle | 75 |
|
Innovation: EHR-driven registries and reminders |
|
|
Evidence Development: Physician-specific monthly Healthcare Effectiveness Data and Information Set (HEDIS) metrics |
|
|
Incentive: Straight pay for performance |
|
|
|
|
TABLE 9-3 Value Learning: ProvenHealth Navigator
|
|
|
| Results | Improvement |
|
|
|
| Admissions | Decreased 16% |
| Readmissions | Decreased 30% |
| Quality metrics | Improved as noted in Table 9-2 |
|
Innovation: Medical home with population management built into the primary care office |
|
|
Evidence Development: Process and outcome metrics for surgical care |
|
|
Incentive: Fee for service, pay for performance, stipends and shared savings paid based on quality outcomes |
|
|
|
|
better. Examples of best practices from other offices are diffused rapidly. In this environment, the team members can see the impact they are having across an entire population. Every member knows that good outcomes will be celebrated and poor outcomes scrutinized to learn important lessons.
In the ProvenHealth Navigator model, outcome measurement flows directly and naturally from the delivery of care. Understanding the patient
experience, quality outcomes, and the cost of care is a central management function of the practice. Learning to improve these outcomes is built directly into the operations of the practice.
Lessons Learned
We have made mistakes and learned important lessons over the past 5 years. The most significant lessons learned are as follows:
• It is possible to improve delivery systems to optimize the quality, patient experience, and efficiency of care simultaneously.
• Change is difficult to accomplish in the context of daily practice; it requires ongoing attention, additional dedicated staff, and a good motivation.
• Financial support and rewards are essential to make the business case, but:
— individuals respond to multiple drivers, not just payment; and
— transparency, constant feedback, and celebration of success drive staff engagement.
• Clinical and business leadership are critical.
• The provider–payer partnership is central.
• Transparency works: sharing results within and across practices drives improvement.
• Engagement and accountability work best in small units—groups of four to five physicians.
• Clinical transformation is hard work—focusing on initiatives with broad impact delivers the most added value.
• Timely analysis of results is essential to rapid-cycle innovation.
• Innovations affecting small numbers of patients provide limited data for analysis and learning.
The innovations described in this paper impact a relatively small portion of the overall clinical activity of our system. Other parts of the system operate with a more traditional volume-based model, albeit within the culture of a not-for-profit multispecialty group practice. The results demonstrate what is possible within an organization operating two business models. How much more value could be produced in an environment where every operational area was working to optimize patient-centered value? Given the synergistic effects among initiatives that we have seen, we believe it would be possible to produce much more value in a simplified business environment.
Implications for Health Systems
Our experience leads to the following suggestions for organizations, providers, and payers that make a strategic commitment to delivering higher-value care to their communities:
• Make patient-centered value an explicit strategic commitment, and communicate it clearly to the organization.
• Make patient-centered value innovation objectives important drivers of senior leaders’ incentive plans.
• Include the innovation goal in all employee incentive plans.
• Build population registries and other tools with which to manage a population, not just those in the hospital.
• Form payer partnerships to align reimbursement and agree on joint initiatives and R&D investments.
• Explicitly identify the source of added value before selecting a particular initiative.
• Maximize the leverage of care redesign and reimbursement changes to drive the broadest clinical impact with the least administrative work.
• Shorten the learning cycle time:
— build evidence-based guidelines into the flow of care;
— build data capture into standard care processes; and
— measure and feed back results frequently.
• Extend initiatives to as many patients as possible to create mass and momentum for change, as well as meaningful data.
• Establish analytical resources close to the innovation activities to provide rapid evaluation and feedback.
• Celebrate success.
Public Policy Implications
The most significant public policy opportunity to improve value innovation and learning is to create the will for healthcare organizations to deliver high-value outcomes. The reimbursement innovations for providers and MA plans in the recent healthcare reform legislation will drive movement in that direction. The greatest impact would result if public and private payers developed a common approach that gave providers an unambiguous context in which to deliver higher-value care. Other suggestions include the following:
- Begin a public campaign to legitimize patient-centered value as an explicit aim.
- View CMS and the Center for Innovation as payer partners working with providers to deliver patient-centered value.
- Make outcome data rapidly available to providers operating under value-based contracts.
- Increase transparency and stimulate learning by providing claims data to third parties for provider profiling.
- Challenge payers and providers to step up to accountability.
- Develop partnerships with private payers to provide greater patient mass for care transformation efforts by providers.
- Build a rapid learning network; use the EHR capabilities of multiple integrated systems to establish a learning web that can mine current and future data to evaluate treatment impacts.
- Be cautious about evaluating initiatives that occur in provider systems with mixed business models.
Conclusion
Opportunities to improve the value of health care abound, even with the limited knowledge we have today. As the healthcare system becomes digitized, shorter learning and innovation cycles become desirable and inevitable. We will learn from other industries that use refined data management capabilities to adjust their operations in real time. Whether innovation will drive higher value for patients or more revenue and volume for producers is unclear. The most significant step we can take to ensure that innovation serves patients is to reward higher-value outcomes. Public–private payer initiatives with specific providers committed to an unambiguous patient-centered value business model would provide the most robust learning environment. This is the model that can teach us what is possible when every employee wakes up every day committed to learning how to better deliver high-value care for patients and the community.
CREATING A LEARNING CULTURE
Anne F. Weiss, M.P.P., and Bianca M. Freda, M.P.H.
The Robert Wood Johnson Foundation
The American healthcare system faces critical challenges, including poor quality, skyrocketing costs, and troubling racial and ethnic disparities. The ACA of 2010 arguably should provide tools to address many of these challenges. But it is unrealistic to expect that the nation’s healthcare system need only undergo a one-time transformation. Rather, the healthcare system will need the ability to identify problems proactively, develop solutions for those problems quickly, and create a culture that rewards
solutions and promotes the ongoing search for problems and their respective solutions. Essentially, real reform requires that health care become an ongoing learning enterprise. Unfortunately, health care currently is not that sort of system. In fact, American health care offers few incentives for, and indeed poses formidable barriers to, learning and problem solving. There is, however, hope. Work supported by The Robert Wood Johnson Foundation (RWJF) is helping the field understand some of the important necessary next steps toward such a learning system. Many observers have noted that the current system of paying for health care in the United States creates disincentives for high-quality care: it encourages wasteful and fragmented care and does not reward providers who struggle to deliver good care (Miller, 2009). RWJF’s work to improve healthcare quality suggests that there are, however, powerful nonfinancial incentives that can be used to influence behavior and shape a learning culture.
RWJF launched its Quality/Equality strategy and its signature initiative, Aligning Forces for Quality (AF4Q), in 2008. RWJF’s board of directors has made a $300 million commitment to the strategy through 2015. The strategy was designed around two principles: first, that while quality is a national problem, health care is delivered locally, and fixing it requires local action; second, that those who receive, give, and pay for care—consumers, providers, and purchasers—need to team up and align their efforts to create lasting change (Painter and Lavizzo-Mourey, 2008).
AF4Q is being implemented in 17 targeted regions. Three are states (Minnesota, Wisconsin, and Maine); one is a rural county in California; and most of the rest are multicounty or metropolitan areas. In each region, a multistakeholder team of healthcare leaders, physicians, nurses, consumers, health plans, business, and others carry out three key activities: they issue public performance reports on hospitals and physicians, develop a sustainable capacity or infrastructure to help physicians improve, and work to engage consumers in using healthcare information.
For this strategy to succeed, different stakeholder groups need to reach fundamental agreement on difficult tasks, such as defining and measuring good care, engaging professionals in efforts to improve care, and getting patients and consumers more involved in different aspects of their care. And they have to accomplish these tasks in the absence of any meaningful policy, social, or economic incentives. Although there is certainly overwhelming evidence of various kinds of healthcare quality problems, different groups generally understand those problems differently (AHRQ, 2009).
The challenge of getting different stakeholders aligned around common goals in AF4Q is very much like the challenges to creating a learning health system. RWJF and its partners have addressed these challenges by using strategic communications, engaging health system leaders, and engaging consumers.
Using Strategic Communications
During 2007–2009, RWJF, in partnership with several strategic communications firms, embarked on a series of message research projects with the general public, physicians, consumers, and employers. In general, these projects involved a review of existing research, individual interviews, focus groups, and telephone or online surveys. The firms developed evidence-based messages, which were extensively sourced to ensure that they would be credible. Messages were distributed widely to AF4Q community teams and other grantees, who were trained in using the messages and were given interactive tools, such as a slide builder. The messages, training, and tools have been extremely well received by the AF4Q communities. There are lessons to be learned about each audience for these communications and ways to reach them effectively, which should also prove useful in efforts to create a learning culture.
Research on the general public was conducted in part by a firm, Olson Zaltman Associates, with a unique methodology based on theories of cognitive learning: that people learn and perceive the world according to a few universal frames or metaphors, and these metaphors help them derive meaning from a wide range of related concepts. Therefore, the firm’s approach is to identify these universal emotional metaphors and use them as the foundation for messaging and engagement efforts. In the case of health care, Olson Zaltman Associates’ research reveals that people view health care as a journey from a state of confusion and complexity to one of relief and simplicity, and they see quality health care as a patient–provider relationship that takes them to their goal, around multiple barriers, and results in comfort and peace of mind. The essence of quality health care from patients’ perspective is having a close relationship with their medical provider that is based on trust.
Subsequent message research with a physician audience emphasized AF4Q’s focus on measuring and publicly reporting on the quality of care. This research revealed that physicians are understandably focused on how performance data are collected, adjusted, and analyzed and how the data will be used; they expressed the greatest confidence in initiatives led by their peers. Physicians were interested in how they compared with their colleagues but did not want this information made public. They did not expect their patients to use public performance information. The results of this research were used to develop messages that acknowledge problems with previous efforts to measure and report quality and physicians’ frustration with the healthcare system. These messages give physicians reasons to participate in the project and ask them to contribute their leadership, expertise, and influence to help improve care and make their patients better partners in care. It is also important to link the process of measuring and reporting on quality with payment reform.
Messages were developed for employers as well, based on insights provided by AF4Q communities. These insights revealed the need to communicate very basic reasons why employers should take an interest in poor healthcare quality and offer specific ways they can contribute. Major messages used with the employer audience include both the direct and hidden, indirect costs of poor health care; the added premium costs of wasteful, poor-value care; and examples of companies that have made a difference.
Engaging Health System Leaders
Health system leaders, such as hospital board members, do not always make quality a strategic priority (Jha and Epstein, 2010). Fewer than half of hospital board members rate quality of care as a top priority, and only a minority have been trained in quality. A number of quality improvement initiatives sponsored by RWJF have explored ways to engage board members and senior executives in efforts to measure and improve quality (RWJF, 2008). Based on those experiences, a number of recommendations can be made for engaging health system leaders in a learning community:
- Make the case based on both mission and margin: build evidence for how learning is “the right thing to do” but also is good for the bottom line.
- Use a trusted intermediary, not a consultant, to reach hospital leaders.
- Make learning activities a standing agenda item, with dashboard metrics that align with other institutional goals.
- Ask health system leaders to play a role in publicly showcasing and communicating about results, as well as in motivating staff.
Engaging Consumers
Consumer engagement is a critical strategic component of AF4Q, as it should be in a learning healthcare system. RWJF’s goal is for consumers to access and use health and performance information to make healthcare decisions at key points. Consumer representation in all aspects of a learning organization, including governance and decision making, is critical to achieving the goal of patient-centered care (Regenstein and Andres, 2010). Consumer representatives may require ongoing training and support to play a meaningful role.
Authentic consumer representation involves individuals who do not have a financial stake in the healthcare system. They may represent a specific constituency, be it faith-based, disease-based, or population-based (NPWF, 2009). Individuals who are current or retired employees of a
healthcare organization and their spouses are often tagged as “consumer” representatives but may not be able to play that role convincingly.
Too often, healthcare improvement initiatives focus on what is technically and politically feasible rather than what is of greatest importance to patients and families. This is due, in part, to the relative absence of information on meaningful outcomes that capture patients’ experience over time and in different settings, compared with an abundance of information on specific clinical processes and transactions. For example, while it is costly to collect information on patient experience, these measures provide direct information about the patient-centeredness of care at both the practice and provider levels, and positively correlate with processes of care for both prevention and disease management (Shaller et al., 2010). AF4Q sites are working to make the results of patient experience surveys more widely available, despite the difficulty of finding a sustainable business model for doing so. A learning health system should focus on and promote the issues that matter to patients and families.
Creating a Learning Culture: Some Conclusions
Although not backed by rigorous research results at this point, some insights about how to create a learning culture within the healthcare system have emerged from RWJF’s experience in promoting social change and AF4Q’s experience to date:
- Test change in local markets—Although healthcare quality is obviously driven by federal and state policy, as well as private market developments at every level, health care is delivered locally, and it is important to gain experience in different market environments around the country.
- Invest in message research and adhere rigorously to tested messages—Strategic communication is a proven critical component for achieving social change (Hurley et al., 2009).
- Insist on participation by multiple stakeholders (Sequist et al., 2008).
- Engage authentic consumer participation.
- Measure and focus on what matters.
- Value transparency.
- Do not neglect financial incentives—Although this paper has focused on nonfinancial ways to create a learning culture, creating such a culture is difficult in the face of payment systems that often punish, rather than reward, learning and improvement (RWJF, 2010).
REFERENCES
AHRQ (Agency for Healthcare Research and Quality). 2009. National healthcare disparities report. http://www.ahrq.gov/qual/nhqr09/nhqr09.pdf (accessed October 14, 2010).
Berwick, D., T. Nolan, and J. Whittington. 2008. The Triple Aim: Care, health, and cost. Health Affairs 27:759-769.
CBO (Congressional Budget Office). 2010. Analysis of the President’s 2011 budget: Letter from CBO director, Douglas W. Elmendorf to Daniel K. Inouye. http://www.cbo.gov/ftpdocs/112xx/doc11231/03-05-apb.pdf (accessed June 1, 2010).
Commonwealth Fund. 2010. Framework for a high performance delivery system. http://www.commonwealthfund.org/Content/Publications/Fund-Reports/2006/Aug/Framework-for-a-High-Performance-Health-System-for-the-United-States.aspx (accessed October 15, 2010).
Hurley, R., P. Keenan, G. Martsolf, D. Maeng, and D. Scanlon. 2009. Early experiences with consumer engagement: Initiatives to improve chronic care. Health Affairs 28(1):277-283.
IOM (Institute of Medicine). 1999. To err is human. Washington, DC: National Academy Press.
———. 2001. Crossing the quality chasm: A new health system for the 21st century. Washington, DC: The National Academies Press.
———. 2007. The learning healthcare system: Workshop summary. Washington, DC: The National Academies Press.
Jha, A., and A. Epstein. 2010. Hospital governance and the quality of care. Health Affairs 29(1):182-187.
Miller, H. 2009. Better ways to pay for health care: A primer on healthcare payment reform. Network for regional healthcare improvement. http://www.rwjf.org/files/research/nrhiseriesbettewaystopay.pdf (accessed June 20, 2011).
Mullen, K., R. Frank, and M. Rosenthal. 2010. Can you get what you pay for? Pay-for-performance and the quality of healthcare providers. The RAND Journal of Health Economics 41(1):64.
NPWF (National Partnership for Women and Families). 2009. Guide to engaging consumer advocates in AF4Q alliances. http://www.forces4quality.org/resource/guide-engaging-consumer-advocates-af4q-alliances (accessed October 15, 2010).
Painter, M., and R. Lavizzo-Mourey. 2008. Aligning forces for quality: A program to improve health and health care in communities across the United States. Health Affairs 27(5):1461-1463.
Regenstein, M., and E. Andres. 2010. Aligning forces for quality: Local efforts to transform American health care. Washington, DC: The Center for Health Care Quality, George Washington University Department of Health Policy.
RWJF (Robert Wood Johnson Foundation). 2008. Expecting success toolkit, chapter 2: Getting buy-in from the c-suite. http://www.rwjf.org/pr/product.jsp?id=30064 (accessed October 15, 2010).
———. 2010. Good for health, good for business: The case for measuring patient experience of care. http://www.forces4quality.org/resource/case-patient-experience (accessed October 15, 2010).
Sebelius, K. 2010. Statement of Kathleen Sibelius, Secretary U.S. Department of Health and Human Services, on the President’s fiscal year 2011 budget before the Subcommittee on Labor, Health and Human Services, Education, and Related Agencies, Committee on Appropriations, U.S. House of Representatives.
Sequist, T., E. Schneider, M. Anastario, E. Odigie, M. Marshall, W. Rogers, and S. D. Gelb. 2008. Quality monitoring of physicians: Linking patients‘ experiences of care to clinical quality and outcomes. Journal of General Internal Medicine 23(11):1784-1790.
Shaller, D., K. Browne, D. Roseman, and S. Levitan-Edgeman. 2010. Measuring patient experience as a strategy for improving primary care. Health Affairs 29:5.






















