
1
Dietary Reference Intakes
INTRODUCTION
The term Dietary Reference Intakes (DRIs) is new to the field of nutrition. It refers to a set of at least four nutrient-based reference values that can be used for planning and assessing diets and for many other purposes. The DRIs replace the periodic revisions of the Recommended Dietary Allowances, which have been published since 1941 by the National Academy of Sciences. This is a comprehensive effort being undertaken by the Standing Committee on the Scientific Evaluation of Dietary Reference Intakes of the Food and Nutrition Board (FNB), Institute of Medicine, National Academy of Sciences, with the involvement of Health Canada. See Appendix A for a description of the overall process and its origins.
WHAT ARE DIETARY REFERENCE INTAKES?
The reference values, collectively called the DRIs, include the Estimated Average Requirement (EAR), the Recommended Dietary Allowance (RDA), the Adequate Intake (AI), and the Tolerable Upper Intake Level (UL).
A requirement is defined as the lowest continuing intake level of a nutrient that, for a specified indicator of adequacy, will maintain a defined level of nutriture in an individual. The chosen criterion on which nutritional adequacy for a nutrient is based may differ according to the life stage or gender of the individual. Hence, partic-
ular attention is given throughout this report to the choice and justification of the criterion used to establish requirement values.
This approach differs somewhat from that used recently by the joint World Health Organization, Food and Agriculture Organization, and International Atomic Energy Agency (WHO/FAO/IAEA) Expert Consultation on Trace Elements in Human Nutrition and Health (WHO, 1996). That publication uses the term basal requirement to indicate the level of intake needed to prevent pathologically relevant and clinically detectable signs of a dietary inadequacy. The term normative requirement indicates the level of intake sufficient to maintain a desirable body store or reserve. In developing DRIs, emphasis is placed instead on the reasons underlying the choice of the criterion of nutritional adequacy used to establish the requirement. They have not been designated as basal or normative.
Unless otherwise stated, all values given for EARs, RDAs, and AIs represent the quantity of the nutrient or food component to be supplied by foods from the diet that are similar to those consumed by a life stage or gender group in Canada and the United States. If the food source of the nutrient is very different (as in the diets of some ethnic groups), or if the source is supplements, adjustments may need to be made for differences in nutrient bioavailability. When this is an issue, it is discussed for the specific nutrient under the heading “Special Considerations.”
As has been the practice in the past with recommendations regarding dietary allowances from the FNB (NRC, 1980, 1989a), the DRIs included in this report are intended to apply to the healthy general population. RDAs and AIs are dietary intake values that should minimize the risk of developing a condition that is associated with that nutrient in question and that has a negative functional outcome. They could not necessarily be expected to replete individuals who are already malnourished, nor would they be adequate for certain disease states marked by increased requirements. Qualified medical and nutrition personnel must tailor recommendations for individuals who are known to have diseases that greatly increase requirements, or who have increased sensitivity to developing adverse effects associated with higher intakes. Although at times these reference intakes may serve as the basis for such individual recommendations, qualified professional adaptation that is specific to each situation is necessary.
CATEGORIES OF DRIs
Each type of DRI refers to average daily nutrient intake over time. Some deviation around this average value over a number of days is expected.
Estimated Average1Requirement
The Estimated Average Requirement (EAR) is the daily intake value that is estimated to meet the requirement, as defined by the specified indicator of adequacy, in 50 percent of the individuals in a life stage or gender group (see Figure 1-1). At this level of intake, the other 50 percent of individuals in a specified group would not have their nutritional needs met. The EAR is used in setting the RDA (see below).
Recommended Dietary Allowance
The Recommended Dietary Allowance (RDA) is the average daily dietary intake level that is sufficient to meet the nutrient requirements of nearly all (97 to 98 percent) healthy individuals in a specific life stage and gender group (see Figure 1-1). The RDA is intended primarily for use as a goal for daily intake by individuals.
The EAR forms the basis for setting the RDA. If the variation in requirements is well defined and the requirement is normally distributed, the RDA is set at 2 standard deviations (SD) above the EAR:
RDA = EAR + 2 SDEAR.
If the SDs reported in studies are inconsistent, or if sufficient data on variation in requirements are not available for other reasons, a standard estimate of variance will be applied. This estimate assumes
|
1 |
It is recognized that the definition of EAR implies a median as opposed to a mean or average. The median and average would be the same if the distribution of requirements followed a symmetrical distribution, and would diverge as a distribution became skewed. Three considerations prompted the choice of the term estimated average requirement: (1) data are rarely adequate to determine the distribution of requirements, (2) precedent has been set by other countries that have used the same term for reference values similarly derived (COMA, 1991), and (3) the impreciseness of the data evaluated makes the determination of a statistically reliable median extremely unlikely. |
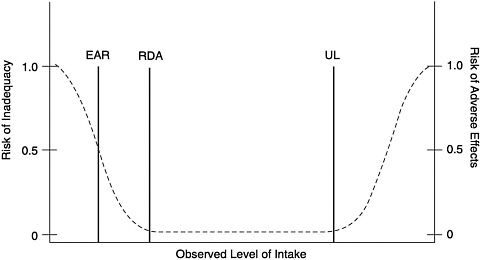
FIGURE 1-1 Dietary reference intakes. This figure shows that the Estimated Average Requirement (EAR) is the intake at which the risk of inadequacy is 0.5 (50%) to an individual. The Recommended Dietary Allowance (RDA) is the intake at which the risk of inadequacy is very small—only 0.02 to 0.03 (2 to 3%). The Adequate Intake (AI) does not bear a consistent relationship to the EAR or the RDA because it is set without being able to estimate the average requirement. It is assumed that the AI is at or above the RDA if one could be calculated. At intakes between the RDA and the Tolerable Upper Intake Level (UL), the risks of inadequacy and of excess are both close to 0. At intakes above the UL, the risk of adverse effect may increase.
a coefficient of variation (CV; SD divided by the mean × 100) of 10 percent, which is equal to 1 SD, such that
RDA = 1.2 × EAR.
If the distribution of the nutrient requirements is known to be skewed for a population, other approaches will be used to find the ninety-seventh to ninety-eighth percentile.
The assumed CV of 10 percent is based on extensive data on the variation in basal metabolic rate (FAO/WHO/UNA, 1985; Garby and Lammert, 1984), which accounts for about two-thirds of the daily energy needs of many individuals residing in Canada and the United States (Elia, 1992), and on the similar CV of 12.5 percent estimated for protein requirements in adults (FAO/WHO/UNA, 1985). The assumption is made that the CV of requirements is similar
for most nutrients if special outside factors do not apply. In all cases, the method used to derive the RDA from the EAR is stated.
Other Uses of the EAR
Together with an estimate of the variance of intake, the EAR may also be used in the assessment of the intake of groups or in planning for the intake of groups (Beaton, 1994) (see Chapter 9).
Adequate Intake
If sufficient scientific evidence is not available to calculate an EAR, a reference intake called an Adequate Intake (AI) is used instead of an RDA. The AI2 is a value based on experimentally derived intake levels or approximations of observed mean nutrient intakes by a group (or groups) of healthy people. In the opinion of the DRI Committee, the AI for children and adults is expected to meet or exceed the amount needed to maintain a defined nutritional state or criterion of adequacy in essentially all members of a specific healthy population. Examples of defined nutritional states include normal growth, maintenance of normal circulating nutrient values, or other aspects of nutritional well-being or general health.
The AI is set when data are considered to be insufficient or inadequate to establish an EAR on which an RDA would be based. For example, for young infants for whom human milk is the recommended sole source of food for most nutrients for the first 4 to 6 months, the AI is based on the daily mean nutrient intake supplied by human milk for healthy, full-term infants who are exclusively breastfed. For adults, the AI may be based upon review of data from different approaches (e.g., dietary and experimental intakes of calcium) that each alone do not permit a reasonably confident estimate of an EAR.
The issuance of an AI is an indication that more research is needed to determine, with some degree of confidence, the mean and distribution of requirements for a specific nutrient. When this research is completed, it should be possible to replace AI estimates with EARs and RDAs.
|
2 |
It should be emphasized that the AI is different from both the RDA as defined here and from the “lower limit of the population mean intake range for nutritional sufficiency” used in the WHO report Trace Elements in Human Nutrition and Health (1996), which are each derived from information about the EAR. |
Comparison of the AI with the RDA
Similarities. Both the AI and RDA are to be used as a goal for individual intake. In general, the values are intended to cover the needs of nearly all persons in a life stage group. (For infants, the AI is the mean intake when consuming human milk by infants in the age group. Larger infants may have higher needs, which they meet by consuming more milk.) As with the RDAs, AIs for children and adolescents may be extrapolated from adult values if no other usable data are available.
Differences. There is much less certainty about the AI value than about the RDA value. Because AIs depend on a greater degree of judgment than is applied in estimating the EAR and subsequently an RDA, the AI may deviate significantly from the RDA, if it could have been determined, and may be numerically higher than the RDA, if it were known. For this reason, AIs must be used with greater care than is the case for RDAs. Also, the RDA is always calculated from the EAR, using a formula that takes into account the expected variation in the requirement for the nutrient (see previous section).
Tolerable Upper Intake Level
The Tolerable Upper Intake Level (UL) is the highest level of daily nutrient intake that is likely to pose no risks of adverse health effects in almost all individuals in the specified life stage group. As intake increases above the UL, the risk of adverse effects increases. It is based on an evaluation conducted using the methodology for risk assessment of nutrients described in Chapter 3 of this report. The need for setting ULs grew out of the increased fortification of foods with nutrients and the use of dietary supplements by more people and in larger doses.
The term tolerable intake was chosen to avoid implying a possible beneficial effect. Instead, the term connotes a level of intake that can, with high probability, be tolerated biologically. The UL is not intended to be a recommended level of intake, and there is no established benefit for healthy individuals if they consume a nutrient in amounts above the recommended intake (RDA or AI). As in the case of applying AIs, professionals should avoid very rigid use of ULs and first assess the characteristics of the individuals and/or group of concern; for example, source of nutrient, physiological state of the individual, length of sustained high intakes, etc.
For some nutrients there may be insufficient data on which to
base a UL. This indicates a need for caution. It does not mean that high intakes pose no risk of adverse effects.
Determination of Adequacy
The major focus of the development of EARs and AIs has been the determination of the most appropriate indicator of adequacy, followed by the derivation, from available data, of the EAR or AI. A key question is “Adequate for what?” In many cases, a continuum of benefits can be ascribed to various levels of intake of the same nutrient. A specified marker or indicator may be deemed the most appropriate to determine risk of deficiency for a nutrient, while another indicator may be the best marker in determining risk of chronic degenerative disease for that nutrient.
Each EAR or AI is described in terms of the selected criterion or outcome. For example, the dietary intake recommended as the AI for vitamin D for older adults (> 70 years) is based on both a biochemical marker (circulating 25-hydroxyvitamin D) and a functional outcome marker (reduced fractures and bone loss). Using data from clinical studies, an intake of vitamin D associated with normal circulating 25-hydroxyvitamin D concentrations was derived. This intake was supported by clinical trials in which supplemental calcium and vitamin D were associated with a reduced risk of fracture over three years and a reduction in loss of bone mineral density at specific bone sites. Thus, two sets of data form the basis for the AI. Since the individual contributions of the added calcium and vitamin D to the attenuation of bone loss cannot be evaluated, an AI was established. Whether these higher intakes of vitamin D at younger ages will reduce risk of osteoporosis and fracture in later life remains to be determined.
USES OF DIETARY REFERENCE INTAKES
Imbedded in the framework of DRIs is the following approach. When requirements are estimated to decrease risk of disease, particularly chronic degenerative disease where associations may not be easily identified in short-term studies, there must be a preponderance of epidemiologic evidence that is supported by clinical trials and biologically plausible mechanisms before such associations are used to establish recommendations. Given that chronic degenerative diseases and developmental abnormalities may not be detectable for significant periods of time, it is quite possible that individuals who have increased risk due to diet may not be identifiable,
and their long-term intake may be less than that which apparently decreases risk of the disease state.
If the strength of the data that associate risk of disease with the nutrient in question is sufficient to permit AIs to be based on such data, and national survey intake data indicate that the median intake is below the AI, then methods must be determined for individuals to increase consumption in order to decrease risk due to inadequate dietary intakes. Primary methods to accomplish this include educating consumers to change their food consumption behavior, increasing intake of fortified foodstuffs, providing dietary supplements, or a combination of these methods. It is not the function of this report, given the scope of work outlined, to analyze the potential impact of using these methods.
The benefits of food as the source of nutrients are well described in previous FNB reports (NRC, 1989a, 1989b). Obtaining RDAs and AIs from unfortified food continues to have the advantage of (1) providing intakes of other beneficial nutrients and food components, for which RDAs and AIs may not be determined, and (2) potentially enhancing intakes through interactions with other nutrients simultaneously. It is recognized, however, that the low energy intakes reported in recent national surveys and thought to result from decreased physical activity may mean that it would be unusual to see changes in food habits to the extent necessary to maintain intakes by all individuals at levels recommended in this report. Eating fortified food products represents one method by which to increase or maintain intakes without major changes in food habits. For some individuals at higher risk, nutrient supplements may be desirable in order to meet reference intakes.
It is not the function of this report, given the scope of the work (see Appendix A, Origin and Framework of the Development of Dietary Reference Intakes), to address applications of the DRIs, including assessment of the adequacy of intakes of various population groups and planning for intakes of populations or for groups with special needs. However, some uses for the different types of DRIs are described briefly in Chapter 9. A subsequent report will focus on uses of DRIs in various settings.
COMPARISON WITH OTHER COUNTRIES
Expert groups in many countries have developed reference values for nutrient intakes (Table 1-1). The number of life stage groups identified by these countries varies considerably. For example, the number of age categories identified within the first year of life rang-
TABLE 1-1 Reference Nutrient Values Used by Various Countries and Groups
|
Country/Region |
Year |
Number of Life-Stage Groupsa |
Number of Infant Groups |
Age at which Males and Females are First Treated Separately (years) |
EAR RDI RDNI |
AI RNI |
PRI |
RDA |
|
Belgium |
1994 |
4 |
2 |
11 b |
||||
|
Canada |
1990 |
17 |
2 |
7 |
|
|||
|
European Communityc |
1993 |
9 |
1 |
11 |
|
|||
|
Germany |
1991 |
14 |
2 |
10 |
|
|||
|
Netherlands |
1992 |
14 |
2 |
10 |
|
|
||
|
Nordic countries |
1989 |
13 |
2 |
11 |
|
|||
|
Sweden |
1989 |
13 |
2 |
11 |
|
|||
|
United Kingdom |
1991 |
14 |
4 |
11 |
|
|
||
|
United States |
1989 |
13 |
2 |
11 |
|
|||
|
NOTE: EAR, Estimated Average Requirement. United Kingdom: the required intake of a group of people for energy, protein, a vitamin, or a mineral. About half will usually need more than the EAR and half less. RDI and RDNI, Recommended Daily Nutrient Intake: the average nutrient intake that meets the requirement needs of 50 percent of a group. The remaining 50 percent of the group will have requirements above the RDI. RNI, Reference Nutrient Intake or AI, Adequate Intake. United Kingdom, Netherlands: an amount of the nutrient that is enough or more than enough to meet the needs of about 97 percent of people in a group. Canada: RNI = the recommended nutrient intakes of essential nutrients. PRI, Population Reference Intake: the intake that is enough for virtually all healthy people within a group. RDA, Recommended Dietary Allowance. United States: the intake that meets the nutrient needs of 97 to 98 percent of a group. Netherlands: the intake that meets the nutrient needs of practically all healthy people in a defined population/age category; applied to planning the food supply for the population group (similar to PRI). a Males and females treated separately after age 7, 10, or 11. b Except for energy. c Adults >18 years all grouped together; age < 6 months not addressed. SOURCES: Belgian National Council for Nutrition, 1994; COMA, 1991; European Community, 1993; German Society of Nutrition, 1991; Health Canada, 1990; National Food Administration, 1989; Netherlands Food and Nutrition Council, 1992; NRC 1989a; PNUN, 1989. |
||||||||
TABLE 1-2a Magnesium Nutrient Standards for Children Ages 1 to 3 Years and for Adult Females
|
Magnesium Nutrient Standards |
||
|
Country/Region |
Children 1–3 years (mg) |
Adult Females (mg) |
|
Average Requirement or Equivalent |
||
|
Germany |
80 |
300 |
|
Nordic countries |
150 |
300 |
|
Sweden |
150 |
300 |
|
United Kingdom |
65 |
250 |
|
Reference Nutrient Intake or Equivalent |
||
|
Belgium |
80-85 |
330 |
|
Canada |
40–50 |
200a |
|
European Community |
NDb |
150–500 |
|
Netherlands |
60–70c |
250–300c |
|
United Kingdom |
85 |
270 |
|
United States |
80 |
280 |
|
a Higher for women >51 years. b ND = Not determined. c Range given assuming a relationship with body weight. SOURCES: Belgian National Council for Nutrition, 1994; COMA, 1991;European Community, 1993; German Society of Nutrition, 1991; HealthCanada, 1990; National Food Administration, 1989; Netherlands Foodand Nutrition Council, 1992; NRC 1989a; PNUN, 1989. |
||
es from one to four. Although the United Kingdom (UK) (COMA, 1991) and The Netherlands (Netherlands Food and Nutrition Council, 1992) use two categories of reference values, and the UK includes an estimate of safe upper levels, the other countries listed in Table 1-1 provide only one each.
Two general types of reference values are used: (1) an estimate of the average requirement or (2) the intake that will meet the requirement of 97 to 98 percent (or virtually all) of the population. The reference values given differ by country. This is illustrated in Table 1-2a and Table 1-2b, which give the magnesium and phosphorus values for children ages 1 to 3 years and for females (mainly of childbearing years). Average requirements specified by several countries exceed the values set by other countries for intakes that would meet the needs of virtually all the population within that age group. Criteria chosen for estimating average requirements vary from country to country, as do the judgments made where limited data are available.
TABLE 1-2b Phosphorus Nutrient Standards for Children Ages 1 to 3 Years and for Adult Females
|
Phosphorus Nutrient Standards |
||
|
Country/Region |
Children 1–3 years (mg) |
Adult Females (mg) |
|
Average Requirement or Equivalent |
||
|
Germany |
NDa |
ND |
|
Nordic countries |
800 |
800 |
|
Sweden |
800 |
800 |
|
United Kingdom |
214 |
406 |
|
Reference Nutrient Intake or Equivalent |
||
|
Belgium |
700 |
800 |
|
Canada |
300–350 |
850 |
|
European Community |
300 |
550 |
|
Netherlands |
400–800b |
700–1,400b |
|
a ND = Not determined. b Range depends on absorption expected. SOURCES: Belgian National Council for Nutrition, 1994; COMA, 1991;European Community, 1993; German Society of Nutrition, 1991; HealthCanada, 1990; National Food Administration, 1989; Netherlands Foodand Nutrition Council, 1992; NRC 1989a; PNUN, 1989. |
||
PARAMETERS FOR DIETARY REFERENCE INTAKES
Life Stage Categories
The life stage categories described below were chosen with all the nutrients to be reviewed in mind, rather than only those included in this report. Additional subdivisions within these groups may be added in later reports. For example, pregnancy may be subdivided into two or more periods to accommodate women's changing needs for certain nutrients. Differences will be indicated by gender when warranted by the data.
Infancy
Infancy covers the period from birth through 12 months of age and is divided into two 6-month intervals. The first 6-month interval was not subdivided further because intake is relatively constant during this time. That is, as infants grow, they ingest more food; however, on a body weight basis their intake remains the same.
During the second 6 months of life, growth velocity slows, and thus total daily nutrient needs on a body weight basis may be less than those during the first 6 months of life.
For a particular nutrient, average intake by full-term infants who are born to healthy, well-nourished mothers and exclusively fed human milk has been adopted as the primary basis for deriving the AI for most nutrients during the first 6 months of life. The value used is thus not an EAR; the extent to which intake of human milk may result in exceeding the actual requirements of the infant is not known, and ethics of experimentation preclude testing the levels known to be potentially inadequate. Therefore, the AI is not an estimated average requirement in which only half of the group would be expected to have their needs met.
Using the human milk-fed infant as a model is in keeping with the basis for estimating nutrient allowances of infants developed in the last RDA (NRC, 1989a) and RNI (Health Canada, 1990) reports. It also supports the recommendation that exclusive breastfeeding is the preferred method of feeding for normal full-term infants for the first 4 to 6 months of life. This recommendation has been made by the Canadian Paediatric Society (Health Canada, 1990), the American Academy of Pediatrics (1982) and in the FNB report Nutrition During Lactation (IOM, 1991).
In general, for this report, special consideration was not given to possible variations in physiological need during the first month after birth (when, for example, urinary phosphorus loss is lower due to immature glomerular filtration rate [Brodehl et al., 1982; Svenningsen and Lindquist, 1974]) or to the variations in intake of nutrients from human milk that result from differences in milk volume and nutrient concentration during early lactation.
Specific DRIs to meet the needs of formula-fed infants are not proposed in this report. The previously published RDAs and RNIs for infants have led to much misinterpretation of the adequacy of human milk because of a lack of understanding about their derivation for young infants. Although they were based on human milk composition and volume of intake, the previous RDA and RNI values allowed for lower bioavailability of nutrients from nonhuman milk. In order to assist in deriving appropriate intakes of infants fed foods other than human milk, considerations for applying the AIs to formulas are addressed under the “Special Considerations” sections in Chapter 4, Chapter 5, Chapter 6, Chapter 7 through Chapter 8.
Ages 0 through 6 Months. To derive the AI value for infants ages 0 through 6 months, the mean intake of a nutrient was calculated based on the average concentration of the nutrient from 2 through
6 months of lactation using consensus values from several reported studies (Atkinson et al., 1995), and an average volume of milk intake of 780 ml/day as reported from studies of full-term infants by test weighing, a procedure in which the infant is weighed before and after each feeding (Butte et al., 1984; Chandra, 1984; Hofvander et al., 1982; Neville et al., 1988). Because there is variation in both of these measures, the computed value represents the mean. It is expected that infants will consume increased volumes of human milk as they grow.
Ages 7 through 12 Months. During the period of infants' growth acceleration and gradual weaning to a mixed diet of human milk and solid foods from ages 7 through 12 months, there is no evidence for markedly different nutrient needs within this period. The basis of the AI values derived for this age category was the sum of the specific nutrient provided by 600 ml/day of human milk, which is the average volume of milk reported from studies in this age category (Heinig et al., 1993), added to that provided by the usual intakes of complementary weaning foods consumed by infants in this age category (Specker et al., 1997). This approach is in keeping with the current recommendations of the Canadian Paediatric Society (Health Canada, 1990), the American Academy of Pediatrics (1982), and Nutrition During Lactation (IOM, 1991) for continued breastfeeding of infants through 9 to 12 months of age with appropriate introduction of solid foods.
One problem encountered in trying to derive intake data in infants was the lack of available data on total nutrient intake from a combination of human milk and solid foods in the second 6 months of life. Most intake survey data for the macrominerals do not identify the milk source, but the published values indicate that cow milk and cow milk formula were most likely consumed.
Toddlers: Ages 1 through 3 Years
The greater velocity of growth in height during ages 1 through 3 compared with ages 4 through 5 provides a biological basis for dividing this period of life. Because children in the United States and Canada from age 4 onwards begin to enter the public school system, ending this life stage prior to age 4 seemed appropriate. Data are sparse for indicators of nutrient adequacy on which to derive DRIs for these early years of life. In some cases, DRIs were derived from data extrapolated from studies of infants or of children aged 4 years or older.
Early Childhood: Ages 4 through 8 Years
Because major biological changes in velocity of growth and changing endocrine status occur during ages 4 through 8 or 9 years (the latter depending on onset of puberty in each gender), the category of 4 through 8 years is appropriate. For many nutrients, a reasonable amount of data are available on nutrient intake and various criteria for adequacy (such as nutrient balance measured in young children aged 5 through 7 years) that can be used as the basis for the EARs and AIs for this life stage group.
Puberty/Adolescence: Ages 9 through 13 Years and 14 through 18 Years
Recognizing that current data support younger ages for pubertal development, it was determined that the adolescent age group should begin at 9 years. The mean age of onset of breast development (Tanner Stage 2) for white females in the United States is 10.0 years (SD 1.8); this is a physical marker for the beginning of increased estrogen secretion (Herman-Giddens et al., 1997). In African American females, onset of breast development is earlier (mean 8.9 years (± 1.9). The reasons for the observed racial differences in the age at which girls enter puberty are unknown. The onset of the growth spurt in girls begins before the onset of breast development (Tanner, 1990). The age group of 9 through 13 years allows for this early growth spurt in females.
For males, the mean age of initiation of testicular development is 10.5 to 11 years, and their growth spurt begins 2 years later (Tanner, 1990). Thus, to begin the second age category at 14 years and to have different EARs and AIs for females and males for some nutrients at this age seemed biologically appropriate. All children continue to grow to some extent until as late as age 20; therefore, having these two age categories span the period 9 through 18 years of age seemed justified.
Young Adulthood and Middle Age: Ages 19 through 30 Years and 31 through 50 Years
The recognition of the possible value of higher nutrient intakes during early adulthood to achieving optimal genetic potential for peak bone mass was the reason for dividing adulthood into ages 19 through 30 years and 31 through 50 years. Moreover, mean energy expenditure decreases during this 30-year period, and needs for
nutrients related to energy metabolism may also decrease. For some nutrients, the DRIs may be the same for the two age groups. However, for other nutrients, especially those related to energy metabolism, AIs or EARs (and RDAs) are likely to differ for these two age groups.
Adulthood and Older Adults: Ages 51 through 70 Years and > 70 Years
The age period of 51 through 70 years spans the active work years for most adults. After age 70, people of the same age increasingly display variability in physiological functioning and physical activity. A comparison of people over age 70 who are the same chronological age may demonstrate as much as a 15- to 20-year, age-related difference in level of reserve capacity and functioning. This is demonstrated by age-related declines in nutrient absorption and renal function. Because of the high variability in functional capacity of older adults, the EARs and AIs for this age group may reflect a greater variability in requirements for the older age categories. This may be most applicable to nutrients for which requirements are related to energy expenditure.
Pregnancy and Lactation
Recommendations for pregnancy and lactation may be subdivided because of the many physiological changes and changes in nutrient needs that occur during these life stages. In setting EARs and AIs for these life stages, however, consideration is given to adaptations to the increased nutrient demand—such as increased absorption and greater conservation of many nutrients. Moreover, there may be net losses of some nutrients that occur physiologically regardless of the nutrient intake. Thus, for some nutrients, there may not be a basis for EAR or AI values that are different during these life stages than they are for other women of comparable age.
Reference Weights and Heights
The reference weights and heights selected for adults and children are shown in Table 1-3. The values are based on anthropometric data collected during 1988 –1994 as part of the Third National Health and Nutrition Examination Survey (NHANES III) in the United States.
The median heights for children aged 4 through 8, for adoles-
TABLE 1-3 DRI Reference Heights and Weights for Children and Adultsa
|
Gender |
Age |
Median Body Mass Index, kg/m2 |
Reference Height, cm (in) |
Reference Weight,b kg (lb) |
|
Male, female |
2–6 months |
— |
64 (25) |
7 (16) |
|
7–12 months |
— |
72 (28) |
9 (20) |
|
|
1–3 years |
— |
91 (36) |
13 (29) |
|
|
4–8 years |
15.8 |
118 (46) |
22 (48) |
|
|
Male |
9–13 years |
18.5 |
147 (58) |
40 (88) |
|
14–18 years |
21.3 |
174 (68) |
64 (142) |
|
|
19–30 years |
24.4 |
176 (69) |
76 (166) |
|
|
Female |
9–13 years |
18.3 |
148 (58) |
40 (88) |
|
14–18 years |
21.3 |
163 (64) |
57 (125) |
|
|
19–30 years |
22.8 |
163 (64) |
61 (133) |
|
|
a Adapted from NHANES III, 1988-1994. b Calculated from body mass index and height for ages 4 through 8 years and older. |
||||
cents aged 9 through 13 and 14 through 18, and for young adults aged 19 through 30 were identified, and the weights for those heights were based on Body Mass Index (BMI) for the same individuals within the group. Since there is no evidence that weight should change with aging if activity is maintained, the reference weights for 19- through 30-year-old young adults are applied to all adult age groups.
The most recent nationally representative data available for Canadians (from the 1970–1972 Nutrition Canada Survey [Demirjian, 1980]) were reviewed. In general, median heights of children from 1 year of age in the United States were greater by 3 to 8 cm (1 to 2 1/2 inches) compared to children of the same age in Canada measured two decades earlier (Demirjian, 1980). This could be partly explained by approximations necessary to compare the two data sets, but more possibly by a continuation of the secular trend of increased heights for age noted in the Nutrition Canada survey when it compared data from that survey to an earlier (1953) national Canadian survey (Pett and Ogilvie, 1956).
Similarly, median weights beyond age 1 year derived from the recent survey in the United States (NHANES III, 1988–1994) were also greater than those obtained from the older Canadian survey (Demirjian, 1980). Differences were greatest during adolescence, ranging from 10 to 17 percent higher. The differences probably reflect the secular trend of earlier onset of puberty (Herman-Gid-
dens et al., 1997), rather than differences in populations. Calculations of BMI for young adults (for example, a median of 22.6 for Canadian women compared to 22.8 for American women) resulted in similar values, indicating that by adulthood there was greater concordance between the two surveys.
The reference weights chosen for this report were based on the most recent data set available from either country, recognizing that earlier surveys in Canada indicated shorter stature and lower weights during adolescence compared to those from surveys in the United States.
Reference weights are used primarily when setting the EAR, AI, or UL for children or when relating the nutrient needs of adults to body weight. For the 4- to 8-year-old age group, it can be assumed that a small 4-year-old child will require less than the EAR and that a large 8-year-old will require more than the EAR. However, the RDA should meet the needs of both.
SUMMARY
Dietary Reference Intakes is a generic term for a set of nutrient reference values that includes Estimated Average Requirement, Recommended Dietary Allowance, Adequate Intake, and Tolerable Upper Intake Level. These reference values are being developed for life stage and gender groups in a joint U.S.-Canadian activity. This report, which is the first in a series, covers the DRIs for calcium and four related nutrients: phosphorus, magnesium, vitamin D, and fluoride.

















