
Crisis Standards of Care
A Systems Framework for Catastrophic Disaster Response
Volume 5: Alternate Care Systems
Committee on Guidance for Establishing Standards of Care for Use in Disaster Situations
Board on Health Sciences Policy
Dan Hanfling, Bruce M. Altevogt, Kristin Viswanathan, and Lawrence O. Gostin, Editors
INSTITUTE OF MEDICINE
OF THE NATIONAL ACADEMIES
THE NATIONAL ACADEMIES PRESS
Washington, D.C.
|
THE NATIONAL ACADEMIES PRESS |
500 Fifth Street, NW |
Washington, DC 20001 |
NOTICE: The project that is the subject of this report was approved by the Governing Board of the National Research Council, whose members are drawn from the councils of the National Academy of Sciences, the National Academy of Engineering, and the Institute of Medicine. The members of the committee responsible for the report were chosen for their special competences and with regard for appropriate balance.
This study was supported by Contract No. HHSP23320042509XI between the National Academy of Sciences and the Department of Health and Human Services. Any opinions, findings, conclusions, or recommendations expressed in this publication are those of the author(s) and do not necessarily reflect the view of the organizations or agencies that provided support for this project.
Library of Congress Cataloging-in-Publication Data
Crisis standards of care : a systems framework for catastrophic disaster response / Committee on Guidance for Establishing Standards of Care for Use in Disaster Situations, Board on Health Sciences Policy ; Dan Hanfling … [et al.], editors.
p. ; cm.
Includes bibliographical references.
ISBN 978-0-309-25346-8 (hardcover) — ISBN 978-0-309-25347-5 (pdf) I. Hanfling, Dan.
II. Institute of Medicine (U.S.). Committee on Guidance for Establishing Standards of Care for Use in Disaster Situations.
[DNLM: 1. Disaster Medicine—standards—United States. 2. Emergency
Medical Services—standards—United States. 3. Emergency Treatment—
standards—United States. WA 295]
363.34—dc23
2012016602
Additional copies of this report are available from the National Academies Press, 500 Fifth Street, NW, Keck 360, Washington, DC 20001; (800) 624-6242 or (202) 334-3313; http://www.nap.edu.
For more information about the Institute of Medicine, visit the IOM home page at: www.iom.edu.
Copyright 2012 by the National Academy of Sciences. All rights reserved.
Printed in the United States of America
The serpent has been a symbol of long life, healing, and knowledge among almost all cultures and religions since the beginning of recorded history. The serpent adopted as a logotype by the Institute of Medicine is a relief carving from ancient Greece, now held by the Staatliche Museen in Berlin.
Suggested citation: IOM (Institute of Medicine). 2012. Crisis Standards of Care: A Systems Framework for Catastrophic Disaster Response. Washington, DC: The National Academies Press.
THE NATIONAL ACADEMIES
Advisers to the Nation on Science, Engineering, and Medicine
The National Academy of Sciences is a private, nonprofit, self-perpetuating society of distinguished scholars engaged in scientific and engineering research, dedicated to the furtherance of science and technology and to their use for the general welfare. Upon the authority of the charter granted to it by the Congress in 1863, the Academy has a mandate that requires it to advise the federal government on scientific and technical matters. Dr. Ralph J. Cicerone is president of the National Academy of Sciences.
The National Academy of Engineering was established in 1964, under the charter of the National Academy of Sciences, as a parallel organization of outstanding engineers. It is autonomous in its administration and in the selection of its members, sharing with the National Academy of Sciences the responsibility for advising the federal government. The National Academy of Engineering also sponsors engineering programs aimed at meeting national needs, encourages education and research, and recognizes the superior achievements of engineers. Dr. Charles M. Vest is president of the National Academy of Engineering.
The Institute of Medicine was established in 1970 by the National Academy of Sciences to secure the services of eminent members of appropriate professions in the examination of policy matters pertaining to the health of the public. The Institute acts under the responsibility given to the National Academy of Sciences by its congressional charter to be an adviser to the federal government and, upon its own initiative, to identify issues of medical care, research, and education. Dr. Harvey V. Fineberg is president of the Institute of Medicine.
The National Research Council was organized by the National Academy of Sciences in 1916 to associate the broad community of science and technology with the Academy’s purposes of furthering knowledge and advising the federal government. Functioning in accordance with general policies determined by the Academy, the Council has become the principal operating agency of both the National Academy of Sciences and the National Academy of Engineering in providing services to the government, the public, and the scientific and engineering communities. The Council is administered jointly by both Academies and the Institute of Medicine. Dr. Ralph J. Cicerone and Dr. Charles M. Vest are chair and vice chair, respectively, of the National Research Council.
COMMITTEE ON GUIDANCE FOR ESTABLISHING STANDARDS OF CARE FOR USE IN DISASTER SITUATIONS
LAWRENCE O. GOSTIN (Chair), O’Neill Institute for National and Global Health Law, Georgetown University Law Center, Washington, DC
DAN HANFLING (Vice-Chair), Inova Health System, Falls Church, VA
DAMON T. ARNOLD, Illinois Department of Public Health, Chicago (retired)
STEPHEN V. CANTRILL, Denver Health Medical Center, CO
BROOKE COURTNEY, Food and Drug Administration, Bethesda, MD
ASHA DEVEREAUX, California Thoracic Society, San Francisco, CA
EDWARD J. GABRIEL,* The Walt Disney Company, Burbank, CA
JOHN L. HICK, Hennepin County Medical Center, Minneapolis, MN
JAMES G. HODGE, JR., Center for the Study of Law, Science, and Technology, Arizona State University, Tempe
DONNA E. LEVIN, Massachusetts Department of Public Health, Boston
MARIANNE MATZO, University of Oklahoma Health Sciences Center, Oklahoma City
CHERYL A. PETERSON, American Nurses Association, Silver Spring, MD
TIA POWELL, Montefiore-Einstein Center for Bioethics, Albert Einstein College of Medicine, New York, NY
MERRITT SCHREIBER, University of California, Irvine, School of Medicine
UMAIR A. SHAH, Harris County Public Health and Environmental Services, Houston, TX
JOLENE R. WHITNEY, Bureau of Emergency Medical Services (EMS) and Preparedness, Utah Department of Health, Salt Lake City
Study Staff
BRUCE M. ALTEVOGT, Study Director
ANDREW M. POPE, Director, Board on Health Sciences Policy
CLARE STROUD, Program Officer
LORA TAYLOR, Senior Project Assistant (until January 2012)
ELIZABETH THOMAS, Senior Project Assistant (since February 2012)
KRISTIN VISWANATHAN, Research Associate
RONA BRIER, Editor
BARBARA FAIN, Consultant for Public Engagement
_________________
* Resigned from the committee October 2011.
Reviewers
This report has been reviewed in draft form by individuals chosen for their diverse perspectives and technical expertise, in accordance with procedures approved by the National Research Council’s Report Review Committee. The purpose of this independent review is to provide candid and critical comments that will assist the institution in making its published report as sound as possible and to ensure that the report meets institutional standards for objectivity, evidence, and responsiveness to the study charge. The review comments and draft manuscript remain confidential to protect the integrity of the deliberative process. We wish to thank the following individuals for their review of this report:
Richard Alcorta, Maryland Institute for Emergency Medical Services Systems
Knox Andress, Louisiana Poison Center
Connie Boatright-Royster, MESH Coalition
Susan Cooper, Tennessee Department of Health
Lance Gable, Wayne State University Center for Law and the Public’s Health
Carol Jacobson, Ohio Hospital Association
Amy Kaji, Harbor-UCLA Medical Center
Jon Krohmer, Department of Homeland Security
Onora Lien, King County Healthcare Coalition
Suzet McKinney, The Tauri Group
Peter Pons, Denver Health Medical Center
Clifford Rees, University of New Mexico School of Law
Linda Scott, Michigan Department of Community Health
Robert Ursano, Uniformed Services University School of Medicine
Lann Wilder, San Francisco General Hospital and Trauma Center
Matthew Wynia, American Medical Association
Although the reviewers listed above have provided many constructive comments and suggestions, they were not asked to endorse the conclusions or recommendations nor did they see the final draft of the report before
its release. The review of this report was overseen by Dr. Georges Benjamin, American Public Health Association. Appointed by the Institute of Medicine, he was responsible for making certain that an independent examination of this report was carried out in accordance with institutional procedures and that all review comments were carefully considered. Responsibility for the final content of this report rests entirely with the authoring committee and the institution.
Contents
VOLUME 1: INTRODUCTION AND CSC FRAMEWORK
2 Catastrophic Disaster Response: Creating a Framework for Medical Care Delivery
4 Cross-Cutting Themes: Ethics, Palliative Care, and Mental Health
VOLUME 2: STATE AND LOCAL GOVERNMENT
6 Prehospital Care: Emergency Medical Services (EMS)
7 Hospitals and Acute Care Facilities
VOLUME 5: ALTERNATE CARE SYSTEMS
8 Out-of-Hospital and Alternate Care Systems
Roles and Responsibilities of Out-of-Hospital and Alternate Care Systems
| ACS | Alternate Care System |
| CDC | Centers for Disease Control and Prevention |
| CSC | crisis standards of care |
| DMAC | disaster medical advisory committee |
| EMS | emergency medical services |
| EOC | emergency operations center |
| ESAR-VHP | Emergency System for Advance Registration of Volunteer Health Professionals |
| ESF | Emergency Support Function |
| FEMA | Federal Emergency Management Agency |
| HHS | Department of Health and Human Services |
| HICS | hospital incident command system |
| ICS | incident command system |
| JIS | joint information system |
| MAC | multiagency coordination |
| MOU | memorandum of understanding |
| MRC | Medical Reserve Corps |
| NDMS | National Disaster Medical System |
| NIMS | National Incident Management System |
Volume 5 8: Out-of-Hospital and Alternate Care Systems
Although much of disaster and surge capacity planning focuses on hospital-based care, approximately 89 percent of health care is delivered in outpatient settings. Of an estimated 1.2 billion outpatient visits in 2007, fewer than 17 percent were to emergency departments or hospital-associated clinics (Schappert and Rechtsteiner, 2011); total hospitalizations were 34.4 million in the same year (Hall et al., 2010). Especially during an epidemic, failure to leverage outpatient resources may result in catastrophic overload of inpatient and hospital-affiliated resources (Sills et al., 2011). For this reason, efforts to improve the integration of outpatient care assets into disaster response are critical, not only to improve the provision of crisis care but also to avoid crisis care. Current federal, state, and local disaster planning efforts have focused on integrating the hospital system and public health agencies. Following recent mass evacuations of residential care facilities (for hurricanes and fires), increased attention has been paid to outpatient nursing and long-term care units; however, individual and small-group practice settings have received little attention or integration into broader disaster planning efforts.
The value of the outpatient sector—its diversity—is also its challenge; the numbers and types of clinics and providers in a given area (in addition to long-term care, outpatient surgery, and other medical facilities) hamper detailed coordinated planning. Some outpatient facilities may be part of larger health care systems and thus much more able to coordinate information and develop policies that are consistent with a larger community response. Some may be community health centers—publicly funded entities with more than 8,000 sites across the nation. Those that are federally funded through the Department of Health and Human Services (HHS) recently have been required to improve their level of disaster preparedness. Such publicly funded clinics and programs benefit from the fact that they often serve at-risk populations with publicly employed providers, and provide an established mechanism and chain of command for clinical policy development, expertise, and medical direction that can be leveraged in public health emergencies. However, most facilities are independent group and solo private practices that may have no connection to local disaster planning and indeed, may not have a disaster or surge capacity plan at all. The ability of local public health or other government response agencies to engage all of these providers and clinics is compromised by their heterogeneity and the lack of available personnel, time, and funding. This gap in disaster preparedness is a potential barrier that can undermine the delivery of crisis care in mass casualty incidents such as a pandemic.
This chapter focuses on the need to include outpatient facilities and providers in disaster response to
maximize a community’s available resources. It describes the roles and responsibilities of the outpatient sector in a disaster response and the operational considerations associated with incorporating these facilities and providers into local and regional response. Although the chapter is not designed to be an operational guide for selection or operation of these facilities, it enumerates the functions and tasks required of outpatient facilities and providers to plan for and respond to a disaster. The template at the end of the chapter provides further detail on these functions and tasks for each type of outpatient care entity. While emergency medical services (EMS) may contribute to some of these strategies, their role in disaster response is addressed separately in Chapter 6.
ROLES AND RESPONSIBILITIES OF OUT-OF-HOSPITAL AND ALTERNATE CARE SYSTEMS
Disaster outpatient care—particularly the use of alternate care systems (hotlines, alternate care sites)—has been a gray area where public health and health care responsibilities frequently overlap. The result often has been less than optimal planning, with public health entities unwilling or unable to take responsibility for coordinating the care of ill or injured patients, and private health care systems unwilling or unable to take responsibility for setting up alternate care sites that would be established in unregulated facilities and therefore not within their current regulatory standards. Preincident discussion and strategizing between the two sectors are critical to a successful disaster response. Public health entities cannot simply “assign” private health care to develop outpatient surge capacity, and private health care cannot assume that public health can provide the clinical leadership or resources (especially medical providers) needed to establish effective alternate care systems. The two have a joint responsibility and distinct but equally necessary roles in efforts to advance planning for outpatient care under crisis standards of care (CSC) conditions to ensure that health care goals during a disaster can be accomplished through coordinated efforts. The coordination of these efforts can be facilitated through public health agencies and health care coalitions. Table 8-1 provides a sampling of the respective responsibilities of the outpatient and public health sectors during a disaster.
Outpatient Care Resources
Outpatient care resources include solo and group practices, surgical and procedure centers, long-term care facilities, group home and congregate environments, and home care/durable medical equipment vendors. All of these entities should have a disaster plan. (Facilities that are reviewed by the Joint Commission often are better prepared than solo practices or nonresidential facilities.) These plans should include mechanisms to
• Communicate—receive health alerts and other public information, as well as communicate with staff, patients, and partner facilities during a disaster.
• Contribute—adjust practices to the demands of the incident, and assist in meeting patients’ health needs through expanded or novel mechanisms.
• Coordinate—coordinate policies and practices with either a partner health system or local government emergency response (including public health) recommendations. This process should be determined in advance of an incident, and the necessary electronic and other mechanisms should
TABLE 8-1
Sample of Responsibilities of the Outpatient and Public Health Sectors During a Disaster
| Function | Health Care Sector | Public Health Sector |
| Overall | Providers, private infrastructure, medical materiel support, medical care and decision making, clinical policy development/technical expertise | Organizational support, situational awareness, liaison to emergency management/emergency operations center (EOC) and state/local government (including legal authorities and regulatory, policy, and logistical support [e.g., sites for care]) |
| “Electronic care”: telephone triage/ expanded patient hotlines/web-based assessment and prescribing | Augment and unify telephone advice and prescribing systems; update and modify advice “scripting" | Set up public lines/resources when demand exceeds available augmented resources; provide mechanisms for backup to 911 and other call centers; facilitate phone script coordination; address prescribing and practice regulatory issues |
| Ambulatory alternate care sites (e.g., “flu centers” or minor trauma care sites) | Augment existing clinics, and open new clinics in other spaces; assist in staffing public health clinics | Set up clinics in high-incidence/impact areas where health care resources are inadequate; provide site and logistics support (and potential staffing from Medical Reserve Corps and other public sources); address prescribing and practice regulatory issues |
| Nonambulatory alternate care sites (hospital overflow; may include medical shelter for nonambulatory patients) | Provide policy, medical direction, staffing, and special medical materiel support to site | Provide site and logistical support in conjunction with emergency management; legal/regulatory protections |
| Population-based interventions | Provide vaccinations and prophylaxis in conjunction with public health policy and directives (may include closed points of distribution) | Coordinate overall provision of interventions, including public sites and their staffing |
be in place and tested. The process for changing clinical policies should be understood in advance since adjustments are required during an incident (e.g., to staffing, personal protective equipment, treatment guidelines, referral guidelines).
Outpatient Providers and Facilities
Providers
The roles and responsibilities of outpatient providers fall into two categories:
• Medical skills—may be utilized in their usual practice environment; in alternate care systems/ assignments (including, e.g., serving as members of the Medical Reserve Corps [MRC], answering patient hotlines); and perhaps even in their neighborhood, as they may become a nexus for care that their neighbors cannot otherwise access (e.g., after an earthquake or flood that isolates the area or during an epidemic when they are a trusted and available source of information) (Schultz et al., 1996).
• Infrastructure—practice environments may be adjusted to help meet the demands of an overwhelming incident. For example, clinic functions may be
o expanded—using expanded hours, modifying care practices, and adjusting schedules to accommodate increased acute care (and deferring elective appointments), clinics can “surge” to accommodate additional patients; and
o repurposed—outpatient infrastructure may be repurposed during an incident as, for example, when a subspecialty clinic adjusts its hours or closes to enable the space to be used for acute care.
Integrating outpatient providers into a disaster response requires that they have both an awareness of their role within their facility and system and a way to coordinate their practice with broader community efforts; this includes having a mechanism with which to monitor the common operating picture of the incident. Hospitals and acute care facilities, in coordination with government emergency response entities (including public health agencies), should educate out-of-hospital and alternate care providers on a variety of response topics prior to an incident to support an effective response. Table 8-2 lists disaster planning issues for outpatient providers.
In some communities, providers offer their skill set for disaster response by preregistering with a local MRC (Medical Reserve Corp, 2011) unit or with the Emergency System for Advance Registration of Volunteer Health Professionals (ESAR-VHP) (ASPR, 2011b). This facilitates their credentialing and integration into a community response, such as by assisting at shelters. These providers then can serve under the umbrella of the government emergency response entity (e.g., emergency management agency, public health agency) with state and/or federal liability protections. A preregistration system also may help mitigate the convergent volunteerism that results in many providers coming to the site of an incident in an unstructured manner that does not support the response effort (Cone et al., 2003). However, these public health emergency response systems often do not offer providers a mechanism for surging in their own private-practice
TABLE 8-2
Disaster Planning Issues for Outpatient Providers
| General |
• Knowledge of significant/likely hazards to facility • Mechanisms of staff and patient notification/incidentcommunications • Facility resources |
| Staffing |
• Usual resources • Supplemental resources and their sources • Education and training (including source andmechanism for just-in-time training) • Staff surge planning (e.g., change in hours) • Legal/regulatory issues (e.g., liability, contract issues, reimbursement issues) |
| Clinical Care |
• Patient flow, triage, scheduling, diversion • Infection prevention and control • Surveillance/detection responsibilities • Treatment protocols/patient prioritization (including, e.g., telephone prescribing, hotline/advice line referrals) |
NOTE: Adapted from CDC working group on Alternate Care Systems and used with permission of Cpt. Deborah Levy, PhD, MPH.
settings or a means of integrating their practice with the community response. A basic infrastructure of preparedness is a requisite for the delivery of care during a disaster, but is not often considered in a busy practice. Augmentation of simple day-to-day activities and integration into existing disaster communication channels can help providers contribute to the response without imposing large financial or time commitments.
Clinics
This category encompasses a broad array of organizational structures, from multispecialty system-affiliated clinics and federally qualified health clinics to solo independent practitioners. The vast majority of this infrastructure is private, although there are some publicly operated clinics. Additionally, urgent care facilities, clinics based in retail stores, and pharmacies that may provide some medical screening and care should be engaged in disaster response. Finally, contributions from providers of nontraditional care, such as dentists, veterinarians, and others, may be required to support surge requirements during a disaster.
Surgical and Procedure Centers
These facilities may be repurposed to provide acute care, nonambulatory hospital overflow care, or elective surgeries not possible at hospitals (during infectious disease incidents), depending on the demands of the incident, the specifics of the facility, and the needs of the community. The need for modified regulatory and licensure standards (e.g., changes in the scope of care) should be addressed in advance in the event that federal, state, or local government entities (such as public health) mandate the delivery of triaged care in these facilities.
Long-Term Care Facilities
Many types of facilities are encompassed by this category. Most long-term care facilities have limited surge capacity to accommodate hospital discharges, although they should not be overlooked as a resource. They may have a role in particular in rural areas, where hospital-associated long-term care facilities may not operate at capacity, and demand in the community may not justify a separate alternate care site. Long-term care facilities should be prepared to shelter in place (including without power) during a major incident, and to modify patient care and referral policies (including when patients are referred to the emergency department) depending on the resources available within the health care system. Long-term care facilities also should plan for a disproportionate impact of certain incidents (e.g., a pandemic involving a novel influenza strain) on their residents (AHRQ, 2007a). Finally, a long-term care facility should have memorandum of understanding (MOU) in place both within its jurisdiction and in a distant jurisdiction to support evacuations or the delivery of CSC during an incident.
Group Home and Congregate Environments
These types of locations (e.g., schools, businesses) with on-site medical personnel may provide dispensing or vaccination/prophylaxis services in conjunction with government disaster response efforts, especially those of public health agencies. They also should be prepared to provide sheltering or isolation for their residents/ students during an incident and adjust referral criteria and care policies to reflect current community practices during a disaster.
BOX 8-1
Home Care Agencies’ Allocation of Scarce Resources
During the 2011 Southern California blackout, home oxygen generators failed and had to be replaced by nonpowered oxygen tanks and systems, which were in short supply. A home care agency determined that it would give priority to patients with active treatment plans (i.e., hospice patients were last to be served). As a result, many hospice patients were taken to area emergency departments for symptomatic relief.
Key issues:
• Many home medical devices are dependent on electrical power.
• H ome care agencies should have a plan for prioritizing support for these patients, and these plans should be communicated prior to an incident. Overall guidance (e.g., from respiratory care societies) is needed on the management of home oxygen and ventilator patients during a disaster to help standardize support and backup systems.
• Hhe cost of maintaining portable oxygen cylinders for rare incidents is problematic.
• H evice-dependent patients should have a care plan in case of system failure.
• H mergency departments may be overwhelmed by patients with chronic care needs when home care services cannot be maintained.
SOURCE: Greenwald et al., 2004.
Home Care/Durable Medical Equipment Vendors
Home care/durable medical equipment vendors should have plans to prioritize their services based on the nature of an incident (and adjust them as the incident evolves over time). These plans also should cover clients that are quarantined, isolated, or sheltering in place because of weather or other emergencies (see Box 8-1). Home care and durable medical equipment vendors may play critical roles as well in providing equipment and services to shelters and alternate care sites (AHRQ, 2011; Rebmann et al., 2011).
Family-Based Care
Home care provided by family members can play a critical role in preventing the medical system from being overloaded, whether during a pandemic or an incident such as a blackout. Families should be prepared for expanded responsibilities during an incident. Further, home care agencies should develop mechanisms to communicate issues related to CSC during an incident.
Alternate Care Systems
Although the previous section addressed outpatient entities whose existence is not tied to disaster response, recent experience (e.g., the H1N1 pandemic, Hurricane Katrina) demonstrates that such entities can serve to reduce patient volume at hospitals and are a crucial response component. When a disaster overwhelms the surge capacity of both hospitals and these traditional outpatient entities, alternate care systems may be established. The common types of alternate care systems and their functions are described in the following sections. Each type provides for the needs of specific patient groups (e.g., ambulatory and nonambulatory,
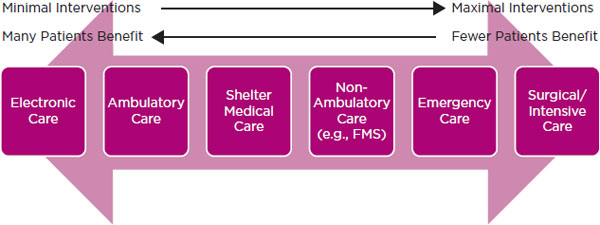
FIGURE 8-1
Relationship between degree of intervention at an alternate care site and number of patients that can benefit from the intervention. NOTE: FMS = federal medical station.
surgical, emergency, shelter based), requires a certain amount of time to set up, and may be more appropriate in certain types of disasters (e.g., an evolving epidemic versus a no-notice mass casualty incident). Figure 8-1 illustrates that as the degree of intervention increases, the number of patients that can receive the intervention decreases. Especially when CSC are in effect, the goal of providing the most benefit to the greatest number of people should influence the types of alternate care systems established. The following discussion expands on foundational work sponsored by the U.S. Soldier Biological and Chemical Command on modular emergency medical systems planning for disasters, including documents on acute care centers and neighborhood emergency help centers (DOD, 2001a,b).
One of the primary benefits of alternate care systems is their flexibility: both government emergency response entities and private health care institutions can establish them to maximize the efficiency of reaching an entire community. For instance, mass prophylaxis and vaccination centers are used in campaigns to inoculate a large population, and thus are generally operated by public health departments in community locations (NACCHO, 2008). However, health care facilities also may have a critical role to play in administering these interventions as closed points of dispensing (NACCHO, 2008) for their own institutions, as may nonhealth facilities (such as businesses or corporations) for their employees. These strategies should be incorporated into local public health dispensing plans and those associated with established health care coalitions.
Electronic Alternate Care Systems
Basic interventions can be provided to a large number of people for specific criteria/symptoms using minimal resources via electronic means. Online and telephone assessment and prescribing (implemented successfully in many jurisdictions for early antiviral treatment during the 2009 H1N1 pandemic, for example, through poison control centers) provide a method for treating at-risk individuals rapidly and without face-to-face encounters (Kellermann et al., 2010). Health insurance- and health system-based telephone and web systems, augmented by government emergency response systems as needed, can help meet demand (AHRQ, 2005, 2007c). Referral policies and telephone scripting may have to be adjusted to provide consistency across agencies/entities. Similar systems also can provide psychological assessments for patients with anxiety or
depression related to a disaster. In addition, telemedicine may be used to augment specialty care (Nicogossian and Doarn, 2011). Experts from outside the affected area may be used to provide consultation to support overwhelmed local resources; for example, burn experts outside an affected area may provide hotline or telemedicine support to community providers. Emerging social media technologies may also play a role.
Ambulatory Care Facilities
These facilities (e.g., “flu centers” or casualty collection points) are intended to serve the minimally ill or injured who cannot be accommodated by the usual outpatient infrastructure. The need for such facilities, as well as their staffing and supply, varies greatly depending on the type of incident and the phase of the incident. Acute need for such sites may be seen during a pandemic or after a massive no-notice incident, such as an earthquake or detonation of an improvised nuclear device. Health care facilities may set these units up in nontraditional locations on their premises (CBS News, 2009; Chung et al., 2011; Cruz et al., 2010) or at other sites under their control. Public sites may be initiated if the capacity of the health care system is overwhelmed or if selected populations or areas are disproportionately affected. These public sites also may be in nontraditional locations (e.g., veterinary clinics, dental clinics, schools). Preplanned supplies for infectious and trauma incidents should be considered for ambulatory care facilities. However, it is advisable to work with state Centers for Medicare & Medicaid Services offices to ensure that appropriate waivers are obtained.
Shelter-Based Care
The medical care needs of the sheltered population may be extensive, and a high level of medical expertise and materiel may be required at public shelters (e.g., for patients that are oxygen dependent, receive dialysis, or have behavioral health needs). Current recommendations are to avoid special shelters for those with medical or other physical/functional limitations because of the potential for discrimination due to failure to prepare for their needs in general shelters. Thus, the medical community should work with government emergency response entities (and the MRC and other groups) to ensure adequate medical staff and supply support for shelters, depending on demographics and the specifics of an incident.
Nonambulatory Care/Hospital Overflow
Often set up in flat-space areas (convention or event centers, gymnasiums, armories), these sites provide overflow for patients that are nonambulatory but have less intensive medical needs than hospitalized patients. Significant work has been done on the planning and supply of these sites (AHRQ, 2007b; Hick et al., 2004; JCAHO, 2005; Skidmore et al., 2003; State of California, 2012a,b).
Federal Medical Stations
These 150-bed units are designed to provide basic nonambulatory care to hospital overflow patients with minimal medical needs or to shelter patients with more advanced outpatient needs. Requested by state health or emergency management agencies, they are designed to be moved into “structures of opportunity” in the community, such as schools or convention centers. Although multiple federal medical stations are available, the supply is clearly inadequate for a multistate or national event (e.g., a pandemic, a major earthquake), and the request and setup process requires days. Federal medical stations may be integrated with shelter-based or nonambulatory care or be independent (ASPR, 2012). The federal medical station organization and logistics may be helpful templates for local planning for nonambulatory care centers.
Emergency Care Replacement/Overflow
Usually provided in a specialty trailer or temporary specialty structure, emergency care replacement or overflow sites provide replacement capacity for damaged emergency departments (particularly in smaller communities). They also can provide temporary increased capacity for a single facility or area during a special event or major incident, particularly one involving health care or transportation infrastructure damage that limits access to emergency care. The level of care provided often can be equal to that provided in a hospital environment. Setup usually takes a matter of hours. The number of patients that can be served is limited by the size of the structure (Blackwell and Bosse, 2007; D’Amore and Hardin, 2005).
Surgical/Intensive Care or Inpatient Replacement/Overflow
Also provided in specialty trailers or temporary specialty structures, these care sites provide specialty services in communities whose infrastructure is damaged or inadequate (Bar-Dayan et al., 2005; D’Amore and Hardin, 2005; Rhodas et al., 2005). The infrastructure requirements of such sites are significant (D’Amore and Hardin, 2005; Kreiss et al., 2010). Although these sites often can provide advanced services, at times they can be inserted into situations in which they are the only advanced care infrastructure, which can lead to both capacity and capability issues with respect to supplies and specialty providers (Bar-On et al., 2011; Burnweit and Stylianos, 2011; Kreiss et al., 2010; Merin et al., 2010).
Mass Mortuary
Although not a matter of clinical care per se, structured planning for mortuary services during a major incident is critical to maintaining the dignity and timely and orderly processing of the deceased, as well as social order. Plans for surge capacity mass mortuary sites should be planned in coordination with the jurisdiction’s coroner and office of emergency management for possible logistical support. In addition, plans should include options for staffing (incorporating a National Disaster Medical System [NDMS] disaster mortuary operational response team when possible, as well as state-based resources to support a mass fatality or mortuary incident) (ASPR, 2011A), equipment, identification, family support/viewing, processing, and holding/ storage. Such sites are an important part of disaster planning, but are not addressed further in this report. In developing mass mortuary plans, coordination with EMS and hospitals is essential.
In many communities, public health agencies are the only entities capable of harnessing the vast array of outpatient resources for disaster care for the community’s benefit. In other communities, public health agencies have a role that involves coordination or is secondary to efforts being led by health care entities themselves. Given the variability in both structure and relationships among entities engaged in health-related activities in communities nationwide, it is not possible to identify which entity should take the lead in all cases in harnessing resources for disaster care. Regardless, it is important that this entity be able to monitor, communicate about, and coordinate public and private resources across a region. Such entities will have to leverage the resources and expertise of health care, health care coalitions, and private-sector partners, as well as other public emergency response agencies, to accomplish these goals. This section describes how such entities
can coordinate the expansion of outpatient care and summarizes a framework for maximizing the utility of outpatient disaster medical care.
Expansion of Care
As demand exceeds existing outpatient resources, it becomes necessary to maximize the ability of hospitals and acute care facilities and systems to expand capacity. Every response coordination entity, especially departments of public health, should monitor this situation and work with health care entities to determine the next steps to be taken if private capacity and capabilities become overwhelmed or demand forecasting predicts that this will occur. Proactive planning for the next steps is critical to avoid falling behind the demand curve. Close coordination is required, and each incident will demand different utilization of the resources of outpatient facilities and alternate care systems. This is perhaps the most difficult aspect of planning as, given the variations across facilities and systems in the resources needed and available, no single strategy applies, and the success of the response depends on the commitments and coordination of the stakeholder entities in responding to incident-driven needs in a flexible, scalable fashion. Hospitals and acute care facilities should work closely with local public health agencies to determine priorities for therapies and services. Emergency response entities should ensure that appropriate regulatory and logistical issues of care are addressed in coordination with other public and private agencies. Hospitals and acute care facilities should ensure that a clinical care committee (in some cases, a very small command group/staff) determines what services can be offered and how these services fit with community priorities. In some cases, this decision making may occur at the health system level. The goal for independent facilities is that, although these decisions are made by a small group, they are informed by broad information sources channeled through emergency response coordination entities and are consistent with a common response strategy. Box 8-2 provides an example of the difficulties that can arise in making decisions about the allocation of outpatient resources even when high-level guidance is available. Table 8-3 illustrates how the emphasis of the outpatient response shifts according to the incident type, duration, and phase.
Local Emergency Response Planning to Incorporate Outpatient Care
Local emergency response planning for outpatient disaster medical care entails the following five elements:
• Communication and coordination plan—The ways in which providers and facilities exchange information with government agencies, such as public health and other health entities, is critical to maintaining the flexibility required to implement strategies and tactics that are usually incident and time dependent. Outpatient facilities often are left out of usual notification loops and may not have an around-the-clock point of contact. Also, these entities generally are not involved in traditional mass casualty incidents, so determining at what point they have a role and then activating that role requires a process, such as a multiagency coordination plan (FEMA and Emergency Management Institute, 2008), that includes assessment of the situation and determination of what health care assets will be required to address the demand. Additionally, robust public and provider engagement efforts should be undertaken in advance of and during a mass casualty incident to
BOX 8-2
Allocation of Outpatient Resources
During the 2009 H1N1 pandemic, the Centers for Disease Control and Prevention’s (CDC’s) Advisory Committee on Immunization Practices (ACIP) provided recommendations on priority groups for influenza vaccine (CDC, 2009a). However, initial vaccine supplies were limited, and states had to determine which priority groups would receive vaccinations first. One state decided to make health care workers the highest-priority group, while an adjoining state determined that the highest priority would be children with at-risk health conditions. A consequence was that providers in health care systems that spanned the border were eligible for priority vaccine at some of their worksites but not others. This led to significant frustration being directed at the hospital infection control unit and local and state public health agencies.
Key issues:
• Federal guidance is valued by the states for several reasons, including provision of a rationale for otherwise contentious allocation decisions.
• Limitations of this guidance may create inconsistencies that necessitate appropriate risk communication to minimize confusion and mistrust.
• lituational awareness requires communication with adjoining jurisdictions that may be implementing justifiable but different plans.
• Health care workers often work at institutions in multiple jurisdictions, creating the potential for significant inconsistencies.
enhance both communication and coordination (see Chapter 9). Finally, local public health often maintains contact information for private health care entities and practices for purposes of health communications in nonemergency situations, which could be utilized as a resource during CSC.
• Leadership for public alternate care systems—This includes planning for solutions that distribute patient volume (e.g., hotlines) and establishing public sites for ambulatory and nonambulatory care based on the community’s resources (Cinti et al., 2008; Lam et al., 2006). These plans should be flexible, particularly with respect to ambulatory care, to allow for the spontaneous development of sites near a disaster scene (and management of the convergence of victims, family members, and volunteers on that area) (Cone et al., 2003). Support for these ambulatory sites of care (especially in a no-notice incident) requires close coordination with EMS, emergency management, and other response entities.
• Provider engagement—This includes education about disaster relief opportunities (e.g., MRC registration) and the provision of crisis care (e.g., principles, sources of information, community engagement efforts).
• Provider mobilization in an emergency—In an era when many outpatient providers have limited or no hospital or health system practices/privileges, a designated organizer of unaffiliated outpatient providers is required (e.g., public health agency, health care institution consortium, local/state medical society). Official tasking and activation by government emergency response entities often confers legal and regulatory protections that should be defined prior to an incident.
• Interface for crisis care between local/regional emergency response entities, including public health agencies, medical systems, and the state—This interface includes the relationship between the state disaster medical advisory committee (SDMAC) and any regional constructs, such as the regional DMAC, regional triage teams, and other mechanisms. The activation of such groups and their operational role should be established and exercised.
TABLE 8-3
Out-of-Hospital Response Emphasis According to Incident Type,* Duration, and Phase
| Type of Incident | Early in Incident | Mid-Incident | Late in Incident |
| Anthrax Terrorist Attack (1 week) |
• Outpatient surge capacity, including screening guidelines • Private alternate care sites • Hotline and web-based triage and prescribing for exposures • Public and closed points of distribution of prophylaxis |
• Early incident strategies plus o Nonambulatory alternate care sites (for hospital overflow—including federal medical stations) o Mass fatality management |
• Nonambulatory alternate care sites (for hospital overflow or as bridge to transfers) • Mass fatality management |
| Catastrophic Earthquake (24 weeks) |
• Outpatient surge capacity for minor trauma • Private alternate care sites for minor trauma • Public alternate care sites (support of spontaneous and preplanned sites of care) |
• Shelter medical support • Nonambulatory alternate care sites (often as bridge to transfers) • Emergency and surgical care—replacement for damaged infrastructure |
• Shelter medical support • Emergency, surgical, and intensive care—replacement for damaged infrastructure |
| Detonation of Improvised Nuclear Device (4 weeks) |
• Outpatient surge capacity for minor trauma • Private alternate care sites for minor trauma • Public alternate care sites for trauma (support of spontaneous and preplanned sites of care) |
• Nonambulatory alternate care sites (often as bridge to transfers) • Public screening sites for triage/treatment of radiation injuries • Outpatient surge capacity for trauma and radiation injuries (symptomatic management and laboratory evaluation) • Evacuation point medical care (for medical evacuees) • Palliative care • Mass fatality management |
• Shelter medical support • Outpatient surge capacity for follow-up evaluation and care for radiation injuries • Palliative care • Mass fatality management |
| Pandemic (12 weeks) |
• Outpatient surge capacity, including isolation • Private alternate care sites • Hotline and web-based triage and prescribing for early illness/exposure • Vaccination sites—private and public |
• Early incident strategies plus o Public “flu centers” o Augmented home care o Nonambulatory alternate care sites (for hospital overflow) o Mass fatality management |
• Outpatient surge capacity • Private alternate care sites • Hotline and web-based triage and prescribing for early illness/exposure • Mass fatality management |
*The emphasis is heavily influenced by the actual impact of an incident.
Reimbursement and Financing Issues
Reimbursement of hospitals and acute care facilities for disaster-related expenditures often is difficult even with proper documentation given the private nature of most facilities and the reimbursement requirements of the Federal Emergency Management Agency (FEMA). Time and material expenses should be carefully tracked and, when possible, purchases and authorization of personnel time should be public actions (that is, ordered by public health or emergency management agencies rather than by a private health care facility) to enhance the prospects for reimbursement. Reimbursement by insurance companies for care provided in nontraditional settings (e.g., “flu centers") is an area that requires further clarification. If the site is staffed by usual health care providers and meets usual regulatory and other requirements, billing and reimbursement may be pursued in the normal manner (CMS, 2009). If, however, public sites, personnel, or supplies are used, private reimbursement usually is not possible (or necessarily permissible). Discussion of different scenarios with public and private payers prior to an incident is advisable.
Many of the functions and tasks required of the various outpatient care entities to plan for and implement CSC are similar in nature. Thus, the following descriptions of the general functions of outpatient care facilities are meant to serve as a broad guide; specific functions and tasks for outpatient care facilities, long-term care facilities, home care/medical equipment vendors, and alternate care systems are enumerated in Template 8.1 at the end of this chapter. The functions presented in this section should be regarded as optimal, not minimal, and are unlikely to be implemented without significant time and funding commitments that are not priorities in current preparedness programs. Nonetheless, they offer concrete goals for outpatient sector preparedness. The term “facility” often is used below, but the principles apply equally to the other types of outpatient entities cited above. Following these general descriptions for outpatient care entities is a section describing the function and tasks of outpatient providers; these functions and tasks make up the final section of Template 8.1.
General Functions of Outpatient Care Facilities
Function 1. Alerting. It is crucial that a facility’s disaster plan include indicators and triggers delineating the transitions from conventional to contingency to crisis care. The actions subsequently taken should be based not only on these indicators and triggers but also on the specific context of the disaster. Facilities should be able to disseminate alerts to and receive alerts from all relevant local and regional stakeholders (including partner facilities, local and state governments, and the National Weather Service).
Function 2. Notification. Facilities should maintain up-to-date contact information for staff and exercise their notification systems. Command staff and leadership should be aware of how they will be notified and how they can contact their facility in the event of a disaster. Facilities also should designate
technical experts and determine and exercise ways of exchanging input with them, including advice on incident-specific issues and policies (e.g., infection control in a pandemic).
Function 3. Command. The command staff or leadership of a facility should receive training appropriate to the facility’s size and potential response role in a National Incident Management System (NIMS)-compliant system (e.g., the hospital incident command system [HICS]) (California Emergency Medical Services Authority, 2007; FEMA, 2011a). This includes ensuring the availability of job aids to guide decision making and an understanding of how and when to transition care standards.
Function 4. Control. During or after a disaster, facilities should be able to rapidly secure their location or relocate if they cannot, implement situational assessment capabilities, request resources and acquire additional staff, and integrate those additional resources into their operations. The command staff or leadership of the facility should understand the protocols and procedures for each of these tasks and how their staff interfaces with local and regional command centers.
Function 5. Communication. Widespread disasters are likely to affect traditional lines of communication, so facilities should have procedures in place to maintain situational awareness and communication with their staff, patients, and local and regional public and private care providers through electronic, web-based, and hardcopy means. As part of an integrated response network, outpatient care providers also should know how to request local resources (e.g., ambulances through the 911 system) and how to contact local and regional command centers. Finally, there is a need for channels of communication with the local emergency operations center (EOC), health department, and emergency management agency.
Function 6. Coordination. Coordination of outpatient care requires true joint planning and unified command during an incident. It is critical that a trusted source be identified that can represent the outpatient sector’s situation, needs, and policy issues to the public health/Emergency Support Function (ESF)-8 decision makers at the EOC or multiagency coordination center. This entity provides a “seat at the table” for the many outpatient facilities and disciplines represented and can process and filter this information for the ESF-8 lead agency.
Separate representation for clinics, long-term care facilities, and other entities may be required, depending on the area and the incident. The specific mechanism used to coordinate is not as important as the fact that it exists and is understood by stakeholders. Although many successful hospital coalitions exist in the United States, few can claim to represent the outpatient sector effectively. Increased funding and time need to be allocated to reaching these providers and practices to ensure that they have a voice in planning and implementing the response to emergencies that affect the outpatient sector. This may be accomplished through existing coalitions or the establishment of new mechanisms for coordination and collaboration among outpatient care entities. These public-private partnerships are critical to a successful whole-community response during a disaster.Function 7. Public Information. Based on situational awareness, demand forecasts, and other information, consistent risk communications should be developed to inform the public about where and when
to seek medical care. Failure to maintain consistency in this information may rapidly lead to chaos or inappropriate overburdening of existing infrastructure. Timely and effective messages may significantly reduce patient volumes, allowing resources to be applied to those who most require and/or will benefit from care. A robust jurisdictional joint information system with the ability to integrate the needs of the outpatient sector and public information officers will greatly facilitate this process (FEMA, 2011b).
Function 8. Operations. As resource shortages increase in the face of growing demand, command/ supervisory staff should know how transitions from conventional to contingency and crisis care affect their resource use. These effects include the need for changes to staff scopes of practice, increased repurposing of patient care space, and the reuse and reallocation of supplies.
The societal impact of a disaster requiring the outpatient sector’s response cannot be underestimated. Communities can expect a large surge in demand for mental health support services (discussed in detail in the mental health section of Chapter 4). Mental health under CSC will require specific competencies of mental health, social services, and health care staff. Efforts also will be required to enhance community resilience through “neighbor-to-neighbor, family-to-family” support systems (such as certain psychological first aid models created specifically for use by community members as needed). The resilience of the health care workforce is paramount to the success of the CSC strategy.
One-shot, one-size-fits-all approaches, such as some stress debriefing once common for providers, are no longer recommended and may result in exacerbating the mental health problems of those most affected by a disaster (Bisson et al., 1997, 2007; IASC, 2007; McNally et al., 2003; NIMH, 2002). The replacement for those outmoded approaches is more integrated efforts to enhance the resilience of the workforce specifically with respect to mass casualty events, including CSC, as part of CSC preparedness (Schreiber and Shields, 2012).
Incident command operations need to encompass integrated mental health operations as part of incident command system (ICS)/EOC and medical/health operations. Recent models developed for Los Angeles County, Seattle/King County, the American Red Cross’s National Operations Center/Disaster Mental Health, and a new national prototype specifically for children utilize real-time situational awareness of triage/mental health risk in patients/disaster victims and responders (including health care workers, support staff, and their families) across varied disaster systems of care (e.g., hospitals, schools, shelters, public health settings) to guide actual mental health operations within the ICS (see Schreiber et al., in press). Other recommended features include a common picture of• population-level mental health risks (traumatic loss, multiple traumatic losses) using a common rapid mental health triage system across disaster systems of care, including EMS;
• mental health risks among health care workers; and
• mental health resources, including emerging national models of Internet-based intervention (Ruggiero et al., 2006).
Addressing the social and psychological challenges of CSC requires a triage-driven mental health incident management system and community resilience efforts through community engagement (see Chapter 9). Also required are basic “neighbor-to-neighbor, family-to-family” psychological first aid
competencies that leverage the community, responders, and family members as the first line of psychosocial support (see the American Red Cross’s “Coping in Times of Crises” and the “Listen, Protect and Connect” psychological first aid models).
Although most outpatient and long-term care facility staff have some experience with end-of-life issues, they are unlikely to be comfortable with the provision and management of palliative care on a broader scale. Facilitating provision of the medications and education required for families to administer this care in the home environment may be critical during epidemics and other catastrophic incidents. Accomplishing this requires education of home care, ambulatory care, and alternate care system providers and the availability of basic medications and instructional resources. See the palliative care section of Chapter 4 for further discussion.
Function 9. Logistics. Logistical requirements at alternate care sites are substantial. A few key considerations are noted in Table 8-4. Additional information on logistics related to other functions is provided under those functions.
Staffing resources may be significantly impacted by the incident itself. Access to the facility, family obligations, duty to other facilities/agencies (e.g., in cases of employment at multiple sites), and provider illness all may impact the availability of these resources. Agreements with partner facilities and staffing agencies may be helpful in maintaining adequate staffing levels. Planning for the incorporation of external staff should address credentialing, privileging, reimbursement, worker’s compensation, liability protection (including adequate legal protection for staff actions [see Chapter 3]), roles, orientation, mentoring and supervision, and access (e.g., to the facility, technology systems). In some cases, on-site accommodation of staff may be necessary (e.g., a blizzard that maroons staff at a long-term care facility), which also requires advance planning.
The MRC and other sources of volunteer providers are likely better suited to staffing public sites of care than to assisting at private institutions. The roles of MRC personnel should be discussed and agreed upon by the agencies involved.
Scope-of-practice issues may arise in scarce resource situations. Providers should always act in the best interest of the community. It may be necessary to offer just-in-time training to equip providers with new knowledge and skills, but this training should be geared to the minimum risk and maximum population benefit possible (e.g., training a provider to administer an inhaler for bronchospasm would be a minimal-risk extension of practice, whereas training a provider to manage a ventilated patient would present a potential significant risk).
Facilities and agencies should determine in advance what supplies are likely to be problematic during a major incident. These may include high-technology interventions that have limited availability, disposables required in large quantities during an incident, and supplies available from limited sources/ vendors or available in limited numbers. Examples are liquid and tank oxygen sources for situations in which home care clients who rely on powered oxygen generators are without power and N95 masks during a pandemic. Optimally, coping strategies should be identified prior to an incident.
Facilities should understand the mechanism for requesting resources from public agencies, such as local public health departments, if their vendor supplies are inadequate. This includes Strategic National Stockpile resources as applicable in accordance with the jurisdictional plan. A mechanism for triag
TABLE 8-4
Sample Logistical Considerations for Alternate Care Sites
| Category | Considerations |
| Site | Access/permissions, timeline to operational, availability (e.g., schools not always available), size, function, access for those with functional limitations, safety issues, restrooms, water/showers, loading dock, etc.; may include supplemental water, oxygen, power, and other considerations |
| Traffic Control | Parking and vehicle movement for staff, emergency medical services (EMS), families |
| Communications | Including radio, web-based, public address |
| Staffing | Medical, administrative, and support (including lab and pharmacy) |
| Medical Supplies | Durable and disposable (pharmaceuticals, intravenous fluids, dressings, diagnostics, protective equipment, etc.) |
| Administrative Supplies | Including computers and networks |
| Personal Care Supplies | Bedding, cots/beds, personal hygiene supplies |
| Food Services | Staff and patients |
| Security Services | External and internal, accountability for valuables |
| Transportation | Patients (internal and external) and materials |
| Check-in/Check-out and Badging | Time keeping, badges |
| Credentialing | Verification system |
| Registration and Patient Tracking | Patient registration and tracking systems |
| Medical Records | Records, filing, archiving/storage |
| Sanitation | Usual and medical waste |
| Animal Control/Husbandry | If pets kept on site |
ing resources when requests exceed available stocks should be in place and acceptable to stakeholders. Selected medications, vaccine, or durable medical equipment may be in short supply, and facilities may have to implement resource allocation strategies (e.g., follow Centers for Disease Control and Prevention [CDC] recommendations for treatment, apply community standards for use of N95 masks by health care workers).
Surge capacity often is limited in outpatient health care facilities because of the lack of classrooms and flat-space areas that often are available in hospitals. However, it may be possible to repurpose some clinic areas (e.g., a physical therapy area could be used for outpatient care). Additionally, tenting or other temporary facility capacity may be used in some situations. The capacity for ambulatory care is likely best enhanced by triage of appointment types, use of electronic assessment and prescribing, and adjustments to hours of operation.
Optimal alternate care site locations are dependent on the mission of the site. Ambulatory care sites may use venues (e.g., churches or schools) similar to those used for vaccination and mass prophylaxis sites, although they should not collocate without careful consideration of the risks involved. Nonambu
latory care sites require larger flat-space areas and significantly more infrastructure (e.g., showers, food). Thus, a convention center, large gymnasium, or incident center may be more suitable for these functions. Some capacity is potentially available on hospital grounds, but often is limited. Tools for the identification of alternate care sites have been developed (AHRQ, 2004, 2009).
The operation of such sites requires partnership among public health agencies, emergency management agencies, and private health care entities to ensure that staffing and supply needs are met. Generally speaking, the higher the level of care required, the more infrastructure is required per patient; the higher associated costs and space requirements limit the ability of jurisdictions to prepare for this level of mass care. Field hospitals from federal and other sources may be available and useful in certain situations. The ability of these units to be self-sufficient is helpful in environments where infrastructure is damaged, but greatly increases cost and complexity. Using existing infrastructure to house alternate care sites often is preferable to using fully portable infrastructure. Utilizing public spaces and codifying operations at such sites requires emergency management and public health authorities.
Certain incidents may require special considerations, planning, and adaptations. For example, an incident involving a transmissible infectious agent will have implications for patient flow, quarantine, isolation, exposure of noninfected patients, personal protective equipment, visitor/escort policies, vaccination, and home care recommendations (APIC, 2009; CDC, 2009b).
Many patients require specialized resources and planning for adequate outpatient care. Examples include pediatric patients, those with physical or cognitive limitations, those with limited access to transportation, and those who are dependent on health care technologies (e.g., power-dependent ventilator, oxygen generator, dialysis equipment). Special considerations in the planning process also are entailed for those with limited English skills and other cultural and/or ethnic needs (HHS, 2011).
As an example, planning for pediatric care in a disaster includes components of specialized provider education, specialized clinical equipment, dietary needs, bedding and care materials, child/age-appropriate activities, family reunification/family resources, behavioral health support, and supervision (especially for unaccompanied minors). These components are significantly different from those involved in usual shelter/outpatient care planning (NYCDHMH, 2007).
Regional specialty centers and groups may have plans for some of these situations (e.g., burn care, pediatric care, renal replacement therapy [Kopp et al., 2007]), and outpatient facilities should understand their role in/interface with these plans. Outpatient facilities should ensure that they have appropriate supplies and resources available according to their role in community disaster referral plans (e.g., office-based pediatric-specific equipment or basic dressing supplies) (AAFP, 2012; AAP, 2011; National Commission on Children and Disasters, 2009).
Long-term care patients who should be evacuated from their facilities present special challenges. For example, more than 50 percent of nursing home residents have cognitive impairments (AHAF 2012; The American Geriatrics Society Foundation for Health in Aging, undated). When possible, it is highly beneficial for nursing staff to remain with these patients and for as many personal supplies (e.g., glasses, dentures) and records as possible to be moved with the patients. During Hurricane Irene, nursing home residents whose staff remained with them at the shelters fared much better than those who
were turned over to general shelter staff.1 However, long-term care facilities should include plans for evacuation of any special populations as part of their organization’s emergency response plan.
Planning for patients with physical disabilities at alternate care and shelter sites is critical, as 12 percent of the population have severe disabilities that should be accommodated, and many more are impacted at lower levels of disability (U.S. Census Bureau, 2006). Physical access, assistance with activities of daily living, control of the environment for those with cognitive impairments, and accommodation of other physical impairments should be addressed. Failure to address these issues may lead to further illness, injury, or unnecessary hospitalization.
Function 10. Planning. Outpatient facility planning should emphasize the following functions and tasks:
• the decision-making and incident management process at the facility (and/or within the facility’s health care system), including
o how and when to activate emergency plans at the facility and what this involves (many outpatient facilities have very basic emergency plans and little experience with incident management),
o decision making in response to a threat (e.g., shelter in place, evacuate),
o authorities at the facility level (versus the corporate or system level),
o availability of technical experts—regionally or system based—that can provide policy and clinical guidance related to the specifics of the incident (e.g., infection control, burn care, pediatric care),
o use of an action planning process for ongoing assessment and adjustment of strategies and tactics, and
o exercise and evaluation plans;
• facility resources and redundancy of logistical elements, such as supply chains and critical services (e.g., electricity, water);
• the interface mechanism/process between the facility and partner facilities, coalitions, and local government emergency response entities (such as public health), including the facility or coalition role in multiagency coordination and the process for resource requests;
• the primary role (and potential secondary roles) of the facility and its providers during an incident (including, e.g., shelter in place, augmented services, restricted services);
• the potential role of the facility providers within an alternate care system or as support staff at affected hospitals (with increasing emphasis on hospitalist services, few outpatient providers maintain hospital privileges); and
• means of communication between the facility and its patients, staff, and liaison/partner agencies (many outpatient facilities do not have staff notification mechanisms—these may be simple calling lists or technology based).
_________________
1 Personal communication, Lewis Soloff, New York City Department of Health, November 16, 2011.
Function 11. Administration. Administrators and clinic managers should examine what authorities they have during a crisis, and if an incident commander is designated, what authorities they are delegated. During crisis situations, having adequate authority and decision-making processes ensures that the decisions made will have the support of the administration. Especially within multifacility health systems, specific policy language may be necessary to clarify the scope of proactive decision making when triage of treatment or resources is required. Within health systems, surge capacity plans should be reviewed by corporate administration so adopted plans have overarching support.
Regulatory and legal protocols governing the provision of care, reimbursement, provider licensure and practice, EMS transport, facility licensure, and other elements may have to be modified or suspended to facilitate the provision of whole-community care. Applicable statutes and regulations should be identified prior to an incident, as well as emergency orders and regulatory changes that would facilitate response. This may be an appropriate task for corporate clinic entities and medical societies.
The generation of medical records at alternate care sites raises additional issues that should be addressed in planning. These issues include what level of records is to be kept, who will be responsible for their storage, and what will be done about access and data privacy, as well as the public versus private nature of the records and the data they contain.
Emergency management and public health agencies should understand their powers during a disaster, including during a public health versus a general emergency, and any regulatory or other relief that can facilitate the use of alternate care systems. They also should have a clear understanding of their authorities relative to their political leadership and a process for keeping their administrators and political leaders informed during the response to the incident.
Functions of Outpatient Providers
Function 1. Notification. Providers should maintain up-to-date contact information at all of their affiliated institutions. They also should participate in exercises of notification systems, both to ensure their own familiarity with those systems and to allow the facility to identify and resolve any related issues.
Function 2. Command, Control, Communications, and Coordination. Providers should receive role-appropriate incident command training that encompasses where to report, what their place is in the organizational structure of the facility’s and the region’s response, and how to provide and access situational updates. Providers also should be aware of volunteer opportunities beyond their commitment to a particular facility, including as a part of the MRC and/or the ESAR-VHP.
Function 3. Public Information. Individual providers should familiarize themselves with how to input information into and extract information from facility and public sources (likely electronic or telephone based). Coordination of communication with the joint information system is crucial to the success of risk communication efforts.
Function 4. Operations. Providers should know their facility’s process for expanding care—including relevant strategies used in their area—as demand overwhelms available resources. To operate effectively under CSC conditions, providers must thoroughly understand their triage roles (if any), be able to recognize psychological issues that may arise, and be aware of their potential role as palliative care providers.
Function 5. Logistics (space, staff, supplies). Providers should be well versed in how to expand their patient care space to accommodate a significant increase in patient volume, which in a no-notice incident can overwhelm their facility quickly. Providers themselves may become a scarce resource as patient volume increases; familiarity, through education and exercises, with the ways in which their own roles will change with shifts in the care continuum will allow them to maximize the use of their time and effort. These changes can include an expansion or contraction of their traditional scope of practice, adjusted documentation requirements, and incorporation of external staff into the unit. Finally, providers should know how to request additional resources and what procedures they should follow to substitute, conserve, adapt, and reuse those resources.
Function 6. Legal Issues. The legal terrain of providing care during a disaster, especially one that requires the use of CSC, can be daunting. Providers should not wait until an incident has occurred to learn about their legal protections and liabilities in different disaster scenarios (e.g., in a declared versus a nondeclared emergency, as a public versus private care provider). Chapter 3 provides a detailed discussion of the legal issues associated with disaster response.
Function 1. Alerting
Task 1
Health care facility is able to receive and manage alerts from partner facilities (corporate, health care coalitions, hospital, or other facility partners), public health agencies (health alert network), and the National Weather Service.
Task 2
Emergency response plan provides triggers and process for incident command to activate the CSC plan and indicators (if applicable) to prompt consideration of activation.
Function 2. Notification
Notes and Resources
Institution should at least annually test notification systems and ensure that up-to-date contact information is available.
Task 1
Institution is able to alert staff within and external to the facility, including
• medical, administrative, and support staff; and
• command/supervisory staff (especially if part of the larger system).
Notification mechanisms account for redundancy in case a disaster affects usual means of contact/consultation.
Task 2
Facility identifies technical experts that can work with the administration to determine issues/policies related to infection control, infectious diseases, pediatric care, mental health care, and other specialties as required by the role of the facility. (These may be identified regionally.)
Function 3. Command
Task 1
A hospital incident command system (HICS) (or other modified National Incident Management System [NIMS]- and community-compliant system) appropriate to the institution’s size and role is utilized. Includes
• understanding how decisions regarding changes to facility policy or clinical practice are implemented during an incident (decisions system- or facility-based?);
• training and exercising with key staff;
• command staff being trained in the full continuum of care, including use of crisis spaces and staffing;
• command staff understanding incident action planning and use of the planning section during longer-term incidents (including the interface with the corporate structure as applicable); and
• appropriate resources (job aids) being available to guide capacity expansion decisions.
Function 4. Control
Task 1
Command staff/leadership understand, to the degree necessary for the size/scope of the facility’s engagement, the interface for resource requests and the acquisition process (as well as any existing plans for resource triage/allocation) with
• local public health and emergency management,
• local/regional hospital or other partner coalitions, and
• state resources (usually through local emergency management).
Task 2
Command and other appropriate staff understand transfer and diversion policies in the area and their function during disaster situations (including any agreements to receive ambulances or referral patients and what to do when emergency medical services [EMS] cannot rapidly transfer a patient from the facility to the hospital).
Task 3
Command staff understand the processes for sheltering, relocation, and evacuation in response to threats to the facility.
Task 4
Command staff understand options for security/access controls and community law enforcement support during a disaster.
Task 5
Facility plan reflects a phased expansion of surge capacity/capabilities for conventional, contingency, and crisis care situations.
Task 6
Command staff understand the process for rapid facility and response assessment in the immediate aftermath of an incident to gain situational awareness.
Task 7
Command staff/administrators understand the process for determining facility shut-down procedures (if required) and notification/diversion of patients.
Task 8
Command staff/administrators understand their authorities relative to the facility and its role in any larger system (e.g., authority to change staffing, hours, policy).
Function 5. Communications
Task 1
Facility has policies and procedures in place for sharing situational updates with staff, patients, and other facilities and agencies as necessary (ideally via multiple methods, potentially including):
• staff e-mails, text messages, paging, telephone, and other devices;
• announcements, handouts, and postings; and
• web-based and social media.
Task 2
Facility has the ability to communicate with
• local EMS (911 system) for emergency transportation,
• the local emergency operations center (or representative to same),
• the local/regional health and medical multiagency coordination center (as applicable), and
• other hospitals/partner facilities in the area.
Function 6. Coordination
Task 1
Command staff understand the interface between the institution and local public health and emergency management agencies and any local/regional health care coalitions during a disaster.
Task 2
Institution understands the function of the state disaster medical advisory committee and any regional medical coordination center or regional disaster medical advisory committees, as well as the means by which information is received from or communicated to these bodies.
Task 3
If facility is part of a health care system, plans document the integration of facility response with the corporate response structure and processes.
Task 4
If facility has a limited patient population (Department of Veterans Affairs [VA], pediatric, or other specialty facility), there is guidance/a plan for how that facility contributes to the response when an incident affects either its usual target population or other groups disproportionately.
Function 7. Public Information
Task 1
Facility coordinates information with other agencies and facilities and participates in jurisdictional joint information system (JIS) activities as appropriate.
Function 8. Operations
Notes and Resources
The mental health section of Chapter 4 provides a more detailed discussion and examples.
The palliative care section of Chapter 4 provides a more detailed discussion.
Conventional, Contingency, and Crisis Care Conditions
Task 1
Under conventional care conditions, command/supervisory staff know how to maximize capacity, including postponing elective appointments, adjusting staffing and hours, and other changes.
Task 2
Under contingency care conditions, command/supervisory staff can implement plans for repurposing patient care areas (e.g., changes to waiting areas to segregate infectious patients, space expansion) and understand the decision process for changes to clinical practice.
Task 3
Under CSC conditions, same as under contingency care conditions, but options are expanded to include
• reuse and reallocation of supplies,
• changes in staff roles or facility role (e.g., change from specialty clinic to “flu center"), and
• adjusted standards for patient care according to circumstances.
Mental Health
Task 1
Facility has a plan for triage-driven management of psychological casualties, including participation in local/regional plans for disaster mental health incident management.
Task 2
Facility has all personnel trained in basic “neighbor-to-neighbor, family- to-family” psychological first aid that includes psychological triage.
Task 3
Facility has a health care worker personal resilience plan with inoculation, self-triage, and evidence-based care elements.
Palliative Care
Task 1
Facility has anticipated the need for adequate symptomatic management (analgesia, antiemetics, anxiolytics) for its patients (including those that will not receive other treatments). These medications may be in short supply in community pharmacies.
Task 2
Palliative care is addressed in the emergency operations plan, including palliative care principles, triage tools if applicable, home care and medical equipment referrals, counseling referrals, and family support resources.
Task 3
Palliative care training (including just-in-time training) can be made available to facility staff.
Function 9. Logistics
Notes and Resources
See http://www.health.state.mn.us/oep/healthcare/scarce/index.html.
Staffing
Task 1
Call-back criteria and policies are in place and include maintenance of current and accurate employee contact information.
Task 2
Facility assesses the number of staff potentially available during whole-community incidents, including situations that limit access to the facility, affect staff families, or result in provider illness/injury.
Task 3
Facility has planned for on-site accommodation of staff and family members as appropriate.
Supplies
Task 1
Identify key potential scarce resources based on types of incidents and stockpiles or identify alternative sources for these supplies if possible (e.g., N95 masks, selected medications).
Task 2
For highly vulnerable supplies, identify strategies for appropriate substitution, conservation, adaptation, reuse, and reallocation.
Task 3
For local or state cached supplies (such as a local pharmaceutical cache) or Strategic National Stockpile (SNS) supplies, facility understands the process for request, receipt, and distribution of these supplies through public health agencies.
Space
Task 1
Facility has examined available patient care space and conversion of non-patient care areas to patient care, as possible.
Special Considerations
Task 1
Patient groups requiring special consideration are identified, and, to the degree possible, equipment and supplies to address the needs of these
groups are purchased and/or stockpiled in relation to the facility’s size and role in the community. Considerations include (but are not limited to)
• pediatric patients;
• potential need for airborne isolation;
• patients with functional limitations (e.g., hearing or visually impaired);
• patients needing dialysis/renal replacement therapy; and
• severely mentally ill adults/severely emotionally disturbed children.
Task 2
Facility understands any regional plans or resources for specific groups (e.g., regional pediatric or dialysis networks) and its role in such plans.
Function 10. Planning
Task 1
Facility understands how to access appropriate technical specialists and how they interface with the facility’s (or corporate) command and planning functions (may be a regionally shared function—for example, a regional disaster medical advisory committee).
Task 2
Facility and/or system uses an action planning process and can modify the strategies, tools, or process based on evolving incident information.
Task 3
Facility and/or corporate bylaws and credentialing policies and procedures account for the use of outside staff during a disaster, including the use of local/regional staff in accordance with coalition agreements, and for the integration of outside staff, including orientation, mentoring, and supervision.
Task 4
Policies for altered staffing ratios, shift lengths, and staff roles are examined, and any collective bargaining issues are identified, if not addressed.
Task 5
Facility understands the process and supporting agreements (e.g., related to worker’s compensation, liability) for sharing staff with other facilities in need, including staffing of alternate care sites.
Function 11. Administration/Legal Issues
Notes and Resources
See Chapter 3 for a more detailed discussion.
Task 1
Administration (including corporate administration outside of the facility) examines its delegation-of-authority processes and makes any changes necessary to ensure that CSC decisions are supported
(i.e., that facility decision makers are acting with the support of administration).
Task 2
Administration understands relevant changes to facility authorities and protections when state declarations of emergency/public health emergency are made, including legal protections or obligations for medical providers (e.g., duty to serve).
Task 3
Facility and/or corporate legal counsel are aware of surge capacity plans and implications for patient care.
Task 4
State and local laws and regulations that would constrain the institution’s ability to implement CSC plans and possible solutions are identified (may be a regional effort—see Chapter 3 for a detailed discussion of functions).
Core Functions of the Outpatient Sector in CSC Planning and Implementation
Long-Term Care Facilities
Function 1. Alerting
Task 1
Long-term care facility is able to receive and manage alerts from partner facilities (corporate, hospital, or other facility partners), public health agencies (health alert network), and the National Weather Service.
Task 2
Emergency response plan provides triggers and the process for incident command activation.
Function 2. Notification
Task 1
Institution is able to alert staff within and external to the facility, including
• medical, administrative, and support staff; and
• command/supervisory staff (especially if part of the larger system).
Notification mechanisms should account for redundancy in case a disaster affects usual means of contact/consultation.
Task 2
Facility identifies technical experts (may be shared regionally) that can work with administration to determine issues/policies for infection control, infectious diseases, palliative care, and other specialty considerations.
Function 3. Command
Task 1
An HICS system (or other modified NIMS- and community-compliant system) is in place. Includes
• understanding how decisions regarding changes to facility policy or clinical practice are implemented during an incident (decisions system- or facility-based?);
• training and exercising with key staff;
• command staff being trained in the full continuum of care, including use of crisis spaces and staffing;
• command staff understanding incident action planning and use of the planning section during longer-term incidents (including the interface with the corporate structure as applicable); and
• appropriate resources (job aids) being available to guide capacity expansion decisions.
Function 4. Control
Task 1
Command staff understand the interface for resource requests and the acquisition process (as well as any existing plans for resource triage/ allocation) with their local partners (regional medical coalitions and public health and emergency management agencies as applicable).
Task 2
Command and other appropriate staff understand the interface with EMS and what services EMS will provide during evacuation and other events associated with an incident.
Task 3
Command staff understand the processes for sheltering, relocation, and evacuation in response to threats to the facility.
Task 4
Command staff understand options for security/access controls and community law enforcement support at their facility during a disaster.
Task 5
Command staff/administrators understand the process for determining facility shut-down procedures (if required).
Function 5. Communications
Notes and Resources
Task 1
Facility has policies and procedures in place for providing situational updates to staff, patients, and their families. Ideally, these mechanisms have redundancy in case of failure of the primary system.
Task 2
Facility has the ability to communicate with
• local EMS (911 system) for emergency transportation,
• the local emergency operations center (or representative to same),
• the local/regional health and medical multiagency coordination center (as applicable), and
• other partner facilities as applicable.
Function 6. Coordination
Task 1
Command staff understand how they are expected to interface with local public health and emergency management agencies and/or existing health care coalitions during an incident.
Task 2
Institution understands the function of the state disaster medical advisory committee and any regional medical coordination center or regional disaster medical advisory committees, as well as the means by which information is received from or shared with these bodies.
Task 3
If facility is part of a health care system, plans document the integration of facility response with the corporate response structure and processes.
Function 7. Public Information
Task 1
Facility contributes to jurisdictional JIS activities as appropriate.
Function 8. Operations
Notes and Resources
Conventional, Contingency, and Crisis Care Conditions
Task 1
Under contingency care conditions, command and unit staff are aware of how to adjust staff hours and responsibilities and resident locations to maximize capacity.
Task 2
Under CSC conditions, same as under contingency care conditions, but options are expanded to include
• reuse and reallocation of supplies;
• significant changes in staff roles; and
• adjusted standards for patient care according to circumstances (e.g., adjusting referral criteria to medical care vs. care at long- term care facility).
Mental Health
Task 1
Facility has a plan for triage-driven management of psychological casualties, including participation in local/regional plans for disaster mental health incident management.
Task 2
Facility has all personnel trained in basic psychological first aid (PFA) that includes psychological triage.
Task 3
Facility has a health care worker personal resilience plan with triage and referral elements.
Palliative Care
Task 1
Facility has planned for adequate symptomatic management (e.g., analgesia, antiemetics, anxiolytics) for patients (including those that will not receive other treatments).
Task 2
Palliative care is addressed in the emergency operations plan, including palliative care principles and resources, incorporation of incident-specific triage criteria when applicable, and patient/family support resources.
Task 3
Palliative care awareness training is provided to staff, and just-in-time training can be made available.
Function 9. Logistics
Notes and Resources
Staff
Task 1
Call-back policies are in place, including maintenance of current and accurate employee contact information.
Task 2
Facility considers alternative staffing plans during incidents that limit access to the facility or result in provider illness/family illness.
Task 3
Facility has planned for on-site accommodation of staff and family members as appropriate.
Supplies
Task 1
Identify key potential scarce resources based on types of incidents and, to the degree possible, stockpiles or identify alternative sources for these supplies (e.g., N95 masks, antivirals, vaccines).
Task 2
For highly vulnerable supplies, identify strategies for appropriate substitution, conservation, adaptation, reuse, and reallocation as appropriate.
Task 3
For local or state cached supplies (such as a local pharmaceutical cache) or SNS supplies, facility understands the process for request, receipt, and distribution of these supplies.
Space
Task 1
Facility has examined available patient care space and conversion of non-patient care areas to patient care, as possible.
Function 10. Planning
Task 1
Facility and/or corporate bylaws and credentialing policies and procedures account for the use of outside staff during a disaster, including use of the Medical Reserve Corps or staff from partner facilities.
Task 2
Need for orientation, mentoring, education, and supervision of outside staff is anticipated.
Task 3
Policies for altered staffing ratios, shift lengths, and staff roles are examined, and any collective bargaining issues are identified, if not addressed.
Task 4
Facility understands the process and supporting agreements (e.g., related to worker’s compensation, liability) for sharing staff with other facilities in need, including staffing of alternate care sites.
Function 11. Administration/Legal Issues
Notes and Resources
See Chapter 3 for a more detailed discussion.
Task 1
Administration (including corporate administration outside of the facility) examines its delegation-of-authority processes and makes any changes necessary to ensure that CSC decisions are supported (i.e., that facility decision makers are acting with the support of administration).
Task 2
Administration understands relevant changes to facility authorities and protections when state declarations of emergency/public health emergency are made, including legal protections or obligations for medical providers (e.g., duty to serve).
Task 3
Laws and regulations that would constrain the institution’s ability to implement CSC plans and possible solutions are discussed/identified. (This may be a regional process.)
Core Functions of the Outpatient Sector in CSC Planning and Implementation
Home Care/Medical Equipment Vendors (referred to as “Home Care")
Function 1. Alerting
Task 1
Home care agencies are able to receive and manage alerts from public safety, corporate administration, public health agencies (health alert network), and the National Weather Service as appropriate.
Task 2
Emergency response plan provides triggers and process for supervisor (incident commander if ICS used) to activate the surge capacity/ CSC plan and indicators (if applicable) to prompt consideration of activation.
Function 2. Notification
Task 1
Able to alert staff within and external to the agency, including health care system partners as appropriate.
Task 2
Staff understand what they are to do in a disaster, and appropriate notification policies are in place.
Function 3. Command
Task 1
Emergency response plan accounts for
• understanding the organization and authorities of the incident management structure,
• training and exercising with key staff on the disaster response plan/crisis plan,
• familiarizing command staff with incident action planning principles, and
• appropriate resources (job aids) being available to guide disaster decisions.
Function 4. Control
Task 1
Command staff understand the interface for resource requests (as well as any existing plans for resource triage/allocation) with local public health/emergency management agencies and/or local health coalitions as applicable.
Task 2
Command staff understand the processes for sheltering, relocation, and evacuation in response to threats to the agency, including facility assessment (includes suspension of services because of unsafe delivery conditions).
Task 3
Command staff understand options for community law enforcement support for their personnel during a disaster if required.
Task 4
Agency plan reflects a phased expansion of surge capacity/capabilities for conventional, contingency, and crisis care conditions.
Function 5. Communications
Task 1
Agency has policies and procedures in place for sharing situational updates with staff and clients (optimally redundant strategies in case of power or other system failures).
Task 2
Agency has the ability to communicate with (as appropriate)
• the local emergency operations center,
• the local/regional health and medical multiagency coordination center (as applicable), and
• other partner agencies/facilities in the area.
Function 6. Coordination
Task 1
Command staff understand the policy interface between the agency and local public health and emergency management agencies and local/regional hospital coalitions.
Task 2
If agency is part of a health care system, plans document the integration of agency response with the corporate response structure and processes.
Task 3
Agency has a plan for coordinating the scope of home care services provided with other home care agencies to avoid significant inconsistencies.
Function 7. Public Information
Notes and Resources
See http://www.fema.gov/emergency/nims/ PublicInformation.shtm.
Task 1
Agency provides information to the JIS for public dissemination as appropriate to its services.
Function 8. Operations
Notes and Resources
Conventional, Contingency, and Crisis Care Conditions
Task 1
Under contingency care conditions, command and unit staff can implement strategies for supply substitution, conservation, and adaption; extension of staff responsibilities; and patient care strategies (which patients will receive services depending on demand).
Task 2
Under CSC conditions, same as under contingency care conditions, but expanded options to include
• reuse and reallocation of supplies (e.g., triage of home oxygen supplies),
• changes in staff roles,
• increased family provision of care and necessary education,
• provision/facilitation of palliative care,
The mental health section of Chapter 4 provides a more detailed discussion.
The palliative care section in Chapter 4 provides a more detailed discussion.
• resource allocation and triage decisions and interface with any regional triage teams/regional disaster medical advisory committees, and
• adjustments to patient care protocols according to circumstances.
Mental Health Care
Task 1
Understand how to access local mental health system resources.
Task 2
A mental health triage system for at-risk patients, co-workers, and selftriage (for example, PsySTART) is in place.
Task 3
Staff are trained in psychological first aid to support at-risk patients, co-workers, and themselves.
Palliative Care
Task 1
Agency has planned for adequate symptomatic management (analgesia, antiemetics, anxiolytics) for clients (including those that will not receive other treatment modalities).
Task 2
Palliative care is addressed in the emergency operations plan, including palliative care resources, the physician decision-making process, education, and any agency-specific procedures.
Task 3
Palliative care training (including just-in-time training) is developed and performed according to the agency plan.
Function 9. Logistics
Notes and Resources
See http://www.health.state.mn.us/oep/healthcare/scarce/index.html.
Staffing
Task 1
Call-back criteria and policies are in place, including maintenance of current employee contact information.
Task 2
Agency assesses the number of staff potentially available for large- scale incidents, anticipating limits due to community access problems (e.g., flooded roads), family obligations, or employee illness.
Supplies
Task 1
Identify key potential scarce resources based on types of incidents and to the degree possible stockpiles or identify alternative sources for these supplies (e.g., home oxygen concentrators, oxygen tanks for use during power failures).
Task 2
For highly vulnerable supplies, identify strategies for appropriate substitution, conservation, adaptation, reuse, and reallocation.
Task 3
For local or state cached supplies (such as a local pharmaceutical cache) or SNS supplies, agency understands the process for request, receipt, and distribution of these supplies.
Special Considerations
Task 1
Patient groups requiring special consideration are identified and, to the degree possible, equipment and supplies to address the needs of these groups are purchased and/or stockpiled in relation to the agency’s size and role in the community. Includes (but is not limited to)
• pediatric patients;
• need for isolation/infection control;
• patients with functional limitations (e.g., hearing or visually impaired); and
• patients needing dialysis/renal replacement therapy.
Task 2
Agency understands any regional plans or resources for specific groups (e.g., pediatric-specific disaster supplies, regional pediatric or dialysis networks) and its role in such plans.
Function 10. Planning
Task 1
Agency is aware of the role of the state or regional disaster medical advisory committees and understands how to receive information from those bodies (or communicate with them if applicable).
Task 2
Agency (or partner) has a plan for the clinical care committee or technical experts to review current response strategies and make modifications based on evolving information during a long-term incident.
Task 3
Policies for altered shift lengths and staff roles are examined, and any collective bargaining issues are identified, if not addressed.
Task 4
Use of nontraditional assistance (family members, volunteers, Medical Reserve Corps providers) to provide care is addressed as needed within the emergency operations plan.
Task 5
Orientation, mentoring, education, and clinical care policies for nonagency supplemental staff are anticipated (e.g., Medical Reserve Corps).
Task 6
Agency understands the process and supporting agreements (e.g., related to worker’s compensation, liability) for sharing staff with other agencies or facilities in need, including staffing of alternate care sites.
Function 11. Administration/Legal Issues
Notes and Resources
See Chapter 3 for more detailed discussion.
Task 1
Administration (including corporate administration outside of the facility) examines its delegation of authority to incident commanders during a disaster and makes any changes necessary to ensure that CSC decisions are supported (i.e., that the incident commander is acting with the authority of the agency). During a crisis, administration may require additional communications and coordination with the incident commander.
Task 2
Administration understands relevant changes to agency authorities and protections when state declarations of emergency/public health emergency are made, including legal protections or obligations for medical providers (e.g., duty to serve).
Task 3
Agency and/or corporate legal counsel are aware of surge capacity/ CSC plans and implications for patient care (e.g., plans to triage the provision of home care or of medical resources).
Task 4
Legal counsel identifies state and local laws and regulations that would constrain CSC plans and possible solutions (this may be a regional analysis).
Core Functions of the Outpatient Sector in CSC Planning and Implementation
Alternate Care Systems (ACS)
Function 1. Alerting
Task 1
Public health and health care coalitions (at a minimum—likely also includes emergency management and EMS) identify a multiagency coordination (MAC) group prior to an incident that can assess and address the need for alternate care sites.
Task 2
Process (and triggers and indicators, as applicable) for alerting the
medical advisory committee is defined in emergency operations plans at the agency, coalition, and jurisdiction levels according to local plans.
Function 2. Notification
Notes and Resources
Institution should at least annually test notification systems and ensure that up-to-date contact information is available.
Task 1
MAC group has a notification mechanism (including a redundant mechanism in case of failure of the primary mechanism) for informing stakeholders of activation/demobilization of Alternate Care Systems (ACS), including
• EMS;
• hospital coalitions/partner health care facilities;
• regional disaster medical advisory committee/clinical care committee members; and
• appropriate technical experts (including those in toxicology, radiation safety, infectious disease, critical care, emergency medicine, trauma surgery, blood banking, dialysis, pediatrics, and burn surgery as required).
Task 2
Expectations of involved agencies and technical experts are understood prior to an incident, and appropriate activation/notification policies are in place.
Function 3. Command
Task 1
Public health takes a leadership role in ESF-8 (Health and Medical) at the local and state levels to assess available resources vs. actual or potential demand, and to implement public alternate care systems as required to supplement the usual health care system and any private (health care organized) alternate care sites.
Task 2
A NIMS-compliant ICS is utilized to coordinate ESF-8 assets. Includes
• use of unified command when no one agency has the lead role (e.g., public health and hospital system);
• an understanding of where technical specialists, the clinical care committee, and the triage team fit into the incident management structure;
• training and exercises with key staff;
• use of incident action planning and planning section functions during longer-term incidents; and
• appropriate resources (job aids) to guide decisions regarding ACS.
Task 3
Public agencies (public health, emergency management) understand their authorities to initiate ACS within the community at public sites
(private sites are established by the health care facilities that operate them).
Function 4. Control
Task 1
MAC group and ACS site staff understand the interface for resource requests and the acquisition process (as well as any existing plans for resource triage/allocation) with local and state emergency management.
Task 2
Emergency management agreements/plans reflect how public health and health care facilities support sheltered populations with medical needs.
Task 3
ACS site staff understand the need for security/access controls and community law enforcement support options as appropriate.
Task 4
ACS options reflect a phased expansion of surge capacity/capabilities for conventional, contingency, and crisis care situations (from electronic to augmented services at private and public sites).
Task 5
MAC group has a process for ongoing incident analysis to maintain situational awareness and facilitate ACS decisions.
Function 5. Communications
Task 1
Public health agencies have policies and procedures for exchanging situational updates with hospitals/outpatient care facilities, EMS, and emergency management.
Task 2
MAC group/center has a means of communicating with key stakeholders (including those listed under Function 2, Task 1) to maintain incident communications (including redundant communications mechanisms as required).
Function 6. Coordination
Task 1
MAC group understands the interfaces among local public health and emergency management agencies and local/regional hospital coalitions, including existing agreements.
Task 2
MAC group understands the function of the state disaster medical
advisory committee and any regional medical coordination center or regional disaster medical advisory committees, and can activate/ facilitate regional groups according to local plans.
Function 7. Public Information
Notes and Resources
See http://www.fema.gov/emergency/nims/PublicInformation.shtm.
Task 1
MAC group ensures that appropriate risk communications relevant to ACS are developed for the public regarding when and where to seek care (e.g., traditional media, websites, calling programs, e-mail, social media). This includes the ability to reach key cultural groups served by ACS.
Task 2
MAC group or public health agencies coordinate information with other agencies and participate in JIS and JIC activities when implemented by the jurisdiction, state, or coalition.
Function 8. Operations
Task 1
Local/state public health agencies maintain an inventory of usual and surge medical resources.
Task 2
Local/state public health agencies understand private/public ACS capacities to augment health system capacity, including
• telephone hotlines and other “electronic care” (including coordination with private and public safety answering points);
• ambulatory care ("flu centers” or triage/casualty collection points); and
• nonambulatory care (shelter-based care, hospital overflow, federal medical station integration, limited emergency/surgical care).
Task 3
For each of these public sites (or for similar sites that are incident specific) MAC group understands the activation process (and any authorities or agreements involved).
Task 4
Plans are made for patient registration, tracking, and record keeping, including access to and storage of medical records.
Task 5
Plans are made for laboratory and pharmacy services appropriate to the site, including clinical ordering and results systems.
Task 6
Scope of clinical operations is defined and modified according to the evolving needs of the incident and the supplies available.
Task 7
ACS site has staff trained to provide psychological first aid to patients/ evacuees, can implement psychological triage processes (such as PsySTART) as required, and has a referral/management plan for those with acute mental health needs.
Task 8
ACS policies and education address the provision of palliative care (either on site or facilitated in the home environment).
Function 9. Logistics
Staffing
Task 1
Local public health agencies identify sources of potential staffing (e.g., health care systems/coalitions, Medical Reserve Corps, EMS) for the various types of public ACS sites.
Task 2
ACS credentialing policies and procedures are congruent with applicable regulations and statutes.
Task 3
Plans are made for staff orientation, education, and supervision.
Task 4
Capacity of nontraditional resources (family members, volunteers) to provide nonmedical care is examined and addressed as needed within the ACS operations plan.
Task 5
Legal liability, worker’s compensation, compensation, and other issues are addressed according to the source of the staff (e.g., hospital, volunteer, MAC group).
Supplies
Task 1
Supply lists for each type of ACS (shelter, ambulatory, nonambulatory) are developed, optimally, including the source of initial supply and resupply.
Task 2
Emergency management and public health agencies, health care facilities, and medical supply vendors understand their role in the ACS setup, resupply, and delivery processes.
Task 3
For local or state cached supplies (such as a local pharmaceutical cache) or SNS supplies, MAC group/ACS facility understands the process for request, receipt, and distribution of these supplies.
Space
Task 1
Health care facilities identify privately owned spaces for ACS establishment on site or at other owned and modified sites.
Task 2
Public health and emergency management agencies identify public spaces for major ACS facilities and establish any necessary agreements or authorities required to utilize them (recognizing that no-notice incidents may require ACS sites at ad hoc locations).
Special Considerations
Task 1
Patient groups requiring special consideration are identified, and, to the degree possible, equipment and supplies to address the needs of these groups are purchased and/or stockpiled in relation to the expected size of the alternate care site, potentially including
• pediatric patients,
• patients with behavioral and cognitive impairment,
• the need for isolation/infection control, and
• the need for contamination assessment (post-HAZMAT or radiological dispersal device with population-based exposure).
Task 2
Facility understands any regional plans or resources for specific groups (e.g., pediatric-specific disaster supplies, regional pediatric or dialysis networks) and the ACS site’s role in these plans.
Function 10. Planning
Task 1
Technical specialists are available as needed to provide input on infection control, clinical care, and other issues arising at the ACS site. This may include input from the regional or state disaster medical advisory committee.
Task 2
Planning section maintains situational awareness and modifies clinical care guidelines or supply/staffing requests to meet demand/anticipated demand.
Task 3
Planning section addresses policy modifications and demobilization based on incident demands.
Function 11. Administration
Notes and Resources
See Chapter 4 for a more detailed discussion.
Authority
Task 1
Public health and emergency management examine their delegation of authority to public ACS site incident commanders during a disaster and make any changes necessary to ensure that CSC decisions to open an ACS site are supported (i.e., that the incident commander is acting with the authority of the agency and any necessary political entities). During a crisis, the administration may require additional communications and coordination with the incident commander.
Task 2
Public health and emergency management agencies understand their authorities to open and provide ACS services, including the ability to facilitate private ACS sites through use of regulatory relief and emergency orders.
Regulatory and Legal Issues
Task 1
Health care facilities and emergency management agencies understand relevant changes to agency/facility authorities and protections when state declarations of emergency/public health emergency are made, including legal protections or obligations for medical providers (e.g., duty to serve).
Task 2
Agency heads/political leaders are aware of surge capacity/CSC plans and implications for patient care, including ACS sites.
Task 3
Legal counsel identify state and local laws and regulations that would constrain public and private ability to open ACS sites and potential relief mechanisms.
Core Functions of the Outpatient Sector in CSC Planning and Implementation
Out-of-Hospital Providers
Function 1. Notification
Task 1
Providers ensure that up-to-date contact information and acknowledgment of receipt of exercise and incident messaging are provided to employers (and any other relevant groups, such as the MRC).
Function 2. Command, Control, Communications, and Coordination
Task 1
When a disaster occurs that affects the providers’ facility/agency, providers understand where they report, to whom they answer, and how to execute their roles. They also understand the range of their potential roles within the rest of the health care system and opportunities for volunteer assignment (for example, reassignment to an alternate care site or a hospital within the corporate system).
Task 2
Providers know how to contact and provide situational updates to and/ or request resources from their administrator/emergency operations center/command center as applicable to the facility/agency plan.
Task 3
Providers receive incident command training appropriate to their role in the command structure, including
• knowledge of the location of plans and actions for the full continuum of care in their area, including the use of crisis spaces and staffing; and
• understanding of appropriate resources (job aids) to guide capacity expansion decisions or other unit-based plans.
Function 3. Public Information
Task 1
Providers understand key sources of facility/community information in a disaster (e.g., web, social media, e-mail, hotline).
Function 4. Operations
Notes and Resources
See the ethics section of Chapter 4.
Task 1
Providers understand facility-based actions during expansion of care from conventional to crisis (e.g., expanded facility hours, scheduling changes, triage of appointments, use of ancillary spaces).
Task 2
Providers are prepared to perform triage as it relates to their role (may involve triage of appointments, or may involve another triage role within their system, such as telephone triage).
Task 3
Providers likely to perform triage (both reactive and proactive) understand the criteria they may consider (as well as what not to consider) when making triage decisions.
See the mental health and palliative care sections of Chapter 4 for a more detailed discussion.
Task 4
Providers understand sources of employee mental health support.
Task 5
Providers understand normal stress reactions and coping mechanisms, as well as danger signs, and receive training in psychological first aid and psychological triage appropriate for their roles.
Task 6
Providers understand their potential role in providing/facilitating palliative care during a disaster.
Function 5. Logistics
Task 1
Providers understand the utilization of space in their facility and other expansion plans that involve their department/unit.
Task 2
Providers understand how their unit staffing and hours may change during a disaster.
Task 3
Providers understand how their role may be changed/expanded during a crisis, including incorporation of staff from outside the unit or facility, and any potential roles at other sites within their health system (if applicable).
Task 4
Providers understand how record keeping and other duties may change in crisis situations (e.g., where to find and how to use paper forms).
Task 5
Providers understand the process for requesting necessary clinical resources during an incident.
Function 6. Legal Issues
Notes and Resources
Chapter 3 provides a more detailed discussion.
Task 1
Providers understand legal obligations and liabilities for practice both within and outside of their facility/agency when
• a disaster or public health emergency has been declared,
• a disaster or public health emergency has not been declared, and See the mental health and palliative care sections of Chapter 4 for a more detailed discussion.
• when providing other disaster relief functions (for example, if serving as a Medical Reserve Corps or disaster medical assistance team member).
AAFP (American Academy of Family Physicians). 2012. Disaster recovery and response. Leawood, KS: AAFP, http://www.aafp.org/online/etc/medialib/aafp_org/documents/clinical/bt/resouces/disasterrecovery.Par.0001.File.dat/DisasterRecovery.pdf (accessed February 27, 2012).
AAP (American Academy of Pediatrics). 2011. Disaster preparedness for pediatric practices: An online tool. http://practice.aap.org/disasterpreptool.aspx (accessed February 27, 2012).
AHAF (American Health Assistance Foundation). 2012. The facts on Alzheimer’s disease. http://www.ahaf.org/alzheimers/about/understanding/facts.html (accessed February 27, 2012).
AHRQ_(Agency for Healthcare Research and Quality). 2004. Rocky Mountain regional care model for bioterrorist events: Locate alternate care sites during an emergency. Publication No. 04-0075. Rockville, MD, http://archive.ahrq.gov/research/altsites.htm (accessed February 27, 2012).
AHRQ. 2005. Health Emergency Assistance Line and Triage Hub (HEALTH model). http://archive.ahrq.gov/research/health/ (accessed February 27, 2012).
AHRQ. 2007a. Nursing homes in public health emergencies: Special needs and potential roles. Publication No. 07-0029-1. Rockville, MD: AHRQ, http://archive.ahrq.gov/prep/nursinghomes/nhomerep.pdf (accessed February 27, 2012).
AHRQ. 2007b. Providing mass medical care with scarce resources: A community planning guide, edited by Phillips, S. J., and A. Knebel. Publication no. 07-0001. Rockville, MD: AHRQ, http://archive.ahrq.gov/research/mce/ (accessed March 4, 2012).
AHRQ. 2007c. Adapting community call centers for crisis support. http://archive.ahrq.gov/prep/callcenters/callcenters.pdf (accessed February 27, 2012).
AHRQ.2009. Disaster alternate care facilities: Selection and operation. Publication no. 09-0062. Rockville, MD: AHRQ, http://archive.ahrq.gov/prep/acfselection/dacfrep.htm (accessed February 27, 2012).
AHRQ. 2011. Home health patient assessment tools: Preparing for emergency triage. Publication no. 11-M020-EF. Rockville, MD: AHRQ, http://archive.ahrq.gov/prep/homehealth/homehealth.pdf (accessed February 27, 2012).
The American Geriatrics Society Foundation for Health in Aging. Undated. Nursing home care. http://www.healthinaging.org/agingintheknow/chapters_print_ch_trial.asp?ch=15#Lives (accessed May 30, 2009).
APIC (Association for Professionals in Infection Control and Epidemiology, Inc.). 2009. Infection Prevention for Alternate Care Sites—APIC. Washington, DC: APIC, http://www.mintie.com/assets/pdf/education/APIC%20IP%20for%20ACS%202009.pdf (accessed February 27, 2012.
ASPR (Assistant Secretary for Preparedness and Response). 2011a. Disaster Mortuary (OperationalResponse Teams (DMORTs). Washington, DC: HHS (Department of Health and Human Services), http://www.phe.gov/Preparedness/responders/ndms/teams/Pages/dmort.aspx (accessed February 27, 2012).
ASPR. 2011b. About ESAR-VHP. http://www.phe.gov/esarvhp/pages/default.aspx (accessed March 5, 2012).
ASPR. 2012. Federal Medical Station (FMS). Washington, DC: HHS, http://www.phe.gov/Preparedness/support/medicalassistance/Pages/default.aspx#fms (accessed February 27, 2012).
Bar-Dayan, Y., A. Leiba, P. Beard, D. Mankuta, D. Enselhart, Y. Beer, M. Lvnn, Y. Weiss, G. Martonovits, P. Benedek, and A. Goldberg. 2005. A multidisciplinary field hospital as a substitute for medical hospital care in the aftermath of an earthquake: The experience of the Israeli Defense Forces field hospital in Duzce, Turkey 1999. Prehospital Disaster Medicine 20(2):103-106.
Bar-On, E., E. Lebel, Y. Kreiss, O. Merin, S. Benedict, A. Gill, E. Lee, A. Pirotsky, T. Shirov, and N. Blumberg. 2011. Orthopaedic management in a mega mass casualty situation: The Israel Defense Forces field hospital in Haiti following the January 2010 earthquake. Injury 42(10):1053-1059.
Bisson, J. I., P. L. Jenkins, J. Alexander, and C. Bannister. 1997. Randomized controlled trial of psychological debriefing for victims of acute burn trauma. British Journal of Psychiatry 171:78-81.
Bisson, J. I., M. Brayne, F. M. Ochberg, and G. S. Everly. 2007. Early psychosocial intervention following traumatic events. American Journal of Psychiatry 164(7):1016-1019.
Blackwell, T., and M. Bosse. 2007. Use of an innovative design mobile hospital in the medical response to Hurricane Katrina. Annals of Emergency Medicine 49(5):580-588.
Burnweit, C., and S. Stylianos. 2011. Disaster response in a pediatric field hospital: Lessons learned in Haiti. Journal of Pediatric Surgery 46(6):1131-1139.
California Emergency Medical Services Authority. 2007. Disaster Medical Services Division—Hospital Incident Command System (HICS). http://www.emsa.ca.gov/hics/ (accessed February 27, 2012).
CBS News. 2009. Kids with H1N1 camp out at hospital. www.cbsnews.com/stories/2009/09/23/…/main5331312.shtml (accessed September 23, 2009).
CDC (Centers for Disease Control and Prevention). 2009a. 2009 H1N1 vaccination recommendations. Atlanta, GA: CDC, http://www.cdc.gov/h1n1flu/vaccination/acip.htm (accessed February 27, 2012).
CDC. 2009b. Pandemic influenza pediatric office plan template: Product of a pediatric healthcare response to pandemic H1N1 influenza stakeholder meeting. Atlanta, GA: CDC, http://www.bt.cdc.gov/healthcare/pdf/pediatric_office_plan.pdf (accessed February 27, 2012).
Chung, S., S. Monteiro, T. Hogencamp, F. J. Damian, and A. Stack. 2011. Pediatric alternate site of care during the 2009 H1N1 pandemic. Pediatric Emergency Care 27(6):519-526.
Cinti, S. K., W. Wilkerson, J. G. Holmes, J. Shlafer, C. Kim, C. D. Collins, K. Bandy, F. Krupansky, M. Lozon, S. A. Bradin, C. Wright, J. Goldberg, D. Wagner, P. Rodgers, J. Atas, and B. Cadwallender. 2008. Pandemic influenza and acute care centers: Taking care of sick patients in a nonhospital setting. Biosecurity and Bioterrorism: Biodefense Strategy, Practice, and Science 6(4):335-344.
CMS (Centers for Medicare & Medicaid Services). 2009. Hospital alternative care sites during H1N1 public health emergency. http://www.cms.gov/H1N1/Downloads/AlternativeCareSiteFactSheet.pdf (accessed February 27, 2012).
Cone, D. C., S. D. Weir, and S. Bogucki. 2003. Convergent volunteerism. Annals of Emergency Medicine 41:457-462.
Cruz, A. T., B. Patel, M. C. DiStefano, C. R. Codispoti, J. E. Shook, G. J. Demmler-Harrison, and P. E. Sirbaugh. 2010. Outside the box and into thick air: Implementation of an exterior mobile pediatric emergency response team for North American H1N1 (swine) influenza virus in Houston, Texas. Annals of Emergency Medicine 55(1):23-31.
D’Amore, A. R., and C. K. Hardin. 2005. Air Force Expeditionary Medical Support Unit at the Houston floods: Use of a military model in civilian disaster response. Military Medicine 170(2):103.
DOD (Department of Defense). 2001a (December 1). Acute care center: A mass casualty care strategy for biological terrorism incidents. Washington, DC: DOD, http://www.ecbc.army.mil/downloads/bwirp/ECBC_acc_blue_book.pdf (accessed February 13, 2012).
DOD. 2001b (May 1). Neighborhood emergency help center: A mass casualty care strategy for biological terrorism incidents. Washington, DC: DOD, http://disasterhelp.net/resources/nehc_green_book.pdf (accessed February 13, 2012).
FEMA (Federal Emergency Management Agency). 2011a. NIMS resource center. http://www.fema.gov/emergency/nims/ (accessed February 27, 2012).
FEMA. 2011b. Public information. http://www.fema.gov/emergency/nims/PublicInformation.shtm (accessed February 27, 2012).
FEMA and Emergency Management Institute. 2008. National Incident Management System independent study 701—Multi-Agency Coordination System (MACS) course. Emmitsburg, MD: FEMA. http://training.fema.gov/EMIWeb/IS/is701.asp (accessed July 31, 2008).
Greenwald, P. W., A. F. Rutherford, R. A. Green, and J. Giglio. 2004. Emergency department visits for home medical device failure during the 2003 North America blackout. Academic Emergency Medicine 11(7):786-789.
Hall, M. J., C. J. DeFrances, S. N. Williams, A. Golosinskiy, and A. Schwartzman. 2010. National hospital discharge survey: 2007 summary. Report no. 29. Hyattsville, MD: National Center for Health Statistics.
HHS (Department of Health and Human Services). 2011. Guidance for integrating culturally diverse communities into planning for and responding to emergencies: A toolkit. Washington, DC: HHS Office of Minority Health, http://www.hhs.gov/ocr/civilrights/resources/specialtopics/emergencypre/omh_diversitytoolkit.pdf (accessed January 11, 2012).
Hick, J. L., D. Hanfling, J. Burstein, C. DeAtely, D. Barbisch, G. Bogdan, and S. Cantrill. 2004. Healthcare facility and community strategies for patient care surge capacity. Annals of Emergency Medicine 44:253-261.
IASC (Inter-Agency Standing Committee). 2007. IASC guidelines on mental health and psychological support in emergency settings. Geneva, Switzerland: IASC.
JCAHO (Joint Commission on Accreditation of Healthcare Organizations). 2005. Surge hospitals: Providing safe care in emergencies. Oakbrook Terrace, IL: JCAHO, http://www.jointcommission.org/assets/1/18/surge_hospital.pdf (accessed February 27, 2012).
Kellermann, A. L., A. P. Isakov, R. Parker, M. T. Handrigan, and S. Foldy. 2010. Web-based self-triage of influenza-like illness during the 2009 H1N1 influenza pandemic. Annals of Emergency Medicine 56(3):288-294.
Kopp, J. B., L. K. Ball, A. Cohen, R. J. Kenney, K. D. Lempert, P. E. Miller, P. Muntner, N. Qureshi, and S. A. Yelton. 2007. Kidney patient care in disasters: Emergency planning for patients and dialysis facilities. Clinical Journal of the American Society of Nephrology 2(4):825-838.
Kreiss, Y., O. Merin, K. Peleg, G. Levy, S. Vinker, R. Sagi, A. Abargel, C. Bartal, G. Lin, A. Bar, E. Bar-On, M. J. Schwaber, and N. Ash. 2010. Early disaster response in Haiti: The Israeli field hospital experience. Annals of Internal Medicine 153(1):45-48.
Lam, C., R. Waldhorn, E. Toner, T. V. Inglesby, and T. O’Toole. 2006. The prospect of using alternative medical care facilities in an influenza pandemic. Biosecurity and Bioterrorism: Biodefense Strategy, Practice, and Science 4(4):384-390.
McNally, R. J., R. A. Bryant, and A. Ehlers. 2003. Does early psychological intervention promote recovery from posttraumatic stress? Psychological Science in the Public Interest 4(2):45-79.
Medical Reserve Corp. 2011. Homepage of the Division of the Civilian Volunteer Medical Reserve Corps. http://www.medicalre-servecorps.gov/HomePage (accessed March 5, 2012).
Merin, O., N. Ash, G. Levy, M. J. Schwaber, and Y. Kreiss. 2010. The Israeli field hospital in Haiti: Ethical dilemmas in early disaster response. New England Journal of Medicine 362(11):e38.
NACCHO (National Association for County and City Health Officials). 2008. Alternative methods of dispensing: Model highlights. Washington, DC: NACCHO, http://www.naccho.org/topics/emergency/SNS/upload/POD-Article-5_nonlinear.pdf (accessed February 27, 2012).
National Commission on Children and Disasters. 2009. National Commission on Children and Disasters homepage. http://www.chiildrenanddisasters.acf.hhs.gov (accessed November 29, 2011).
Nicogossian, A. E., and C. R. Doarn. 2011. Armenia 1988 earthquake and telemedicine: Lessons learned and forgotten. Telemedicine Journal and E-Health 17(9):741-745.
NIMH (National Institute of Mental Health). 2002. Mental health and mass violence: Evidence-based early psychological intervention for victims/survivors of mass violence. A workshop to reach consensus on best practices. NIH publication no. 02-5138, Washington, DC: U.S. Government Printing Office.
NYCDHMH (New York City Department of Health and Mental Hygiene). 2007. Preparedness focus areas: Pediatric preparedness. New York: NYCDHMH, http://www.nyc.gov/html/doh/html/bhpp/bhpp-focus-ped-toolkit.shtml (accessed November 29, 2011).
Rebmann, T., B. Citarella, D. S. Subramaniam, and D. P. Subramaniam. 2011. A home health agency’s pandemic preparedness and experience with the 2009 H1N1 pandemic. American Journal of Infection Control 39(9):725-731.
Rhodas, E.. A. Vicuna, and R. C. Merrell. 2005. Intermittant and mobile surgical services: Logistics and outcomes. World Journal of Surgery 29(10):1335-1339.
Ruggiero, K. J., H. S. Resnick, R. Acierno, S. F. Coffey, M. J. Carpenter, A. M. Ruscio, R. S. Stephens, D. G. Kilpatrick, P. R. Stasiewicz, R. A. Roffman, M. Bucuvalas, and S. Galea. 2006. Internet-based intervention for mental health and substance use problems in disaster-affected populations: A pilot feasibility study. Behaviour Research and Therapy 37(2)190-205.
Schappert, S. M., and E. A. Rechtsteiner. 2011. Ambulatory medical care utilization estimates for 2007. Vital and Health Statistics 13(169):1-38.
Schreiber, M., and S. Shields. 2012. Anticipate, Plan, and Deter: Building resilience in emergency health responders. Presented at the 2012 NACCHO (National Association of City and County Health Officials) Public Health Preparedness Summit, Anaheim, California.
Schreiber, M., R. Gurwitch, and M. Wong. 2006. “Listen, Protect, and Connect—Model & Teach” psychological first aid for children. Washington, DC: FEMA, http://www.ready.gov/sites/default/files/documents/files/PFA_SchoolCrisis.pdf (accessed February 27, 2012).
Schreiber, M., B. Pfefferbaum, L. Sayegh, and J. Coady. In press. The way forward: The national children’s disaster mental health concept of operations. Disaster Medicine and Public Health.
Schultz, C. H., K. L. Koenig, and E. K. Noji. 1996. A medical disaster response to reduce immediate mortality after an earthquake. New England Journal of Medicine 34(7):438-444.
Sills, M. R., M. Hall, H. K. Simon, E. S. Fieldston, N. Walter, J. E. Levin, T. V. Brogan, P. D. Hain, D. M. Goodman, D. D. Fritch-Levens, D. B. Fagbuyi, M. B. Mundorff, A. M. Libby, H. O. Anderson, W. V. Padula, and S. S. Shah. 2011. Resource burden at children’s hospitals experiencing surge volumes during the spring 2009 H1N1 influenza pandemic. Academic Emergency Medicine 18(2):158-166.
Skidmore, S., W. Wall, and J. Church. 2003. Modular emergency medical system: Concept of operations for the acute care center(ACC). Mass casualty strategy for a biological terror incident. http://disasterhelp.net/resources/acc_conops.pdf (accessed February 27, 2012).
State of California. 2012a. Development of standards and guidelines for healthcare surge during emergencies—alternate care sites [draft text]. http://bepreparedcalifornia.ca.gov/NR/rdonlyres/3C71BC63-5B32-486E-A66F-917CC53E9A77/0/DraftAltCareSitesWTO.pdf (accessed February 27, 2012).
State of California. 2012b [draft text]. Government-authorized alternate care site operational tools manual. http://bepreparedcalifornia.ca.gov/NR/rdonlyres/C2AD6528-F781-4D8C-B900-828A1C2C6F0C/0/Operational_ACS_Ops_Tool_FINAL.pdf (accessed February 27, 2012).
U.S. Census Bureau. 2006. Profile America facts for features. Washington, DC: U.S. Census Bureau, http://www.census.gov/newsroom/releases/archives/facts_for_features_special_editions/cb06-ff10-2.html (accessed February 27, 2012).






























































