
Ensuring that members of society are healthy and reaching their full potential requires the prevention of disease and injury; the promotion of health and well-being; the assurance of conditions in which people can be healthy; and the provision of timely, effective, and coordinated health care. A wide array of actors across the United States—including those in both primary care1 and public health—contribute to one or more of these elements, but their work is often carried out in relative isolation. Achieving substantial and lasting improvements in population health2 will require a concerted effort from all of these entities, aligned with a common goal. The integration of primary care and public health could enhance the capacity of both sectors to carry out their respective missions and link with other stakeholders to catalyze a collaborative, intersectoral movement toward improved population health.
In recognition of this potential, the Health Resources and Services Administration (HRSA) and the Centers for Disease Control and Prevention (CDC) requested that the Institute of Medicine (IOM) convene a committee of experts to examine the integration of primary care and public health. The 17-member Committee on Integrating Primary Care and Public Health comprises experts in primary health care, state and local public health, service
_________________
1The committee recognizes that mental health is an inextricable part of primary care. When primary care is discussed in this report, the committee means it to be inclusive of mental health.
2When discussing the term “population health,” the committee chose to adopt Kindig and Stoddart’s definition (2003, p. 381): “the health outcomes of a group of individuals, including the distribution of such outcomes within the group.”
integration, health disparities, health information technology, health care finance, health care policy, public health law, workforce education and training, organizational management, and child health. The committee was charged to:
• Identify the best examples of effective public health and primary care integration and the factors that promote and sustain these efforts. These examples were to illustrate shared accountability; workforce integration; collaborative governance, financing, and care coordination; and the effective use of information technology to promote integration and achieve high-quality primary care and public health.
• Examine ways by which HRSA and CDC can use provisions of the Patient Protection and Affordable Care Act (ACA) to promote the integration of primary care and public health.
• Discuss how HRSA-supported primary care systems and state and local public health departments can effectively integrate and coordinate to improve efforts directed at cardiovascular disease prevention, as well as other issues relevant to health disparities or specific populations, such as maternal and child health and colorectal cancer screening, and describe actions HRSA and CDC should take to promote these changes.
Funding for this study was provided by HRSA, CDC, and the United Health Foundation.
In conducting the study, the committee held five formal meetings, as well as three subgroup meetings, and used a variety of sources: the published literature, discussions with HRSA and CDC, presentations from practitioners, and commissioned papers. In drawing on these sources, the committee developed a list of key principles for the integration of primary care and public health, which are outlined below and discussed in detail in Chapter 2. These principles were used as a guiding framework in presenting examples of successful integration, identifying opportunities for interagency collaboration, and formulating the recommendations presented in this report.
KEY TERMS
Primary Care
The committee adopted an earlier IOM definition of primary care: “the provision of integrated, accessible health care services by clinicians who are accountable for addressing a large majority of personal health care
needs, developing a sustained partnership with patients, and practicing in the context of family and community” (IOM, 1996, p. 1). Primary care in the United States is delivered through both private providers and those supported by government agencies, such as the Veterans Health Administration and HRSA. HRSA-supported health centers serve over 19 million patients a year (HRSA, 2011) and provide a safety net for society’s most vulnerable populations. Although most primary care is delivered through the private sector, both private and government-supported primary care share common features: both are person-rather than disease-focused, provide a point of first contact for whatever people might consider a health or health care problem, are comprehensive, and coordinate care (Starfield and Horder, 2007).
Public Health
The committee adopted a definition of public health that likewise was borrowed from an earlier IOM report: “fulfilling society’s interest in assuring conditions in which people can be healthy” (IOM, 1988, p. 140). To meet this definition, public health has shifted its primary focus from addressing infectious disease to tackling chronic disease. To ensure healthy conditions, public health encompasses a diverse group of public and private stakeholders (including the health care delivery system) working in a variety of ways to contribute to the health of society. Uniquely positioned among these stakeholders is governmental public health. Because health departments are legally tasked with providing essential public health services, they are required to work with all sectors of the community. This allows them to serve as a catalyst for engaging multiple stakeholders to confront community health problems. In addition, their assessment and assurance functions put them in close contact with the community and in touch with the community’s health needs. While public health defined broadly in this report goes beyond governmental public health, the committee recognized that health departments play a fundamental role in creating healthy communities and focused on them when possible.
Integration
While integration can be an imprecise term, integration of primary care and public health was defined for this report as the linkage of programs and activities to promote overall efficiency and effectiveness and achieve gains in population health. The committee conceived of integration in terms of multiple variables—levels, partners, actions, and degree. For this report, the agency and local levels are discussed. Partners for the agency level include HRSA, CDC, and other agencies as necessary; partners for the local level
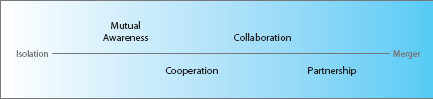
FIGURE S-1 Degrees of integration.
include a primary care entity, a public health entity (with a preference for health departments), the community, and other stakeholders as necessary. The variable of actions required a shared goal of improved population health; a willingness and ability to contribute to that goal; and, ideally, a commitment to an ongoing process and continual dialogue. Finally, the committee conceived of integration as degrees on a continuum ranging from isolation to merger (Figure S-1) and focused on mutual awareness, cooperation, collaboration, and partnership, with a preference for activities moving toward greater integration.
CONTEXT FOR INTEGRATION OF PRIMARY
CARE AND PUBLIC HEALTH
The opportunity currently exists to shift the health system in significant ways. A number of relatively new developments have converged to create this opportunity. The dramatic rise in health care costs has led many stakeholders to explore innovative ways of reducing costs and improving health. As health research continues to clarify the importance of social and environmental determinants of health and the impact of primary prevention, there is growing recognition that the current model of investment in the nation’s health system is unacceptable. At the same time, an unprecedented wealth of health data is providing new opportunities to understand and address community-level health concerns. And most important, the passage of the ACA presents an overarching opportunity to change the way health is approached in the United States.
This pivotal time makes it possible to achieve sustainable improvements in population health, a key goal for health system reform. Pursuit of this goal will require a balance of investment and clarity of roles across activities that address the broad determinants of health, population-level behaviors, and individual health care—activities in which primary care and public health have prominent roles.
Primary care and public health presently operate largely independently, but have complementary functions and the common goal of ensuring a
healthier population. By working together, primary care and public health can each achieve their own goals and simultaneously have a greater impact on the health of populations than either of them would have working independently. Each has knowledge, resources, and skills that can be used to assist the other in carrying out its roles. They should be viewed as “two interacting and mutually supportive components” of a health system designed to improve the health of populations (Welton et al., 1997, p. 262).
Among agencies within the Department of Health and Human Services (HHS), HRSA and CDC have especially important roles to play in improving population health. Both have articulated a vision of how their work can impact the broader determinants of health (Frieden, 2010; HRSA, 2010), and both see themselves as having a public health mission. HRSA plays a strategic role in helping to ensure access to personal health services for uninsured and vulnerable populations through its support for the provision of primary care and preventive services at health centers, Ryan White clinics, and rural health clinics, as well as training programs for the primary care and public health workforces and maternal and child health programs. And with its focus on health promotion, disease prevention, and preparedness, CDC is recognized as a global leader in public health. The agency works with local and state health departments on a number of efforts, including implementing disease surveillance systems, preventing and controlling infectious and chronic diseases, reducing injuries, eliminating workplace hazards, and addressing environmental health threats. It is significant that these agencies have come forward to pursue integration.
PRINCIPLES FOR INTEGRATION
To gain an understanding of current and recent efforts to integrate primary care and public health, the committee reviewed past integration efforts to identify some of the ways in which primary care and public health can interact, as well as the benefits of and barriers to successful collaboration. The committee gathered examples of integration by searching peer-reviewed journal and grey literature databases, querying relevant stakeholders, and drawing on its members’ own experiences. A thorough review of these examples revealed some prominent themes and lessons and made it possible to select case studies that reflect the major components of successful integration. The review informed the development of a set of principles that the committee believes are essential for successful integration of primary care and public health:
• a shared goal of population health improvement;
• community engagement in defining and addressing population health needs;
• aligned leadership that
— bridges disciplines, programs, and jurisdictions to reduce fragmentation and foster continuity,
— clarifies roles and ensures accountability,
— develops and supports appropriate incentives, and
— has the capacity to manage change;
• sustainability, key to which is the establishment of a shared infrastructure and building for enduring value and impact; and
• the sharing and collaborative use of data and analysis.
While the committee believes that all of these principles are ultimately necessary for integration, it also believes that integration can start with any of these principles and that starting is more important than waiting until all are in place.
EXAMPLES OF INTEGRATION
From the literature review, the committee identified a number of examples of successful integration efforts. These examples appear in a diverse array of communities and help demonstrate the breadth of possibilities for primary care and public health interactions. Drawing on these experiences, the committee derived some lessons about the composition and focus of recent efforts to integrate primary care and public health:
• In many of the examples, integration was driven by a specific health issue that was identified as a community area of concern, such as chronic disease, prevention, or the health needs of a specific population.
• Participants in integration initiatives varied widely, including an array of primary care and public health entities and other contributors, such as community organizations, academic institutions, businesses, and hospitals.
• Key opportunities for integration included the sharing and use of data and the development of a workforce capable of functioning in an integrated environment.
Through its review of the literature, the committee sought examples to use as case studies that would demonstrate well-developed relationships between public health and primary care. With these examples, the committee wished to highlight ongoing linkages between primary care and public health entities that extend beyond a single project, demonstrate a commitment to an ongoing relationship between the two disciplines, and reflect the
above principles for integration. The committee selected three communities to showcase:
• Durham, North Carolina;
• San Francisco, California; and
• New York, New York.
AREAS IN WHICH HRSA AND CDC CAN
STRENGTHEN INTEGRATION
To explore the potential for interagency collaboration to foster the integration of primary care and public health, the committee examined how HRSA-supported primary care systems and public health departments could integrate efforts in three specific areas: maternal and child health (specifically the Maternal, Infant, and Early Childhood Home Visiting Program), cardiovascular disease prevention, and colorectal cancer screening. These areas were selected because they lend themselves to a life-course perspective, include elements of mental and behavioral health, and touch on issues relevant to health disparities. They also represent a mix of programs led by HRSA and CDC.
In its review of these three areas (discussed in Chapter 3), the committee was struck by two things. First is the vastly different organizational structures of HRSA and CDC, which create logistical barriers to the formation of partnerships. These structural differences mean there often is no natural link between the agencies. This situation is not necessarily negative. In fact, like puzzle pieces that fit into place, these structural differences can actually assist in promoting better coordination. In the short run, however, the differences can mean that staff from one agency do not always have a natural counterpart in the other. Second, despite these barriers, there is a genuine willingness among the two agencies to work together.
The committee’s examination of the above three areas revealed some key ways in which integration can be encouraged. They include the value of using community health workers, the opportunities provided by data sharing, and the possibility of a third party to foster integration. The committee encourages HRSA and CDC to explore these possibilities in the three areas examined by the committee, as well as others.
POLICY AND FUNDING OPPORTUNITIES
Federal policy and funding are the greatest levers available to HRSA and CDC for encouraging the integration of primary care and public health on the ground. As the most ambitious health policy in a generation, the ACA provides an unusual opportunity to work toward that goal. While the
ACA does not explicitly address the integration of primary care and public health, it provides a menu of initiatives that agencies and communities can exploit to make gains in improving population health.
The ACA authorizes HRSA and CDC to launch a number of new programs that on their own merit promise to be noteworthy, but if coordinated and managed collaboratively from their inception could generate significant momentum in population health at the national, state, and local levels. Particularly promising provisions of the act (highlighted in Chapter 4) fall into four categories—community investments and benefits, coverage reforms, health care transformation, and reshaping the workforce. These provisions are summarized in Table S-1.
|
Affordable Care Act Provision |
HRSA and CDC Opportunities |
|
Community Transformation Grants (ACA §§ 4002 and 4201) The provision authorizes and funds community transformation grants to improve community health activities and outcomes. |
• Given that Community Transformation Grants can be viewed as the public health counterpart to the Centers for Medicare & Medicaid Services (CMS) Innovation Center (CMMI) pilots, HRSA and CDC should be aware of the communities where both of these programs are involved. • As community resources for wellness improve through the Transformation Grant system, it may be possible to encourage state and local health department recipients to develop linkages with primary care providers as a central focus of their program planning. • CDC could also begin to link those resources to CMMI pilots, which must be able to link their patients and physician practices with community resources. |
|
Community Health Needs Assessments (ACA § 9007) The provision amends the Internal Revenue Code by adding new section 501(r), “additional requirements for certain hospitals.” The new requirements apply to all facilities licensed as hospitals and organizations recognized by the Treasury secretary as hospitals and spell out new obligations for all hospitals seeking federal tax exempt status. |
• HRSA and CDC could engage with community hospitals and national hospital associations to develop approaches to hospital community benefit planning, as well as promote approaching jointly the selection of interventions and implementation strategies to address identified problems—for example, the extension of primary care services into nontraditional settings; the formation of collaboratives among community primary care providers and local public health and other agencies; and community health promotion activities involving diet, exercise, and injury risk reduction, as well as other population-level interventions. |
|
Affordable Care Act Provision |
HRSA and CDC Opportunities |
|
Medicaid Preventive Services (ACA §§ 4106 and 2001) The provision gives states the option to improve coverage of clinical preventive services for traditional eligibility groups, as well as Medicaid benchmark coverage for newly eligible persons, redefined to parallel the act’s definition of essential health benefits, which includes coverage for preventive services. It also provides Medicaid incentives for prevention of chronic diseases. |
• Primary care providers and public health departments could become participating Medicaid providers and collaborate in designing programs to furnish preventive services to adult and child populations. • HRSA and CDC could collaborate with CMS on the development of joint guidance regarding coverage of preventive services. Such guidance might explain both the required and optional preventive service provisions of the law, as well as federal financing incentives for coverage of those services. Such guidance also might describe best practices in making preventive services more accessible to Medicaid beneficiaries through the use of expanded managed care provider networks and out-of-network coverage in nontraditional locations such as schools, public housing, and workplace sites; qualification criteria for participating providers; recruitment of providers; measurement of quality performance; and assessment of impact on population health. • HRSA and CDC have a crucial role to play in the implementation of state demonstrations, particularly in outreach to community providers to enlist them as active participants in such demonstrations, training and technical support to state Medicaid agencies, outreach to public health departments and health centers in demonstration states, and collaboration with CMS on the development of outcome standards and scalability criteria. |
|
Community Health Centers (ACA § 5601) The provision expands funding for health centers. |
• An imperative for HRSA is to preserve and strengthen the role of health centers as core safety net providers of clinical care and prevention in the communities they serve. Incentives could be built into funding for these centers to promote activities and linkages with local public health departments and encourage community engagement and partnerships for community-based prevention. • Outreach campaigns to promote clinical preventive services in underserved communities, as well as initiatives aimed at improving the quality of primary care for populations with serious and chronic health conditions, could focus on how to improve the performance of health centers. |
|
Affordable Care Act Provision |
HRSA and CDC Opportunities |
|
National Prevention, Health Promotion and Public Health Council and the National Prevention Strategy (ACA § 4001) The provision creates the National Prevention, Health Promotion and Public Health Council to create a collaborative national strategy to address health in the nation. |
• HRSA and CDC could use the Council as a mechanism for working with other agencies around the integration of primary care and public health. |
|
CMS Innovation Center (CMMI) (ACA § 3021) The provision establishes CMMI to develop, conduct, and evaluate pilots for improving quality, efficiency, and patient health outcomes in both the Medicare and Medicaid programs, with an emphasis on dual enrollees. |
• HRSA and CDC could engage with CMMI in the implementation of its community health innovation program to develop models that would leverage clinical care to achieve a broader impact on population health. • In the CMMI provisions of the ACA and elsewhere in the act, a major thrust of health care reform is attention to dually eligible Medicare/Medicaid beneficiaries. HRSA and CDC could develop an initiative aimed at improving the health and health care of this population. |
|
Accountable Care Organizations (ACOs) (ACA § 3022) The provision authorizes the secretary of the Department of Health and Human Services (HHS) to enter into agreements with ACOs on a shared savings basis to improve the quality of patient care and health outcomes and increase efficiency. |
• HRSA could encourage health centers to form ACOs and link with public health departments in this endeavor. • HRSA and CDC could develop models of collaboration between public health departments and ACOs that include safety net providers. Such models might emphasize the role of public health in needs assessment, performance measurement and improvement, health promotion, and patient engagement, all of which are central elements of ACOs. |
|
Affordable Care Act Provision |
HRSA and CDC Opportunities |
|
Patient-Centered Medical Homes (ACA § 3502) The provision authorizes state Medicaid programs to establish medical homes for Medicaid beneficiaries with chronic health conditions, and authorizes the secretary of HHS to award grants for the establishment of health teams to support primary care. |
• HRSA and CDC could collaborate on further development of the medical home model and its team-based approach to care and encourage the inclusion of local public health departments in that model. • HRSA and CDC could provide technical support to state Medicaid agencies seeking to pursue the medical home model, imparting best practices in the design and development of a medical home that is comprehensive, efficient in care delivery, and patient/family-centered. This support also could be expanded to include the development of performance measurement tools for measuring progress in these areas. • HRSA and CDC could develop a sustainable model for the medical home in Medicare and Medicaid that encourages inclusion of local public health departments, supports multiple population types, and can be translated for private health insurance as well. |
|
Primary Care Extension Program (ACA § 5405) The provision authorizes the Agency for Healthcare Research and Quality (AHRQ) to award competitive grants to states for the establishment of Primary Care Extension Programs to improve the delivery of primary care and community health. |
• HRSA and CDC could work with AHRQ to ensure that Primary Care Extension Programs include a public health orientation and integrate community health issues into practice- and clinic-based primary care improvement activities. • HRSA and CDC, working jointly with AHRQ, could seek collaboration with CMMI to fund Primary Care Extension Program models for which there is evidence for improving personal and population health. |
|
National Health Service Corps (ACA § 5207) The provision expands funding for the National Health Service Corps. |
• HRSA and CDC could collaborate in prioritizing the recruitment and placement of National Health Service Corps resources and developing linkages with existing Epidemic Intelligence Service (EIS) officers placed in state and local health departments. |
|
Affordable Care Act Provision |
HRSA and CDC Opportunities |
|
Teaching Health Centers (ACA § 5508) The provision authorizes and funds the establishment of and ongoing operational support for teaching health centers, which must be community-based. |
• HRSA could work with teaching health centers to adopt the patient-centered medical home curriculum and ensure that any curriculum used to train residents includes strong community and public health components—ideally with residents working on projects that concretely promote primary care-public health integration. • HRSA and CDC could work with the centers on training programs that would be aimed at producing competency to work in community health teams, given the emphasis placed on teams under the ACA. |
NOTE: ACA = Patient Protection and Affordable Care Act.
Despite these opportunities, the current funding system for primary care and public health is not well positioned to promote integration. For example, competing funding streams have the effect of creating silos at the local level rather than encouraging cooperation across entities. Similarly, most funding streams from HRSA and CDC are inflexible, limiting what local entities can do with the funds and how they could be used for integration. Finally, it should be noted that the funds available to HRSA and CDC for supporting and integrating primary care and public health are quite small relative to the funds available to the Centers for Medicare & Medicaid Services (CMS). By joining forces, the three agencies could create much greater momentum toward integration.
RECOMMENDATIONS
In the committee’s view, the principles for integration outlined above serve as a framework for action. The committee developed five recommendations—aimed at the agency and department levels—whose implementation would assist the leadership of CDC, HRSA, and HHS in creating an environment that would support the broader application of these principles.
Agency Level
Recommendation 1. To link staff, funds, and data at the regional, state, and local levels, HRSA and CDC should:
• identify opportunities to coordinate funding streams in selected programs and convene joint staff groups to develop grants, requests for proposals, and metrics for evaluation;
• create opportunities for staff to build relationships with each other and local stakeholders by taking full advantage of opportunities to work through the 10 regional HHS offices, state primary care offices and association organizations, state and local health departments, and other mechanisms;
• join efforts to undertake an inventory of existing health and health care databases and identify new data sets, creating from these a consolidated platform for sharing and displaying local population health data that could be used by communities; and
• recognize the need for and commit to developing a trained workforce that can create information systems and make them efficient for the end user.
Recommendation 2. To create common research and learning networks to foster and support the integration of primary care and public health to improve population health, HRSA and CDC should:
• support the evaluation of existing and the development of new local and regional models of primary care and public health integration, including by working with the CMS Innovation Center (CMMI) on joint evaluations of integration involving Medicare and Medicaid beneficiaries;
• work with the Agency for Healthcare and Research Quality’s (AHRQ’s) Action Networks on the diffusion of best practices related to the integration of primary care and public health; and
• convene stakeholders at the national and regional levels to share best practices in the integration of primary care and public health.
Recommendation 3. To develop the workforce needed to support the integration of primary care and public health:
• HRSA and CDC should work with CMS to identify regulatory options for graduate medical education funding that give priority to provider training in primary care and public health settings and specifically support programs that integrate primary care practice with public health.
• HRSA and CDC should explore whether the training component of the Epidemic Intelligence Service (EIS) and the strategic placement of assignees in state and local health departments offer additional opportunities to contribute to the integration of primary care and public health by assisting community health programs supported by HRSA in the use of data for improving community health. Any opportunities identified should be utilized.
• HRSA should create specific Title VII and VIII criteria or preferences related to curriculum development and clinical experiences that favor the integration of primary care and public health.
• HRSA and CDC should create all possible linkages among HRSA’s primary care training programs (Title VII and VIII), its public health and preventive medicine training programs, and CDC’s public health workforce programs (EIS).
• HRSA and CDC should work together to develop training grants and teaching tools that can prepare the next generation of health professionals for more integrated clinical and public health functions in practice. These tools, which should include a focus on cultural outreach, health education, and nutrition, can be used in the training programs supported by HRSA and CDC, as well as distributed more broadly.
Department Level
Recommendation 4. To improve the integration of primary care and public health through existing HHS programs, as well as newly legislated initiatives, the secretary of HHS should direct:
• CMMI to use its focus on improving community health to support pilots that better integrate primary care and public health and programs in other sectors affecting the broader determinants of health;
• the National Institutes of Health to use the Clinical and Translational Science Awards to encourage the development and diffusion of research advances to applications in the community through primary care and public health;
• the National Committee on Vital and Health Statistics to advise the secretary on integrating policy and incentives for the capture of data that would promote the integration of clinical and public health information;
• the Office of the National Coordinator to consider the development of population measures that would support the integration of community-level clinical and public health data; and
• AHRQ to encourage its Primary Care Extension Program to create linkages between primary care providers and their local health departments.
Recommendation 5. The secretary of HHS should work with all agencies within the department as a first step in the development of a national strategy and investment plan for the creation of a primary
care and public health infrastructure strong enough and appropriately integrated to enable the agencies to play their appropriate roles in furthering the nation’s population health goals.
REFERENCES
Frieden, T. R. 2010. A framework for public health action: The health impact pyramid. American Journal of Public Health 100(4):590-595.
HRSA (Health Resources and Services Administration). 2010. Public Health Steering Committee recommendations: Reinvigorating HRSA’s public health agenda. Washington, DC: HRSA.
HRSA. 2011. Uniform Data System 2010 national data. Washington, DC: Bureau of Primary Care, HRSA, U.S. Department of Health and Human Services.
IOM (Institute of Medicine). 1988. The future of public health. Washington, DC: National Academy Press.
IOM. 1996. Primary care: America’s health in a new era. Washington, DC: National Academy Press.
Kindig, D., and G. Stoddart. 2003. What is population health? American Journal of Public Health 93(3):380-383.
Starfield, B., and J. Horder. 2007. Interpersonal continuity: Old and new perspectives. British Journal of General Practice 57(540):527-529.
Welton, W. E., T. A. Kantner, and S. M. Katz. 1997. Developing tomorrow’s integrated community health systems: A leadership challenge for public health and primary care. Milbank Quarterly 75(9184684):261-288.
















