
6
Conclusions and Recommendations
The committee believes child and adolescent health is important in and of itself—as a measure of a society’s values and capabilities—and as a direct determinant of subsequent productivity and later longevity. Timely, high-quality, readily accessible, and transparent information enables society to assess the impacts of programs and activities that may influence child and adolescent health. Such information enables society to compare the relative health of the nation’s young people and the youth of other nations, as well as specific subgroups of American youth—defined by geography, race, socioeconomic status, or other characteristics—so we can make the policy and program changes that can achieve national health and health care goals. Similarly, measurement of the quality of children’s health care enables society as a whole to understand the value of investments in health care services so as to make better decisions about these investments. Quality measures reveal which systems are functioning more or less effectively for which populations, again so we can improve the performance of those systems to achieve better short- and long-term outcomes, reduce suffering, advance safety, and achieve health equity.
Preceding chapters highlight the wealth of measures used to monitor the health status of children and adolescents and the quality of health care services they receive. Those chapters also point to the shortcomings and limitations of these measures and the challenges associated with integrating data sources and methods from diverse health and health care surveys and administrative records. While significant progress has been made, the nation has not yet balanced competing priorities and limited resources in developing measures that can support useful analyses of the extent to which
children and adolescents in the United States are healthy or are receiving high-quality health care.
In reviewing the findings presented in the preceding chapters of this report, the committee formulated three sets of conclusions. The first set focuses on the nature, scope, and quality of existing data sources with information about child and adolescent health and health care quality. The second set involves conclusions about gaps in measurement areas that provide opportunities for improving future data collection, analysis, and reporting efforts broadly. These gaps focus in particular on the social and behavioral determinants of health and health care quality and the importance of incorporating a life-course perspective in existing data sets. The third set includes conclusions related to gaps in methodological approaches that would benefit from future attention. These three sets of conclusions provide the foundation for the recommendations that follow, which are framed by a stepwise approach to measuring health and health care quality for children and adolescents.
The Nature, Scope, and Quality of Existing Data Sources
- Multiple and independent federal and state data sources exist that include measures of the health and health care quality of children and adolescents.
- The fragmentation of existing data sources impedes access to and timely use of the information they collectively provide.
- Existing data sources have their individual strengths and limitations, but no single data set derived from these sources provides robust information about the health status or health care quality of the general population of children and adolescents.
- Lack of standardization in the measurement of disparities in health and health care quality limits the ability to identify, monitor, and address persistent health disparities among children and adolescents. The use of standardized definitions and measures for disparities is especially important as the nation moves toward greater reliance on computer-generated forms and other electronic data sources. Lessons learned from the use of standard formats for classification of race and ethnicity data, as well as for self-identification responses by informants (or parents), can inform the standardization process.
- Common definitions and consistent data collection methods would improve the standardization of common data elements (such as
insurance coverage) across multiple settings, such as health care, education, and human services, in federal and state data sets. Coordination among current national and state-level data collection efforts and the creation of common data elements could reduce duplication and maximize the effective use of resources.
Gaps in Measurement Areas
The conclusions in this area focus on the social and behavioral determinants of health and health care quality. Multiple longitudinal studies document the impact of physical and social environments (e.g., toxic exposures, safe neighborhoods, or crowded housing), behaviors (e.g., diet or the use of alcohol or drugs), and relationships (e.g., parent-child attachment) on the health status of children and adolescents and their use of health care services. Earlier IOM/NRC reports have documented the extent to which such information is lacking in existing federal health and health care data sets, and stressed that these contextual factors are key influences on the short- and long-term health outcomes of children and adolescents.
- Existing goal-setting efforts in the public and private sectors offer a foundation from which to develop national goals for children and adolescents in priority areas of health and health care quality.
- Quality measures for preventive services deserve particular attention for children and adolescents because most individuals in these age groups are generally healthy and because early interventions may prevent the onset of serious health disorders as the child or adolescent becomes an adult. Preventive measures could direct attention to both the content of screening procedures and the rate of use of follow-up services that were recommended in response to the identification of risk factors.
- Standardized measures of child health and the quality of relevant health care are important for all child health problems, but especially for preventable, ongoing, or serious health conditions. Moreover, the implications of the existence of a health condition may vary with the age of the child or adolescent. As noted in Chapter 4, child health problems include a large number of relatively rare conditions, such as sickle cell disease, which occurs only among certain racial and ethnic groups of children and adolescents. Many federal data sets do not have a sufficient number of children with these specific conditions to offer detailed analyses in the quality of care. In other cases, developmental conditions may be a source of concern within specific age groups. For example, an early sign of a health problem may be slower rates of physical growth, but later
-
implications may include poorer school achievement, perhaps due to repeated absences (Byrd and Weitzman, 1994; Weitzman et al., 1982), or behavioral issues that may further impede school success (Gortmaker et al., 1990). Special health conditions may vary in severity across different children and over time and have implications for adult health.
- Variations persist in data elements pertaining to race, ethnicity, income, wealth, and education. Core data elements for socioeconomic status need to be identified that can feasibly be collected in a standardized manner, while introducing a life-course approach that can be applied across multiple data sets, especially those that collect information about early stages of development.
- The health of other family members, especially parents and other caregivers, may directly affect the health of children and adolescents, as well as their access to and use of health care services. Family-focused measures (e.g., the health conditions affecting parents, their employment status, and family and household structure) are a new frontier for research in the development of measures. Understanding the relationship between parental and child health will involve new forms of data collection that can be used to analyze mother child and father child health patterns. The linkage between maternal and child health is one of the most important areas to explore. Family-focused measures will also improve understanding of parent-child relationships that influence the need for, access to, and use of health care services.
- With respect to social determinants of health, data are needed to determine those elements that offer timely potential for prediction of disparities. Key items for consideration are information on socioeconomic status, including family structure and family income in relation to family size; educational, literacy, and language proficiency levels of parents/guardians; neighborhood conditions (including rates of violence and mobility, school density and status, and environmental quality); and economic hardships, such as housing insecurity or homelessness and food insecurity/hunger.
- Race/ethnicity, socioeconomic status, primary language spoken at home, and parental English proficiency all affect disparities in health and health care and therefore are relevant topics for data collection for all children and adolescents. Determining the conditions under which racial and ethnic characteristics are an accurate proxy for social influences on health and health care quality is a significant challenge.
- Measures of health literacy are important for adults’ ability to understand information that is relevant for children’s healthy de-
-
velopment and in ensuring adolescents’ understanding of their own health status. These measures reside on the margins of health measures and deserve greater recognition in the identification of future research priorities and the testing of new measures in national surveys.
- Biological influences on the health of children and adolescents are an important focus for measures of health and health care quality; also important are measures of behaviors and levels of functioning. Functional status measures, for example, offer opportunities to describe health across multiple conditions, with direct implications for service needs, patterns of use, and care effectiveness. Measures focused on the needs of the “whole child,” as opposed to individual clinical concerns, can address the distinct needs of children and adolescents, including their unique epidemiology, their dependent status, and their developmental stages. Functional status measures are one of the cornerstones recommended in Children’s Health, the Nation’s Wealth (IOM and NRC, 2004). Current child and adolescent health measures lack the capacity to capture important functional and developmental data; however, valid measures in these areas that have been tested across diverse populations do not yet exist. The inclusion of greater patient and family voice in the measurement of levels of functioning is an area that deserves particular attention.
- Measures of care transitions are important, especially for children with special health care needs. The creation and use of these measures would direct attention to episodes of care, as well as the design of consistent measures that can be used to follow children and adolescents over time across multiple care settings.
- New areas of focus entail place-based measurement, targeting selected geographic regions and population groups at the state, county, and even neighborhood levels. Place-based measurement for children’s health and health care quality may be strengthened by efforts that draw explicitly on strategies described in the IOM report Performance Measurement: Accelerating Improvement (IOM, 2006b).
Methodological Areas That Deserve Attention
- Many data sources cannot be used to assess the status of specific groups of children and youth, particularly vulnerable populations who are at risk of poor health outcomes because of their health conditions or social circumstances. Implementing an integrated ap-
proach involves determining specific criteria for selecting reference groups, such as the following:
- —age, gender, racial and ethnic characteristics, geographic location, and special health care needs;
- —social and economic features, such as household income and parental educational levels;
- —plan enrollment data at either a macro (i.e., public or private) or micro (i.e., Medicaid managed care or private point-of-service plan) level, length of plan enrollment, and eligibility criteria; and
- —selected health conditions (such as asthma or mental health disorders) and parental health status.
- The selection of reference group criteria would benefit from interactions with state and local health officials, as well as those concerned with the health and health care quality of children and adolescents in their region, particularly underserved populations. The selection of criteria could also be guided by the perspectives of both consumers and users, who may regard the relevance and timeliness of the data as highly important, and those involved in data collection, who may be more concerned with validity, reliability, and accuracy.
- Greater transparency is necessary to expose the strengths and limitations of different surveys in tracking the status of key child and adolescent populations of interest; in identifying appropriate reference groups over time; and in implementing innovative measurement practices that can adapt to changing conditions, changing populations, and opportunities for health improvement. Such transparency is challenging, especially in circumstances where the data pool may be extremely small because of rare conditions, few providers or care settings, or stigma association with certain conditions. Experience with the creation and use of performance measures associated with the cystic fibrosis registry (Richesson et al., 2009), for example, illustrates how such transparency could be developed while protecting individual rights to privacy and confidentiality.
- Linking or aggregating databases (combining data derived from multiple jurisdictions, institutions, and population subgroups or from different time periods) would reduce variations among multiple data sources and decrease the burden of data collection on individual states, providers, health plans, and households.
- —The time is ripe for developing collaborative efforts to improve the timeliness of data collection and the transparency of data sources in order to foster state and local efforts to improve health care quality. Such state and local efforts encourage col-
-
laboration; foster the use of population health and administrative data sets among health care providers and their institutions and other service settings; and support quality improvement practices.
- —In some cases, data aggregation efforts have involved the creation of registries to pool data on immunization coverage, as well as data on selected rare health conditions (such as cystic fibrosis or childhood cancers) that involve complex health care services. Such registries can be extremely valuable in comparing health outcomes (such as mortality or hospitalization rates) among different providers and health care settings and identifying opportunities to introduce best practices that could improve health outcomes.
- —Opportunities to create such registries may be available for other health conditions, such as sickle cell disease, HIV/AIDS, and mental health and behavioral disorders.
- While it is often difficult to connect data from the clinical records of children and adolescents enrolled in public health insurance plans to population health surveys and administrative data sets, such efforts will increase understanding of the social context and life-course influences that may affect children’s health status and their access to and use and quality of health care services (IOM and NRC, 2004, p. 135). The legal challenges presented by laws such as the Health Insurance Portability and Accountability Act (HIPAA) and the Family Educational Rights and Privacy Act of 1974 (FERPA) deserve appropriate remedies, but they should not be viewed as insurmountable for efforts to link multiple data sets. Efforts to promote data sharing within individual states using, for example, the Medicaid databases and vital statistics records, deserve encouragement and support.
- Longitudinal data (with multiple observations for the same children/families over time) would enrich the quality of measures used in population health surveys and health care quality studies. Such data are critical to understanding the long-term implications of interventions and health status measures during prenatal development, infancy, childhood, and adolescence, and their relationship to adult health outcomes within a life-course framework (NRC, 1998, p. 1). Incorporation of a life-course perspective into health care quality measures for children and adolescents deserves serious consideration in the creation and design of a comprehensive measurement system. Despite the inevitable challenges for measurement, the life-course perspective is key, creative, underutilized, and promising. The emerging science of fetal and early childhood
-
predictors of health outcomes lends particular importance to the need for longitudinal data sets. Incorporating this perspective could be achieved through longitudinal data sets that can follow population groups across multiple settings and across time to monitor the outcomes of preventive and early interventions, as well as the health consequences associated with early social environments.
- Electronic data capture and linkage would greatly enhance future measurement activity. Expanding data collection beyond geographic and claims information to capture state-level policy and community-level characteristics would enable analysis of the variability and impact of coverage, eligibility, and payment policies. Measurement efforts would be optimally useful if closely tied to current knowledge about specific functional health goals, meaningful use of health information technology, and established best practices for data extraction. Special attention will be needed to ensure that advances in electronic data capture adhere to existing privacy and confidentiality guidelines and laws. Ongoing attention will also be needed to resolve emerging issues related to privacy and confidentiality in future measurement efforts.
- While electronic health records have potential for significant retrieval of selected variables across multiple records, they do not necessarily offer conceptual or metric precision. The data are locked in a multitude of disparate systems designed for purposes other than analyses of health and health care quality.
A STEPWISE APPROACH TO MEASURING HEALTH AND HEALTH CARE QUALITY FOR CHILDREN AND ADOLESCENTS
The drivers for the creation and use of health and health care quality measures for younger populations are different from and lag far behind those for the development of quality measures for adult and elderly populations. The absence of strong private-sector incentives for the measurement of health care quality in younger populations, coupled with the compelling need to improve health care quality and population health outcomes for underserved children and adolescents, supports the need for a strong public presence in the design, collection, use, and reporting of such measures.
In reviewing early efforts and recent initiatives focused on improving health and health care quality measures for children and adolescents, the committee sought to build on the experience gained from earlier Institute of Medicine (IOM) health and health care quality studies (see Appendix C), legislative guidance, the Agency for Healthcare Research and Quality (AHRQ) core measures, efforts of the Centers for Medicaid and Medicare Services (CMS), and health care reform initiatives. Each of these efforts
offers guidance for identifying important areas for measurement, but they have significant limitations. First, the variations among them impede consensus on the priorities for future quality measurement strategies. Second, areas that are important to the health and health care quality of children and adolescents continue to lack valid and reliable measures, as was noted earlier in the review of the core set of measures for children’s health care quality recommended by the Secretary of Health and Human Services (HHS). Third, while many health care quality measures for children and adolescents (such as immunizations or safety procedures in administering medication) are comparable to those for the general adult population, others need to be adapted to the particular developmental needs of children and adolescents, which differ substantially from those of adults and may not be explicitly addressed in existing measures.
Federal agencies have made progress in addressing these shortcomings, such as the creation of an initial core group of standardized measures of quality of health care for children and adolescents. But the emphasis on using only valid, reliable, and feasible measures has resulted in neglecting the development of measures for important areas of health for which evidence is limited (such as mental health, substance use, oral health, and relatively rare chronic conditions), as well as for the content of and follow-up to preventive and early intervention services.
To address these shortcomings and limitations, the committee proposes a stepwise approach for improving measures of the health and health care quality of children and adolescents, based on the conclusions presented above. Strengthening the capacity of existing national and state-level data sets to provide routine guidance on areas of concern regarding the health and health care quality of children and adolescents could be achieved by improving the science as well as the use of measurement in five key areas that inform the steps in this approach. While the steps are proposed in a linear way, the committee recognizes that efforts may not adhere to this exact sequence, and back-and-forth movement may be necessary before the ultimate goal is achieved. The essential point is that each of the following steps is necessary in working toward a coherent system of measurement:
- Step 1—Set shared health and health care quality goals for all children and adolescents in the United States, especially those served by Medicaid and Children’s Health Insurance Program (CHIP) health plans.
- Step 2—Develop annual reports and standardized measures based on existing data sets of health and health care quality that can be collected and used to assess progress toward those goals. This step focuses on achieving comparability across federal and state data sources, aligning the selection of measures with goals and priority
-
needs, removing measures that are no longer necessary, and targeting measures to provide more insight into the nature and severity of health and health care disparities for underserved populations.
- Step 3—Create new measures and data sources in priority areas that can capture basic information about the behavioral and social conditions that exert profound influences on child and adolescent health and health care services.
- Step 4—Improve methods for data collection, reporting, and analysis in areas that are difficult to measure, linking existing data sets to make greater use of their contents and improving the timeliness of access to available data.
- Step 5—Improve public and private capacities to use and report data, drawing on existing data sources, as well as developing new federal−state and public−private partnerships to support special-population studies, the development and selection of measures, and the appropriate use of measures.
Figure 6-1 provides a graphic representation of the stepwise approach to measuring health and health care quality for children and adolescents. As depicted, the process is necessarily continuous and calls for evaluation of the measurement system itself in terms of transparency, accessibility, timeliness, quality, and feasibility. The entire approach is supported by research and evidence; survey, administrative, and medical records data; the health information infrastructure; and stakeholders.
The committee’s primary objective is to set in motion a process by which progress that has been achieved in identifying key domains for measuring the health of children and adolescents—by going beyond health conditions to assess health functioning, health potential, and health influences—can be incorporated into existing and future efforts to measure the quality of health care for these populations. The report Children’s Health, the Nation’s Wealth (IOM and NRC, 2004, p. 1) demonstrates that some valid and reliable measures already exist in each of these domains, and many take a life-course perspective, derived primarily from population health surveys. However, while rudimentary measures exist in some areas of functioning and the social determinants of health, significant work needs to be undertaken to develop consensus around the best available measures that do not yet meet key thresholds of validity or reliability, but offer significant promise in improving understanding of the social circumstances that influence children’s health and health care quality.
In addition, extensive work has begun to take advantage of emerging technologies and other data collection methods that can support the analysis of multiple variables from diverse data sources to provide more timely and accessible information about the health and quality of health
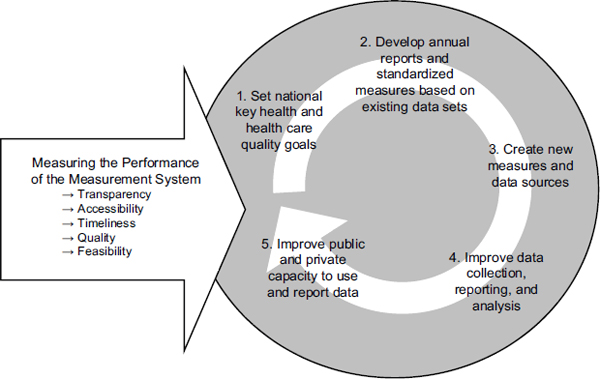
FIGURE 6-1 A stepwise approach to measuring health and health care quality for children and adolescents.
care for children and adolescents. Such efforts offer promise for informing the creation and selection of new measures, as well as the removal of comparatively inferior measures from administrative data sets as clinically rich electronic health records (EHRs) begin to emerge. Such electronic records hold the potential for identifying key relationships of interest that deserve consideration—such as those between health status and geographic location at different stages of development—provided such relationships can be established through the linkage of different data sources, the enhanced use of electronic data, or the development of new survey methods.
In the following sections, the committee offers recommendations for implementing each step of the proposed stepwise approach. In some areas, the committee offers specific guidance for implementing its recommendations, focusing in particular on those efforts that may be taken by the sponsors of this study, AHRQ and CMS. Box 6-1 provides a summary of key implementing actions for the committee’s recommendations.
Setting national and state-level goals for the health of children and adolescents would provide a structure within which to prioritize the next generation of health care quality measures, and would clarify the relative
BOX 6-1
Suggested Key Implementation Actions for the Committee’s Recommendations
Secretary of Health and Human Services (HHS)
- Undertake a series of convening efforts designed to standardize definitions of race, ethnicity, special health care needs, and socioeconomic status in data sets pertaining to children and adolescents.
- Stimulate a series of research initiatives in diverse agencies to encourage the creation of valid and reliable indicators of the primary language spoken at home and parental English proficiency.
- Establish priority areas for future measures of health care disparities.
HHS Data Council
- Routinely convene experts in public health, health care quality, and data sources associated with public and private health plans to identify opportunities for coordinated and integrated measures of preventive services for children and adolescents.
- Coordinate with HHS agencies to validate functional and developmental measures that can apply to chronic health conditions for children and adolescents in existing data sets.
- Support efforts to identify and reconcile sources of variation among different child health surveys and to build consensus on the reference groups that merit consistent attention.
Federal Interagency Forum on Child and Family Statistics
- Undertake a series of convening efforts designed to standardize definitions of race, ethnicity, special health care needs, and socioeconomic status in data sets pertaining to children and adolescents.
- Work with other federal agencies (such as the Departments of Education and Justice) to identify opportunities to support state and local efforts that link health data for children and adolescents with school performance and community safety indicators.
- Work with other federal agencies to develop strategies for integrating multiple data sets into a comprehensive data system capable of monitoring influences on children’s health outcomes.
- Work with other federal agencies to ensure that data on race/ethnicity, socioeconomic status, special health care needs, primary language spoken at home, and parental English proficiency are consistently collected in national and state surveys for all children and adolescents.
Agency for Healthcare Research and Quality (AHRQ) (in consultation with HHS)
- Identify priorities for future data aggregation efforts, and develop mechanisms to support these programs in public and private health care settings.
AHRQ and the Centers for Medicare and Medicaid Services (CMS)
- Assess current capacity to identify the social and economic status of children and adolescents in national and statewide data sources, and take steps to introduce associated measures where they are not available.
- Collaborate to support research and convening efforts focused on the development of measures that can be used to assess the content of basic preventive services associated with well-child visits, Early Periodic Screening, Diagnosis, and Treatment (EPSDT), and other preventive screens.
- Coordinate these efforts with evidence-based preventive services and programs for children and adolescents that are supported by other federal agencies.
- Conduct research on selected features of the families and neighborhoods of vulnerable populations of young people that exert significant influences on their health and health care quality.
- Introduce key measures for children and adolescents that capture such data as household income, levels of parental education, and family structure.
- Where feasible, introduce measures that can capture state-level policy and community characteristics.
- Develop guidelines to encourage greater transparency in monitoring the health outcomes (including mortality and morbidity rates) associated with the treatment of selected chronic conditions in different health settings and funded by different health plans.
- Convene a series of discussions with community leaders, educators, parents, and providers to explore approaches to linking diverse data sets through the use of unique identifiers while also protecting individual rights and respecting family privacy.
- Encourage collaboration with the National Health Information Network, the Key National Indicators Initiative, and related efforts to create community health maps and develop “smart targeting” techniques that focus on the status and particular needs of children enrolled in Medicaid and CHIP plans, as well as other vulnerable populations of children and adolescents.
- Convene state-based health plans to identify measures for key preventive health care strategies that could be incorporated into the core set of priority health care quality measures for children and adolescents.
roles of health care services and improvements in health care quality, as well as offer a basis for accountability, in achieving those goals. The goals could be derived as a set of critical objectives for children and adolescents from such sources as Healthy People 2010 and Healthy People 2020 for children and adolescents. They could also be reported as part of the annual national quality strategy and national prevention strategy reports prepared by the Secretary of HHS. In addition to specifying these goals, HHS agencies will need to establish lead agency roles in coordinating data linkage efforts. Questions to be resolved include the following:
- Should different agencies be responsible for health and health care data?
- Should health care services data be linked to efforts to improve quality and if so, at what level?
- Should different jurisdictions be encouraged or given incentives to coordinate and cooperate for efficiency in data coordination and linkage? How might this be achieved?
The answers to these questions will determine who has primary responsibility, and should be held accountable, for specific functions. Models to consider include designating a single agency with authority for coordinating multiple data sources, or, through interagency coordination efforts, building a robust data system with the capacity to collect information on important variables.
As discussed in Chapter 4, the committee built on earlier work that goes beyond the traditional focus on such indicators as morbidity, mortality, and chronic and acute conditions and identified seven priority areas to inform the setting of goals for health and health care quality for children and adolescents:
- childhood morbidity and mortality,
- chronic disease conditions,
- preventable common health conditions (especially mental and behavioral health and oral health),
- functional status,
- end-of-life conditions,
- health disparities, and
- social determinants of health.
These seven areas encompass the traditional measures of disease conditions, but also include new indicators of health and health care quality at the end of life and the social determinants of health. Pervading these seven
areas is the need for a life-course perspective that can be used to examine how each area applies to different stages of development for infants, toddlers, children in middle childhood, and adolescents. As noted earlier, the recent IOM report, Leading Health Indicators for Healthy People 2020, stressed the importance of life-course approach and concluded that “the life course approach provides a useful framework for viewing health determinants and their relative importance at different stages of life, and for guiding the development of targeted health policies, programs, and actions to improve health” (IOM, 2011b). This current committee reaffirms the importance of setting national goals within a life-course perspective to focus attention on the need to develop positive indicators of health and well-being for different age groups and encourage the development of conditions and services that support such positive outcomes.
Frieden (2010) and others have identified an array of strategies that contribute to improving health outcomes: individual counseling and education, clinical interventions, long-lasting protective interventions (such as immunizations), changes in the environmental context for individual decision making (such as the use of protective equipment), and strategies addressing socioeconomic factors that influence health status (such as reducing poverty or increasing educational achievement). For specific populations—for example, those with life-threatening conditions such as cystic fibrosis or cancer—high-quality clinical care is a direct determinant of health; for more general populations, the latter strategies, such as public health or legal interventions that reduce exposure to tobacco or improve social and economic well-being, may be stronger influences on health outcomes.
Recommendation 1: The Secretary of Health and Human Services (HHS) should convene an interagency group to establish national health and health care quality goals for children and adolescents within a life-course framework.
The absence of a specified set of national goals that can guide measurement of the health and health care quality of children and adolescents and inform the health care quality improvement activities of multiple agencies creates a situation in which multiple measures exist without a clear sense of importance, priority, or connectedness. Federal and state agencies need to achieve consensus on a set of goals that captures the areas most important to monitor and measure, regardless of the quality of data sources and methods currently available to support the assessment of performance in achieving those goals. Existing measures can then be mapped against the goals to highlight areas in which measures are already available and identify areas that are important to monitor but lack valid and reliable measures.
HHS agencies can then assess the degree to which their grant-making priorities and research initiatives align with the established health and health care quality goals for children and adolescents.
The above seven priority areas often overlap and cannot be considered in isolation; however, each presents unique measurement challenges and opportunities that merit separate consideration. Most of the existing health and health care quality measures for children and adolescents are focused on the first two areas and draw extensively on administrative data sets. However, important initiatives have emerged within a few data sources that provide opportunities to build new measures in the remaining five areas. These initiatives warrant increased support because of their capacity to inform the next generation of health care quality measures, as well as the emerging health information technology infrastructure. Population health data sources, in particular, offer valuable resources to support new health care quality measures that go beyond traditional measures associated with treatment for acute and chronic disease.
In addition to support for these initiatives, extensive collaboration will be required among multiple agencies and sectors, as well as other key stakeholders and consumers of the data, to develop the next generation of measures, especially in areas that involve disparities, social and behavioral determinants of health, and a life-course perspective. Interagency working groups and public–private collaborations will need to be formed and charged to develop action steps with defined timelines. Agency leaders will need to be designated to assume responsibility and accountability for developing measures and data sets that can address these gaps in a timely way.
Multiple public- and private-sector efforts are already under way to identify priority health and health care quality goals for children and adolescents, such as indicators included in Healthy People 2010 and 2020 (HHS, 2000a), the annual child well-being reports prepared by the Interagency Forum on Child and Family Statistics (FIFCFS, 2009), the Kids Count activities supported by the Annie E. Casey Foundation (Mather and Adams, 2006), and the annual Child Well-Being Index supported by the Foundation for Child Development (Land and FCD, 2010). These efforts draw on multiple data sources of varying quality and focus on different areas of interest. A national goal-setting effort for child and adolescent health and health care priorities could draw attention to those areas in which advances in the quality of health care services can contribute to improvements in health outcomes. This effort could also focus attention on opportunities for advances in public health or social policy to make important contributions.
STEP 2: DEVELOP ANNUAL REPORTS AND STANDARDIZED MEASURES BASED ON EXISTING DATA SETS
The goal-setting effort of Step 1 would highlight areas in which measurement of the quality of child and adolescent health and health care services is strong, as well as areas in which valid and reliable measures do not yet exist, areas that are difficult to measure, and populations that are difficult to reach. Step 2 focuses attention on the need to develop annual reports and standardized measures in the seven priority areas based on existing data sets, building on the multiple efforts of professional, public, and private-sector organizations.
While a large number of measures exist, efforts to monitor and improve the health and health care quality of children and adolescents are hampered by the absence of routine annual reports that focus on child and adolescent health and health care quality, as well as variations in both the measures themselves and the underlying data sources that support them. In the latter area, the committee has identified two issues of particular concern: (1) the absence of consistent measurement of disparities in health and health care quality to support the development of targeted interventions at the national and state levels, and (2) the retention of unnecessary or obsolete measures resulting from the adoption of standardized core measure sets over time, which can be addressed through a periodic review process.
Existing Opportunities to Include Children and Adolescents in Annual HHS Reports
The Secretary of HHS is already required to produce annual reports on health care quality and disparities (HHS, 2010a, 2010b), as well as annual reports on national prevention initiatives (HHS, 2011b; NPC, 2010). These reports provide valuable opportunities to include specific attention to children and adolescents and to draw attention to the ways in which their needs may different from those of older populations.
Standardized Measurement of Disparities in Health and Health Care
The changing demography of America’s youth increases the importance of recognizing and addressing pervasive disparities and inequities in child and adolescent health and health care. As with the measurement of health and health care quality, the measurement of disparities involves multiple dimensions and criteria. Though many studies measure disparities in terms of racial or ethnic differences, disparities also involve issues of gender, household income, educational status of the child or parent, insurance type, and medical practice setting (see Chapter 2).
Individual states are inconsistent in the way they classify race and ethnicity data in the Medicaid Statistics Information System (MSIS) (see Chapter 5). These inconsistencies highlight the importance of technical and methodological approaches that can reduce variation while allowing for individual choice. This issue is not unique to health and health care quality data for children and adolescents. Federal and state statistical systems would benefit from opportunities to exchange insight and experience in developing effective solutions. This is a recurrent theme throughout this report, as reflected in the committee’s recommendations and the suggested key implementation actions outlined below and summarized in Box 6-1.
The composition of population groups that are represented in existing data sets, as well as the methodological limitations of the survey measures and administrative data themselves, deserve significant attention. One study of Consumer Assessment of Healthcare Providers and Systems (CAHPS)like questions about patient experiences of care, for example, has called attention to variations in the applicability of the survey items to people with different cultural or other social traits (Morales et al., 2001). The absence of language diversity and the lack of rigorous methodological work on the cross-cultural validity of multiple survey measures are notable shortcomings in existing health care quality data sets. These shortcomings are especially evident in evaluating the patient-centeredness component of care, when parents are asked to assess their child’s general status, their satisfaction with the services their child has received, and/or the extent to which their child’s health needs have been adequately addressed.
Assessment of children’s and adolescents’ health will benefit from efforts to (1) adopt standardized definitions and measures of these characteristics, (2) routinely include socioeconomic information (minimally household income as an increment of the federal poverty level and educational attainment of parents), and (3) introduce data on language proficiency in existing data collection on the health and health care quality of children and adolescents. All these actions will be increasingly important in response to the growing poverty rates and increasing racial and ethnic heterogeneity of younger populations.
As noted earlier in this report, compared with U.S. adults, U.S. children and adolescents are disproportionately of nonwhite race/ethnicity, a fact of particular significance because poor and minority children have greater special health care needs than their nonpoor and white counterparts (Flores, 2010). Children and adolescents in these groups also are more frequently insured through public health plans. For example, more than 50 percent of African American and 48 percent of Latino children have public insurance such as Medicaid or CHIP (DeNavas-Walt et al., 2010). Thus the develop-
ment of health indicators that can provide a basis for considering the health status of these groups in relationship to the general population of children and adolescents is a particularly urgent need.
Recommendation 2a: The Secretary of HHS should include specific measures of the health and health care quality of children and adolescents in annual reports to Congress as part of the Secretary’s national quality and prevention strategy initiatives.
Recommendation 2b: These measures should include standardized definitions of race/ethnicity, socioeconomic status, and special health care needs, with the goal of identifying and eliminating disparities in health and health care quality within a life-course framework. Identifying and reducing disparities in health and health care will require collecting data on race/ethnicity, socioeconomic status, special health care needs, primary language spoken at home, and parental English proficiency for all children and adolescents.
Disparities in health and health care can be assessed by collecting data on race/ethnicity, socioeconomic status, special health care needs, primary language spoken at home, and parental English proficiency for all children and adolescents. Specific actions that could be taken to implement this recommendation include the following:
- All HHS agencies, especially AHRQ and CMS, could assess their current capacity to identify the social and economic status of children and adolescents in national and statewide data sources and take steps to introduce associated measures where they are not available.
- The Federal Interagency Forum on Child and Family Statistics could undertake a series of convening efforts to standardize definitions of race, ethnicity, special health care needs, and socioeconomic status in data sets pertaining to children and adolescents.
- The Federal Interagency Forum on Child and Family Statistics could work with other federal agencies to ensure that data on race/ethnicity, socioeconomic status, special health care needs, primary language spoken at home, and parental English proficiency are consistently collected in national and state surveys for all children and adolescents.
- The Secretary of HHS could stimulate a series of research initiatives within diverse agencies to encourage the creation of valid and reliable measures of the primary language spoken at home and parental English proficiency.
- The Secretary of HHS could establish priority areas for future measures of health care disparities, including disparities of health care access and utilization. Suggested areas include
- —prenatal care and neonatal development (i.e., prematurity and birth weight),
- —early childhood preventive care services and school readiness,
- —transitions from adolescence to young adulthood,
- —children with special health care needs (e.g., Down syndrome, cystic fibrosis),
- —oral health,
- —mental and behavioral health (including substance abuse), and
- —health care access and utilization.
A Periodic Review Process
As national health and health care quality goals change over time, certain measures or data sources may become obsolete or unnecessary, new data sources and measurement methods may emerge, and gaps may develop in areas that are important to monitor but difficult to measure. A process needs to be in place for conducting routine reviews of the recommended core set of standardized measures to identify those that are no longer appropriate for monitoring, those that support timely and reliable assessments of health and health care quality, and gaps that could benefit from investments in research to stimulate measurement in areas that are difficult to assess or for populations that are difficult to reach.
Standardization can produce measures with the potential to aid in robust comparative assessments across jurisdictions and time periods, but it often comes at a cost if lessons learned through the application of such measures are not shared with those involved in the development and selection of measures (McDonald, 2008). Standardization may result in the adoption of suboptimal measures at any given time based on the data sources available and the status of measure development. A periodic review process can help ensure that standardization does not result in the entrenchment of suboptimal measures (i.e., those that do not respond to changes in clinical evidence, understanding of the determinants of health, or measurement science). A periodic review process should include assessing each measure from the standardized core set to determine whether there is new evidence or information about the characteristics of the measure, its underlying data sources, or its application context (McDonald, 2008; Pancholi and Geppert, 2008), as well as to consider how it could incorporate features of new similar measures. The results of this assessment would provide a basis to revise, replace, or retire measures when justified. The evidence base for measures and associated data elements applicable to children and adoles-
cents is limited compared with that for the adult population (McDonald, 2009). As a result, new information is likely to emerge rapidly, making a continual learning environment for measures for children and adolescents even more important.
The committee tried to avoid wherever possible major new demands for state-level data collection beyond current capacities without identifying resources to support such efforts. In some cases, many states are already collecting, analyzing, and reporting important child health data, as noted in prior chapters. Strengthening these efforts while providing additional funding to those states without these capacities can make the improvement of national child and adolescent health data more feasible. States often are required to report important data in such areas as health events and service provision as a condition for receipt of federal funding. In such cases, standardization in data collection efforts (through the creation of common data elements) and in the format for reporting may be a feasible route to the goal of improving the quality of national statistics on child health and health care. In other cases, new surveys may be needed to complement existing efforts. Ultimately, the national goal should be focused on developing useful measures of health and health care quality that address the priorities and needs of the users of the data.
The periodic review process provides an opportunity to address effective and valid data collection approaches and to ensure that respondents (especially parents and adolescents) are clear about the meaning and intent of the questions being asked. This is an important concern as parents may feel they need to put the best face on their children’s health status. In the case of adolescents, many parents may honestly not know about all the sources of health care that their children have accessed. Important validation efforts are therefore needed as new concepts in such areas as care coordination, prevention, and medical homes assume a larger role in health care delivery.
Recommendation 3: The Secretary of HHS should develop a strategy for continuous improvement of the system for collecting, analyzing, and reporting health and health care quality measures for children and adolescents. This strategy should include periodic review of those measures that are used, recommended, or required by the federal government.
The AHRQ work on quality indicators initiated under the Evidence-based Practice Center Program is one example of this type of process that already exists at the federal level and could potentially be replicated for any standardized measures or measure sets. The development and maintenance of the AHRQ quality indicators are grounded in the methods of evidence-
based medicine, applied to measurement. Initially, AHRQ and Healthcare Cost and Utilization Project (HCUP) partners requested an evidence project to refine the original HCUP quality indicators. The motivation for this refinement was to meet the needs of those who were collecting the data and were working within their states to supply hospitals, legislators, policy makers, and the public at large with meaningful information based on the routinely collected administrative data sets available at the time.
As the program evolved, AHRQ initiated a support contract to ensure ongoing refinement of the indicators, including retirement of measures. Thus the guiding philosophy of the program is continuous quality improvement based on user experience and changes in medical evidence. In addition, the program includes expansions within domains and data sets initially covered, as well as expansions to new domains without ties to any particular data set to reflect new priorities in health care. Throughout the process, AHRQ and the quality indicator team have continued to innovate to expand measurement methods, always evaluating measures from initial assessment to implementation, followed by feedback and support throughout their life in the field. Documentation of the revision, replacement/expansion, and retirement of measures is available on a website (AHRQ, 2008) so that users of the measures have standard specifications but know that annual updates will reflect any new information.
STEP 3: CREATE NEW MEASURES AND DATA SOURCES IN PRIORITY AREAS
As noted above, most of the current health and health care quality measures for children and adolescents are focused on significant causes of mortality and morbidity and chronic health conditions (Beal et al., 2004). Among the seven priority areas, preventive services and the social determinants of health—using a life-course perspective—deserve particular emphasis in the development of measures of the health and quality of health care for children and adolescents.
Measures Addressing Preventive Services
The core set of measures for children’s health care quality recommended by the Secretary of HHS includes a strong emphasis on preventive services, but it lacks a similar emphasis in important areas that are particularly relevant for children and adolescents, such as oral health and mental and behavioral disorders. For example, dental caries are the leading cause of infectious disease among children and adolescents (HHS, 2000b). Likewise, in any given year, the percentage of young people with mental, emotional, or behavioral disorders is estimated to be between 14 and 20
percent (IOM, 2009c). Such disorders can include early drug or alcohol use or antisocial or aggressive behavior and violence that frequently emerge during childhood and adolescence. These disorders are included in selected data sources, but they frequently are omitted from national surveys. In addition, many children and adolescents in troubled circumstances (such as child welfare systems or juvenile detention centers) are not included in routine survey samples, and their family history or residential placements are not included in administrative records.
Recommendation 4: The Secretary of HHS should develop new measures of health and health care quality focused on preventive services with a life-course perspective. These measures should focus on common health conditions among children and adolescents, especially in the areas of oral health and mental and behavioral health, including substance abuse.
The new National Prevention Strategy mandated in the Affordable Care Act offers an opportunity to improve the quality of data sources with respect to the measurement of preventive services for children and adolescents. This effort would benefit from collaboration among multiple HHS agencies:
- AHRQ and CMS could provide collaborative support for research and convening efforts focused on the development of measures that can be used to assess the content of basic preventive services associated with well-child visits, early periodic screening, diagnosis, and treatment (EPSDT), and other preventive screens.
- AHRQ and CMS could coordinate these efforts with evidence-based preventive services and programs for children and adolescents that are supported by other federal agencies (such as the Healthy Start program supported by the Health Resources and Services Administration [HRSA] and selected public health screening efforts for sexually transmitted infections, underage drinking, and substance use).
- The HHS Data Council could routinely convene experts in public health, health care quality, and data sources associated with public and private health plans to identify opportunities for coordinated and integrated measures of preventive services for children and adolescents.
- AHRQ and CMS should convene state-based health plans to identify measures for key preventive health care strategies that could be incorporated into the core set of priority health care quality measures for children and adolescents.
- While the creation of consistent measures that can be used to assess health care quality for diverse populations deserves substantial attention, additional effort is necessary to develop a system that can foster the implementation and use of such measures. Recent legislative initiatives such as the Affordable Care Act and other federal efforts to support the development of health information technology offer substantial opportunities to foster the inclusion of children and adolescents in these efforts to build the next generation of data sources and data collection methods.
- Some aspects of these changes will likely support implementation of the approach proposed in this report aimed at improving quality measurement and outcomes for children. For example, increased emphasis on payment for outcomes and other value-based payment strategies will necessitate an increased investment in data collection and analysis, as well as the development of new quality metrics that correspond to the new service delivery structures, especially those that focus on preventive interventions for children and adolescents. Other aspects of these changes may impede progress toward the approach proposed by the committee. For example, increased use of bundled payments may reduce the amount or quality of administrative data available to measure care content and processes. These cross-currents reinforce the importance of measuring quality and outcomes for children for private payers, in addition to Medicaid and CHIP, and including measures at multiple levels of the health care system (e.g., the physician, plan, and accountable care organization [ACO] levels).
Measures Addressing Social and Behavioral Determinants of Health Using a Life-Course Perspective
While the need for improved measures of health care disparities and preventive services has already attracted attention, few data sources currently provide opportunities to incorporate new measures in such areas as the social and behavioral determinants of health or incorporate a life-course approach to measuring health functioning and health potential. Measures in these areas would facilitate important analyses and reporting on child and adolescent health and health care quality, and deserve special consideration given the dependent status of children and adolescents and the growing numbers who live in poor and low-income families. In generating the necessary measures and data sources in these areas, extensive collaboration among multiple public and private stakeholders will be necessary.
Recommendation 5: The Secretary of HHS should support interagency collaboration within HHS to develop measures, data sources, and reporting focused on relationships between the social determinants of health and the health and health care quality of children and adolescents.
Recommendation 6: The Secretary of HHS should encourage interagency collaboration within HHS to introduce a life-course perspective that strengthens the capacity of existing data sources to measure health conditions, levels of functioning, and health influences (including access to and quality of care) for children and adolescents.
Specific actions that could be taken to implement these recommendations include the following:
- The HHS Data Council could support efforts to identify and reconcile sources of variation among different child health surveys and to build consensus on the reference age, racial/ethnic, and socioeconomic groups that merit consistent attention.
- The HHS Data Council could coordinate with HHS agencies to validate functional and developmental measures that can apply to chronic health conditions for children and adolescents in existing data sets. This effort would involve testing similar measures of functional status across different health conditions and populations to establish thresholds and categories and to highlight key dimensions of functional status, including calibration of parental/youth reporting and intervention strategies. Such efforts might also include measures of family care and intergenerational care in existing survey efforts.
- AHRQ and CMS could collaborate with other HHS agencies (particularly HRSA and the Centers for Disease Control and Prevention [CDC]) to conduct research on selected features of the families and neighborhoods of vulnerable populations of young people that exert significant influences on their health and health care quality (such as family structure, rates of mobility, and violence).
- AHRQ and CMS could adopt key measures for children and adolescents that capture data in such areas as household income, levels of parental education, and family structure. Such measures already exist, for example, in population health databases such as the NSCH and NS-CSHCN, but have yet to be introduced in health care quality data sources.
- The effort to introduce social determinants into new and existing data sets in other federal agencies will require
- —identifying key aspects of socioeconomic status to be incorporated into data collection efforts,
- —prioritizing other factors as standard elements in data collection efforts, and
- —prioritizing the data sources to be modified to include these elements.
- Where feasible, AHRQ and CMS should introduce measures that can capture state-level policy and community characteristics. Such data will enable analysis of the variability and impact of coverage, eligibility, and payment policies, which may vary across multiple jurisdictions. This effort would benefit from additional investments in research design and survey instruments. Child and adolescent health status and health care quality may be directly influenced by the capacity of the health care resources within communities. Eligibility for and use of available services may also be affected by state and national criteria and regulations and their implementation.
- The Federal Interagency Forum on Child and Family Statistics could develop coordinated strategies for sharing results from longitudinal studies of children and adolescents with those who design and analyze population health and administrative data sets for these populations. The gaps between these separate efforts prevent the discovery of key data elements or relationships emerging from longitudinal studies that could strengthen the quality of data sources that rely on other methods. Longitudinal data focus attention on the sequence of conditions, experiences, and resources that influence child health outcomes. Infant mortality rates in certain regions, for example, may result not from the scarcity or low quality of neonatal facilities but from the absence of high-quality prenatal care for pregnant women, especially those who have difficulty navigating health care services because of limited English proficiency, changes in employment or family structure, or low health literacy. Placing more emphasis on achieving high-quality care in neonatal facilities may have a limited pay-off when the real problem resides in behavioral, educational, and social factors, such as legal restrictions on public health care services for undocumented immigrants.
- The HHS Secretary could stimulate the development of registries and other data aggregation strategies for rare but chronic conditions that affect many children and adolescents (such as cystic fibrosis and sickle cell disease). Such strategies will provide a basis for analyzing practices and disparities in hospital and ambulatory care settings and identifying opportunities for quality improvement.
Recommendation 7: The Secretary of HHS should place priority on interactions between HHS agencies and other federal agencies to strengthen the capacity to link data sources in areas related to behavioral health and the social determinants of health and health care quality.
In addition to the internal interagency collaboration with the U.S. Department of Health (as suggested in Recommendation 5), opportunities exist to foster integration of federal data sets that could link health and health care quality data to other child and adolescent outcomes, in areas such as education, employment, and public safety. These collaborative efforts would require interactions between HHS agencies and other federal departments. Specific actions that could be taken to implement this recommendation include the following:
- The HHS Data Council could work with other federal agencies (such as the Departments of Education and Justice) to identify opportunities to support state and local efforts that link health data for children and adolescents with school performance and community safety indicators, with special consideration of the challenges created by HIPAA and FERPA regulations.
- The Federal Interagency Forum on Child and Family Statistics could work with other federal agencies to develop strategies for integrating multiple data sets into a comprehensive data system capable of monitoring influences on children’s health outcomes, including
- —environmental indicators that inform analyses of interactions between health influences and child health conditions;
- —geographic indicators that facilitate comparisons of health and nonhealth factors linked across population health survey(s), claims data, administrative records, EHRs, and other data sources; and
- —encouragement for the inclusion of innovative measures in current population health surveys, such as diet, nutrition, and media exposure for children and adolescents, as well as other measures that respond to changing technologies and emerging health concerns.
STEP 4: IMPROVE DATA COLLECTION, REPORTING, AND ANALYSIS
The Importance of Data Aggregation and Transparency
Several strategies can be used to improve data sources and methods for data collection, reporting, and analysis: (1) data aggregation strategies, including the use of registries and data linkage opportunities; (2) the development of mechanisms to foster greater transparency of performance indicators; (3) the use of unique identifiers that allow analysts to link data on the same child from different administrative data sets to obtain a more robust profile of the characteristics of the child and his or her social context and health and educational outcomes (for an in-depth analysis of unique identifiers, see IOM, 2010b); and (4) greater use of longitudinal studies, which follow the same cohort of children over time to monitor their health conditions and the health care services they receive.
The importance of longitudinal measurement has been cited in multiple other studies (see, for example, the IOM report on performance measurement, IOM, 2006b, pp. 119–120). Longitudinal measurement fosters child-centered analysis, breaking down the divisions among data created by the different silos of the health care system and other service settings that engage the child and his or her family. Longitudinal measures are especially useful in monitoring care transitions, from hospital to ambulatory care, from primary care to other service settings, and from pediatric care to adult care settings (the times when breakdowns and errors in care are most likely to occur) (Coleman and Berenson, 2004). Longitudinal studies also enable assessment of whether the child’s or adolescent’s needs have been identified and met within an appropriate care setting. In addition, longitudinal measurement is necessary to determine both the short- and long-term outcomes of care, identifying intervening factors that may enhance or impede the effects of a high-quality health care system.
Creating opportunities to link data across multiple health care settings, as well as connecting health and health care data to education and human service data sources, will improve timeliness and foster greater transparency as to the multiple factors that affect the well-being of children and adolescents. Such efforts will require both methodological and technical advances and the resolution of concerns related to privacy and data sharing. Timely and transparent data sets can also help in explaining to participants the rationale for data collection efforts, including their purpose and the means by which the data will be used to assist their own and other children and adolescents nationwide. This understanding is key to ensuring that all segments of the population, including marginalized groups, will be fully represented in survey and administrative data sources. Patient advo-
cacy and other community-based organizations can play an outreach role in the community so that underrepresented populations will not interpret participation negatively.
Enhancing Timeliness: Moving Health and Health Care Quality Data into the Digital Age
The rationale for timeliness is obvious—information that lags or is collected only infrequently is of little value in informing program and policy decisions. Similarly, decision making is impaired by poor-quality data that reflect the health or quality of health care services for children and adolescents neither truthfully nor precisely. Transparency is necessary if the data are to be believable; otherwise, the data will not lead to action. Accessibility is critical as well if the data are to inform public discourse and lead to prompt action.
Linking data across multiple health care settings, as well as linking administrative records to education and human service data systems, will improve timeliness and foster greater transparency as to the multiple factors that affect the health and health care quality of children and adolescents.
Recommendation 8: The Secretary of HHS should identify significant opportunities to link data across health care, education, and human service settings, with the goal of improving timeliness and fostering greater transparency as to the multiple factors that affect the health of children and adolescents and the quality of services (including health care, educational, and social services) aimed at addressing those factors.
Recommendation 9: The Secretary of HHS should promote policy, research, and convening efforts that can facilitate linkages among digital data sets while also resolving legal and ethical concerns about privacy and data sharing.
Specific actions to be considered in implementing these recommendations include the following:
- The HHS Data Council, in consultation with various other HHS agencies, such as AHRQ, HRSA, CDC, and the National Center for Health Statistics (NCHS), could identify priorities for future data aggregation efforts and develop mechanisms to support these programs in public and private health care settings.
- AHRQ and CMS, in consultation with other HHS agencies, could develop guidelines to encourage greater transparency in monitoring the health outcomes (including mortality and morbidity rates)
-
associated with the treatment of selected chronic conditions in different health settings and funded by different health plans.
- CMS could expand and improve access to Medicaid data for quality measurement in child and adolescent health, including improving states’ access to encounter data (e.g., from the MSIS), resolving anomalies in state-level claims and enrollment records, and encouraging states to link to other databases (e.g., the National Vital Statistics System [NVSS]).
- Use of a unique identifier would facilitate aggregation of data and longitudinal studies, especially for children who are served in multiple public and private settings. Establishment of a system of unique identifiers would require cooperation across multiple institutions and providers of care. When a unique identifier is not available, statistical methods can be used for matching across data sets, but problems of duplication and undercoverage make this approach challenging. CMS has already developed unique identifiers for health records that are collected as part of the MSIS (see Chapter 5). The state-assigned identifier can be used consistently to identify a given individual across different years and different enrollment periods, making it possible to track Medicaid beneficiaries over time within the state. At present, however, it is not possible to track children and adolescents who move to different state jurisdictions. The MSIS has not been widely used for national reporting under CHIPRA, but HHS is now in the early stages of collecting and analyzing annual MSIS data within 6 months of state submission.
- AHRQ and CMS could develop a series of demonstration experiments involving the use of unique identifiers to foster life-course analyses and to strengthen the capacity to link records across multiple health care settings, as well as to link health data with sources of education and community safety data. Such experiments should build on innovative local and regional models that are already employing unique identifiers in data warehouses, such as the Kids Integrated Data Set (KIDS) initiative in Philadelphia and the Multi-State Foster Care Data Archive administered by the Chapin Hall Center for Children.
- AHRQ and CMS could convene a series of discussions with community leaders, educators, parents, and providers to explore solutions for linking diverse data sets through the use of unique identifiers while also protecting individual rights and respecting family privacy.
- AHRQ and CMS could encourage collaboration with the National Health Information Network, the Key National Indicators Initia-
tive, and related efforts to create community health maps and develop “smart targeting” techniques (seeking niche populations based on predetermined criteria) that focus on the status and particular needs of children enrolled in Medicaid and CHIP plans, as well as other vulnerable populations of children and adolescents.
STEP 5: IMPROVE PUBLIC AND PRIVATE CAPACITIES TO USE AND REPORT DATA
The conclusions presented earlier in this chapter emerged from the committee’s review of research studies on the measurement of health, health care quality, and health disparities for children and adolescents. These studies consistently demonstrate that improving measurement in these areas requires building capacities to use and report data at the federal and state levels. The emerging health information technology infrastructure offers an opportunity to emphasize the distinct needs of children and adolescents and to link those needs to family data in health information exchanges, for example, as well as to supplement traditional electronic information with data from other sources (including parents). These linked data sets could track children across public and private data sources, as well as link with public health data through birth certificates and newborn screening data sets.
Simply building more capacity will not suffice, however. It will also be important to develop an integrated approach that can aggregate and combine measures of the health status of children and adolescents (drawn from population health surveys) with measures of health care quality for those services that are actually used by children, adolescents, and their families. Additionally, measures are needed with which to compare the quality and utilization of services with the types and severity of children’s health needs due to chronic health disorders or risk factors that make them vulnerable to adverse health outcomes.
Efforts to build federal, state, and even local capacity for place-based measures can resolve some of the current difficulties of integrating health measures, measures of social context and other health influences, and health care quality measures focused on services within the health care setting. Such efforts will require innovative approaches to compiling and extracting data from existing surveys and databases. They will also require a conceptual framework that can prioritize and operationalize key measures of social context and health influences, as well as criteria that can be used to designate the appropriate reference groups of common interest. Some states are prepared to serve as laboratories for the creation of new measures for difficult-to-measure indicators or difficult-to-reach populations, and they would benefit from the development of incentives that would encourage voluntary compliance now.
At the same time, improving federal and state data collection capacity will not be sufficient to ensure that the data will lead to better child and adolescent health outcomes. Collaboration needs to be strengthened between those who collect the data and those who are expected to use the data to shape current and future interventions in health care and other service-based or community settings. Fostering this collaboration involves investing in the capacity of communities, states, providers, consumers, and others to use the data effectively to drive decision making in light of limited resources, as well as to monitor changes given the introduction of new policies or investments over time. Capacity for the use of data on health and health care quality also involves understanding the importance of tailoring interventions to the needs of different racial/ethnic, geographic, and other segments of the population and tracking longitudinally how disparities respond to changes in health care resources, processes, and policies.
Recommendation 10: The Secretary of HHS should establish a timetable for all states to report on a core set of standardized measures that can be used in the health information technology infrastructure to assess health and health care quality for children and adolescents. Congress and HHS should formulate alternative strategies (through incentive awards, demonstration grants, and technical assistance, for example) that would enable states to develop the necessary data sources and analyses to meet such requirements.
Progress has occurred within various data collection efforts on forming collaborations with the states and public−private partnerships that can foster the creation and use of health and health care quality measures addressing the particular needs of children and adolescents. However, much remains to be done, and federal leadership can provide guidance to establish policy regarding standard and minimum data elements, to create forums for consensus building, and to sponsor research in areas where new measures or existing measures could be tested with diverse reference groups. The report Children’s Health, the Nation’s Wealth (IOM and NRC, 2004) emphasizes the need for federal leadership in taking responsibility for measuring and monitoring the health of children and adolescents. That report also calls for the creation of a specific unit within HHS to address “development, coordination, standardization, and validation of data across the multiple HHS data collection agencies, to support state-level use of data, and to facilitate coordination across federal departments” (IOM and NRC, 2004, p. 6). To date, the problems associated with multiple data collection efforts across multiple federal agencies persist. While the creation of a high-level unit with responsibility and resources for tracking health data
on children and adolescents across multiple agencies remains elusive, some steps could be taken now to undertake the policy actions, convening efforts, and research initiatives described above.
Building capacity at the national, state, and local levels is critical to ensure the use of available indicators and performance measures.
- AHRQ could foster such capacity building by funding demonstration grants for the development and testing of national data linkage models incorporating content and communication standards that facilitate the aggregation of state- and agency-specific health and health care quality measures for children and adolescents. Ideally, these projects would assess the value of these linkages, the timeliness of data access, the usefulness of existing data sources, and opportunities to streamline redundant data collection efforts.
- State-level data are needed to monitor performance, accountability, and improvements in the health status and quality of care of children and adolescents. While states are routinely burdened with data collection requirements for numerous federal programs, they frequently lack the capacity to conduct their own analyses of state-level data sources. Some states have initiated innovative practices aimed at moving beyond traditional data silos, as described in Chapter 5.
- Also of value would be local-area studies addressing specific communities with unmet needs, particularly those that cut across state jurisdictions or that require analysis of selected demographic groups (such as children whose primary language at home is not English). Such studies would focus attention on selected reference groups that require more intensive and coordinated strategies because of their high rates of mobility, frequent turnover with multiple health plans, and high risk of poor health conditions. Data linkage and data “layering” strategies, such as those that have been demonstrated in Austin and Philadelphia (as described in Chapter 5), deserve further consideration and support as well.
The direction of policy and resources toward improving the health and health care quality of children and adolescents in recent years is an encouraging sign that the distinct needs of these populations are being recognized. Such efforts could build on the experience and expertise associated with measures of health and health care quality for adults, but they also need to recognize the unique needs of children and adolescents. Opportunities are available now to apply the conclusions and recommendations set forth
in this chapter to enhance the measures used in population health surveys and administrative data sources. Recognizing that individuals and organizations may disagree about the best means of achieving the essential intent of a particular recommendation, the committee proposes a national dialogue on the characteristics and key features of the recommendations themselves before the course by which they might be incorporated into public policy or private practice is charted.
Implementation of the recommendations presented in this chapter call for strong national and state-based leadership, as well as modest additional resources to go beyond traditional boundaries and incorporate data elements that can deepen our understanding of the complex interactions among health, health care quality, and the social determinants of health for children and adolescents. Innovations in electronic technologies and data gathering methods offer opportunities to create new measures that can inform our understanding of important health disparities, preventable health conditions, the social determinants of health, and a life-course approach to the assessment of health and health care quality for America’s children and adolescents.


































