
7
Monitoring and Reporting
In addition to the specific aspects of the study charge addressed in earlier chapters of this report, this committee was charged with making recommendations on the creation of an annual reporting mechanism on the status of cancer research among ethnic minority and medically underserved populations. This chapter offers a discussion of the different measures of process (e.g., the number of research grants targeted to the study of cancer in ethnic minority and medically underserved populations) and outcomes (e.g., cancer incidence and mortality statistics) that could be included in such a report and provides relevant recommendations.
The committee first reviewed prior congressional requests relevant to the reporting of cancer research in general. A prior Senate Committee on Appropriations had expressed concern about the increasing incidence of cancer and rates of mortality from cancer, especially among people ages 55 and older (U.S. Congress, Senate, 1990). Although the Senate committee commended the National Cancer Institute (NCI) for its "success in generating information and understanding of many fundamental biological processes at the cellular and molecular levels" (p. 89), it was concerned that the translation of this information into better prevention and treatment had not resulted in decreased rates of mortality. It requested that NCI convene a special committee to recommend the most appropriate measures for assessing progress against cancer.
In appropriating funds for the National Institutes of Health (NIH) for
fiscal year 1997 (P.L 104–208), the Senate Appropriations Subcommittee on Labor, Health and Human Services, and Education focused on cancer in ethnic minority and medically underserved populations. The legislation stated that "cancer crosses all groups in America, but often takes its deadliest toll among minorities and the medically underserved." As examples, it quoted a higher rates of cervical cancer among Hispanic women and prostate cancer among African-American men, and lower rates of survival from lung cancer among Native Americans. The latter Senate committee expressed similar concern about cancer among ethnic minority and medically underserved populations that the prior Senate Committee on Appropriations had expressed about cancer among older members of the general population. It recognized that NIH support for research, training, recruitment, and information dissemination regarding minority health issues had improved; but it was concerned that this segment of the population continued to experience disproportionately higher risks for cancer. The Senate committee believed that "the gravity of this issue demands that every appropriate effort be taken to ensure that the programs and the activities of the Nation's chief medical research institution produce long-term gains against cancer that will benefit all Americans."
Both Senate committees sought a better mechanism for monitoring and reporting of results that will affirm a commitment to equity. For this reason the Institute of Medicine Committee on Cancer Research Among Minorities and the Medically Underserved reviewed the response to the previous Senate Committee on Appropriations request for information on cancer among older Americans, with the hope that the mechanisms suggested for reporting on ethnic minority and medically underserved populations would be consistent with the mechanism for reporting on the rest of the population. In accordance with the Senate request for information on older Americans, the Extramural Committee, chaired by Lester Breslow, was formed to assess measures of progress against cancer (Extramural Committee to Assess Measures of Progress Against Cancer, 1990). That committee approached the problem of reporting from the perspective of linking the population with the problem of cancer and linking the processes of cancer intervention with measurable results. Similarly, this chapter first discusses the reporting of results and then discusses the reporting of certain processes in cancer research that relate specifically to ethnic minority and medically underserved populations. The committee distinguishes between monitoring and reporting, the former being a continuous activity, and the latter serving an intermittent activity.
Reporting of Results
Ethnic Minority Groups
At the beginning of the 20th century, health statistics classified the U.S. population into two groups: the white population and everyone else, who were simply non-white. By about the middle of the century, African Americans were recognized as a specific group. During the civil rights movement, however, there was not consensus, even among African Americans, about the use of racial designations. Some felt that racial designations would be used to support racism, but others thought that the use of racial designations was useful for purposes of health planning and assessing the improvement of health status. At this time, the cancer mortality rate among African Americans was just beginning to exceed that among whites. Classification schemes were totally based on race, and Hispanics were not identified. There was a further problem of classification when Hispanics were identified, because they did not fit the usual racial designations. As a result it was necessary to further identify Hispanic whites and non-Hispanic whites. The classification then became racial and ethnic. All other ethnic groups were included in the "Other" category.
With the increasing diversity of the U.S. population, it has become clear that racial designations are inadequate, confusing, and misleading. At the same time there is increasing demand to recognize the identities of the various ethnic groups included in the U.S. population. Until recently there was no routine reporting on cancer among ethnic minorities other than African Americans. This was corrected by the Surveillance, Epidemiology, and End Result (SEER) program monograph entitled Racial/Ethnic Patterns of Cancer in the United States 1988–1992 (Miller et al., 1996). That report, however, does not include data on the medically underserved population, and the source documents from which reports such as that of Miller et al., (1996) are prepared do not provide such information. The problem, then, is to find a method of reporting on cancer information that routinely includes data on ethnic minority and medically underserved populations without at the same time producing an excessive amount of data.
Health statistics are usually described as rates that are calculated from a numerator (numbers of people affected) and a denominator (the numbers of people in the population at large). The denominator is discussed first. In classifying the population, the committee has taken into account the fact that the census and all government agencies must conform to U.S. Office of Management and Budget (OMB) Directive No. 15 (U.S. Office of Management and Budget, 1977) and subsequent revisions. That classification reflects the old notions of four races. An important change would
be to discontinue use of the old and divisive racial classifications and to recognize the scientific view that all humans are members of one race. The population would then be classified into ethnic groups. Under this arrangement, Hispanics and whites would not be divided. One may choose to be identified either as Hispanic or as white. Pending this change, NCI could simply omit the term ''racial" from its titles without doing any harm to the War on Cancer or acting in violation of OMB Directive No. 15. All Hispanics would then be classified as Hispanics or whites by self-identification. This would also allow NCI to avoid violating another important principle of classification: that the categories be mutually exclusive and totally exhaustive. It should not be possible for a person to be placed into two different groups simultaneously, and the system should accommodate the entire population.
This change would not be merely semantic, because it would avoid some of the ambiguity that currently decreases the reliability of calculations. Data for all ethnic groups could be reported in this way, but because of the increasing diversity of the U.S. population, it would still be necessary to aggregate small population groups into "macro-ethnic" groups. As noted earlier, "macro-ethnic" groups include, for example, Asian-American populations (whose subgroups include individuals of Chinese, Japanese, Korean, Indian, Southeast Asian, and other Asian descent). This becomes important because in the smallest population groups the number of cases of cancer will be small and the calculated rates will be unstable or unreliable. In addition, in reporting on ethnic minorities it is useful to present data on the rest of the population to make the classification complete for purposes of comparison.
The top margin of a summary table on cancer mortality could be as follows:
|
Ethnic Group A |
Ethnic Group B |
Ethnic Group C |
Ethnic Group D |
All Others |
Total |
Medically Underserved Populations
Data on the medically underserved population are not usually included in cancer statistics reports. The information could be obtained by revision of the source documents to include the necessary data or by special studies. Implementation of the required changes will take time, but the revision of source documents would have a more permanent effect. The source document for calculating incidence could be modified to include this information. Retrieval of the information from the death certificate may be more problematic. For this reason it may be better to obtain the
necessary data from the cancer incidence registries. Data may come from other databases such as those that are part of the Medicare program, but in that case, it would also be necessary to extrapolate the data to the general population. There may also be some differences of opinion about what should characterize the status of medically underserved individuals. Possible factors could include socioeconomic status, access to care, or occupation. The National Center for Health Statistics (NCHS) is already exploring ways of providing such information, as reported in Health United States, 1998 (National Center for Health Statistics, 1998).
Ideally, it would be best if the medically underserved status could be displayed in the same table with the ethnic group status, since the medically underserved status would cut across all ethnic groups. In that case the data for medically underserved and non-medically underserved individuals would be shown for each ethnic group. For the sake of clarity, however, it might be best to show the relationship between the two variables and cancer in separate tables, and until the data for medically underserved individuals can be incorporated into source documents, it may be necessary to obtain the information by performing special studies or by linkage with other databases.
Many Cancer Sites
Cancer is not a single disease, and the complexity of the disease combined with the increasing diversity of the population makes it necessary to group various forms of cancer for purposes of planning and control, in the same way that it is necessary to aggregate smaller ethnic groups into macro-ethnic groups. It is customary to focus on those forms of cancer that present the greatest risk because of the magnitude and severity of the problems involved. In recent years the major causes of death from cancer in the United States among all ethnic groups have been cancers involving the lung, female breast, prostate, and colon-rectum. It is important that these forms of cancer be identified when one attempts to assess progress against cancer for the nation as a whole. If one ranked the top five causes of death for each ethnic group, however, the list would be different for each ethnic group, and herein lies the importance of monitoring and reporting on cancer among different ethnic groups. Cancer of the cervix, for example, is not among the five leading causes of death among white women, but it is among African-American women. It may also be among the top five for white women who are medically underserved, but this group is not currently considered in reports of the causes of death. Cancer of the breast is the leading cause of cancer death among Hispanic women, but cancer of the lung is the leading cause of cancer death among white women. If one groups the categories by giving priority to the burden of
cancer, then all the major causes of death for all ethnic groups must be included. Although cancers at many sites are continuously monitored, reporting should routinely focus on the sites associated with the greatest burden of cancer while aggregating data on cancers at other sites.
Aggregation of deaths from cancer from those causing the highest rate of mortality to those causing the lowest rate of mortality is only one approach to the problem. The Breslow Committee suggested consideration of three other alternatives: cancers that can be grouped according to preventable cancers, cancers that can be controlled by timely screening and detection, and cancers against which efficacious treatments exist (Extramural Committee to Assess Measures of Progress Against Cancer, 1990). These alternatives would facilitate easy linkage to the present state of knowledge and practice with respect to prevention, control, and treatment. Whatever aggregation method is used, the objective would be to avoid the overwhelming amount of data that would be accumulated if the data included all possible types of cancer for all ethnic groups. As in the case of the group by ethnic groups, the aggregation should include entries for "all other sites" and for total sites.
The left margin of the table would then appear as follows:
|
Site A |
|
Site B |
|
Site C |
|
Site D |
|
All other |
|
All sites |
Reporting on Mortality
Despite the problems associated with recording and coding of deaths, the mortality data remain the most important measure of success of the efforts being made against cancer. The denominator data for calculation of the rates are derived from the census and the numerator data are derived from death certificates. The mortality data are obtained from NCHS of the Centers for Disease Control and Prevention. Reported data would be the most recent available, which currently means information on events that occurred 2 or more years prior to publication. A separate table could then show changes in mortality, and it is the change or lack of change that
becomes the basis for discussions about progress. For those who are intimidated by statistics, presentation of the same trends in graphical form may be important.
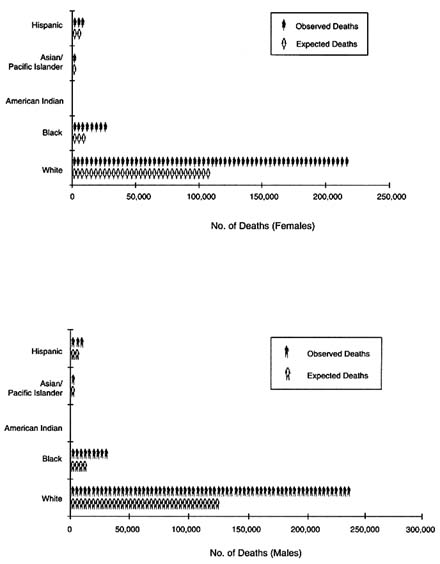
Another alternative is to present the data in terms of "potential reduction of deaths." Various ethnic groups experience different rates of mortality from cancer at different sites. The reasons for these differences are not always clear, but one could construct a hypothetical U.S. population based on the lowest rates of each of the leading causes of cancer in any ethnic group. Using this as a reference population, one could compare the number of deaths that now occur in each ethnic group with the number of deaths that would have occurred in the hypothetical population with the best rates at major sites drawn from any ethnic group. The difference between the number of deaths that occurred and the number that would have occurred in the hypothetical population would be the potential reduction. This could also be expressed as the percent potential reduction, and it would be the goal of the cancer program to approach the "all American best rate" for all ethnic groups.
The committee asked NCHS to do such calculations, and their findings are significant (Figure 7-1). The total observed annual numbers of deaths from cancer among men for the period covered (1990 to 1995) was 276,146, but if the rate of cancer among all Americans was the lowest rate of cancer for any ethnic group, the expected number of deaths among men would have been 137,476. This is a potential reduction of 138,670 deaths, or 50 percent. The potential reduction for women was comparable. The white population, because of its majority size, would have experienced the greatest reduction in the number of deaths. The African-American population would have experienced the greatest percent reduction because of its greater burden of cancer. A more rigorous study of cancer among the various ethnic groups of the United States would be of great help in achieving the potential reduction in the numbers of deaths from cancer. Each ethnic group could set its own target on the basis of its own potential reduction and participate fully in the effort to reach the target. In the same manner, targets can be set for the medically underserved population when data are collected for this group.
The entire report (National Center for Health Statistics, 1998) of NCHS is included in Appendix F, but the caveats deserve special consideration, and are fully stated here.
|
1. |
Quality of data varies by "race" and ethnicity in both death certificate and Census data. The quality of data for the white and the African-American populations are good in contrast to that for other groups. American Indian data are estimated to be underreported by about 10 percent. With respect to population data, perhaps the most serious problem is the |
|
|
reported 33 percent increase in the American Indian population between 1960 and 1990 that reflects increased preference to self-report as an American Indian. |
|
2. |
Age-specific death rates, especially those for the elderly, are under-reported. |
|
3. |
Hispanic origin and "race" are separate items. NCHS picked the best rates going across these two variables, but show the deaths for both Hispanic origin and "race." |
|
4. |
Hispanic origin was not reported on all state death certificates in this time period. The rates used in the calculation were based on 46 states and the District of Columbia. The observed death count was inflated to a national total by using the reciprocal of the fraction of the Hispanic population living in these 46 states and D.C. |
|
5. |
The number of events, particularly at young ages for certain ethnic minority groups, are small. This would affect the stability of the rates. To counter that tendency, NCHS used data for the 1991–95 time period. In the summary table, NCHS has expressed the number of deaths in terms of a single year of data. |
|
6. |
The reduction for all cancer sites combined differs depending on whether the values are summed across specific sites or is done separately. The reduction is greater when the values are summed. |
These cautions are valid regardless of the approach that is used and serve to indicate the limitations of the data that one continuously faces. Any or all of the methods could be used whether the primary focus is on the general population, on ethnic minority groups, or on the medically underserved population.
It may be useful to present the information in several forms. Another method would be to measure progress against the objectives defined for the nation, such as the objectives outlined in Healthy People 2000 (U.S. Public Health Services, 1991) or Healthy People 2010. The national objectives are set on the basis of what is known to be preventable. Objectives were set for total cancers and for cancers of the lung, breast, cervix, and colon-rectum. The objectives were based on the assumptions of improved tobacco control, increased rates of use of mammography and the Pap smear, and both the early detection of and improvements in treatments for colorectal cancer. Goals were not set for prostate cancer, awaiting evidence of methods of effective prevention or treatment. In some cases Healthy People has set specific targets for some ethnic minority groups.
The summary data can be refined and presented in separate tables on the distribution of cancer by age and sex for each ethnic group, averages over a specific period, annual rates, and trends over a prolonged period. The trends in mortality are very important because this is a matter of
prime interest to Congress and to the public at large. For example, Congressman Louis Stokes has repeatedly asked at appropriations hearings about the rate of mortality from cancer among African Americans. He is quoted as having recently asked the director of NCI the following question on behalf of the American people: "Last year, you told us that African American men had the highest rate of prostate cancer in the world. Is that still the situation?" (Cancer Letter, 1998). This is one reason why the trends in mortality should be the primary basis of reports to Congress. A graph showing trends is often more powerful than a large display of numbers. The trends may show progress, no progress, or a worsening of the cancer problem.
Other Measures of Progress
In addition to mortality it is important to include information on trends in incidence and survival. If either prevention or treatment has not been able to be affected, the mortality rate will be unchanged. Under these circumstances it is helpful to be able to explain that even though the case fatality rate is unchanged, there has been an improvement in the length of survival. Sometimes this improvement is small, measured in days to a few months, but sometimes differences in lengths of survival provide clues to patterns of cancer treatment and access to cancer care, and increased lengths of survival may be important, especially if the quality of life is good. In the attempt to explain changes in the rates of mortality from cancer among the various ethnic groups, it is therefore necessary to present evidence not only on mortality but also on incidence and survival.
The incidence and survival data are provided by the SEER program at NCI and are usually presented in the same format as the mortality data, in which the rates for various cancer sites and ethnic groups are presented, and the data are refined to show distributions by age and gender. The Breslow Committee indicated that the SEER program's system is of very high quality but did "not provide sufficient data about the occurrence of cancer in important segments of the population" (Breslow et al., 1990, p. 827). This would have been true with respect to ethnic minority and medically underserved populations. This problem has been partially addressed by a report that appeared in 1996, Racial/Ethnic Patterns of Cancer in the United States 1988–1992 (Miller et al., 1996). In discussing the incidence data, it is necessary to emphasize what progress in increasing the efficacy of prevention efforts has been made and how this progress could influence the incidence of cancer reported for each ethnic group. This would relate the knowledge to the statistical findings and especially to the mortality data.
It is then helpful to provide information on early detection, treatment,
and survival. This could be related to current knowledge about carcinogenesis, early detection, and treatment and to steps that could alter the outcome. As in the case of mortality data, the incidence and survival data report events that may be 2 or 3 years older than current knowledge. These data are associated with their own set of problems that are different from those for the mortality data and require explanation. For example, an increase in incidence could mean a real increase in the rate of occurrence of the disease, or it might reflect an increase in the aggressiveness of screening.
Despite these problems, an explanation for the occurrence of progress is not difficult when in fact there is progress. The problems that have arisen in the past have largely been due to a lack of improvement in the measures that one usually considers strong evidence of progress. Previously, the mortality data did not coincide with the impressive reports of progress reported in scientific articles and press releases. Members of the public and their representatives expected better results, but some scientists appeared to confirm the idea that real progress had been made. This confusion was understandable in view of the fact that the mortality rate from cancer was increasing 0.4 percent per year from 1973 to 1990. The evidence of progress was easily accepted when there was evidence of a significant decrease of 0.5 percent per year from 1990 to 1995. However, differences with respect to the causes of the decline were expressed. According to John Bailar, the government had no role in directing the improvements. In his opinion the improvements were due to the decisions of millions of individuals to improve their lifestyles (Bailar and Gornik, 1997). The decline in the rate of mortality from cancer at all sites combined was greater for blacks and Hispanics than it was for whites, whereas the rate of mortality from cancer among Asians and Pacific Islanders was unchanged.
The problem is more difficult when no progress with respect to mortality can be reported. Under these circumstances it is most critical to consider additional measures, but consideration of all available measures helps to clarify the rates of mortality from cancer and may suggest additional areas where improvements are possible. In addition to the direct measures of the rate of mortality from cancer, the incidence rate, the survival rate, and quality of life, the Breslow Committee recommended the inclusion of indirect measures (Extramural Committee to Assess Measures of Progress Against Cancer, 1990). Examples included smoking rates, levels of alcohol consumption, rates of use of the Pap smear and mammography, treatment by protocol, quality of laboratory tests, patterns of care, and psychosocial factors such as time hospitalized, levels of drug use, and time to return to work after the occurrence of cancer. These measures of progress would be used where relevant. In this way the reports are both outcome and process oriented.
Special Process Items
The U.S. Congress has been interested in results, but it is also interested in the process. In the case of ethnic minority and medically underserved populations, it is aware that unless there is a specific focus on their problems, they are likely to be ignored. Congress is therefore seeking a reporting mechanism that will permit members to be assured that issues of research on cancer among ethnic minority and medically underserved populations are not ignored. The dominant strategy of NIH of supporting investigator-initiated research is a perfect mechanism for ignoring ethnic minority and medically underserved populations. It is commendable that NCI plans to be more inclusive in its research activities and include ethnic minority and medically underserved populations as part of the general research program, but that is not enough. The Senate Committee report suggests that it wants to know about an NIH strategy for specifically targeting the cancer research needs of these groups over and above a general statement of inclusion. For this reason the Senate is not likely to be impressed by statistical analyses that ignore the questions concerning the relative share of NIH resources allocated to cancers disproportionately affecting medically underserved and ethnic minority populations.
A section added to specific reports should include the following statements:
- a statement of research programs specifically targeted toward ethnic minority and medically underserved populations;
- a list of ethnic minority scientists who have participated in decision making and performed research in the programs that have been outlined
- a list of ethnic minority scientists and researchers who have proposed concepts that might be the basis of research activities; and
- a statement of the method by which communication has been established between NCI and ethnic minority and medically underserved communities and the extent to which the communication is two-way and effective. The statement should include some of the major issues of discussion, including issues of survivorship.
This opens for NCI a more democratic process that should increase NCI's effectiveness with ethnic minority and medically underserved populations.
Linking Research Findings
Another approach to reporting is to assume that the overall strategic objective of the research program is to reduce rates of mortality from
cancer. The objective is achieved by research that focuses on understanding the mechanisms of cancer development, testing the efficacies of interventions for prevention and treatment, and testing the effectiveness of interventions in the general population. The results of such research can be reported by providing such quantitative measures as mortality rates, incidence rates, survival rates, and qualitative measures such as quality of life. This can be followed by a discussion of the new knowledge related to the findings. It may be that despite the improvements in knowledge there is no improvement in results because that knowledge has not yet had time to be applied or is not being applied to the extent possible. The discussion would also explain where there are gaps in knowledge that hinder progress. These gaps become the basis for the future research agenda, which could include a modification of the present strategy. There may also be gaps in the research process, such as the availability of adequately trained investigators in prevention research.
Regardless of what research is done, the War on Cancer cannot be won by NCI. This war will require much work at the individual level, and NCI can claim neither all of the credit nor all of the blame.
The linking of progress to advances in research has several consequences. It becomes clear that progress against cancer depends not only on good research but also on the application of the knowledge derived from that research. The use of that knowledge goes beyond the domain of the research community. Much of it depends on the actions of individuals, but the research community can help by doing a more effective job of educating professionals and the public and analyzing the reasons for the failure to put knowledge into practice. It would appear that NCI has not given enough attention to this matter and that it may be necessary for some other entity to fill this gap, especially for ethnic minority and medically undeserved populations. This method of reporting would emphasize both results and process and would suggest possible changes in strategy. Without the linkage it is easy to understand the suspicion among ethnic minority and disadvantaged individuals that NCI is more interested in describing than in improving. Furthermore, stating the necessary change in strategy, if any, that results from the findings would permit the U.S. Congress to understand NCI's priorities and would support requests for funding.
Types and Timing of Reports
Reports on the incidence of cancer among ethnic minority and medically underserved populations may be presented in several forms, depending on the purposes and the audience for which they are intended. The most important report would be a summary report intended for the U.S.
Congress and the public. Such a report would not attempt to describe the status of each of the more than 100 diseases classified as cancer, nor would it attempt to describe all possible ethnic groups. Ethnic groups and cancer sites would be aggregated. The five cancer sites responsible for the highest rates of mortality from cancer and the macro-ethnic groups representing the largest segments of the population would be included. These macro-ethnic groups would be white, African American, Hispanic, Asian American (including Pacific Islanders), and Native American. Data for medically underserved individuals may be included as subgroups of data for all ethnic groups in the same table or may be included in a separate table. The report would include all the features mentioned above, including rates, explanations of rates on the basis of current knowledge, gaps in knowledge, and changes in strategy. This summary report would be issued every year.
Another type of report, a special report, would focus on one macro-ethnic group including the medically underserved population. This would permit expanded coverage of a specific ethnic group and its components in comparison with other ethnic groups. This coverage would be summarized but would also include data for a larger range of cancer sites. For example, it could report on data for Asian Americans but would include data for the subgroups of Asian Americans not included in the summary reports. The report would cover the same results and process areas as the summary report. It would also be a report to Congress and the public but would have a more limited circulation since it would be especially targeted to the one or two macro-ethnic groups involved. Because some of the ethnic groups have small populations in terms of the overall U.S. population, it is less likely that there would be statistically observable and reliable differences over a short time. For this reason, a 5-year period would be appropriate for any one group, but the reports may appear annually and may feature a different ethnic group, with the different ethnic groups covered in some form of rotation.
Summary
The reporting to the U.S. Congress and the public should first focus on results and trends primarily by use of mortality data. Progress will not be dramatic but it should be steady. The statistics can be presented in a variety of ways to increase their clarity to a wider audience. One can also examine the processes of early detection, prevention, and treatment as contributing factors. Two kinds of reports have been suggested to be submitted annually. To address the additional concerns of Congress with respect to ethnic minority and medically underserved populations, it has been suggested that a special section of the appropriate reports include
specific statements about strategies, targeted programs, participation by ethnic minority and medically underserved populations in the process, and communication between these communities and NCI. Although the Senate report refers to NIH, most suggestions have been directed toward NCI as the principal focus for cancer research. At the same time, it is clear that progress against cancer is not totally dependent on NCI and the research that it funds.
Recommendation 7-1: The committee recommends a regular reporting mechanism to increase NIH accountability to the U.S. Congress and public constituencies. Such reports should
- report on data on progress against cancer using the nomenclature ''ethnic groups" rather than "racial" groups and include data on medically underserved populations with ethnic group data;
- provide data on the incidence of cancer at several cancer sites, including those cancers that disproportionately affect ethnic minority and medically underserved populations;
- consider as one alternative reporting of mortality data in terms of "potential reduction of deaths," a statistic that is based on the lowest mortality rate among U.S. ethnic groups and that emphasizes the need for cross-cultural studies to ascertain optimal strategies for cancer prevention, treatment, and control;
- link research findings to reductions in cancer incidence and mortality and identify any gaps that may occur in this linkage; and
- report on "process" developments, such as the number and type of research programs specifically targeted to ethnic minority and medically underserved groups and the contributions of ethnic minority scientists and community groups to the research priority-setting process.















