
12
Valvular Heart Disease
The chapter on valvular heart disease (VHD) adds new listings specific to VHD. The awarding of disability is appropriate for all patients with severe symptomatic aortic stenosis and for other types of severe VHD associated with severe symptomatic impairment. Disease severity is determined by the echocardiogram and functional impairment by a careful history and physical examination and in some cases exercise testing.
DESCRIPTION
Valvular heart disease (VHD) is characterized by damage to or a congenital defect in one or more heart valves: mitral, aortic, tricuspid, and pulmonary. Heart valves have a single function: to permit unobstructed forward blood flow through the heart. Damaged or defective valves can cause two types of problems: either they fail to open properly (a condition called stenosis) impeding blood flow, or they leak (a condition called regurgitation) permitting back flow. Regurgitation occurs because a valve does not close tightly, which allows blood to flow back into the previous chamber from where it came. Mitral regurgitation is most often due to prolapse, a condition in which the valve leaflets bulge into the left atrium during a heartbeat. Stenosis occurs when the heart valve cannot fully open because the valve flaps, or ring, have become thick, stiff, or fused together, preventing sufficient supply of blood to flow through the valve.
Valve conditions may be congenital, arise from inflammation, or occur due to complications from infections. Mild or moderate disease is usually
asymptomatic at first, but due to the progressive and degenerative nature of the disease, may eventually become severe and lead to heart failure and death if left untreated. In general, VHD is related to aging. Prevalence is increasing as the U.S. population ages and lives longer. Aortic stenosis is the most common valve disease in the United States, followed by mitral regurgitation, aortic regurgitation, and mitral stenosis.
Symptoms of VHD in decreasing frequency include shortness of breath or dyspnea, chest pain and palpitations, and syncope or near syncope. Because nearly all patients with severe disease will present with one of these symptoms, VHD can usually be evaluated using the algorithms for these symptom categories described in Figure 12-1.
DIAGNOSTIC CRITERIA AND METHODS
Two simple principles govern the management of VHD and the probability that a patient is disabled from it: the presence of symptoms and the severity of the lesion. Table 12-1 presents the categories of disease severity for each valve lesion. In general, but with rare exceptions, only severe disease is capable of causing symptoms and disability. VHD should be diagnosed based on clinical evaluation of the patient and assessment by
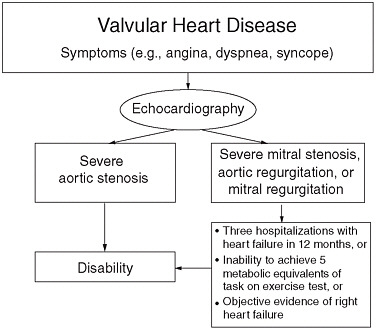
FIGURE 12-1 Determining listing-level disability for claimants with valvular heart disease.
TABLE 12-1 Characterization of Severe Valve Disease
|
Aortic Stenosis |
|||
|
|
Mild |
Moderate |
Severe |
|
Jet velocity (m per second) |
< 3.0 |
3.0–4.0 |
> 4.0 |
|
Mean gradient (mm Hg) |
< 2.5 |
25–40 |
> 40 |
|
Valve area (cm2) |
> 1.5 |
1.0–1.5 |
< 1.0 |
|
Valve area index (cm2 per m2) |
|
|
< 0.6 |
|
Mitral Stenosis |
|||
|
|
Mild |
Moderate |
Severe |
|
Mean gradient (mm Hg) |
< 5 |
5–10 |
> 10 |
|
Pulmonary artery systolic pressure (mm Hg) |
< 30 |
30–50 |
> 50 |
|
Valve area (cm2) |
> 1.5 |
1.0–1.5 |
< 1.0 |
|
Aortic Regurgitation |
|||
|
|
Mild |
Moderate |
Severe |
|
Qualitative |
|
|
|
|
Angiographic grade |
1+ |
2+ |
3–4+ |
|
Color Doppler jet width |
Central jet, width < 25% of LVOT |
More than mild but no signs of severe AR |
Central jet, width > 65% LVOT |
|
Doppler vena contracta width (cm) |
< 0.3 |
0.3–0.6 |
> 0.6 |
|
Quantitative (catheterization or echocardiography) |
|
|
|
|
Regurgitant volume (ml per beat) |
< 30 |
30–59 |
≥ 60 |
|
Regurgitant fraction (%) |
< 30 |
30–49 |
≥ 50 |
|
Regurgitant orifice area (cm2) |
< 0.10 |
0.10–0.29 |
≥ 0.30 |
|
Additional Essential Criteria |
|
|
|
|
Left ventricular size |
|
|
Increased |
|
Mitral Regurgitation |
|||
|
|
Mild |
Moderate |
Severe |
|
Qualitative |
|
|
|
|
Angiographic grade |
1+ |
2+ |
3–4+ |
|
Color Doppler jet area |
Small, central jet (< 4 cm2 or < 20% LA area) |
Signs of MR more than mild present but no criteria for severe MR |
Vena contracta width > 0.7 cm with large central MR jet (area > 40% of LA area) or with a wall impinging jet of any size, swirling in LA |
|
Doppler vena contracta width (cm) |
< 0.3 |
0.3–0.69 |
≥ 0.70 |
echocardiography (see Table 12-1). Obtaining detailed information about patients’ related symptoms while reviewing their medical histories is important to confirm the presence of possible comorbidities or detect possible VHD in asymptomatic patients.
Diagnosis by echocardiography is the standard technique by which to confirm VHD, as well as determine disease severity and prognosis. Echocardiography evaluates valve structure and function (Bonow et al., 2006).
TREATMENT
There are no effective long-term medical therapies for severe VHD. Valve replacement or repair performed either surgically or by catheter intervention are the only effective therapies. Mortality risk with such intervention ranges from 1 to 20 percent and can be as high as 30 percent depending on circumstances, including the presence of other cardiac conditions, the skill of the surgeon, age of the patient, and the presence of a host of comorbidities including lung, kidney, and neurological disease.
DISABILITY
Approximately 8 million Americans have some form of VHD. Approximately 800,000 patients have valve disease that becomes serious enough to warrant some level of disability. Of those, roughly 80,000 a year undergo heart surgery to repair or replace defective valves.
Once it is determined that the patient has severe symptomatic VHD, the algorithm in Figure 12-1 should be used to determine disability. Aortic
stenosis is treated separately from the other lesions because symptomatic severe aortic stenosis is universally fatal if untreated (usually within 5 years or less of onset of symptoms) and is an automatic indication for disability unless aortic valve replacement is performed. Patients with this condition should not perform manual work, because it is possible that they could experience sudden death on the job.
CONCLUSIONS AND RECOMMENDATIONS
Severe symptomatic VHD leads to heart failure and death if left untreated and may be the cause of serious disability. Disability is determined on the basis of the presence of severe anatomic valve disease determined by echocardiography or other appropriate medical imaging and the symptoms caused by it. The committee concludes it is reasonable to provide disability at the listing level to symptomatic patients with severe valve disease, including aortic stenosis, mitral stenosis, aortic regurgitation, and mitral regurgitation.
Unlike other cardiac impairments, determining disability using measurements of functional criteria is not advised for symptomatic individuals with severe aortic stenosis, because there is risk to the patient in performing exercise tests. Furthermore, the severity of disease for patients with severe symptomatic aortic stenosis is sufficient to grant disability at the listing level without other indications of functional limitation, such as evidence of related heart failure.
RECOMMENDATION 12-1. Provide a listing-level pathway to disability for symptomatic claimants with objective evidence via echocardiogram or other appropriate medically acceptable imaging of severe aortic stenosis, characterized by mean gradient greater than 40 mm Hg, jet velocity greater than 4.0 m/sec, valve area less than 1.0 cm2, and valve area index less than 0.6 cm2/m2.
Severe mitral stenosis, aortic regurgitation, or mitral regurgitation may also warrant disability at the listing level, but these patients must demonstrate functional limitation in addition to an objective diagnosis of severity. Functional limitation may be demonstrated by repeated hospitalizations with heart failure, or an inability to achieve 5 metabolic equivalents of task on an exercise test, or objective evidence of right heart failure in the patient’s medical record. Individuals with moderate or mild valve disease may still be disabled by their impairment, however, but the committee agrees these impairments would not warrant disability at the listing level.
RECOMMENDATION 12-2. Provide a listing-level pathway to disability for symptomatic claimants with objective evidence via echocar-
diogram or other appropriate medically acceptable imaging of severe mitral stenosis, aortic regurgitation, or mitral regurgitation and demonstrated functional limitation. Objective evidence is measured by one of the following:
-
Severe mitral stenosis characterized by mean gradient greater than 10 mm Hg, pulmonary artery systolic pressure greater than 50 mm Hg, and valve area less than 1.0 cm2; or
-
Severe aortic regurgitation characterized by regurgitant volume greater than or equal to 60 ml/beat, and regurgitant orifice area greater than or equal to 50 cm2, and increased left ventricular size; or
-
Severe mitral regurgitation characterized by regurgitant volume greater than or equal to 60 ml/beat or regurgitant fraction greater than or equal to 50 percent, and regurgitant orifice area greater than or equal to 0.40 cm2, and enlarged left atrial size and enlarged left ventricular size.
Functional limitation(s) from severe mitral stenosis, aortic regurgitation, or mitral regurgitation would be demonstrated by one of the following:
-
Three hospitalizations with heart failure in 12 months; or
-
Inability to achieve 5 metabolic equivalents of task on an exercise test; or
-
Objective evidence of right heart failure.
Unlike many diseases such as chronic lung disease or certain cancers, treatment for VHD can have a dramatic improving effect on a patient’s functional status. For example, an individual may undergo medical testing revealing results that meet the recommended listing, but then receive treatment and on further testing, no longer meet the disability criteria at the listing level. The most common example of this scenario for VHD would be valve replacement or repair. An applicant with evidence of severe symptomatic valve disease may undergo surgery with complete resolution of symptoms and no functional limitations. Therefore, the committee concludes that any applicant applying for disability who has undergone valve surgery should be reassessed at a minimal duration of 3 months following the procedure, as the individual’s functional status may have changed significantly.
REFERENCE
Bonow, R. O., B. A. Carabello, K. Chatterjee, A. C. de Leon, D. P. Faxon, M. D. Freed, W. H. Gaasch, B. W. Lytle, R. A. Nishimura, P. T. O’Gara, R. A. O’Rourke, C. M. Otto, P. M. Shah, and J. S. Shanewise. 2006. ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Journal of the American College of Cardiology 48(3):e1–e148.








