2
The Co-Occurrence of Child
Maltreatment and Intimate
Partner Violence
A number of speakers in this workshop noted that violence against women and violence against children often occur together and share many common risk factors. For example, Mary Ellsberg, from the International Center for Research on Women, stated that “everything we know about family and community life would suggest that the two issues are intricately linked.”
Speakers estimated the prevalence of child maltreatment and intimate partner violence using statistics from research in the United States, as much of the most recent data on the intersection of child maltreatment and intimate partner violence has come from the United States. A recent study using a nationally representative sample of children up to age 17 found that children who had witnessed intimate partner violence in the previous 12 months were 3.88 times more likely to experience maltreatment during those 12 months than children who had not witnessed intimate partner violence (Hamby et al., 2010). An earlier study found that approximately 35 percent of children in the United States between the ages of 14 and 17 have been exposed to intimate partner violence and that 40 percent of all child abuse victims report violence in the home between their parents (Finkelhor et al., 2009). Although not every child who is exposed to intimate partner violence is also a victim of maltreatment, or vice versa, the data from the United States suggest a spectrum of violence that cannot be easily parsed into its separate components.
Several presenters and workshop participants commented that historically there has been a dearth of data from low- and middle-income countries and that this dearth has begun to be addressed only recently.
International statistics for the co-occurrence of child maltreatment and intimate partner violence that are comparable to those reported for the United States and Europe are scarce. Indeed, most of the prevalence and incidence data discussed during the workshop concerning violence against women and children in low- and middle-income countries address the two issues separately. Some speakers pointed to the World Report on Violence and Health published by the World Health Organization (WHO) as a source of international data on violence against children (Krug et al., 2002). In particular, workshop speaker Claudia García-Moreno noted that this study estimates that 21 percent of urban schoolchildren and 65 percent of rural schoolchildren in Ethiopia report bruises or swelling due to parental beatings. Dr. García-Moreno also cited data from the WHO Multi-Country Study on Women’s Health and Domestic Violence against Women, a study that she coordinated, which estimated the prevalence of intimate partner violence to be between 15 and 71 percent among women in the countries that were surveyed (García-Moreno et al., 2005). Although none of the workshop speakers cited international data focusing on the co-occurrence of violence against women and children, the sample statistics that were provided suggest the need for understanding and addressing violence within families rather than attempting to treat phenomena separately that are often associated with one another.
In addition to discussing the lack of data available from low- and middle-income countries, several speakers noted that efforts to understand and address violence against women are often artificially separated from similar efforts to understand and address violence against children. They noted that programming and funding often target specific populations (e.g., women but not children, or vice versa) rather than using an integrated approach that focuses on common risk factors. Concerns were also voiced about a lack of extant indicators that would allow researchers to collect data to measure the health and well-being of families as a whole, rather than breaking families down into component sub-groups of men, women, and children. Claire Crooks, from the Centre for Addiction and Mental Health, noted in her presentation that it is common practice to exclude from studies children who are exposed to more than one type of violence, as this polyvictimization is seen as a confounder. This presents an additional problem when women who are experiencing intimate partner violence are also perpetrating child maltreatment against their children. Dr. Crooks remarked that the complicated nature of violence within families results in very few programs and researchers “trying to understand the child and mother’s exposure to violence together and figure out how to measure that, how to intervene with that.”
A number of presenters spoke about efforts to address “family violence,” as an attempt to bridge the traditional divide between intimate
partner violence and child maltreatment. Workshop speaker Denise Wilson of the Auckland University of Technology noted that in New Zealand family violence is defined as all violence and abuse occurring in close personal relationships. This can include child abuse and neglect, elder abuse, child-to-parent violence, and sibling violence. Although this terminology is less specific than violence against women and children, it speaks to the interconnected nature of these two problems.
Another attempt to integrate these types of violence is through a multisectoral approach to violence prevention. One example of a multisectoral approach on a national level is the Family Violence Initiative in Canada. Workshop speaker David Butler-Jones, Chief Public Health Officer at the Public Health Agency of Canada, described the Family Violence Initiative as a federal-level collaboration among 15 departments. “It isn’t exclusively involved in departments federally,” he added. “It engages provinces and territories, NGOs [nongovernmental organizations], and others at the same time.”
THE CYCLE OF VIOLENCE
A central concept that underlies many of the discussions at the workshop is the cyclical nature of violence. The concept is particularly important in understanding the lifecourse implications as well as the intergenerational intersection of violence against women and children. In particular, workshop participants referred to the cycle of violence when describing the need to break down the silos that separate programming and funding for the prevention of violence against women from those for the prevention of violence against children. A number of speakers also referred to the cycle of violence in describing the implications of early exposure to violence, either directly or indirectly, throughout an individual’s life. These effects include intergenerational transmission, in which individuals who experienced violence as children subject their own children to violence either through direct means, such as maltreatment, or through indirect means, such as exposure to intimate partner violence.
Dr. Crooks provided a graphic (Figure 2-1) during her presentation that depicted the cycle of violence. The understanding of violence illustrated in that figure demonstrates how individuals who are exposed to violence during various periods in their lives may eventually expose their own children to violence, thus perpetuating the cycle. Dr. Crooks explained that an important point in the cycle of violence is when an individual who has experienced violence exposes his or her own children to violence, either through perpetration or through exposure to intimate partner violence. However, she stressed that there are multiple pathways by which an individual can arrive at the point of intergenerational transmission of violence and that factors related to violence exposure earlier in life can play a significant role.
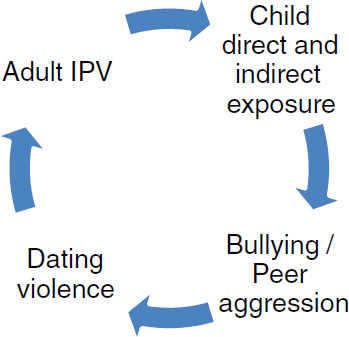
FIGURE 2-1 The cycle of violence.
SOURCE: Crooks, 2011.
A number of workshop participants stressed that although men are the primary perpetrators of violence against women and children, researchers and policy makers cannot ignore the fact that there are also women who abuse their children. Dr. Crooks also noted that not all children who are exposed to violence become perpetrators, although most perpetrators of violence were themselves victims of violence.
Dr. Crooks went on to describe a number of theories and frameworks that are important in understanding the psychosocial mechanisms behind the intergenerational transmission of violence. In particular, she highlighted contributions from the fields of attachment and social learning research. She explained that secure attachment is based on predictable, safe, and consistent caregiving. She further noted that attachment research has demonstrated the importance of very early relationship experiences, explaining that children can develop ideas, which they carry forward with them into adolescence and adulthood, about how safe the world is and about their place in relationships with others. Dr. Crooks commented that this can help to explain why people who experienced violence as children can grow up to do the same things to people in their adult lives.
Dr. Crooks also mentioned social learning theory, which explains that children learn unhealthy and coercive models about how to get their needs met when they are exposed to violence, either as witnesses or as direct victims. Children create models concerning effective strategies for various situations, and when they see that somebody’s needs can be met in the family through abuse and violence, they are more likely to adopt similar strategies
for getting their own needs met, rather than employing good communication and problem-solving skills. The Fourth R curriculum, described by David Wolfe from the Centre for Addiction and Mental Health, is an example of a program that seeks to reduce violence by teaching conflict-resolution and communication skills to middle-school and high-school students. Dr. Wolfe reported that an analysis of the data found that the additional risk of violent delinquency that is normally associated with childhood maltreatment was reduced for students in intervention schools. Additional information on this program can be found in Chapter 8.
Dr. Crooks explained that as behaviors develop, attitudes develop to match. This process can result in what she referred to as “hostile attribution bias.” For example, if an individual is living with violence, chaos, and trauma, that person learns to expect the very worst, and the worst-case scenario becomes the first thought because that is adaptive in dangerous situations. Even when that individual is in a safer environment, such as a school, it is difficult to suddenly disengage those adaptive behaviors. As a result, children with hostile attribution bias may interpret accidents, such as someone bumping into them, as attacks on their safety. They may eventually alienate their peers and be identified as aggressive by teachers. Dr. Crooks noted that this way of viewing the world can continue into adulthood and can contribute to the violence that is perpetrated against children by parents, who see their child’s behavior as hostile in nature.
Many speakers referred to individuals who have been victims of violence eventually exposing their own children to violence. One example of data that have been interpreted as illustrating the cycle of violence came from workshop presenter Gary Barker of both the International Center for Research on Women and Instituto Promundo. According to an initial analysis of data from the International Men and Gender Equality Survey (IMAGES), which were collected from both rural and urban areas in a number of countries, men who reported witnessing violence in their home of origin are nearly twice as likely as other men to report using violence against a female partner later in life (Barker et al., 2011). In addition to this added propensity for violence perpetration and exposure later in life, Dr. Ellsberg said, statistics from the Demographic and Health Surveys (DHS) show that there are also physical health consequences for children whose mothers experience intimate partner violence, such as an increased risk for malnutrition and higher mortality rates.
COMMON RISK FACTORS FOR CHILD MALTREATMENT
AND INTIMATE PARTNER VIOLENCE
Many workshop presenters noted that child maltreatment and intimate partner violence share a number of common risk factors. These comments
were often made in the context of discussions of efforts to prevent violence against women and children. As noted earlier, many participants challenged the wisdom of current violence prevention systems that maintain separate programming and funding streams for different target populations rather than making programming and funding decisions according to risk factors associated with various negative outcomes including violence against both women and children. As Dr. García-Moreno noted, “If we look at some of the risk factors for child maltreatment … there is quite some overlap with the [risk factors] that have been identified for intimate partner and sexual violence.”
Two key types of risk factors emerged during discussions: social determinants and individual factors. The WHO’s Commission on Social Determinants of Health describes social determinants as “the structural determinants and conditions of daily life” (Marmot et al., 2008). The participants of this workshop discussed a number of risk factors that are associated with the ways that governments and societies distribute resources. Hortensia Amaro, a workshop presenter from the Institute on Urban Health Research, remarked on the importance of “thinking about upstream factors across cultures and countries that are associated with toxic stress that children experience [and] are associated with highly strained communities and families.” That statement captured a sentiment expressed by many workshop participants that individuals who are exposed to violence within their families tend to live in families that are experiencing a number of stressors on multiple levels.
Many of the stressors that were noted result from economic conditions and resource allocation at local, national, regional, and sometimes global levels. Some risk factors mentioned in this category include inequitable education systems, unemployment, marginalization of vulnerable populations, and poverty. Dr Barker said that data from the IMAGES study indicates that although, in aggregate, men often have power over women because of social norms, “low-income men perceive themselves as not very powerful or powerless even as they may have and often have more power than their female partners.” Workshop presenter Rachel Jewkes, from the Medical Research Council of South Africa, offered a related remark. “Poorer men and women are likely to abuse and be victims,” she said. “But it may be a manifestation of experiences from childhood.” Her comment expressed a common sentiment—that risk factors, such as poverty, experienced in childhood are not only risk factors for childhood exposure to violence but also can carry through to adulthood and increase the risk of abuse and victimization.
Although many common risk factors are environmental in nature, a number of them are also somewhat more individual and have more to do with interactions among family and community members rather than macro-level systems. Most of these factors cannot be divorced from the
systems that affect them, but they may be considered more proximal to the individual who is either perpetrating violence or being victimized. For example, several workshop participants noted that untreated mental health conditions and substance abuse are strongly associated with violence exposure. Jacquelyn Campbell, co-chair of the forum, noted that the U.S. Human Resources and Services Administration (HRSA) has begun to incorporate intimate partner violence into its work on postpartum depression and depression during pregnancy interventions. Dr. Barker noted that data from the IMAGES study show that men’s reports of feeling stressed or depressed because of a perceived lack of sufficient income or work are more strongly associated with the men engaging in intimate partner violence than were their reports of actual household income or monthly income. This speaks to the intersection between systems factors that contribute to unemployment and poverty and individual factors, such as an individual’s ability to cope with stressful circumstances.
Although many workshop speakers spoke of psychosocial risk factors, a few participants also stressed recent advances in understanding of the biological mechanisms behind violence perpetration and the effects of violence exposure. Michael Phillips, a forum member and workshop participant from Shanghai Jiao Tong University, said, “There is a biological nature to impulsiveness, to alcoholism, to suicide, and to aggressiveness.” And Julian Ford, a workshop presenter from the University of Connecticut Health Center Child Trauma Clinic, described some of the physiological components to violence that are associated with trauma. In particular, he described how, in situations that are perceived by an individual as life-threatening, an “alarm goes off in the brain,” causing the brain to resort to a basic evaluation of safety. When this alarm has been triggered on a regular basis, the brain changes, creating a tendency to misperceive innocuous situations as dangerous, resulting in a fight-or-flight response, Dr. Ford said. “Violence, traumatic stress, life-threatening, life-changing experiences that are sudden, horrifying, overwhelming, these don’t just change a person’s frame of reference or way of thinking—they change their body.”
Another risk factor that is a combination of environmental and individual risk factors is gender socialization. This topic received a great deal of attention from several presenters and was the focus of the presentation by Dr. Jewkes. Gender socialization of children is, she said, “essentially a process of learning social expectations about appropriate goals and practices for men and boys and for women and girls and concomitant expectations and experiences of power.” She added that sources of socialization include social institutions, policies, and laws, as well as communities and families. Dr. Jewkes noted that violence within the home can be particularly harmful because it normalizes controlling and violent behaviors, which play a role in violence against both women and children.
Dr. Jewkes illustrated some of the effects of the coercive enforcement of gender norms with data from Julia Kim. Dr. Kim’s data indicate that a microfinance intervention for women combined with a structured curriculum focused on women’s empowerment decreased poverty and violence exposure, whereas the microfinance intervention alone had an effect on poverty but no effect on violence exposure. Data from the IMAGES study presented by Dr. Barker also spoke to the effects of gender norms. Those data indicate that men whose fathers engaged in domestic work when the men were growing up are more likely to engage in domestic work themselves once they become adults than men whose fathers did not engage in domestic work. Dr. Barker went on to explain that the significance of this finding, in terms of risk factors for violence against women and children, is that we can seek to help men change their behaviors in order to help them “pass on ways that show gender equality, respect for others, and nonviolence.”
PROGRAMS TAKING AN INTEGRATED APPROACH
A number of speakers at the workshop had been asked to speak about particular initiatives or programs with which they have been involved. A number of those participants provided more detailed descriptions of those programs in papers that are included in Chapter 8 of this summary. Some of the programs specifically target violence against women and children, whereas others focus on some of the risk factors that were listed above and are therefore likely to reduce violence exposure among both women and children.
Some of the programs described at the workshop can be characterized as having been developed originally with a focus on preventing violence against children but eventually having incorporated elements that address violence against women, or vice versa. A number of the programs that were discussed also focused on common risk factors that are known to contribute to violence against both women and children. Most commonly, these programs had a strong gender socialization component and targeted social norms. These interventions seem to speak to the value of addressing power dynamics and societal norms around violence when working to reduce violence in families.
High-Risk Domestic Violence Conferencing
Dr. Crooks described a new Canadian initiative that has been launched by the Children’s Aid Society in London, Ontario, to implement what they refer to as high-risk domestic violence conferencing. This is a significant development because the Children’s Aid Society has historically been an agency that has focused on child protective services, and it is now taking
the lead in organizing various individuals and organizations to provide support for high-risk cases. These conferences are designed to reduce multiple risk factors, including those that might increase the risk for the batterer to perpetrate violence in the future.
Parenting Training for Domestic Violence Workers
One workshop attendee discussed a curriculum that was developed to give training in parenting strategies to individuals who work in intimate partner violence programs. She explained that the goal is for these individuals, who are working with women who have experienced intimate partner violence, to learn to help support the parenting, attachment, and development capacities of women and children who are in intimate partner violence programs.
Strengthening Families Program
Workshop speaker Judy Langford, from the Center for Study of Social Policy, described the Strengthening Families Program, a program that is based on resilience research and seeks to reduce child maltreatment. In her discussion of the protective factors that are included in the program’s framework, she noted that several of the factors also address intimate partner violence. In particular, there is a focus on parental resilience, social connections, and having access to intensive services that a family might need when it is experiencing a crisis related to intimate partner violence, substance abuse, or untreated mental illness.
Parenting Program to Promote Couples’ Communication Skills
Agnes Tiwari from the University of Hong Kong described a program that was initially designed to address both intimate partner violence and child maltreatment, although plans are under way for a cluster randomized controlled trial that will evaluate the efficacy of the program in improving couple relationship quality, enhancing parental sense of competence, and reducing postnatal depressive symptoms. Of particular importance in this intervention was the ability of the team that developed the curriculum to adapt an established curriculum to meet the cultural needs of the target population in China. This program used parent education, which was designed to be very hands-on in order to encourage participation by the fathers as well as the mothers, as a way to train parents about infant care and reduce the risk of child maltreatment. Additionally, through discussions that were centered around infant care and child rearing, the program’s administrators were able to guide couples in improving their own communication skills and increasing their understanding of their own relationship styles.
Sexto Sentido and Bell Bajao
Workshop speaker Dr. Ellsberg described two initiatives that have been implemented in low- and middle-income countries, targeting permissive norms around the use of violence. Sexto Sentido, a television program, has become widely popular across Nicaragua. Storylines deal with issues of violence and risky behaviors, and characters model the benefits of having an open dialogue about the consequences of interpersonal violence and challenging accepted societal norms. In India, an organization called Breakthrough implemented the Bell Bajao campaign. The focus of this campaign was to challenge permissive social norms related to violence and to encourage people—especially men—to intervene when they see or hear violence being perpetrated.
Intervention with Microfinance for AIDS and Gender Equity (IMAGE)
On behalf of Julia Kim from the United Nations Development Programme, Dr. Jewkes discussed a microfinance program. In particular, she described a research study that looked at the effects of a microfinance intervention targeting women in a rural area of South Africa. Women in some towns received only the microfinance intervention, while women in other towns received the microfinance intervention as well as a women’s empowerment curriculum. Women who received both reported lower rates of poverty and fewer problems in their households during and after participation in the program. Women who received the microfinance alone experienced reductions in poverty but no change in household problems.
KEY MESSAGES
Although traditionally research in this area has focused on violence against women and violence against children as separate issues, more recently researchers and program designers are exploring ways of integrating the two. In particular, a greater understanding of the intergenerational transmission of violence could be beneficial in furthering the work in preventing both these types of violence. As research becomes more plentiful and shows a high correlation of child maltreatment and intimate partner violence, as well as a number of common risk factors, emerging evidence suggests that implementing programs that address both simultaneously could yield greater results.
REFERENCES
Barker, G., J. M. Contreras, B. Heilman, A. K. Singh, R. K. Verma, and M. Nascimento. 2011. Evolving men: Initial results from the International Men and Gender Equality Survey. Available at http://www.icrw.org/publications/evolving-men (accessed April 26, 2011).
Crooks, C. V. 2011. Cycles of violence. Presented at IOM Workshop on Preventing Violence Against Women and Children. Washington, DC: Institute of Medicine. January 28.
Finkelhor, D., H. Turner, R. Ormrod, and S. L. Hamby. 2009. Violence, abuse, and crime exposure in a national sample of children and youth. Pediatrics 124(5):1411-1423.
García-Moreno, C., C. Watts, M. Ellsberg, L. Heise, and H. A. F. M. Jansen. 2005. WHO Multi-country Study on Women’s Health and Domestic Violence against Women: Initial results on prevalence, health outcomes and women’s responses. Geneva, Switzerland: World Health Organization.
Hamby, S., D. Finkelhor, H. Turner, and R. Ormrod. 2010. The overlap of witnessing partner violence with child maltreatment and other victimizations in a nationally representative survey of youth. Child Abuse & Neglect 34(10):734-741.
Krug, E. G., J. A. Mercy, L. L. Dahlberg, and A. B. Zwi. 2002. World report on violence and health. Biomedica 22 (Suppl 2):327-336.
Marmot, M., S. Friel, R. Bell, T. A. J. Houweling, and S. Taylor. 2008. Closing the gap in a generation: Health equity through action on the social determinants of health. The Lancet 372(9650):1661-1669.