
Rapid access to antibiotics is critical for preventing and treating illness and death due to a bioterrorism attack with a bacterial agent such as Bacillus anthracis (anthrax). Yet the logistics of effectively delivering antibiotics to prevent anthrax infection pose a tremendous challenge because such an attack could potentially expose a large number of people who would require antibiotics within a relatively brief time window. For example, if aerosolized anthrax were released over a large, densely populated area, hundreds of thousands of people could need prophylactic antibiotics to prevent deadly inhalational anthrax (Danzig, 2003; U.S. Congress, 1993). The goal of current planning efforts is to be able to dispense prophylactic antibiotics to all exposed and potentially exposed individuals within 48 hours of the decision to dispense (CDC, 2011a). Although the nation has made much progress in developing plans for the delivery of antibiotics over the last decade, this public health goal continues to be recognized as difficult to achieve because of the challenges involved in implementing and executing these plans.
Given the challenges noted above, interest currently is focused on supplementing existing centralized strategies for the delivery of prophylactic antibiotics with so-called prepositioning strategies, whereby antibiotics are stored at or near locations in which they are anticipated to be needed. Accordingly, the Office of the Assistant Secretary for Preparedness and Response (ASPR), Department of Health and Human Services (HHS), com-
missioned the Institute of Medicine (IOM) to undertake a study that would inform the use of prepositioned antibiotics for the public for protection against an anthrax attack (Box 1-1).
To respond to this charge, the IOM appointed the Committee on Prepositioned Medical Countermeasures for the Public, bringing together 16 experts with a broad spectrum of expertise, including state and local public health preparedness, emergency medicine and response, infectious disease, pediatrics, toxicology, systems analysis and operations research, materials management and supply chains, economics, health systems, the
BOX 1-1
Statement of Task
In response to a request from the Department of Health and Human Services (HHS) Office of the Assistant Secretary for Preparedness and Response (ASPR), the Institute of Medicine will convene an ad hoc committee of subject matter experts to inform the use of prepositioned medical countermeasures (MCM) for the public. The committee will focus on prepositioning antibiotics for protection against a terrorist attack using Bacillus anthracis or a similar pathogen. More specifically, the ad hoc committee will produce a report that will:
• Consider the role of prepositioned medical countermeasures for the public (e.g., prepositioning at home, local stockpiles, and workplace caches) within an overall MCM dispensing strategy that includes traditional MCM dispensing and distribution strategies such as points of dispensing (PODs), taking into account both logistical and non-logistical factors (e.g., safety and ethics).
• Identify and describe key factors and variables that should be included in a strategy for prepositioning MCM for the public (e.g., population demographics, threat status, proximity to high-value targets, proximity to healthcare facilities).
• Discuss preliminary considerations for the development of an incremental and phased MCM prepositioning strategy.
• Based on available evidence, describe economic advantages and disadvantages of various MCM prepositioning strategies for the public.
The committee will develop scenarios, as needed, to illustrate the interaction of the strategic considerations, key factors, and variables in different situations and environments. The committee will base its recommendations on currently available published literature and other available guidance documents and evidence, expert testimony, as well as its expert judgment.
private sector, the social sciences, risk management and communication, bioethics, pharmacy, and faith and civic organizations. Biosketches of the committee members are included in Appendix E. The committee developed this report to assist federal policy makers and state, local, and tribal public health officials, as well as their private-sector and community partners, in evaluating the potential health benefits, health risks, costs, and practical considerations of implementing strategies for prepositioning antibiotics in their communities as a complement to existing, more centralized dispensing strategies.
In the fall of 2001, the United States experienced its first—and thus far only—bioterrorism attack involving B. anthracis, in which the bacterium spores were spread via mail sent through the U.S. postal system. These attacks resulted in 22 cases of documented anthrax; 11 of these cases were inhalational anthrax—the most deadly form of the disease—and resulted in 5 deaths (Jernigan et al., 2002).
Despite relatively limited experience with anthrax in the United States, it is considered one of the most serious threats to national security and the health of the nation for a variety of reasons, including the following:
• B. anthracis occurs in nature and is relatively inexpensive and easy to obtain and grow (CDC, 2009a; Inglesby et al., 2002).
• Inhalational anthrax can result from exposure to a relatively small number of spores and typically is lethal without effective treatment, and prophylaxis or treatment must be initiated within a relatively brief window of time following exposure (Inglesby et al., 2002; Turnbull, 2008).
• Although no nation publicly acknowledges having an offensive biological weapons program, it is estimated that a dozen countries have such programs (Kerr, 2008). The largest anthrax outbreak in history, the Sverdlovsk accident in 1979, is believed to have been the result of an accidental release of aerosolized anthrax from a Soviet Union biological weapons program (e.g., Meselson, 1988). There is also evidence that some terrorist groups have attempted to develop the capability to use anthrax, including the unsuccessful attempts by Japanese cult group Aum Shinrikyo to release anthrax in Tokyo in 1993 and evidence that Al Qaeda has pursued the development of anthrax as a biological weapon (Carus, 2002; Danzig et al., 2011; Mowatt-Larssen, 2010). The actual capability to conduct an attack using anthrax as a weapon is unknown for both national programs and terrorist groups.
• Among terrorist attacks, those involving anthrax may be among the easiest to carry out simultaneously in multiple locations or repeatedly over time (Danzig, 2003).
• Naturally occurring B. anthracis strains sometimes are resistant to certain antibiotics, and B. anthracis can be engineered to be resistant to multiple available antibiotics (Athamna et al., 2004; Brouillard et al., 2006; Inglesby et al., 2002; Price et al., 2003).
In 2004, the Secretary of the Department of Homeland Security (DHS) determined that anthrax presents a threat to the U.S. population of sufficient severity to affect national security (GAO, 2009). In 2006, the Secretary of DHS also determined that multi-drug-resistant anthrax was a material threat to the nation (DHS, 2008; GAO, 2009). The Centers for Disease Control and Prevention (CDC) classifies anthrax as a Category A bioterrorism agent/disease, a designation that indicates the greatest potential to adversely impact public health and result in mass casualties (CDC, 2011b; Rotz et al., 2002).
Concerns About the Current Dispensing System for Medical Countermeasures
All levels of government—federal, state, and local—and the private sector are involved in plans to distribute and dispense antibiotics to the public for protection against an anthrax attack. The backbone of current distribution plans is the Strategic National Stockpile (SNS), a national repository of medicine and medical supplies that can be deployed rapidly around the country to supplement state and local stockpiles (CDC, 2011c). Once medical countermeasures (MCM) from the SNS arrive, state and local public health authorities assume responsibility for distributing and dispensing them to their population.
Because of the scope of the challenge and the resources required, many public health authorities and other policy experts fear that most communities still lack adequate mechanisms and capacity to dispense antibiotics rapidly to all exposed and potentially exposed populations following a large anthrax attack (HSPD-21, 2007). This concern is driven by several factors, briefly outlined in the remainder of this section.
First, the anthrax attack of 2001 represents the nation’s only domestic experience with response to an anthrax attack; the available real-world evidence with which to assess the nation’s ability to dispense MCM following an anthrax attack is limited. Similarly, the number of exposed individuals in 2001 was small compared with estimates of the number of people who could potentially be exposed and infected in a large multicity aerosolized release of B. anthracis. Danzig (2003) predicts 200,000 expected infections
within a 40-mile radius of a small commercial sprayer from a single point source; DHS Planning Scenario 2 uses 328,484 infections from a concealed improvised spraying device in a densely populated urban city (DHS, 2006). Even though the scope of the attack in 2001 was much smaller than these estimates, the response to that event highlighted the challenges and time pressure associated with responding to anthrax and revealed “an unacceptable level of fragility in systems now properly recognized as vital to national defense” (Gursky et al., 2003, p. 97).
Second, there are sparse data from large-scale exercises and few measures of dispensing performance (not just planning), making it difficult to assess the system’s capacity to dispense antibiotics to all potentially exposed individuals within the required time window after a large attack. CDC and other entities have developed criteria and metrics with which to evaluate the development of state and local preparedness plans for the distribution and dispensing of MCM, including CDC’s Technical Assistance Review (TAR) tool and the recently published Public Health Preparedness Capabilities (CDC, 2009b, 2010, 2011d). However, there are few criteria and metrics with which to assess the actual implementation of dispensing plans (TFAH, 2010; Willis et al., 2009).
Third, concerns were fueled by the challenges encountered during efforts to dispense vaccine in response to the 2009 H1N1 influenza pandemic. Lessons learned from response to the influenza pandemic do not transfer directly to an anthrax response because of differences in geographic scope, time window for response, and required countermeasures. However, the distribution, dispensing, and communications challenges that occurred, particularly in the early months of the vaccine program, made concrete for many the immense difficulties of conducting a large antibiotic-dispensing campaign within a time window of approximately 48 hours, as would be required to respond to an anthrax attack (IOM, 2010a).
Finally, observation of responses to other, non-bioterrorism-related disasters have highlighted the tremendous challenges of responding to disasters. Recent examples include the earthquakes in Haiti and Japan and Hurricane Katrina. The aftermath of these disasters underscored the challenges of disaster response, the catastrophic consequences of gaps in preparedness, and the many areas in which improvements could be made. There is little evidence to suggest that mounting a mass MCM dispensing campaign after a major bioterrorism attack would not reveal challenges of a similar magnitude.
Prepositioning and Other Novel Dispensing Strategies
In response to the concerns outlined above, the past few years have seen a burgeoning interest in exploring novel dispensing strategies to complement
the existing system. In 2004, the U.S. Postal Service (USPS) began working with selected large cities to develop plans to use the postal service to distribute antibiotics to residents in their homes after an attack. Drills of the plan were conducted in Boston, Philadelphia, and Seattle in 2006 and 2007, and a pilot program of this model has been developed in Minneapolis-St. Paul (IOM, 2010b). A Presidential Executive Order issued in 2009 instructed the federal government to pursue the development of a national postal model in which postal carriers would distribute antibiotics to residents in their homes for self-administration (Obama, 2010). In response, a National Postal Model was developed by HHS, DHS, the Department of Defense, the Department of Justice, and the USPS (HHS et al., 2011).
Another strategy under exploration is user-managed inventory, in which materials are stockpiled in hospitals, to be used regularly for routine health care purposes and continually replaced to maintain the quantity of stockpiled materials but to avoid expiry (HHS, 2011). In addition, the response to the 2009 H1N1 influenza pandemic saw a great increase in private-sector mechanisms for dispensing of MCM, particularly via pharmacies and private practices (ASTHO, 2010; Merchant Medicine, 2010; ORISE, 2009).
As a supplement to established strategies, federal, state, and local public health authorities and the private sector also are interested in strategies that would preposition MCM closer to their intended users prior to an incident—the topic of the current report (see, for example, Kadlec [2011] for results of a survey of opinions on prepositioning among editors and readers of the journal DomPrep). Prepositioning strategies are being considered because they could potentially help ensure access to MCM for more people within an appropriate time window, decrease stress on the existing dispensing and health care systems, and help ensure fair and equitable access to MCM. Despite the promise of prepositioning strategies, however, prepositioning involves many complex issues that need to be carefully considered before decisions are made about the wide implementation of these strategies (IDSA, 2008; NBSB, 2008). These issues include questions about effectiveness, cost-effectiveness, logistics, the legal and regulatory framework, safety, equity, and sustainability.
Prepositioning and other novel dispensing strategies, as described above, are just one potential component of a larger endeavor to enhance the nation’s capability to prevent illness and death from an anthrax attack. Other components include national security efforts to prevent an attack or mitigate its effects, efforts to enhance detection and surveillance capability, further development of anthrax vaccine and antitoxin strategies, continuous refinement of the current MCM distribution and dispensing system, and efforts to engage the private sector in both the development and the delivery of MCM.
The committee’s work was accomplished over a 12-month period commencing in October 2010. The committee held four meetings between January and June 2011 that included both closed-session deliberations and open-session information-gathering dialogues with subject matter experts and stakeholders. The second committee meeting was held in conjunction with a 2-day public workshop whose objectives were to identify gaps and challenges in current dispensing systems; assess current prepositioning efforts; discuss a range of potential prepositioning strategies; examine ethical, legal, regulatory, and safety issues; and discuss methods, metrics, and available data for evaluating the cost and effectiveness of prepositioning strategies. A shorter open session also was held at the third committee meeting; this open session focused specifically on vulnerable populations, ethical issues, and public engagement. The agendas for both the workshop and the shorter open session are available in Appendix B. Box 1-2 presents a glossary of key terms used in this report.
In addition to the workshop and other information-gathering sessions, the committee surveyed the relevant peer-reviewed literature and other available guidance documents and publications, gathered information through personal contacts, and commissioned a paper on the economic costs and time savings associated with prepositioning strategies (Appendix D). During the study period, the committee also was able to garner relevant insights into public behavior relevant to MCM stockpiling in response to the earthquake, tsunami, and resulting nuclear disaster in Japan in March 2011.
The committee did not review any classified information, including classified information about the risk of an anthrax attack. The committee’s recommendations were informed by the members’ overall understanding of the threat and risk of anthrax today, 10 years after the 2001 anthrax attack. In its approach to this study and the formulation of its recommendations, however, the committee focused on how public health officials should use assessment of the current risk of an anthrax attack in their individual communities to inform decisions about prepositioning.
Strategies for positioning MCM lie along a continuum based on proximity to the location of the anticipated event. At one extreme, for example, MCM from the SNS and commercial stockpiles may be centrally located and distributed postevent to locations throughout the nation; at the other extreme, stockpiles are kept in individual homes for use immediately post-event. This continuum is depicted in Figure 1-1.
BOX 1-2
Glossary of Key Terms
Critical infrastructure personnel, first responders: For this report, the committee broadly defines critical infrastructure personnel and first responders as including those persons who will be expected to report to and stay at work during an attack in order to respond and maintain critical functions within the community. This definition is not meant to counter or supersede definitions of critical infrastructure personnel or first responders used by federal, state, and local planners.
Dispensing: The act of providing medical countermeasures (MCM) to individuals who will take them immediately or at some future defined/ declared time of need. Dispensing also includes providing MCM to heads of households or other nonmedical caregivers for use by those in their care.
Dispensing capacity: The number of individuals to whom a public health dispensing system can dispense MCM per day, whether the MCM are provided directly to individuals or via heads of households or other nonmedical caregivers.
Distribution: The delivery of MCM from stockpiles to receiving, staging, and storage (RSS) sites, as well as delivery from RSS sites to dispensing sites. Distribution may be triggered by an event, or MCM may be distributed to a local storage site or point of dispensing (POD) in anticipation of a potential future need.
Emergency Use Authorization (EUA): An authorization by the Commissioner of the Food and Drug Administration (FDA) for “the use of an unapproved medical product or an unapproved use of an approved medical product during a declared emergency involving a heightened risk of attack on the public or U.S. military forces, or a significant potential to affect national security” (FDA, 2010).
Jurisdiction, community: For this report, the committee uses jurisdiction to refer to state, local, and tribal governments. The committee uses community to refer to these governmental entities in conjunction with private-sector entities, community organizations, and members of the public within the jurisdictional boundaries.
Medical countermeasures (MCM): A drug, biological product, or device that diagnoses, mitigates, prevents, or treats harm resulting from a biological, chemical, radiological, or nuclear agent that causes a public health emergency (PAHPA, Public Law 109-417, Sec403a2(Aii), 2006).
Points of dispensing (PODS): Locations where MCM are dispensed to potentially exposed individuals. PODs may be open or closed, depending on the populations served:
• Open PODs: Locations where MCM are dispensed to all potentially exposed members of the public.
• Closed PODs: Locations where MCM are dispensed to a predefined population, such as employees of a company and their family members. Closed PODs may dispense MCM from a variety of sources, including the Strategic National Stockpile (SNS), state stockpiles, commercial supplies, and on-site workplace caches.
Prepositioning: The storage of MCM at or near the anticipated event location where they will be needed so as to reduce the time required to distribute and dispense initial doses. The placement of MCM lies on a continuum with respect to their physical proximity to the anticipated event location. Prepositioning refers to all potential placements of MCM along this continuum, from forward deployment of MCM through placement of stockpiles in the hands of individuals, as described below. Prepositioned MCM may remain in the control of federal, state, and local governments or may be managed by others, such as health systems, businesses, and individuals.
• Forward-Deployed MCM: MCM stored near the locations from which they will be dispensed.
• Cached MCMa: MCM stored at the locations from which they will be dispensed.
• Predispensed MCM: MCM stored by the intended users or by heads of households or other nonmedical caregivers for use by those in their care. Example strategies include personal stockpiles and MedKits:
— Personal Stockpile: MCM dispensed to individuals pre-event via normal prescribing routes for use during a public health emergency. Individuals may store the MCM in the home, workplace, or other personal location.
— MedKit: A medical kit containing prescription pharmaceuticals that is dispensed pre-event to families or individuals for use only as directed during a public health emergency.
– EUA MedKit: A medical kit allowed by the FDA for off-label use under conditions specified in an Emergency Use Authorization (EUA).
– FDA-approved MedKit: A medical kit approved by the FDA and labeled for use as a predispensed MCM. (Note that an FDA-approved MedKit does not currently exist.)
Prepositioning strategy: The specification of locations where MCM will be stored, and for each location, the amount of antibiotics stored and dispensing methods and protocols for their use in the event of a confirmed or suspected attack (e.g., for general use at public PODs, for use at a specific closed POD, for home use).
Public: All members of a community who are not already adequately covered by separate specialized programs, such as programs for federal mission-essential personnel.
Strategic National Stockpile (SNS): “A national repository of antibiotics, chemical antidotes, antitoxins, life-support medications, IV administration, airway maintenance supplies, and medical/surgical items. The SNS is designed to supplement and re-supply state and local public health agencies in the event of a national emergency anywhere and at anytime within the U.S. or its territories” (CDC, 2011c).
Subpopulation: “An identifiable fraction or subdivision of a population” (Merriam-Webster, 2011).
![]()
aThe term cache is often used broadly to describe stockpiles of MCM, whether held by state or local jurisdictions, healthcare facilities, private sector organizations, among others. For the purposes of this report, and to enable clear discussion of the different properties associated with different types of prepositioning, the committee defines cache more specifically as storage in the location from which they will be dispensed, and uses the term stockpile to cover federal, state, and local stockpiles.
Focus on Anthrax
ASPR asked the IOM committee to focus specifically on the dispensing of antibiotics for anthrax because (1) as noted above, the threat of anthrax currently is considered to be among the highest-priority threats; and (2) the brief time window within which antibiotics must be dispensed to protect effectively against anthrax infection is among the greatest challenges facing the MCM distribution and dispensing system as a whole. In accordance with the committee’s charge, then, the decision-aiding framework, analysis, findings, and recommendations presented in this report are specific to prepositioning of antibiotics for anthrax. The committee hopes that this report will provide a starting point and potential model for evaluating whether and how to preposition MCM to prevent, mitigate, and treat illness and death caused by other biological, chemical, and radiological/ nuclear threats. The committee cautions, however, that the analysis presented herein does not translate directly to such other situations because of differences in the nature of the threat, the time course of the threat, the time within which the MCM must be taken to be effective, and whether the MCM require administration by a health care professional. The find-
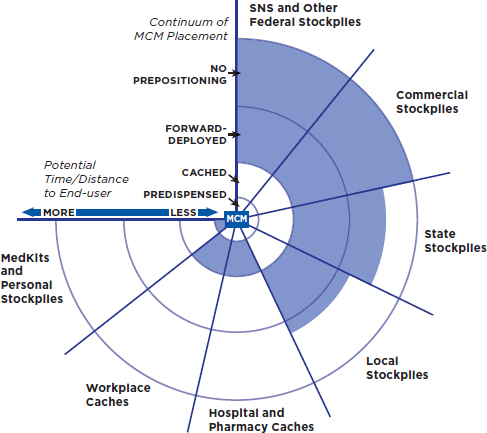
FIGURE 1-1
Strategies for positioning medical countermeasures: Centralized stockpiles distribute medical countermeasures (MCM) to a wider area but may take longer to reach people. Workplace caches and personal stockpiles may allow for more immediate access, but far more MCM are needed.
NOTE: The Strategic National Stockpile (SNS) and other entities may use a mix of placements along this continuum—for example, some forward-deployed stockpiles near areas of high risk combined with some centrally located stockpiles to serve remaining areas.
ings and recommendations presented here will be more closely applicable to other threats in which the characteristics of the threat and the associated MCM are similar to those for anthrax (e.g., another noncontagious disease with a similar time course that is prevented by an MCM that does not require administration by a health care professional). It is important to emphasize, however, that additional analysis will be needed for each threat and associated MCM.
The committee was asked to focus primarily on the response to an attack using a strain of anthrax that is susceptible to the antibiotics currently approved by the Food and Drug Administration (FDA) for anthrax prophylaxis. An attack using a strain of anthrax that is resistant to one or more antibiotics would, however, further challenge all aspects of current dispensing strategies because the majority of stockpiled antibiotics would be ineffective regardless of how early they were administered. In this event, jurisdictions and U.S. Government leaders would need to communicate with the public about alternative treatments, if any, and a massive surge of patients into the health care system would be difficult to avoid. The implications for prepositioning are discussed in more detail in Chapter 2.
Anthrax Vaccine and Anthrax Antitoxin
The committee recognizes two major issues that would significantly affect decisions about prepositioning: widespread use of anthrax vaccine, and the further development and stockpiling of anthrax antitoxin. These issues are briefly discussed here, but because the committee’s charge focused specifically on the distribution and dispensing of antibiotics, they were not a primary emphasis of its deliberations.
Widespread pre-event anthrax vaccination could potentially impact the selection and design of strategies for postexposure prophylaxis using antibiotics, including strategies for prepositioning the antibiotics, because it could decrease the size of the population needing postexposure prophylaxis with antibiotics. Currently, the use of anthrax vaccine adsorbed (AVA) is limited. CDC’s Advisory Committee on Immunization Practices has said that pre-exposure vaccination for emergency responders is not routinely recommended, but “may be offered on a voluntary basis under the direction of a comprehensive occupational health and safety program” (CDC/ACIP, 2010, p. 20). AVA is commercially available in certain travel clinics (Passport Health, 2010). Vaccination of potentially exposed people is recommended after an attack, in conjunction with a 60-day course of antibiotics (CDC/ACIP, 2010). However, pre-event vaccination is not recommended for the general public, and it is impractical for widespread use because it requires multiple initial doses followed by annual boosters (CDC, 2009c; CDC/ACIP, 2010; Roos, 2011).
The second issue is the development and stockpiling of anthrax antitoxin. Toxins produced by B. anthracis bacteria, not the bacteria themselves, cause death (Inglesby et al., 2002). Antibiotics kill the bacteria before they can produce lethal quantities of toxins but are unable to prevent death once the toxins, and the systemic damage they cause, accumulate. Anthrax antitoxin, on the other hand, functionally inhibits one or both of the toxins produced by anthrax, although debate remains as to whether the antitoxin would be as effective when given in a later (fulminant) stage of symptomatic disease, compared with early- or intermediate-stage symptomatic disease (FDA, 2009; Migone et al., 2009). The SNS stockpiles anthrax antitoxin, but not in a quantity sufficient to treat the population that could be exposed in a large anthrax attack, and the drug is not approved by the FDA for the treatment or prophylaxis of anthrax (FDA, 2011; HHS, 2010). In the future, should antitoxin be approved by the FDA and available in sufficient quantities, this MCM could assume a greater role in plans to protect the health of the potentially exposed population. The use of either vaccine or antitoxin also avoids concerns about antibiotic-resistant anthrax, discussed in Chapter 2.
Populations Considered
The committee defined the public to be all members of a community who are not already adequately covered by separate specialized programs, such as those for federal mission-essential personnel (Box 1-2). The committee was prompted to make this distinction because Section 4 of the Executive Order on providing MCM, issued in 2009, identifies federal mission-essential personnel as a specialized group whose work ensures the continuity of operations, and it mandates the specific provision of MCM to these individuals (Obama, 2010). State and local first responders and critical infrastructure personnel are not included in the Executive Order, since it focuses on federal mission-essential personnel. In its second information-gathering session (agenda included in Appendix B), the committee heard testimony about DHS’s internal plan to stockpile and dispense MCM to its employees around the country (Brinsfield, 2011). This information provided context for the committee’s definition of the public (Box 1-2). Some communities should take into account that federal mission-essential personnel stationed in their area will not be part of the public MCM dispensing system.
The committee’s interpretation of the term public in this report includes consideration of entities that are perhaps not perceived as part of the public, such as civic entities and corporations. The committee, however, found that it was impossible in practice, and potentially inadvisable, to draw clear lines separating the public from civic entities and corporations. For example,
most plans to dispense MCM to first responders also include sufficient quantities for their families, the latter being considered members of the general public. Similarly, employees of corporations are most likely to be considered members of the public, especially if they are not directly involved in emergency response activities (e.g., employees of large retail stores). Therefore, most plans to dispense MCM via civic entities or corporations would also entail dispensing to “the public” and, moreover, would impact the capacity needed to dispense MCM via more standard public strategies such as open points of dispensing (PODs). A major benefit of dispensing through corporations, for example, is alleviating the burden on public PODs by reaching concentrated populations who would otherwise use these traditional PODs. For this reason, the committee defined the public broadly as “all members of a community who are not already adequately covered by separate specialized programs, such as those for federal mission-essential personnel.” This usage recognizes the interrelated nature of all programs to dispense MCM within a community while avoiding interfering with any specialized dispensing programs that a jurisdiction may already have.
Additionally, the committee wishes to highlight the importance of giving specific attention to the needs of children and other vulnerable or at-risk populations, including those who, by virtue of socioeconomic status and/ or demographic characteristics, may be at systemically increased risk for lower access to disaster mitigation response. These populations would include, for example, people with low incomes/limited transportation, people with no or limited English proficiency, historically underserved ethnic/racial groups, people with disabilities (especially the vision impaired, hearing impaired, or mobility impaired), people who are homeless, and people who are homebound.
Limitations of the Data
During the course of this study, the committee noted gaps in the available evidence in three particular areas that are critical to its charge. These gaps are introduced briefly here because of their importance to the committee’s overall approach to the study; they are discussed in greater detail in subsequent chapters.
First, the committee found that reliable evidence on human inhalational anthrax, particularly on the incubation period and the relationship of dose to that period, is limited and uncertain. Data come from two primary sources: the accidental release in 1979 of B. anthracis spores from a military microbiology facility in Sverdlovsk, Union of Soviet Socialist Republics (now Yekaterinburg, Russia), and the anthrax attack in the United States in 2001 (Jernigan et al., 2002; Meselson et al., 1994). The committee’s review of the Sverdlovsk data revealed sufficient uncertainties and problems with
data quality to make the data of limited utility. The data and their implications for MCM distribution and dispensing, including prepositioning, are discussed in Chapter 2.
Second, knowledge is insufficient as to the period of time that would likely lapse between the release of anthrax spores and the start of dispensing of MCM. This period includes the time to detection and the time to decision. The former depends on how the attack is detected: environmental detection through a BioWatch sensor, for instance, could take a minimum of 24 hours, while clinical identification of a sick patient could occur days after the release as a result of both the incubation period of the bacteria and the time required for clinical recognition and definitive laboratory testing (Jernigan et al., 2002; Shea, 2003). No data exist to support predictions of the length of time that would lapse prior to the decision to dispense once detection had occurred; this period likely would be somewhat dependent on the U.S. government’s and the jurisdiction’s level of confidence that the detection was not a false positive.
Third, the committee found a dearth of data, and even sparser publicly available data from realistic exercises, on the performance and implementation of current state, local, and tribal dispensing plans. This lack of data made it difficult for the committee to identify gaps in the current system. In addition, the committee recognizes that tremendous variability exists in state and local dispensing plans and capabilities and in the specific characteristics and needs of communities across the nation.
Development of a Decision-Aiding Framework for State, Local, and Tribal Jurisdictions
Many factors associated with decision making vary significantly across communities, including the risk of attack, capabilities, resources, and current public health infrastructure. Therefore, the committee concluded that it would not be possible, or advisable, for it to prescribe a specific set of prepositioning strategies to complement the traditional POD system. Similarly, it was infeasible to attempt to categorize, identify, or address specific gaps present in individual communities across the nation. Instead, the committee has outlined a decision-aiding framework for jurisdictions to use in assessing their existing capabilities to meet the 48-hour goal for completion of MCM dispensing to the population. This approach is intended to provide state, local, and tribal jurisdictions with the framework and knowledge required to select and develop the most effective prepositioning strategies given their current capabilities and the specific needs of their communities.
In the report, the committee presents a qualitative exploration of the potential effects of each of the key elements of the decision-aiding framework on the incremental effectiveness of prepositioning strategies. The com-
mittee also presents a first-order quantitative model for estimating health benefits associated with different prepositioning strategies, a discussion and case study of the estimation of likely economic costs, and a suggested method for using estimates of health benefits and economic costs to explore trade-offs associated with alternative prepositioning strategies and thereby inform decision making.
Identification of Federal/National-Level Actions
Beyond a decision-aiding framework for individual jurisdictions, the committee’s recommendations identify federal/national-level actions that would facilitate the evaluation and development of prepositioning strategies. While all preparedness and response is ultimately local, the federal government has the unique ability to help coordinate regional and national dispensing strategies and provide resources, research, and technical expertise to enhance preparedness. Recognizing that implementation of the actions recommended by the committee should involve partnerships among all levels of government and nongovernmental stakeholders, the committee divides its recommendations into those aimed at the state/local/tribal level and those aimed at the federal/national level to indicate the entity or entities recommended to take the leading role, not the sole actor(s).
Chapter 2 provides an overview of the use of antibiotics for postexposure anthrax prophylaxis, with particular focus on the uncertainties associated with the time window within which antibiotics must be taken to prevent the deadly inhalational form of the disease. Chapter 3 gives an overview of current distribution and dispensing strategies for MCM for anthrax. Chapter 4 presents an overview of the three categories of prepositioning strategies for anthrax antibiotics: forward-deployed MCM, cached MCM, and predispensed MCM. These chapters provide the foundation for Chapter 5, which sets forth a decision-aiding framework to assist federal, state, and local policy makers and public health officials in evaluating the potential benefits and costs of implementing prepositioning strategies to complement existing dispensing strategies and to address specific gaps or overall capacity limitations. This framework encompasses the assessments that jurisdictions should perform to provide the evidence base to inform decision making about prepositioning, the need for ethical principles and public engagement, and a modeling approach that can be used to weigh health benefits and economic costs associated with the alternative prepositioning strategies. Chapter 5 also presents the committee’s findings and recommendations on the costs, benefits, and suitability of alternative prepositioning
strategies. Finally, Chapter 6 presents a summary of the recommended actions for moving forward that includes actions at the state, local, and tribal levels and at the federal/national level, as well as areas in which additional research is needed to provide a more solid evidence base to inform decisions about prepositioning strategies.
The report also includes five appendixes: Appendix A is a list of acronyms used in the report; Appendix B contains agendas for the committee’s public meetings; Appendix C presents a first-order model developed by the committee to estimate health outcomes for any prepositioning strategy; Appendix D is a paper commissioned for this study containing a cost and speed analysis of prepositioning strategies; and Appendix E provides biosketches of the committee members.
ASTHO (Association of State and Territorial Health Officials). 2010. Assessing policy barriers to effective public health response in the H1N1 influenza pandemic. Arlington, VA: ASTHO, http://www.astho.org/Display/AssetDisplay.aspx?id=4933 (accessed June 22, 2011).
Athamna, A., M. Athamna, N. Abu-Rashed, B. Medlej, D. J. Bast, and E. Rubenstein. 2004. Selection of Bacillus anthracis isolates resistant to antibiotics. Journal of Antimicrobial Chemotherapy 52(4):424-428.
Brinsfield, K. 2011 (February 28). Federal stakeholders’ perspectives: Department of Homeland Security. Remarks presented at the Institute of Medicine Public Workshop for the Committee on Prepositioned Medical Countermeasures for the Public, Washington, DC.
Brouillard, J. E., C. M. Terriff, and M. W. Garrison. 2006. Antibiotic selection and resistance issues with fluoroquinolones and doxycycline against bioterrorism agents. Pharmacotherapy 26(1):3-14.
Carus, W. S. 2002. Bioterrorism and biocrimes. The illicit use of biological agents since 1900. Washington, DC: National Defense University Center for Counterproliferation Research, http://www.dtic.mil/dtic/tr/fulltext/u2/a402108.pdf (accessed July 23, 2011).
CDC (Centers for Disease Control and Prevention). 2009a. Emergency preparedness and response: Anthrax and animal hide drums. Atlanta, GA: CDC, http://www.bt.cdc.gov/agent/anthrax/faq/pelt.asp (accessed June 24, 2011).
CDC. 2009b (April). Local technical assistance review. Atlanta, GA: CDC-SNS, www.odh.ohio.gov/ASSETS/.../LocalTARToolApril2009.pdf (accessed May 17, 2011).
CDC. 2009c. Emergency preparedness and response: Anthrax Q&A: Vaccination. Atlanta, GA: CDC, http://www.bt.cdc.gov/agent/anthrax/faq/vaccination.asp (accessed June 24, 2011).
CDC. 2010. Public health preparedness: Strengthening the nation’s emergency response state by state. Atlanta, GA: CDC, http://emergency.cdc.gov/publications/2010phprep/pdf/complete_PHPREP_report.pdf (accessed April 16, 2011).
CDC. 2011a. Cities Readiness Initiative (CRI). Atlanta, GA: CDC, http://www.bt.cdc.gov/cri/ (accessed April 14, 2011).
CDC. 2011b. Bioterrorism agents/diseases. Atlanta, GA: CDC, http://www.bt.cdc.gov/agent/agentlist-category.asp#a (accessed April 16, 2011).
CDC. 2011c. Strategic National Stockpile. Atlanta, GA: CDC-SNS, http://www.cdc.gov/phpr/ stockpile/stockpile.htm (accessed April 14, 2011).
CDC. 2011d. Public health preparedness capabilities: National standards for state and local planning. Atlanta, GA: CDC, http://www.cdc.gov/phpr/capabilities/Capabilities_March_2011.pdf (accessed April 16, 2011).
CDC/ACIP (CDC’s Advisory Committee on Immunization Practices). 2010. Use of anthrax vaccine in the United States: Recommendations of the Advisory Committee on Immunization Practices (ACIP), 2009. Morbidity and Mortality Weekly Report 59(RR-6):1-30. Danzig, R. 2003. Catastrophic bioterrorism: What is to be done? Washington, DC: National Defense University.
Danzig, R., M. Sageman, T. Leighton, L. Hough, H. Yuki, R. Kotani, and Z. M. Hosford. 2011. Aum Shinrikyo: Insights into how terrorists develop biological and chemical weapons. Washington, DC: Center for a New American Security.
DHS (Department of Homeland Security). 2006. National planning scenarios. Raleigh, NC: North Carolina Emergency Management Homeland Security Branch, https://secure.nccrimecontrol.org/hsb/planning/Planning%20Documents/National%20Planning%20Scenarios%202006.pdf (accessed August 11, 2011).
DHS. 2008. Letter from Michael Chertoff to Michael O. Leavitt on Determination Pursuant to ![]() 564 of the Federal Food, Drug, and Cosmetic Act. Washington, DC: DHS, http://www.dhs.gov/xlibrary/assets/ofsec_signed_determination092308.pdf (accessed July 10, 2011).
564 of the Federal Food, Drug, and Cosmetic Act. Washington, DC: DHS, http://www.dhs.gov/xlibrary/assets/ofsec_signed_determination092308.pdf (accessed July 10, 2011).
FDA (Food and Drug Administration). 2009 (October 27). Summary minutes of the anti-infectivedrugs advisory committee meeting. http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/Anti-InfectiveDrugsAdvisoryCommittee/UCM196436.pdf (accessed July 23, 2011).
FDA. 2010. Emergency Use Authorization of medical products: Guidance. Rockville, MD: FDA, http://www.fda.gov/RegulatoryInformation/Guidances/ucm125127.htm (accessed August 25, 2011).
FDA. 2011. Emergency preparedness bioterrorism and drug preparedness: Anthrax. Silver Spring, MD: FDA, http://www.fda.gov/Drugs/EmergencyPreparedness/BioterrorismandDrugPreparedness/ucm063485.htm (accessed June 24, 2011).
GAO (Government Accountability Office). 2009. Project BioShield Act: HHS has supported development, procurement, and emergency use of medical countermeasures to address health threats. Washington, DC: GAO, http://www.gao.gov/new.items/d09878r.pdf (accessed August 22, 2011).
Gursky, E., T. Inglesby, and T. O’Toole. 2003. Anthrax 2001: Observations on the medical and public health response. Biosecurity and Biodefense: Biodefense Strategy, Practice, and Science 1(2):97-110.
HHS (Department of Health and Human Services). 2010. Project Bioshield annual report to Congress: January 2009-December 2009. Washington, DC: HHS, https://www.medicalcountermeasures.gov/BARDA/documents/2009%20BioShield%20Report%20FINAL.pdf (accessed July 10, 2011).
HHS. 2011. Concept of operations: The virtual SNS or User-Managed Inventory (UMI). Washington, DC: HHS, http://www.phe.gov/Preparedness/planning/playbooks/rdd/Pages/conops.aspx (accessed June 22, 2011).
HHS, DHS, DOD (Department of Defense), DOJ (Department of Justice), and USPS (U.S. Postal Service). 2011. National Postal Model for the delivery of medical countermeasures.Washington, DC: HHS, http://www.phe.gov/Preparedness/planning/postal/Documents/eo13527-section2.pdf (accessed July 8, 2011).
HSPD-21 (Homeland Security Presidential Directive). 2007 (October 18). HSPD-21: Public health and medical preparedness. Washington, DC: White House, http://www.fas.org/irp/offdocs/nspd/hspd-21.htm (accessed June 24, 2011).
IDSA (Infectious Diseases Society of America). 2008. Preliminary statement of the Infectious Diseases Society of America on the U.S. Department of Health and Human Service’s proposed informational guidance on home stockpiling of doxycycline for anthrax. Arlington, VA: IDSA, www.idsociety.org/WorkArea/downloadasset.aspx?id=11572 (accessed November 2010).
Inglesby, T. V., T. O’Toole, D. A. Henderson, J. G. Bartlett, M. S. Ascher, E. Eitzen, A. M. Friedlander, J. Gerberding, J. Hauer, J. Hughes, J. McDade, M. T. Osterholm, G. Parker, T. M. Perl, P. K. Russell, K. Tonat; Working Group on Civilian Biodefense. 2002. Anthrax as a biological weapon, 2002: Updated recommendations for management. Journal of the American Medical Association 287(17):2236-2252.
IOM (Institute of Medicine). 2010a. The 2009 H1N1 vaccination campaign: Summary of a workshop series. Washington, DC: The National Academies Press.
IOM. 2010b. Medical countermeasures dispensing: Emergency use authorization and the postal model. Washington, DC: The National Academies Press.
Jernigan, D. B., P. L. Raghunathan, B. P. Bell, R. Brechner, E. A. Bresnitz, J. C. Butler, M. Cetron, M. Cohen, T. Doyle, M. Fischer, C. Greene, K. S. Griffith, J. Guarner, J. L. Hadler, J. A. Hayslett, R. Meyer, L. R. Petersen, M. Phillips, R. Pinner, T. Popovic, C. P. Quinn, J. Reefhuis, D. Reissman, N. Rosenstein, A. Schuchat, W. Shieh, L. Siegal, D. L. Swerdlow, F. C. Tenover, M. Traegar, J. W. Ward, I. Weisfuse, S. Wiersma, K. Yeskey, S. Zaki, D. A. Ashford, B. A. Perkins, S. Ostroff, J. Hughes, D. Fleming, J. P. Koplan, J. L. Gerberding, and the National Anthrax Epidemiologic Investigation Team. 2002 (October). Investigation of bioterrorism-related anthrax, United States, 2001: Epidemiologic findings. Emergency Infectious Diseases 8(10):1019-1028.
Kadlec, R. 2011 (January). DomPrep survey: Medical countermeasures for large-scale biological attacks. DomPrep Journal CBRNE Preparedness Biodefense-Medical Countermeasures Special Report, http://www.domesticpreparedness.com/userfiles/reports/MCMBIO2010.pdf (accessed February 24, 2011).
Kerr, P. K. 2008 (February 20). Nuclear, biological, and chemical weapons and missiles: Status and trends. Congressional Research Service Report for Congress, Order Code RL30699. Washington, DC: Library of Congress, http://www.fas.org/sgp/crs/nuke/RL30699.pdf (accessed June 24, 2011).
Merchant Medicine. 2010. Insight: The retail clinic market in 2009. Shoreview, MN:
Merchant Medicine, http://www.merchantmedicine.com/News.cfm?view=74 (accessed June 22, 2011).
Merriam-Webster. 2011. Online dictionary. http://www.merriam-webster.com/ (accessed August 18, 2011).
Meselson, M. 1988. The biological weapons convention and the Sverdlovsk anthrax outbreak of 1979. Journal of the Federation of American Scientists 41(7):1-6.
Meselson, M., J. Guillemin, M. Hugh-Jones, A. Langmiur, I. Popova, A. Shelokov, and O. Yampolskaya. 1994. The Sverdlovsk anthrax outbreak of 1979. Science 226(5188):1202-1208.
Migone, T. S., M. Subramanian, J. Zhong, L. M. Healy, A. Corey, M. Devalaraja, L. Lo, S. Ullrich, J. Zimmerman, A. Chen, M. Lewis, G. Meister, K. Gillum, D. Sanford, J. Mott, and S. Bolmer. 2009. Raxibacumab for the treatment of inhalational anthrax. New England Journal of Medicine 361(2):135-144.
Mowatt-Larssen, R. 2010. Al Qaeda weapons of mass destruction threat: Hype or reality? Cambridge, MA: Harvard Kennedy School, Belfer Center for Science and International Affairs, http://belfercenter.ksg.harvard.edu/files/al-qaeda-wmd-threat.pdf (accessed July 23, 2011).
NBSB (National Biodefense Science Board). 2008. Personal preparedness discussion: Excerpted from the Summary Report of the National Biodefense Science Board June 18, 2008. Washington, DC: NBSB, http://www.phe.gov/Preparedness/legal/boards/nbsb/Documents/nbsb-excrpt-pp-080618.pdf (accessed February 23, 2011).
Obama, B. 2010. Establishing federal capability for the timely provision of medical countermeasures following a biological attack. Executive Order 13527 of December 30, 2009. Federal Register 75(3):737-738, http://edocket.access.gpo.gov/2010/pdf/2010-38.pdf (accessed August 11, 2011).
ORISE (Oak Ridge Institute for Science and Education). 2009. Abbreviated pandemic influenza plan template for primary care provider offices: Guidance from stakeholders. Oak Ridge, TN: ORISE, http://www.cdc.gov/h1n1flu/guidance/pdf/abb_pandemic_influenza_plan.pdf (accessed June 22, 2011).
Passport Health. 2010. Anthrax. http://www.passporthealthusa.com/vaccines/home.anthrax.html (accessed July 23, 2011).
Price, L., A. Vogler, T. Pearson, J. Busch, J. Schupp, and P. Keim. 2003. In vitro selection and characterization of Bacillus anthracis mutants with high-level resistance to ciprofloxacin. Antimicrobial Agents Chemotherapy 47(7):2362-2365.
Roos, R. 2011 (July 28). Renewal of 2006 preparedness law advances in US House. http://www.cidrap.umn.edu/cidrap/content/bt/bioprep/news/jul2811bioshield.html (accessed August 15, 2011).
Rotz, L. D., A. S. Khan, S. R. Lillibridge, S. M. Ostroff, and J. M. Hughes. 2002. Public health assessment of potential bioterrorism agents. Emerging Infectious Diseases 8(2):225-230. Shea, D. A. 2003 (November 19). The BioWatch Program: Detection of bioterrorism. Congressional Research Service Report to Congress, Order Code RL 32152. Washington, DC: Library of Congress, http://www.fas.org/sgp/crs/terror/RL32152.html (accessed June 24, 2011).
TFAH (Trust for America’s Health). 2010. Ready or not 2010: Protecting the public’s health from diseases, disasters, and bioterrorism. Washington, DC: TFAH, http://healthyamericans.org/assets/files/TFAH2010ReadyorNot%20FINAL.pdf (accessed April 16, 2011).
Turnbull, P. C. 2008. Anthrax in humans and animals, 4th ed. Geneva, Switzerland: World Health Organization.
U.S. Congress. 1993. Proliferation of weapons of mass destruction: Assessing the risks. Office of Technology Assessment, OTA-ISC-559. Washington, DC: U.S. Congress, http://www.vaccines.mil/documents/library/proliferation.pdf (accessed August 30, 2011).
Willis, H. H., C. Nelson, S. Shelton, A. M. Parker, J. A. Zambrano, E. W. Chan, J. Wasserman, and B. A. Jackson. 2009. Initial evaluation of the Cities Readiness Initiative. Technical Report TR-640-CDC. Santa Monica, CA: RAND Corporation, http://www.rand.org/pubs/technical_reports/TR640.html (accessed February 16, 2011).




















