
2
CAN MARIJUANA HELP?

Current knowledge about marijuana's effects derives from three main sources: personal and historical accounts of its use, a limited number of clinical studies, and basic scientific research on marijuana and its constituent compounds. Clinical studies, which are discussed in Part II of this book, measure the overall effects of drugs on human subjects. Basic research, on the other hand, examines the specific effects of drugs on cells and on the biochemical reactions that take place within them. Basic studies have been conducted to characterize the chemicals found in marijuana, their interactions with molecules and cells in the human body, and their effects on experimental animals.
The most readily available information on medical marijuana can be found in historical documents—some more than a thousand years old —as well in the personal stories of people who have taken the drug to relieve medical symptoms. In addition to such anecdotes, scientific research recently has begun to reveal clues to marijuana's potential benefits. This chapter presents a broad summary of both anecdotal and basic scientific evidence of marijuana's promise as a source of medicine.
A BRIEF HISTORY OF MEDICAL MARIJUANA
The marijuana plant—also known as hemp and cannabis—has been used throughout agricultural history as a source of in-

FIGURE 2.1 The Chinese ideogram for marijuana (“ma”) shows two plants, male and female, under a drying shed. (Drawing from Cannabis in Medical Practice, M. L. Mathre, ed., McFarland and Company, Inc., 1997, p. 36.)
toxicant, medicine, and fiber. The earliest known descriptions of marijuana appear in the ancient writings and folklore of India and China, where historians believe it was first used as a ritual intoxicant. Eventually, marijuana was put to common use in folk medicine, usually in the form of a tea or edible extract. The medicinal use of smoked marijuana is largely a recent phenomenon.1
According to Chinese legend, the emperor Shen Nung (circa 2700 B.C.; also known as Chen Nung) discovered marijuana's healing properties as well as those of two other mainstays of Chinese herbal medicine, ginseng and ephedra. In a compendium of drug recipes compiled in 1 A.D., based on traditions from the time of Shen Nung, marijuana is depicted as an ideogram of plants drying in a shed (see Figure 2.1). This ancient text, which is considered to be the world's oldest pharmacopoeia, recommends marijuana for more than 100 ailments, including gout, rheumatism, malaria, and absentmindedness. Centuries later a Chinese medical text (1578 A.D.) described the use of marijuana to treat vomiting, parasitic infections, and hemorrhage. Marijuana continues to be used in China as a folk remedy for diarrhea and dysentery and to stimulate the appetite.2
In India, marijuana has been associated with magic and religion—as well as healing—for thousands of years. Practitioners of traditional Ayurvedic medicine still prescribe marijuana to promote sleep, appetite, and digestion as well as to relieve pain; it is also considered an aphrodisiac and intoxicant.
By contrast, ancient Greek and Roman physicians cautioned that excess use of marijuana could dampen sexual performance.3 Despite this drawback, Galen (2 A.D.) and Pliny the Elder (circa 25 A.D.) as well as Discorides—a doctor in the army of the Roman emperor Nero (1 A.D.)—recommended marijuana as a treatment for a variety of ailments, including earache.
Marijuana's double nature—harmful intoxicant versus beneficial medicine—was debated at least as early as the fifteenth century. At that time, Muslim theologians were faced with the question of whether hashish (a potent drug made from marijuana resin) should be treated like alcohol, which is specifically forbidden by the Koran. In solving this dilemma the scholars distinguished between the use of hashish as an intoxicant, for which they recommended punishment by brutal whipping, and its permissible use as a medicine.4
Muslims also invented techniques to manufacture paper from hemp fibers, a process that was introduced to Europe during the twelfth century. Hemp remained an important component of most paper products until the mid-nineteenth century, when it was replaced by wood pulp. Arab traders are also thought to have conveyed their knowledge of hemp 's medicinal properties to Africa during medieval times. There marijuana came to be widely used to treat a variety of ailments, including snakebite, labor pains, malaria, and dysentery.5
By contrast, there is little evidence that marijuana was used as a medicine in medieval Europe. During the Renaissance, reports from explorers in Asia, Africa, and the Middle East piqued the interest of European herbalists, who also consulted the writings of Galen, Pliny, and other ancient physicians. Nevertheless, medical marijuana continued to be a rarity in the West.6 Meanwhile, demand for hemp fibers as a material for making rope and textiles—especially canvas for sails—grew so strong that by the sixteenth century European nations commanded their colonies to grow the crop. There is, however, no evidence that colonists used the plant for anything but its fiber. It was not until the mid-nineteenth century that Western medicine “discovered” marijuana (see Figure 2.2).7
It was an Irish doctor, William O'Shaughnessy, who was largely responsible for acquainting his Western colleagues with marijuana's healing properties. O'Shaughnessy learned of the herb as a professor at the Medical College of Calcutta. In the 1830s, he created marijuana preparations and tested their effects on animals; convinced that they were safe, he began administering them to patients as a treatment for pain and muscle spasms. He also
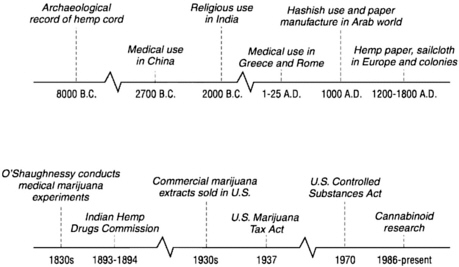
FIGURE 2.2 Medical marijuana timelines.
reported success in using marijuana to treat the often-fatal vomiting and diarrhea associated with cholera.8
O'Shaughnessy's discoveries fascinated physicians in Europe and America, provoking a flurry of Western research on medical marijuana that lasted well into the twentieth century. Hundreds of Indian and Western doctors described marijuana's medical benefits before the Indian Hemp Drugs Commission, convened by the British in 1893-1894. They told of treating cramps, headache, asthma, diabetes, impotence, acute and chronic pain, fever, appetite loss, and scores of other conditions with the plant. On the basis of this testimony, members of the commission concluded that marijuana represented one of the most important drugs in the Indian pharmacopoeia and that “moderate use of hemp drugs is practically attended by no evil results at all.” Thus, the commission recommended against marijuana's prohibition, despite acknowledging the problems posed by its abuse as an intoxicant.9
At the first American conference on the clinical use of marijuana, held by the Ohio State Medical Society in 1860, physicians reported success in using marijuana to treat chronic cough, gonorrhea, pain, and a variety of other conditions. As demand for
marijuana-based medications accelerated, pharmaceutical firms attempted to produce consistently potent and reliable drugs from hemp. By the 1930s at least two American companies—Parke-Davis and Eli Lilly—were selling standardized extracts of marijuana for use as an analgesic, an antispasmodic and sedative (see Figure 2.3). Another manufacturer, Grimault & Company, marketed marijuana cigarettes as a remedy for asthma.10
But shortly after pure marijuana preparations became available, more effective synthetic drugs such as aspirin and barbiturates began replacing herbal remedies. Meanwhile, recreational marijuana smoking became popular among jazz-age musicians and artists in the United States and with it claims that it caused crime, mental illness, and even death. Against the advice of the American Medical Association, the U.S. Congress passed the Marijuana Tax Act of 1937, which imposed tough restrictions on marijuana sales and prescription. As a result, most pharmaceutical companies ceased producing marijuana-based drugs. In 1942 marijuana was removed from the United States Pharmacopoeia (USP) on the grounds that it was a harmful and addictive drug.11
Interestingly, marijuana is not the only drug that has progressed, over the ages, from folk medicine to conventional treatment to highly regulated substance of abuse. The narcotic opium, produced from the dried resin of immature poppy flowers, has been used as a pain remedy for nearly 2,000 years. Taken by mouth, its effects are too weak to encourage abuse. But after smoking opium—which rapidly induces an intense “high”—became popular in seventeenth-century China, many people became addicted to the drug.
Opium soon made its way into Europe and North America, where it was both used as a painkiller and abused by addicts. The pure compound morphine, first isolated from opium in the early eighteenth century, gained wide use as an analgesic, particularly during surgery. Heroin, a chemical derivative of morphine, and codeine, another natural opiate, also were developed as painkillers. As with cannabinoids, the human body produces its own version of opiates, known as endorphins. These compounds interact with nerve cells in the same way as their plant-derived relatives, with similarly soothing results.
Although natural and synthetic opiates are among the most
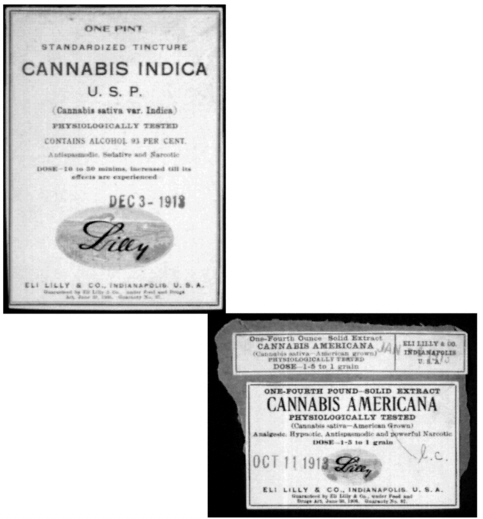
FIGURE 2.3 Lables from patent medicines that contained marijuana. (Courtesy of Eli Lilly and Company Archives.)
effective pain relievers, they are highly regulated due to their great potential for abuse. As a result, many doctors hesitate to prescribe opiate medications except in extreme cases. Nevertheless, opiate abuse is so widespread that the illegal demand for opium far exceeds legitimate medicinal sales of the drug.12
More than a century after opium abuse spread across the globe, marijuana gained worldwide popularity as a recreational drug. By the 1960s, marijuana use had become widespread, and in 1970, the U.S. government passed the landmark Controlled Substances Act. This law organized all drugs with abuse potential into five schedules, according to three criteria: the likelihood that the drug would be abused, its medical usefulness, and the
physical and psychological consequences of its abuse. Marijuana, along with LSD and heroin, was placed in Schedule I, the most restrictive category. Schedule I substances are considered to have no medical use and a high potential for abuse.
That classification continues to be challenged by the National Organization for the Reform of Marijuana Laws and medical marijuana advocates. In addition, since passage of the federal Controlled Substances Act, several states have placed marijuana in a less restrictive category in their own controlled substance laws. In the 1970s and 1980s several states even supported limited clinical studies on medical marijuana. Voters in several states have passed referenda intended to permit marijuana use for medical purposes (see Chapter 11).
USERS' VIEWS
Despite its illegality, millions of Americans use marijuana regularly. A small minority—most of whom had previously used the drug recreationally —smoke or eat it to relieve various medical symptoms. In three public hearings held by the IOM as part of its study of medical marijuana, 43 such patients came forward to relate their experiences (see Figure 2.4); the research team also
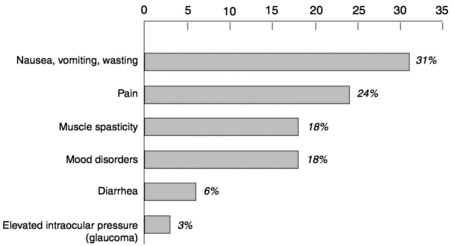
FIGURE 2.4 Reported medical uses of marijuana. Frequency of symptoms among 43 patients who spoke at the IOM's public workshops. Twenty of these patients reported using marijuana to relieve more than one symptom.
spoke with several dozen members of three medical marijuana buyers ' clubs in California. Patients described using marijuana to treat AIDS wasting, spasticity from multiple sclerosis, depression, chronic pain, chemotherapy-induced nausea, and other symptoms. Similar accounts of medical marijuana use in treating an even broader range of conditions appear in Marihuana: The Forbidden Medicine, by Lester Grinspoon and James Bakalar.13
AIDS was the predominant disorder described by medical marijuana users who told their stories to the IOM study team. Many such speakers said they used marijuana to combat wasting and to reduce the side effects of other medications. A typical account follows, presented by a 35-year-old Florida writer who discovered he was HIV-positive in 1987.
Skin rashes, dry mouth, foul metallic aftertaste, numbness of the face, swelling of the limbs, fever spikes, headaches, dizziness, anemia, clinical depression, neuropathy so crippling that I could not type, so painful that the bed sheets felt like sandpaper, nausea so severe that I sometimes had to leave the dinner table to vomit, and diarrhea so unpredictable that I dared not leave the house without diapers.
These are some of the horrors that I endured in the last 10 years during my fight for life against HIV [human immunodeficiency virus]. But these ravages were not caused by HIV itself, or by any of the opportunistic infections that mark the steady progression of AIDS. Each of these nightmares was a side effect of one of the hundreds of medications I have taken to fight one infection after another on my way to a seemingly early grave.
Had you known me three years ago you would not recognize me now. After years of final-stage AIDS, I had wasted to 130 pounds. The purple Kaposi's sarcoma lesions were spreading. The dark circles under my eyes told of sleepless nights and half-waking days. I knew that I was dying.
But still I was fortunate because along the way I rediscovered the ancient understanding of marijuana's medicinal benefit. So I smoked pot. Every day. The pot calmed my stomach against handfuls of pills. The pot made me hungry so that I could eat without a tube. The pot eased the crippling neural side effects so that I could dial the phone by myself. The pot calmed my soul and allowed me to accept that I would probably die soon. Because I smoked pot, I lived long enough to celebrate my thirty-fifth birthday. I lived to sit on the bus without frightening the passenger beside me.
Even at this stage of my recovery, I take a handful of pills almost every day, and will probably continue to do so for the rest of my life. While I am grateful for the life-saving protease inhibitor therapies, they bring with them a host of adverse reactions and undesirable side effects. Smoking marijuana relieves many of these side effects.
I sit here, I believe, as living proof that marijuana can have a beneficial effect in staving off wasting. I figured that every pound of body weight I could maintain, that was another day that I could live in hopes that some effective therapy would emerge.
Others described how marijuana helped them cope with nausea and vomiting during chemotherapy—symptoms that defied otherwise effective treatments:
I guess I am one of the luckier people who will be appearing before you today because my medical problem was testicular cancer. People do die of testicular cancer, but the cure rates are very high, 90 percent or over. There is one form of chemotherapy that seems to work.
Now the down side of the chemotherapy—it is one of the rougher [treatments]. The drug is called cisplatin, and it is known for the nausea that it induces. The legal antinausea drugs were pretty good. For my first two courses of chemotherapy I did not have a problem with nausea. However, by the end of the second course, I could tell that the effect of the Zofran [that I had been given to control my nausea] was wearing off. So, for my third and fourth courses of chemotherapy, I smoked marijuana.
None of my doctors and nurses discouraged me from doing this. I was being treated at NYU Medical Center in New York, and I went for a consultation at Memorial Sloan-Kettering. So I was getting the best possible care.
I found that when I smoked marijuana the effect came . . . in a couple of minutes, and the symptoms of nausea would go away. Interestingly, I did not consider taking Marinol [oral dronabinol, equivalent to THC], and my doctor did not recommend that I try [it]. What I was dealing with was nausea, and it didn't seem to me that taking a pill was a very intelligent or effective way to combat nausea.
I didn't find that it [smoking marijuana] impeded my work [the speaker is a well-known conservative journalist]. It certainly didn't turn me into a drug addict. I had smoked maybe a dozen times recreationally in college. I would never touch a joint again unless I got cancer again and I had to take it [to relieve nausea]. The mere thought of smoking something that is associated with the bad experience [of chemotherapy] is very aversive to me.
Similarly, one woman reported that marijuana helped her keep down her migraine medication:
I started smoking marijuana when I was 19, as a recreational drug. I had no idea of any sort of medical or therapeutic uses whatsoever. Three years before that I had been diagnosed with migraines, and I have suffered [from] them pretty continuously since that time. Right about 1989 or 1990, after I started using marijuana recreationally, a lot more information about marijuana started to become available. At that point I realized that maybe the convergence of my recreational use and my medical condition might be possible.
My doctor had prescribed a [migraine] medicine called Ergomar. It had really bad effects. The headache might go away or it might not. Either way I would definitely throw up if I took the medicine. [I switched to] Imitrex after that. Imitrex does work to remove my migraines, and marijuana never has been able to do that. But marijuana relieves my nausea enough that I can keep my pharmaceutical medication down.
Next to AIDS and chemotherapy-induced nausea, pain appears to be the most frequently cited reason for using medical marijuana. Like several individuals who addressed the IOM team, the following man found that marijuana improved the effectiveness of the narcotic medications he was already taking for pain:
I am a 35-year-old father [and] a United States Air Force disabled veteran. I came to know cannabis in the usual way for a baby boomer, [having] tried it in high school. I left behind cannabis and high school simultaneously in 1981, when I joined the Air Force.
I was serving in the South Pacific . . . when I fell victim to a poorly constructed roadway and crashed my motorcycle. I spent the better part of [the next] two years in and out of the hospital. Now, 14 years, 10 surgeries, and two artificial hips later, I sit before you. You would never guess the extent of my injuries or repairs. I lost parts of my spleen and intestines, and I get . . . awful cramping. I get pain that shoots down to my knee.
I owe a good deal of my excellent recovery to . . . cannabis. My pain medication [Percocet] is less effective without cannabis, and [if I don't use it] I'm forced to take too much narcotic. A few puffs . . . relieve the majority of my stomach spasms, completely eliminate nausea, and allow me to eat an entire meal instead of nibbling.
According to federal law, only eight people in the United States are currently allowed to smoke marijuana for medical rea-
sons. These patients receive marijuana cigarettes prepared by the U.S. government under a Compassionate Use Program, a program that has been closed to new patients since 1992. The surviving participants include this 41-year-old woman who managed her family's men's wear store until she developed multiple sclerosis. She smokes marijuana to relieve several symptoms of multiple sclerosis:
I was diagnosed with multiple sclerosis in 1988. Prior to that I was an active person with ballet and swimming. I [still] swim each day, and I smoke marijuana. Each month I pick up a can filled with the marijuana cigarettes rolled by the government.
At one time I weighed 85 pounds, and now I weigh 105 pounds. [Before I began smoking marijuana], I could not walk. I did not have an appetite. When I found out that there was a program to get marijuana from the government, I decided that was the answer. I was not a marijuana smoker before that; in fact, I used to consider the people I knew who smoked marijuana as undesirables. Now I myself am an undesirable.
But it works. It takes away the backache. With multiple sclerosis, you can get [muscle] spasms. You may have danced all your life . . . but the MS will take that from you. So I use the swimming pool, and that helps a lot. The kicks are a lot [easier] when I have smoked a marijuana cigarette. Since 1991 I've smoked 10 cigarettes a day. I do not take any other drugs. Marijuana seems to have been my helper.
Another legal marijuana user, this Florida woman described how in 1976 she began using the drug to relieve the symptoms of glaucoma. She received legal permission to use it in 1998:
When a doctor told me, a year after I had been diagnosed with glaucoma, that I had better start smoking marijuana, I questioned his sanity. He could see that I had already tried . . . Pilocarpine* and a stronger [drug]. Those gave me horrendous headaches, and I could not tolerate them at all. Diamox [another prescription drug for glaucoma] knocked me flat . . . At that point I realized that if I was going to save my sight at the expense of taking the rest of my body down, then it wasn't worth saving.
|
* |
Pilocarpine and Diamox were among the few drugs available to treat glaucoma in the late 1970s, but they are not popular today because of their side effects. Better glaucoma drugs with fewer side effects are now available. |
Compelling though these accounts are, it would be a mistake to use anecdotal evidence to measure marijuana's clinical value. Only thorough clinical studies can compare marijuana's effectiveness with that of existing medications. However, these anecdotal reports do define certain symptoms that warrant clinical investigation: nausea, wasting, pain, muscle spasms, and increased intraocular pressure.
Interestingly, the IOM study team did not receive any direct reports of less than positive experiences with medical marijuana. A few speakers did mention that they knew people whom marijuana had failed to help. Indeed, patients in several clinical studies have occasionally had adverse reactions to smoked marijuana, including anxiety, panic, and paranoia. These short-term effects appear to occur mainly among first-time and older users.14 It seems doubtful that anyone who reacted this badly to a medication would want to continue taking it, but it is unclear how many potential users of medical marijuana would fall into that category.
No drug—including conventional medications used to treat symptoms for which marijuana has been touted—is free of side effects, however. Medicines represent a balance of risks and benefits. But for marijuana and its constituent chemicals, no one can reliably predict which way that balance will tip for a specific patient.
CANNABINOID SCIENCE
Not long ago most medical treatment was based on anecdotal evidence. Only recently—and only in the world's wealthiest societies—have scientific standards replaced the oral traditions of folk medicine. Although many modern medicines are derived from plants used in traditional healing, they are purified compounds that conform to high standards of safety and efficacy. Thus, before marijuana-based medicines appear on pharmacists' shelves, they must undergo clinical testing to assure that they meet the same exacting standards.
But clinical studies of marijuana are currently difficult to conduct. Scientists interested in pursuing such research face a series of barriers, including limited funding and a daunting thicket of federal and state regulations. No wonder, then, that clinical evi-
dence for marijuana's benefits (discussed in Chapter 4, Chapter 5, Chapter 6, Chapter 7, Chapter 8 through Chapter 9) is limited indeed.
Yet despite the scarcity of clinical data, several biological studies indicate that marijuana-based drugs could potentially ease a variety of symptoms. These studies fall under the category of basic research and are intended to single out marijuana's many effects and study them individually in order to discover how chemicals in marijuana act on various cells and organ systems in the body. Some of these studies suggest that cannabinoids could be used as the basis for developing new, highly specific medicines with fewer side effects.
Biological studies also offer the possibility of finding new treatments by defining symptom-producing processes that occur in individual cells. Often these mechanisms take the form of chains of biochemical reactions that result in sensations such as pain or nausea—symptoms that might be averted if the chain were interrupted at any point. Thus, for any given symptom the potential exists to discover numerous drugs that reinforce each other's effects, because each affects a unique link in the causal chain. Several basic studies indicate that marijuana acts differently from conventional treatments for a variety of conditions, so it may prove to be a valuable source of auxiliary medicines.
The following sections summarize the findings of several recent studies on the biological effects of marijuana and its chemical components. Readers can find more detailed information (including references) on studies described in these sections in Chapter 2 of the 1999 IOM report, Marijuana and Medicine: Assessing the Science Base.
CANNABINOID CHEMISTRY
The active chemicals in marijuana, known as cannabinoids, are produced by resin glands on the female plant's leaves, stems, and calyxes, leaflike structures that sheath its small flowers (see Figure 2.5). Marijuana plants are either male or female; the female plant is the source of the drug. Although marijuana flowers themselves do not produce resin, they become a concentrated source of cannabinoids because resin tends to collect in the flower tops. Individual marijuana plants may contain widely differing
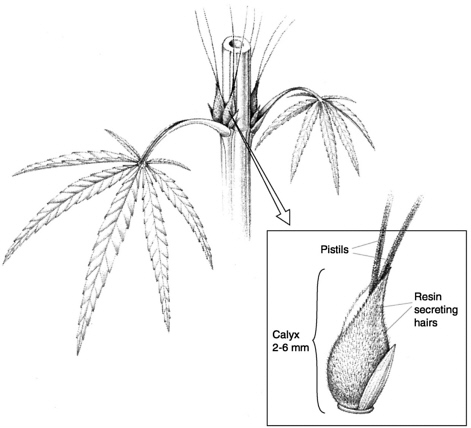
FIGURE 2.5 Female marijuana flowers grow in pairs, close to the main stem at the base of each leaf stem. Each small, petal-less flower is sheathed by a leaf-like structure, the calyx, which is covered with tiny, resin-secreting hairs. The resin contains high concentrations of cannabinoids such as THC, the primary active ingredient in marijuana. (Drawing by Roberto Osti from illustrations in Marijuana Botany: An Advanced Study: The Propagation and Breeding of Distinctive Cannabis. Robert Connell Clarke. Berkeley, CA: Ronin Publishing. 1981.)
amounts of specific cannabinoids due to variations in soil, temperature, humidity, and other growth conditions. And because cannabinoids degrade when exposed to high temperatures, moisture, and sunlight, storage conditions strongly affect the cannabinoid content of dried leaves or flower tops.
More than 60 different but closely related cannabinoids have been isolated from marijuana. They are greasy compounds, barely soluble in water, that dissolve readily in oily fluids. The chemical
structure of most cannabinoids is similar to THC, the main psychoactive ingredient in marijuana. Although researchers have identified several variants of THC, only the most abundant form, delta-9-THC, has been studied extensively (unless stated otherwise, we use the term THC to refer to this compound). The active ingredient in the prescription medicine Marinol is synthetic THC, which is also known by its generic name, dronabinol. Marinol is used to treat chemotherapy-induced nausea and vomiting as well as AIDS wasting syndrome.
Marijuana plants make THC through a multistep process, much as chemists do when they synthesize THC in the laboratory. A series of assembly steps combine several simple molecules to form a cannabinoid compound called cannabigerol. Cannabigerol may be subsequently converted to THC or to another cannabinoid called cannabidiol, which may then be modified to produce THC. It in turn may undergo chemical reactions that convert it to yet another cannabinoid, cannabinol. Unlike THC, neither cannabigerol, cannabidiol, nor cannabinol is psychoactive. Live marijuana plants and dried plant parts contain all of these cannabinoids as well as others that represent either precursors of THC or modified versions of the THC molecule.
CANNABINOIDS AND THE CELL
Although it has long been observed that marijuana alters thinking and behavior, scientists have only recently begun to learn how chemicals in marijuana act on individual cells, both in the brain and elsewhere in the body. That knowledge is crucial to determining exactly how marijuana and its constituent chemicals affect users.
Recent studies indicate that cannabinoids produce most of their effects by binding to proteins, called receptors, on the surfaces of certain types of cells. Many different types of receptor proteins stud the exterior membranes of the cells throughout the human body. Each receptor recognizes only a few specific molecules, known collectively as ligands. When the appropriate ligand binds to its receptor, it typically sets off a chain of biochemical reactions inside the cell. Many drugs, as well as hor-
mones and neurotransmitters, exert their effects by acting as ligands at different receptors.
The cellular receptors that bind THC and its chemical relatives are known as cannabinoid receptors. All vertebrate animals have similar types of cannabinoid receptors on their cells. So do some invertebrates, such as mollusks and leeches—an indication that the receptors fulfill similar functions in a broad range of animal species. Moreover, it suggests that cannabinoid receptors have existed at least since vertebrates first evolved, more than 500 million years ago.
To date, scientists have identified two main types of cannabinoid receptors, known as CB1 and CB2. CB1 receptors are extraordinarily abundant in the brain; for example, the brain has 10 times as many cannabinoid receptors as “morphine ” receptors, which are responsible for the effects of heroin and other opiates (as well as the body's own endorphins). CB2 receptors, on the other hand, are relatively scarce in the brain but plentiful in the immune system.
Cells bearing cannabinoid receptors respond to ligand binding in a variety of ways. When THC binds CB1 receptors in some nerve cells, for example, it triggers a cascade of reactions that ultimately slow down nerve impulses. This might slow a person's reaction time enough to make driving hazardous, but the same process could also dull pain signals traveling along those nerves, thereby providing some pain relief. Likewise, when THC binds CB2 receptors on white blood cells, it may impede their natural response to infection—a bad thing if it lowers a person's resistance to disease but a good thing if it reduces painful inflammation.
Although CB1 and CB2 share some structural and functional similarities, the two receptor types are different enough that it may be possible to design ligands that, unlike THC, would act on only one of them. Medicines based on these ligands would be expected to have fewer side effects due to their greater precision. In recent years researchers have discovered several natural ligands that bind only to CB1 or CB2; they have also synthesized a few such selective ligands. Although currently used only as research tools, these compounds represent an encouraging start toward developing novel medicines based on cannabinoids.
When researchers identify a receptor in the human body that binds a particular drug, such as THC, they next try to find molecules that naturally interact with the receptor in order to learn more about how the receptor functions and what purposes it serves. Scientists have identified several chemicals produced in the body that act on the cannabinoid receptors, CB1 and CB2; however, the physiological functions of these ligands remain unknown. The best studied among these compounds, anandamide (from ananda, the Sanskrit word for “bliss”), appears to act throughout the body, especially on the central nervous system. Anandamide is present in high concentrations—along with abundant CB1 receptors—in areas of the brain that control learning, memory, movement, coordination, and responses to stress. Significant amounts of anandamide are also found in the spleen, which has numerous CB2 receptors, and the heart.
Compared with THC, anandamide binds cannabinoid receptors weakly. As a result, the reactions that anandamide provokes are probably milder than those triggered by THC. Moreover, enzymes in the body quickly break down anandamide, so its effects are also relatively short lived. Another factor that limits anandamide's activity is a phenomenon known as reuptake, the rapid reabsorption of certain types of neurotransmitters after their release from nerve cells (see Figure 2.6), which protects neighboring nerve cells from over-stimulation. In some cases, this “protection” system can be adjusted to provide a therapeutic benefit. For example, the antidepressant Prozac works by blocking the reuptake of the neurotransmitter serotonin. If researchers found an analogous compound that prevented anandamide reuptake, perhaps it could be used to relieve distressed patients by raising the level of natural cannabinoids in their brains. Such a drug could potentially deliver many of the benefits of THC but with fewer side effects.
In addition to anandamide, researchers have identified several chemicals produced by the human body that bind to cannabinoid receptors, and they are continually finding more. These compounds are thought to perform a broad range of functions in the brain. Over the next few years scientists are likely to learn much more about these naturally occurring endogenous cannabinoids.
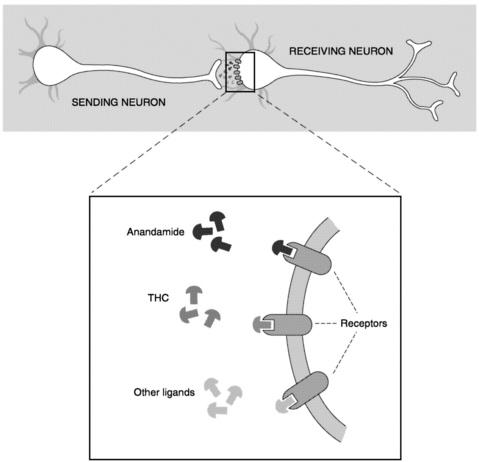
FIGURE 2.6 Signaling between nerve cells. Signal transmission between two neurons (nerve cells) begins as the sending neuron releases chemical messengers called neurotransmitters. Neurotransmitter molecules move across the gap to the receiving neuron, where they are bound by receptors on its surface. Binding may activate the receptor, triggering a chain of events that can alter thought and behavior.
The magnified view shows a variety of ligands binding to different types of receptors present on neurons. Anandamide, which is produced by the body, and THC, the main psychoactive ingredient in marijuana, can function as neurotransmitters. Both compounds bind and activate cannabinoid receptors on nerve cells, much as other neurotransmitters bind and activate their own specific receptors.
Researchers have also noted that cannabinoids can affect the body without binding to receptors. Both THC and cannabidiol have been shown to reduce toxic forms of oxygen that build up in tissues under stress, as do the antioxidant vitamins A and C. Also, because cannabinoids dissolve easily in the fatty membranes enclosing every cell, they may alter membrane function and, along with it, the activity of enzymes and proteins embedded in cell membranes. These properties, too, may prove medically useful.
CANNABINOIDS AND THE NERVOUS SYSTEM
Because cannabinoids and their receptors are naturally present throughout the human body, scientists suspect that the compounds serve a wide variety of physiological functions. That is especially true in the brain and spinal cord, which contain numerous CB1 receptors. When cannabinoids bind to these receptors, they typically set off a chain reaction that slows the transmission of nerve impulses between cells. That is not always the case, however; in other nerve cells, CB1 receptors are arranged in such a way that they speed the delivery of messages along neural pathways.
The largest populations of CB1 receptors are found in parts of the brain that control movement, memory, response to stress, and complex thought—functions that are, not coincidentally, affected by marijuana. Basic research indicates that the body's own cannabinoids play a natural role in all of these processes, as well as in pain perception and the control of nausea and vomiting (see Figure 2.7). Here we will review basic biological evidence that demonstrates how cannabinoids affect movement, memory, pain, nausea, and vomiting. In later chapters we will discuss how these effects have been studied on human patients in clinical settings as they pertain to specific symptoms.
Under the influence of marijuana, many people's bodies sway, and they often have difficulty holding their hands steady. In laboratory experiments, low doses of cannabinoids have been found to stimulate rodents to move around, while larger amounts appeared to inhibit their activity. CB1 receptors are particularly concentrated in the brain regions that coordinate movement, and it is probably these receptors that account for the different effects of
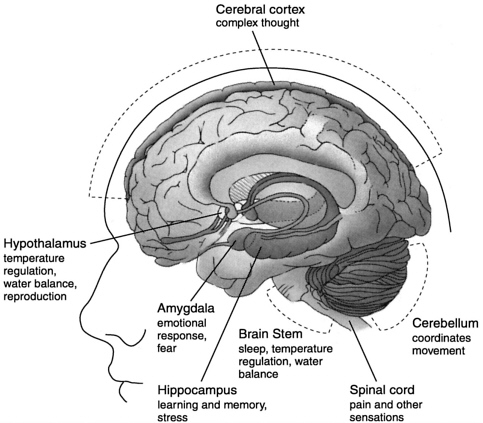
FIGURE 2.7 Locations and functions of brain regions with abundant cannabinoid receptors. Several regions of the brain, which govern a wide range of body functions, contain high concentrations of cannabinoid receptors. Abundant cannabinoid receptors are also present in the following areas not shown in this view of the brain: the basal ganglia, which controls movement; the nucleus of the solitary tract, which governs visceral sensation, nausea, and vomiting; the nucleus acumbens, the brain's reward center; and the central gray area, which registers pain relief.
cannabinoids on movement and activity. The brain regions that coordinate movement include several different sites, among them areas affected by Parkinson's and Huntington's diseases. Because cannabinoids appear to influence movement through a variety of routes, they represent a possible source of new medicines to treat movement disorders.
Marijuana has also been shown to disrupt short-term memory in humans. Memory loss probably occurs when cannabinoids
flood the abundant CB1 receptors in the hippocampus, one of the brain's memory centers. In studies of animals and also in experiments on isolated nerve cells, cannabinoids have been found to decrease nerve cell activity and block processes associated with memory formation in the hippocampus. Cannabinoids also appeared to produce temporary effects that resemble injury to that part of the brain. These findings suggest that medicines based on cannabinoids might have undesirable effects on short-term memory due to their action on the hippocampus.
CB1 receptors are moderately abundant in areas of the brain and spinal cord that control pain perception. Animals given cannabinoids in experiments designed to measure their responses to moderate and escapable pain reacted similarly to those given pain-killing opiate drugs, such as morphine. Cannabinoids and opiates have also been shown to provoke comparable chemical responses in nerve cells isolated from the spinal cord; however, the two types of drugs activate different receptors to produce these similar effects. Perhaps because they act at a separate site, cannabinoids—unlike opiates—also appear to block chronic pain sensations in experimental animals. This is an important finding since some types of chronic pain cannot be relieved even by powerful opiate medications.
Cannabinoids also appear to play a role in pain transmission along peripheral nerves, which detect sensations in all parts of the body and relay messages to the brain via the spinal cord. Peripheral nerve cells display both CB1 and CB2 receptors on their surfaces, and research in experimental animals indicates that cannabinoids specific to each receptor type appear capable of blocking peripheral nerve pain. These results suggest that a mixture of cannabinoids could enhance each other's effects in relieving peripheral pain in humans. On the other hand, it might be better to design pain relievers that do not bind CB1 since, as noted above, that receptor type mediates short-term memory loss.
Nausea and vomiting occur under a variety of circumstances, including viral and bacterial infections, emotional distress, and reactions to medications or poisons. Many people claim to have found relief from these symptoms by smoking or ingesting marijuana. Clinical studies indicate that both THC and smoked marijuana can reduce vomiting to some extent, and researchers have
found cannabinoid receptors in relative abundance in the part of the brain that controls visceral sensations, including nausea and vomiting. Little is known about how cannabinoids interfere with nausea or vomiting, but their effects clearly differ from those of existing antinausea drugs. Although generally quite effective, conventional medications might theoretically be improved by combining them with cannabinoids. Clinical research will be needed to determine how the different medications would actually interact in patients, however.
CANNABINOIDS AND THE IMMUNE SYSTEM
Through the complex interactions of an elaborate network of organs and cells, the immune system protects the body from bacterial and viral invaders. Because there are so many CB2 receptors on the different cells that participate in this defense network, cannabinoids are thought to play a role in the immune response (relatively small numbers of CB1 receptors are also found on immune cells). What role CB2 might play in immunity, however, remains a mystery—especially since researchers have yet to identify a natural cannabinoid that acts on immune cells much as anandamide acts on nerve cells.
In experiments on animals and isolated cells, cannabinoids have been shown to affect components of the immune system in diverse—and sometimes contradictory—ways. Cannabinoids increase, as well as decrease, certain responses to infection, though it can take up to 10 times more drug to produce these effects than it does to alter nervous system functions. Because most relevant experiments to date have measured the immediate effects of high doses of cannabinoids, the consequences to the immune system of chronic low-level cannabinoid exposure, such as might be found among moderate marijuana users, are unknown.
Nevertheless, basic research on cannabinoids and the immune system has produced several intriguing findings that warrant further study. Many of these reports focus on the effects of THC on one of several species of white blood cells, the workhorses of the immune system. Each type of white blood cell serves a different purpose, and all function in concert to defend the body against disease. Some engulf and destroy foreign substances, some pro-
duce antibodies that disable bacteria and viruses, and others issue chemical signals that rally other immune cells to attack and kill invaders.
Several basic studies have provided evidence that cannabinoids can suppress the immune system in a variety of ways, while others have found that cannabinoids can enhance immune responses.15 Certain natural and synthetic cannabinoids (but not anandamide) have been shown to decrease the ability of some types of white blood cells to multiply in response to infection. Some cannabinoids also appear to depress antibody production under some circumstances and to impede the ability of so-called killer cells to assassinate viruses and bacteria.
In addition to immune suppression caused by cannabinoids, marijuana use poses the additional—and probably greater—risk of immune damage due to smoking. Thus, it is important that future studies on the health risks of medical marijuana use distinguish between adverse effects caused by cannabinoids versus those caused by smoking or other delivery methods.
Chapter 3 discusses these and other potentially harmful effects of marijuana on the immune system. But in some cases the immune system must be suppressed in order to cure disease. Allergies, transplant rejection, and inflammatory disorders all result from immune reactions and thus represent potential targets for cannabinoid therapy. In some experiments, certain cannabinoid drugs have been shown to depress the production of cytokines, hormonelike chemicals that direct immune cells to eliminate foreign substances from the body.
Cannabinoids have also been shown to reduce inflammation and tissue damage in rat brain models of head injury, meningitis, and multiple sclerosis. Relatively little basic research has been conducted in this area, but since many pain medications act by reducing inflammation, this effect could be linked to the apparent ability of cannabinoids to relieve pain.
FOLLOWING LEADS FROM BASIC RESEARCH
In recent years researchers have taken important steps toward understanding how chemicals in marijuana affect the cells and tissues of the human body. Many more questions remain to be
answered, but the foundation has been laid for even greater advances in the immediate future. In addition to continued basic studies, clinical research on treating pain and movement disorders with cannabinoids appears promising.
The discovery of cannabinoid receptors, and at least some of the compounds that activate these receptors, opens the door to determining what naturally occurring cannabinoids do and how they work. The next logical steps are to pinpoint the location of natural cannabinoids in the brain and to find out how cells produce, store, release, and take them up. This knowledge can lay the groundwork for discovering different cannabinoid drugs with different effects. By following a similar path, medical researchers have learned to harness the benefits and minimize the risks associated with opiate drugs.
Basic studies have also identified several potential health risks associated with marijuana and cannabinoids, which are discussed in the next chapter. These findings, too, should be pursued through ongoing research.
NOTES
1. Abel EL. 1980. Marihuana: The First Twelve Thousand Years. New York: Plenum; Aldrich MR. 1997. “History of therapeutic cannabis,” in Cannabis in Medical Practice, Mathre ML, ed. Jefferson, NC: McFarland; Grinspoon L and Bakalar JB. 1997. Marihuana: The Forbidden Medicine. New Haven, CT: Yale University Press.
2. Aldrich MR. 1997.
3. Ibid.; Brunner TF. 1973. “Marijuana in ancient Greece and Rome? The literary evidence.” Bulletin of the History of Medicine 47:344-355.
4. Rosenthal F. 1971. The Herb: Hashish Versus Medieval Muslim Society. Leiden, The Netherlands: Brill.
5. Conrad C. 1993. Hemp: Lifeline to the Future. Los Angeles: Creative Xpressions; DuToit BM. 1980. Cannabis in Africa. Rotterdam, The Netherlands: Balkema.
6. Aldrich MR. 1997.
7. Abel EL. 1980.
8. Mikuriya TH. 1973. Marijuana: Medical Papers 1839-1972. Oakland, CA: Medi-Comp Press.
9. Aldrich MR. 1997; Bonnie RJ and Whitebread CH II. 1974. The Marihuana Conviction: A History of Marihuana Prohibition in the United States. Charlottesville: University Press of Virginia.
10. Aldrich MR. 1997.
11. Rosenthal F. 1971.
12. Facklam M and Facklam H. 1992. Healing Drugs. New York: Facts on File.
13. Grinspoon L and Bakalar JB. 1997.
14. Taylor HC. 1998. “Analysis of the medical use of marijuana and its social implications. ” Journal of the American Pharmaceutical Association 38(2):220-227.
15. Institute of Medicine. 1999. Marijuana and Medicine: Assessing the Science Base. Washington, DC: National Academy Press, p. 60.

























