
1
Introduction to Dietary Reference Intakes
Dietary Reference Intakes (DRIs) comprise a set of at least four nutrient-based reference values, each of which has special uses. The development of DRIs expands on the periodic reports called Recommended Dietary Allowances, which have been published since 1941 by the National Academy of Sciences. This comprehensive effort is being undertaken by the Standing Committee on the Scientific Evaluation of Dietary Reference Intakes of the Food and Nutrition Board, Institute of Medicine, National Academy of Sciences, with the involvement of Health Canada. See Appendix A for a description of the overall process and its origins.
WHAT ARE DIETARY REFERENCE INTAKES?
The reference values, collectively called the Dietary Reference Intakes (DRIs), include the Recommended Dietary Allowance (RDA), Adequate Intake (AI), Tolerable Upper Intake Level (UL), and Estimated Average Requirement (EAR).
A requirement is defined as the lowest continuing intake level of a nutrient that will maintain a defined level of nutriture in an individual. The chosen criterion of nutritional adequacy is identified in each chapter; note that the criterion may differ for individuals at different life stages.
Unless otherwise stated, all values given for RDAs, AIs, and EARs represent the quantity of the nutrient or food component to be supplied by foods from a diet similar to those consumed in Canada
and the United States. If the degree of absorption of the nutrient is unusually low on a chronic basis (e.g., because of very high fiber intake), a higher intake may be needed. If the primary source of a B vitamin is a supplement (e.g., B12 for the elderly), a higher percentage of the vitamin may be absorbed and so a smaller intake may be required.
The DRIs apply to the healthy population. RDAs and AIs are levels of intake recommended for individuals. Meeting the recommended intake for the B vitamins and choline would not necessarily be sufficient for individuals who are already malnourished. People with diseases that result in malabsorption syndrome or who are receiving treatments such as hemodialysis or peritoneal dialysis may have increased requirements. Special guidance should be provided for those with greatly increased nutrient requirements. Although the RDA or AI may serve as the basis for such guidance, qualified medical and nutrition personnel should make necessary adaptations for specific situations.
CATEGORIES OF DIETARY REFERENCE INTAKES
Each type of Dietary Reference Intake (DRI) refers to average daily nutrient intake of individuals over time. The amount taken may vary substantially from day to day without ill effect in most cases.
Recommended Dietary Allowance
The Recommended Dietary Allowance (RDA) is the average daily dietary intake level that is sufficient to meet the nutrient requirement of nearly all (97 to 98 percent) healthy individuals in a particular life stage and gender group (see Figure 1-1). The RDA is intended to be used as a goal for daily intake by individuals. The process for setting the RDA is described below; it depends on being able to set an Estimated Average Requirement (EAR). That is, if an EAR cannot be set, no RDA will be set.
Estimated Average Requirement1
The EAR is the daily intake value that is estimated to meet the requirement—as defined by the specified indicator of adequacy—
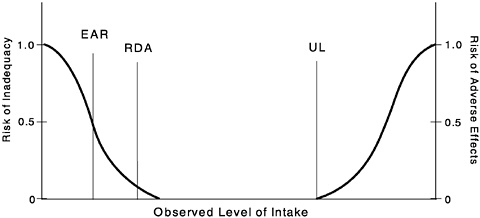
FIGURE 1-1 Dietary reference intakes. This figure shows that the Estimated Average Requirement (EAR) is the intake at which the risk of inadequacy is 0.5 (50%) to an individual. The Recommended Dietary Allowance (RDA) is the intake at which the risk of inadequacy is very small—only 0.02 to 0.03 (2% to 3%). The Adequate Intake (AI) does not bear a consistent relationship to the EAR or the RDA because it is set without being able to estimate the average requirement. It is assumed that the AI is at or above the RDA if one could be calculated. At intakes between the RDA and the Tolerable Upper Intake Level (UL), the risks of inadequacy and of excess are both close to 0. At intakes above the UL, the risk of adverse effects may increase.
in half of the healthy individuals in a life stage or gender group (see Figure 1-1). At this level of intake, the other half of a specified group would not have its nutritional needs met. The general method used to set the EAR is the same for all the B vitamins. The details, which are provided in Chapters 4 through 9, differ because of the different types of data available.
Method for Setting the RDA
The EAR is used in setting the RDA as follows. If the standard deviation (SD) of the EAR is available and the requirement for the
nutrient is normally distributed, the EAR plus 2 SDs of the EAR equals the RDA:
RDA = EAR + 2 SDEAR.
If data about variability in requirements are insufficient to calculate an SD, a coefficient of variation (CVEAR) of 10 percent will be ordinarily assumed. Because
CVEAR = SDEAR/EAR,
and
SD = (EAR × CVEAR),
the resulting equation for the RDA is
RDA = EAR + 2 (0.1 × EAR)
or
RDA = 1.2 × EAR.
The assumption of a 10 percent CV is based on extensive data on the variation in basal metabolic rate (FAO/WHO/UNA, 1985; Garby and Lammert, 1984), which contributes about two-thirds of the daily energy expenditure of many individuals residing in Canada and the United States (Elia, 1992) and on the similar CV of 12.5 percent estimated for the protein requirements in adults (FAO/ WHO/UNA, 1985). If there is evidence of greater variation, a larger CV will be assumed. If the distribution of the nutrient requirement is known to be skewed for a population, other approaches may be used to find the ninety-seventh percentile to set the RDA. In all cases the method used to derive the RDA from the EAR is stated.
For the B vitamins there are few direct data on the requirements of children. Thus, EARs and RDAs for children are based on extrapolations from adult values. The method is described in Chapter 2.
Other Uses of the EAR
Together with an estimate of the variance of intake, the EAR may also be used in the assessment of the intake of groups or in planning for the intake of groups (Beaton, 1994) (see Chapter 13).
Adequate Intake
If sufficient scientific evidence is not available to calculate an EAR, a reference intake called an Adequate Intake (AI) is used instead of an RDA. The AI is a value based on experimentally derived intake levels or approximations of observed mean nutrient intakes by a group (or groups) of healthy people. In the opinion of the committee, the AI for children and adults is expected to meet or exceed the amount needed to maintain a defined nutritional state or criterion of adequacy in essentially all members of a specific healthy population. Examples of defined nutritional states include normal growth, maintenance of normal circulating nutrient values, or other aspects of nutritional well-being or general health.
The AI is set when data are considered to be insufficient or inadequate to establish an EAR on which an RDA would be based. For example, for young infants for whom human milk is the recommended sole source of food for most nutrients for the first 4 to 6 months, the AI is based on the daily mean nutrient intake supplied by human milk for healthy, full-term infants who are exclusively breastfed. For adults the AI may be based on data from a single experiment (e.g., choline), on estimated dietary intakes in apparently healthy population groups (e.g., biotin and pantothenic acid), or on a review of data from different approaches that considered alone do not permit a reasonably confident estimate of an EAR (e.g., dietary and experimental intakes of calcium).
The issuance of an AI indicates that more research is needed to determine with some degree of confidence the mean and distribution of requirements for a specific nutrient. When this research is completed, it should be possible to replace AI estimates with EARs and RDAs.
Comparison of the AI with the RDA
Similarities. Both the AI and RDA are to be used as a goal for individual intake. In general the values are intended to cover the needs of nearly all persons in a life stage group. (For infants the AI is the mean intake when infants in the age group are consuming human milk. Larger infants may have greater needs, which they meet by consuming more milk.) As with RDAs, AIs for children and adolescents may be extrapolated from adult values if no other usable data are available.
Differences. There is much less certainty about the AI value than about the RDA value. Because AIs depend on a greater degree of
judgment than is applied in estimating the EAR and subsequently an RDA, the AI might deviate significantly from and be numerically higher than the RDA if it could be determined. For this reason, AIs must be used with greater care than is the case for RDAs. Also, the RDA is always calculated from the EAR by using a formula that takes into account the expected variation in the requirement for the nutrient (see previous section).
Tolerable Upper Intake Level
The Tolerable Upper Intake Level (UL) is the highest level of daily nutrient intake that is likely to pose no risk of adverse health effects in almost all individuals in the specified life stage group (see Figure 1-1). As intake increases above the UL, the risk of adverse effects increases. The term tolerable was chosen to avoid implying a possible beneficial effect; the term is intended to connote a level of intake that can, with high probability, be tolerated biologically. The UL is not intended to be a recommended level of intake, and there is no established benefit for healthy individuals if they consume a nutrient in amounts exceeding the recommended intake (the RDA or AI).
The UL is based on an evaluation conducted by using the methodology for risk assessment of nutrients (see Chapter 3). The need for setting ULs grew out of the increased fortification of foods with nutrients and the increased use of dietary supplements. For vitamin B6 and choline, the UL refers to total intakes—from food, fortified food, and nutrient supplements. In other instances (i.e., for niacin and folate) it may refer only to intakes from supplements or fortificants or a combination of the two. The UL applies to chronic daily use. Details are given for each nutrient.
For some nutrients, data may not be sufficient for deriving a UL. This indicates the need for caution in consuming amounts greater than the recommended intakes; it does not mean that high intakes pose no risk of adverse effects.
Determination of Adequacy
In the derivation of the EAR or AI, close attention has been paid to the determination of the most appropriate indicators of adequacy. A key question is, Adequate for what? In many cases a continuum of benefits may be ascribed to various levels of intake of the same nutrient. One criterion may be deemed the most appropriate to determine the risk that an individual will become deficient in the
nutrient whereas another may relate to reducing the risk of chronic degenerative disease, such as certain dementias, cardiovascular disease, cancer, diabetes mellitus, some forms of renal disease, or degenerative arthritis.
Each EAR and AI is described in terms of the selected criterion. For example, the dietary intake set for the RDA for folate for women in the childbearing years is based on a combination of biochemical indicators, but a separate recommendation is made for women capable of becoming pregnant to reduce the risk of a neural tube defect in the offspring if pregnancy occurs.
The potential role of B vitamins and choline in the reduction of disease risk was considered in developing the EARs and AIs for this group of nutrients. The types of evidence considered are described in Chapter 2.
For many of the B vitamins, the use of a single indicator of adequacy was deemed inappropriate. For any one B vitamin, several biochemical values provide information about nutrient status, but adverse effects of inadequate intake may not be observable if only one (or possibly more) of the values is outside its normal range. With the acquisition of new data, such as data relating intake to chronic disease or disability, the choice of the criterion for setting the EAR may change.
PARAMETERS FOR DIETARY REFERENCE INTAKES
Life Stage Groups
Reference nutrient intakes are expressed for 16 life stage groups,2 as listed in Table 1-1 and described in more detail in the first report in this series (IOM, 1997). If data are too sparse to distinguish differences in requirements by life stage or gender group, the analysis may be presented for a larger grouping. Differences will be indicated by gender when warranted by the data.
TABLE 1-1 Life Stage Groups
|
Infants 0 through 6 mo 7 through 12 mo |
Females 9 through 13 y 14 through 18 y 19 through 30 y 31 through 50 y 51 through 70 y > 70 y |
|
Children 1 through 3 y 4 through 8 y |
Pregnancy ≤ 14 through 18 y 19 through 30 y 31 through 50 y |
|
Males 9 through 13 y 14 through 18 y 19 through 30 y 31 through 50 y 51 through 70 y > 70 y |
Lactation ≤ 14 through 18 y 19 through 30 y 31 through 50 y |
Reference Weights and Heights
The reference weights and heights selected for adults and children are shown in Table 1-2. The values are based on anthropometric data collected from 1988 to 1994 as part of the Third National Health and Nutrition Examination Survey (NHANES III) in the United States.
The median heights for the life stage and gender groups through age 30 years were identified, and the median weights for those heights were based on median body mass index for the same individuals. Because there is no evidence that weight should change as adults age if activity is maintained, the reference weights for adults aged 19 through 30 years are applied to all adult age groups.
The most recent nationally representative data available for Canadians (from the 1970–1972 Nutrition Canada Survey [Demirjian, 1980]) were reviewed. In general, median heights of children from 1 year of age in the United States were greater by 3 to 8 cm (1 to 2.5 inches) than those of children of the same age in Canada measured two decades earlier (Demirjian, 1980). This could be partly explained by approximations necessary to compare the two data sets but more possibly by a continuation of the secular trend of increased heights for age noted in the Nutrition Canada Survey when it compared data from that survey with an earlier (1953) national Canadian survey (Pett and Ogilvie, 1956).
TABLE 1-2 Reference Heights and Weights for Children and Adults in the United Statesa
|
Gender |
Age |
Median Body Mass Indexb |
Reference Height (cm [in]) |
Reference Weightc (kg [lb]) |
|
Male, female |
2–6 mo |
— |
64 (25) |
7 (16) |
|
|
7–11 mo |
— |
72 (28) |
9 (20) |
|
|
1–3 y |
— |
91 (36) |
13 (29) |
|
|
4–8 y |
15.8 |
118 (46) |
22 (48) |
|
Male |
9–13 y |
18.5 |
147 (58) |
40 (88) |
|
|
14–18 y |
21.3 |
174 (68) |
64 (142) |
|
|
19–30 y |
24.4 |
176 (69) |
76 (166) |
|
Female |
9–13 y |
18.3 |
148 (58) |
40 (88) |
|
|
14–18 y |
21.3 |
163 (64) |
57 (125) |
|
|
19–30 y |
22.8 |
163 (64) |
61 (133) |
|
a Adapted from Third National Health and Nutrition Examination Survey (NHANES III), 1988–1994. b In kg/m2. c Calculated from body mass index and height for ages 4 through 8 years and older. |
||||
Similarly, median weights beyond age 1 year derived from the recent survey in the United States (NHANES III, 1988 to 1994) were also greater than those obtained from the older Canadian survey (Demirjian, 1980). Differences were greatest during adolescence, ranging from 10 to 17 percent higher. The differences probably reflect the secular trend of earlier onset of puberty (Herman-Giddens et al., 1997) rather than differences in populations. Calculations of body mass index for young adults (e.g., a median of 22.6 for Canadian women compared with 22.8 for U.S. women) resulted in similar values, indicating greater concordance between the two surveys by adulthood.
The reference weights chosen for this report were based on the most recent data set available from either country, recognizing that earlier surveys in Canada indicated shorter stature and lower weights during adolescence than did surveys in the United States.
Reference weights are used primarily when setting the Estimated Average Requirements (EARs), Adequate Intakes (AIs), or Tolerable Upper Intake Levels (ULs) for children or when relating the nutrient needs of adults to body weight. For the 4- to 8-year-old age group, it can be assumed that a small 4-year-old child will require less than the EAR and that a large 8-year-old will require more than
the EAR. However, the Recommended Dietary Allowance (RDA) or AI should meet the needs of both.
SUMMARY
Dietary Reference Intakes (DRIs) is a generic term for a set of nutrient reference values that includes the Recommended Dietary Allowance (RDA), Adequate Intake (AI), Tolerable Upper Intake Level (UL), and Estimated Average Requirement (EAR). These reference values are being developed for life stage and gender groups in a joint U.S.-Canadian activity. This report, which is the second in a series, covers the DRIs for folate, other B vitamins (thiamin, riboflavin, niacin, vitamin B6, vitamin B12, pantothenic acid, and biotin), and choline.
REFERENCES
Beaton GH. 1994. Criteria of an adequate diet. In: Shils ME, Olson JA, Shike M, eds. Modern Nutrition in Health and Disease, 8th ed. Philadelphia: Lea & Febiger. Pp. 1491–1505.
COMA (Committee on Medical Aspects of Food Policy). 1991. Dietary Reference Values for Food Energy and Nutrients for the United Kingdom. Report on Health and Social Subjects, No. 41. London: HMSO.
Demirjian A. 1980. Anthropometry Report. Height, Weight, and Body Dimensions: A Report from Nutrition Canada. Ottawa: Minister of National Health and Welfare, Health and Promotion Directorate, Health Services and Promotion Branch.
Elia M. 1992. Energy expenditure and the whole body. In: Kinney JM, Tucker HN, eds. Energy Metabolism: Tissue Determinants and Cellular Corollaries. New York: Raven Press. Pp. 19–59.
FAO/WHO/UNA (Food and Agriculture Organization of the United Nations/ World Health Organization/United Nations). 1985. Energy and Protein Requirements Report of a Joint FAO/WHO/UNA Expert Consultation. Technical Report Series. No. 724. Geneva: World Health Organization.
Garby L, Lammert O. 1984. Within-subjects between-days-and-weeks variation in energy expenditure at rest. Hum Nutr Clin Nutr 38:395–397.
Herman-Giddens ME, Slora EJ, Wasserman RC, Bourdony CJ, Bhapkar MV, Koch GG, Hasemeier CM. 1997. Secondary sexual characteristics and menses in young girls seen in office practice: A study from the Pediatric Research in Office Settings Network. Pediatrics 99:505–512.
IOM (Institute of Medicine). 1997. Dietary Reference Intakes for Calcium, Phosphorus, Magnesium, Vitamin D, and Fluoride. Washington, DC: National Academy Press.
Pett LB, Ogilvie GH. 1956. The Canadian Weight-Height Survey. Hum Biol 28:177– 188.










