
3
HOW HARMFUL IS MARIJUANA?

The most heated arguments over medical marijuana do not concern its ability to alleviate patients' symptoms but rather its potential danger to individual users and to society. This chapter first examines the scientific evidence that marijuana causes physical and psychological injury to individual users. Then it considers the potential social harms that could result from legalizing marijuana for medical uses. More detailed information and complete references for studies described below can be found in Chapter 3 of the 1999 IOM report, Marijuana and Medicine: Assessing the Science Base.
WHERE THERE'S SMOKE, THERE'S HARM
Given the well-known consequences of tobacco smoking, it seems logical to suspect that marijuana could be equally detrimental to physical health. Although free of nicotine, marijuana smoke certainly pollutes the lungs. And since tobacco smoking has been linked to respiratory injury, cancer, emphysema, heart disease, complications of pregnancy, low birth weight, and other ills, it makes sense to worry whether smoking marijuana might prove equally harmful.
Scientists have compared marijuana and tobacco smoking on the basis of many different factors but have failed to find consis-
tent evidence that either substance poses a greater health risk than the other. On the one hand, marijuana joints have been shown to deliver at least four times as much tar to the lungs as tobacco cigarettes of equivalent weight. This difference is due to the lack of filters on joints and because marijuana smokers typically inhale a larger volume of smoke and take it more deeply into the lungs than tobacco smokers do. Marijuana smokers also tend to hold smoke in for a time before exhaling, exposing the lungs to even greater levels of cancer-causing agents.
On the other hand, because they are packed more tightly, commercial cigarettes produce more smoke than hand-rolled joints. That, plus the fact that most tobacco users typically smoke more cigarettes per day than their marijuana-using counterparts, means that over the course of a day most tobacco users take far more smoke into their lungs than people who smoke marijuana exclusively. Thus it is impossible to make precise comparisons between the damage to one's health caused by smoking marijuana versus the damage caused by smoking tobacco. And since an estimated 70 percent of marijuana users also smoke tobacco, it is difficult to conduct epidemiological studies that isolate the effects of marijuana smoking.
Not surprisingly, clinical studies suggest that people who smoke marijuana are more likely to develop respiratory illnesses than are nonsmokers. A survey of outpatient medical visits at a large health maintenance organization (HMO) found that marijuana users were more likely to seek help for respiratory illnesses than people who smoked neither marijuana or tobacco.1 However, the researchers also found that patients who had smoked marijuana for more than 10 years did not seek treatment for respiratory illness with any greater frequency than those who had smoked it for less than 10 years. One possible explanation for this finding is that the people who continued smoking for a long time had not been troubled by respiratory problems such as shortness of breath, while those who did develop uncomfortable symptoms quit smoking relatively quickly. Unfortunately, the marijuana smokers who responded to this survey were not asked if they also used cocaine, which is known to intensify respiratory symptoms. It is also likely that some participants underreported their use of tobacco, alcohol, and marijuana.
A study of 446 volunteers compared the incidence of chronic bronchitis symptoms (excessive cough, sputum production, and wheezing) among habitual marijuana smokers, tobacco smokers, and nonsmokers.2 Roughly one in three of both the marijuana and the tobacco smokers showed one or more of these symptoms, while only about one in 12 of the nonsmokers did. Smokers—even those who did not smoke tobacco —had episodes of acute bronchitis more than five times as often as nonsmokers. Marijuana smokers also performed worse on lung function tests than did nonsmokers.
The average marijuana smoker in this study consumed three to four joints per day; the tobacco users smoked an average of 20 cigarettes per day. In this study of habitual marijuana smokers, participants who smoked both marijuana and tobacco reported no more symptoms of chronic bronchitis overall than those who smoked tobacco alone, an indication that smoking marijuana does not increase the harms caused by smoking tobacco.
Another study did show evidence of such an interaction, but it was conducted on people who smoked considerably less marijuana and tobacco than those who participated in the previously described study. Researchers have found that, in general, the interactive effects of toxic substances tend to be easiest to detect at low exposure levels. This may explain why the lighter smokers in the second study showed signs of increased respiratory damage when they used both marijuana and tobacco, while the heavier smokers in the first study did not. In any case, both studies indicate that marijuana smoke reduces respiratory function.
Habitual smoking of either marijuana or tobacco damages the lining of the bronchial airways. After continuous exposure to smoke, the delicate tissues along these passageways become red and swollen. Smoking also transforms the cells of the bronchial airways. These passages are normally lined with ciliated cells, whose hairlike projections move rapidly to sweep mucus toward the mouth. But when people smoke, these cells are replaced by others that secrete copious amounts of thick mucus, which can only be expelled by the notorious “smoker's cough. ”
Bronchial injury, a more sensitive measure of damage than the symptoms of chronic bronchitis, is even greater among people who smoke both marijuana and tobacco. The damage extends to
the interiors of bronchial cells, which develop a variety of abnormalities. Some of these changes, which are known to be precursors of cancer, have also been discovered in the respiratory tracts of marijuana and hashish smokers who did not use tobacco.
Another form of respiratory injury caused by tobacco smoke is a condition known as chronic obstructive pulmonary disease (COPD), a slow, progressive loss of elasticity in the passages that deliver air to the lungs. People with COPD become short of breath and exhibit symptoms of chronic bronchitis. Attempts to determine whether marijuana smoke also provokes COPD have produced conflicting results. For example, one group reported that smoking as little as a single joint per day significantly impaired small airway function,3 while another failed to detect similar damage even in people who smoked four joints a day for more than 10 years.4 It thus remains to be determined whether chronic marijuana smoking actually causes COPD, but there is good reason to suspect that it does.
While many tobacco smokers accept coughing and shortness of breath as part of the price they pay for the pleasure of smoking, fear of cancer sometimes persuades them to quit. (And then there are people who get little pleasure out of smoking but continue smoking to calm their nerves, that is, to avoid feeling anxious and irritable—the withdrawal symptoms of nicotine addiction.) Whether marijuana users should be similarly concerned remains to be conclusively proven. However, cellular, genetic, and clinical studies all suggest that marijuana smoke is an important risk factor in the development of respiratory cancer.
Many of the same carcinogenic, or cancer-causing, compounds present in tobacco smoke are also found in burning marijuana. In particular, unfiltered smoke from joints contains higher concentrations of a class of chemicals called polycyclic aromatic hydrocarbons (PAHs) than does smoke from tobacco cigarettes. Since marijuana users generally inhale more deeply than tobacco smokers, they may be exposing their lungs to even higher levels of these dangerous substances. Preliminary research also suggests that marijuana smokers' lung cells contain higher levels of an enzyme that converts PAHs into a cancer-causing form. Thus, it is not surprising that several studies implicate marijuana smoking
as a risk factor for lung cancer as well as for mouth and throat cancer.
Several reports have suggested that marijuana smokers are at greater risk than nonsmokers of developing cancers in tissues that come into contact with smoke, such as the lungs, mouth, larynx, pharynx, and esophagus. However, these conclusions were based on series of case reports of patients with these cancers rather than from controlled studies. Thus, the increased frequency of cancers among marijuana smokers cannot be attributed to marijuana alone but may also result from other factors, such as tobacco smoking.
To date, only one large-scale study5 has sought to determine the frequency with which marijuana smokers develop cancer. It included some 65,000 men and women HMO clients between the ages of 15 and 49. Among these people, 1,421 cases of cancer were found, but marijuana use—defined as taking the drug on six or more occasions—appeared to increase only the risk of prostate cancer in men who did not smoke tobacco. No association was found between marijuana use and any other type of cancer, including cancers normally linked to tobacco smoking. However, this study was limited by the fact that many of its participants were younger than the average ages when many cancers appear as well as by the short duration of their marijuana use. Lung cancer, for example, usually develops only after a long exposure to smoking; relatively few marijuana users persist in the habit for more than a few years, and most also smoke tobacco.
Researchers should soon be better able to pursue the question of marijuana's carcinogenicity. More than 30 years have elapsed since the start of widespread marijuana use among young people in the United States, who now constitute a sufficiently large population to support meaningful epidemiological studies. On the other hand, such surveys are difficult to conduct, since far fewer people have smoked marijuana exclusively than have smoked tobacco alone and also because marijuana smokers are likely to underreport their use of the illegal drug.
In contrast to human studies, research on the effects of marijuana smoke at the cellular level provides strong evidence that it contains abundant carcinogens. Exposure to marijuana smoke has been shown to cause chromosomal changes that precede cancer—
and in some cases outright malignancies—in isolated human and animal lung cells. Similar alterations have been detected in the actual lung cells of marijuana smokers and at even higher levels among those who also smoked tobacco.
An especially convincing study evaluated changes in blood cells taken from pregnant women who were exclusive smokers of marijuana and also from their babies after they were born.6 In a class of white blood cells called lymphocytes, the researchers found significantly more DNA aberrations of a type linked to cancer development as compared with lymphocytes from nonsmoking women and their newborns. In previous studies the same group of investigators had found similar changes in the DNA of tobacco smokers, indicating that the substances responsible for this damage are present in both marijuana smoke and tobacco smoke.
Marijuana smoking has also been associated with increased mortality among men with AIDS. This finding is especially important since such patients comprise the largest group of medical marijuana users in the United States. Several factors may contribute to this trend, which is still largely unexplained. It may be that people who use marijuana also tend to engage in risky sexual behavior or intravenous drug use, either of which puts them at higher risk for developing AIDS, but it is also likely that smoking marijuana adds to the burden that HIV places on the immune system. HIV-seropositive individuals who use marijuana regularly appear to be at increased risk of opportunistic infections and Kaposi's sarcoma; for those who smoke more than one-half pack of cigarettes per day, the risk is somewhat lower. If smoking marijuana indeed makes AIDS patients sicker, it remains to be determined whether smoke, cannabinoids, or both are to blame (see Chapter 5).
THE ROLE OF CANNABINOIDS
The vast majority of studies on the physiological consequences of marijuana use have focused on smoking. However, a few researchers have directly evaluated the effects of cannabinoids on isolated cells, experimental animals, and human subjects. Most such studies have examined one of three areas of po-
tential damage: the immune system, the cardiovascular system, and reproductive and fetal health.
As discussed in the last chapter, several biological studies suggest that cannabinoids can depress the immune system's response to infection. In some experiments, white blood cells in experimental animals exposed to THC and other cannabinoids exhibited a reduced capacity to proliferate following infection; some animals also produced fewer than normal antibodies or showed signs of impaired “killer cell” activity.7
Not all studies of this nature implicate cannabinoids as immune suppressants. In fact, some immune functions have been found to increase in response to cannabinoids. Such results are not necessarily contradictory because many physiological processes contribute to immunity. Thus, no single experiment can truly reveal the “big picture” of marijuana's effects on the human immune system. That is particularly true of studies that test the effects of pure cannabinoids such as THC, since marijuana contains a variety of chemicals that may affect immune activity.
Although it demands equally cautious interpretation as studies on individual immune cells, research on disease resistance in animals exposed to cannabinoids more closely tracks the overall impact of cannabinoids on the immune system. Mice infected with pneumonia-causing bacteria died of septic shock when they were injected with THC before and after infection; those that did not receive THC developed immunity to the bacterium and survived. This response was found to vary depending on the amount of THC the mice received and whether it was injected before or after they were infected with the bacteria. Similarly, two doses of THC given before and after infection with the herpes simplex virus appeared to hasten the death of immunodeficient mice, although a single dose of THC prior to infection did not. Both experiments suggest that the timing of THC exposure relative to infection determines whether THC suppresses the immune response.8
Even if cannabinoids themselves cause little or no harm to the immune system, there is good reason to believe that smoking marijuana does. Marijuana smoke been linked to increased mortality in people with AIDS and it also appears to injure an important class of immune cells in the lungs. These cells, called alveolar
macrophages, are primarily responsible for protecting the lungs against infectious microbes, harmful substances, and tumor cells. Compared with nonsmokers, habitual marijuana smokers in a large study were found to have twice as many alveolar macrophages, a sign that their lungs were fighting infection or invasion. People who smoked both marijuana and tobacco had four times as many of the cells as nonsmokers.9
Marijuana smoking was also found to reduce the ability of alveolar macrophages to destroy disease-causing fungus and bacteria as well as tumor cells. Moreover, marijuana smoking appears to depress macrophages ' ability to produce cytokines—hormonelike chemicals that help coordinate the immune response.10 Taken as a whole, these findings indicate that smoking marijuana could have dangerous consequences for patients with compromised immune systems, including people with AIDS and cancer—particularly those who are receiving immunosuppressive chemotherapy—as well as organ transplant recipients.
Exposure to cannabinoids can also affect the cardiovascular system. 11 Although these effects tend to be shortlived, they are far easier to measure than the impact of cannabinoids on the immune system. Both smoked marijuana and THC have been shown to raise heart rate, from 20 to 100 percent above normal in some cases. Oral THC (as well as smoked marijuana) can also exaggerate the drop in blood pressure that occurs when a person rises to standing after lying down, sometimes so much so that the person faints. This reaction rarely occurs after two to three days of repeated exposure to THC or marijuana extract, and it poses little risk for young healthy people. It could, however, present a serious problem for older patients or for people at risk for heart attack or stroke. As chronic marijuana users who began taking the drug during the 1960s approach the age at which cardiovascular disease becomes common, the impact of marijuana use on circulatory health should become clearer. In the meantime, people at risk for cardiovascular disease would be wise to avoid marijuana and THC.
In addition to effects on the immune and cardiovascular systems, researchers have considered the impact of cannabinoids on reproduction. 12 A series of reports involving experimental animals injected with THC indicate that it inhibits several different repro-
ductive functions, from hormone secretion to normal sperm development to embryo implantation. It is important to recognize, however, that most of these studies involved single injections or short-term treatments with the drug, which produced effects that were observed to last for only hours to days. Thus, their results reveal little about the consequences of chronic long-term marijuana or cannabinoid use.
Nevertheless, the few studies that have been conducted to assess THC's effects on human reproduction have produced results that are consistent with those of the animal studies. Fertility research on marijuana users has yielded conflicting results, revealing at worst a short-term depression of reproductive hormones following marijuana use. Over time long-term marijuana users appear to become less sensitive to the inhibitory effects of THC on at least one reproductive factor —luteinizing hormone, which regulates the secretion of testosterone and estrogen. In women the strength of that effect varies with the timing of the menstrual cycle and is most significant between ovulation and the onset of menstruation.
Absent any direct measure of the effects of either marijuana or THC on reproductive function, it seems likely that both substances decrease short-term fertility in men and women. Due to the timing of luteinizing hormone suppression in women, it is also reasonable to predict that THC could interfere with the earliest stages of pregnancy, particularly with embryo implantation. Marijuana smoke appears to pose an even greater threat to pregnant women and couples who are trying to conceive, since it is probably at least as harmful to fetal development as tobacco smoke.
Several epidemiological studies have attempted to trace the effects of marijuana use on pregnancy and fetal development, but their results have been inconsistent. Essentially, the same problems, such as low birth weight, that plague tobacco-smoking mothers and their infants seem to appear among marijuana users. Interestingly, in a study of Jamaican women—who rarely smoke marijuana but prepare it as a tea to relieve morning sickness—no neurobiological or behavioral differences were detected between newborn babies of those who used marijuana and those who did not.13
The Ottawa Prenatal Prospective Study has monitored the effects of prenatal marijuana exposure on the cognitive function of children since 1978.14 So far the study has failed to find evidence that children whose mothers smoked marijuana during pregnancy perform below average on a variety of intelligence tests. Some early cognitive problems were detected among children of women who smoked at least one joint per day during pregnancy, but these deficits were no longer apparent after the children reached age 5. Older children of marijuana users did, however, score slightly lower than those of both nonsmokers and tobacco smokers on tasks that measured their ability to plan ahead and control self-defeating behavior. On the other hand, children whose mothers smoked tobacco during pregnancy scored somewhat lower on tests of language and cognitive skills than the other two groups and continued to do so as late as age 12. In most cases the differences in test scores between groups of comparable children varied by less than 5 percent; thus, the effects, while statistically significant, are subtle.
In summary, there are many reasons to worry that for people who might choose to use marijuana as medicine—and especially those who smoke it—the drug could actually add to their health problems. Proof that habitual marijuana smoking does or does not lead to respiratory cancer awaits the results of extensive, carefully designed epidemiological studies. In the meantime it appears that, for people with chronic medical disorders or those with compromised respiratory or immune systems, smoking marijuana is likely to do more harm than good. Likewise, for people at risk of cardiovascular disease, pregnant women, and couples trying to conceive, the potential risks of either THC or smoked marijuana appear to exceed the potential medical benefits.
MARIJUANA ABUSE
The most talked about health risk associated with marijuana is its potential to promote abuse and addiction. There is great disagreement on this topic and scant evidence that applies specifically to marijuana used solely to relieve medical symptoms. Nevertheless, research from a variety of perspectives—including
biological, clinical, and population studies—paints a reasonably detailed picture of the consequences of chronic marijuana use.
Because it is illegal, some people equate any use of marijuana with abuse. The IOM team chose instead to apply the definition of substance abuse used by the medical profession: that people who abuse marijuana use it repeatedly and to their personal detriment. This is the essence of substance abuse as described by the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV),15 the most widely used diagnostic system for mental health care. When people use marijuana compulsively and have trouble stopping despite the fact that their behavior causes severe problems, their diagnosis is more serious than abuse. The DSM-IV classifies such behavior as substance dependence (see Box 3.1).
THE PHYSIOLOGY OF USE AND ABUSE
Even marijuana users who do not fit the DSM-IV criteria for abuse or substance dependence may experience symptoms of tolerance, physical dependence, and withdrawal. Tolerance, a common response to the repeated use of any drug, occurs when increasing amounts are required to produce a given effect. Physical dependence describes the body's adaptation to frequently used drugs. While physical dependence can lead to substance abuse, it does not necessarily do so. If someone who is physically dependent on a drug stops taking it, he or she is likely to experience withdrawal symptoms. Most drugs that are abused produce tolerance, physical dependence, and withdrawal—but so do caffeine and nicotine as well as many nonaddictive drugs for pain, anxiety, and high blood pressure. For example, if people who take the medication propranolol for hypertension abruptly stop taking the drug, they are likely to experience withdrawal symptoms that include a temporary rise in blood pressure. To avoid these problems, patients must gradually decrease their dose of propranolol before switching to a different hypertension drug.
Regular marijuana users quickly develop tolerance to most of the drug's effects. This may be why heavy users appear to be less impaired than light users after smoking similar amounts of marijuana, despite the finding that heavy users tend to accumulate higher levels of THC in their blood. If users go without marijuana
|
Box 3.1 DSM-IV Criteria for Substance Dependence The fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) defines substance dependence as a group of cognitive, behavioral, and physiological symptoms. A person diagnosed with substance dependence meets at least 3 of the following criteria within a twelve-month period:
Substance abuse with physiological dependence is diagnosed if there is evidence of tolerance or withdrawal. Substance abuse without physiological dependence is diagnosed if there is no evidence of tolerance or withdrawal. |
for a week or so, however, they appear to lose their tolerance to its effects. Interestingly, tolerance to different effects of the same drug can develop at varying rates. Heroin users, for example, become tolerant to the drug's euphoric effects more quickly than they do to its ability to interfere with breathing. Thus, because they tend to increase the amount of drug they take in order to attain the same high, heroin users risk death by asphyxiation.
To our knowledge no marijuana user has ever died of such an overdose. Nevertheless, there are likely to be patients for whom the development of tolerance to cannabinoids would outweigh the benefits of marijuana-based medicines. On the other hand, developing tolerance to certain effects of cannabinoids, such as short-term memory loss or inability to concentrate, could be seen as a benefit. Tolerance to the various cannabinoids may develop at different rates, so it will be important to evaluate their individual effects on mood, movement, memory, and attention if they are to be used as medicines.
People who use marijuana or who take oral THC (e.g., Marinol) appear to become tolerant to some of the drug's effects more quickly than to others. To document this phenomenon, researchers conducted a study of people who smoked marijuana on a daily basis. During the study period, one group of participants smoked marijuana cigarettes four times a day for four consecutive days, while the other group took THC pills on the same schedule. Both thought that the same amount of drug made them feel less and less “high” over the course of four days, but neither group thought that their drug-induced increases in appetite declined over that time. The marijuana-smoking group reported feeling “mellow” after smoking throughout the four days, while the THC-taking group never reported feeling “mellow.”16 The IOM team also heard from several people who had tried both smoked marijuana and oral THC to treat their medical symptoms and whose comparisons of the two drugs resembled those of the study participants.
In addition to human studies, scientists have conducted research on animals to study how tolerance to cannabinoids arises. Like the people in the clinical experiments described above, experimental animals that received THC on an ongoing basis ap-
peared to become tolerant to many of its initial effects, including memory disruption, decreased movement, and pain relief.17
Research also indicates that target cells for THC—those that bear CB1 and CB2 receptors—adapt to chronic THC exposure in ways that contribute to tolerance. Most studies of brain cells detected a decrease in the production of cannabinoid receptors under conditions that mimicked prolonged exposure to cannabinoids. Tolerance to cannabinoids appears to develop at different rates in different regions of the brain, however, which may explain why a few such studies have not found a decline in cannabinoid receptors. This phenomenon could also explain why tolerance to some effects of THC develops more quickly than to other effects. And in addition to their effects on CB1 and CB2 receptors, cannabinoids may have a desensitizing effect on other proteins in target cells.
Although intriguing, the results of these and other basic studies on the effects of cannabinoids should be interpreted with caution. Most basic studies consist of short-term experiments that merely simulate long-term marijuana use by exposing animals to higher amounts of cannabinoids than typically experienced by marijuana users. Moreover, cannabinoids behave differently in the human body depending on whether they are inhaled, injected, or swallowed. While most people ingest cannabinoids by smoking, they are generally injected into laboratory animals. Still, some of the same biochemical responses to chronic cannabinoid exposure that have been observed in experimental animals probably occur in humans as well, though perhaps in subtler forms.
Withdrawal from either marijuana or THC has been shown to cause several distinct symptoms, as reported by participants in clinical studies and adolescents undergoing treatment for substance abuse. These include restlessness, irritability, mild agitation, insomnia, sleep disturbance, nausea, and cramping—uncomfortable sensations, to be sure, but far milder than symptoms associated with alcohol withdrawal (see Table 3.1). Following very high doses of oral THC—the equivalent of smoking between five and 10 joints of average potency per day for 10 to 20 days—withdrawal symptoms also included runny nose, sweating, and decreased appetite, but lasted only four days. 18 In another study,
TABLE 3.1 Common Withdrawal Symptoms Produced by Various Drugs
|
Marijuana |
Nicotine |
Alcohol |
Cocaine |
Opiates (morphine and heroin) |
|
|
Irritability |
X |
X |
X |
X |
|
|
Low Mood, Depression |
X |
X |
X |
||
|
Anxiety |
X |
X |
|||
|
Sleep Disturbance |
X |
X |
X |
X |
X |
|
Nausea |
X |
X |
X |
||
|
Cramps |
X |
X |
|||
|
Increased or Decreased Heart Rate |
X |
X |
X |
||
|
Craving |
X |
X |
X |
X |
|
|
Source: O'Brien CP. 1996. Drug addiction and drug abuse. In: Harmon JG, LimbirdLE, Molinoff PB, Ruddon RW, Gilman AG, Editors Goodman and Gilman's The Pharmacological Basis of Therapeutics. 9th Edition. New York: McGraw-Hill. Pp. 557-577. |
|||||
participants took about half as much THC for only four days but reported that their withdrawal symptoms lasted longer.19
In animals, simply administering THC for several days or weeks and then discontinuing it does not provoke withdrawal symptoms because the drug lingers in the brain, allowing it to gradually adapt. A similar situation probably occurs in human marijuana users who go “cold turkey,” easing the process of withdrawal. However, by administering a chemical block that immediately interferes with THC's effects, researchers can create a sort of instantaneous withdrawal in experimental animals that have been chronically exposed to THC. These animals exhibit dramatic symptoms, including hyperactivity and disorganized behavior, which also occur during withdrawal from opiate drugs.
Tolerance and withdrawal certainly contribute to a drug's ca-
pacity for abuse. But ultimately the better a drug makes people feel, the more likely they are to abuse it. This effect, called reinforcement, generally depends on drug dosage. Caffeine, for example, is reinforcing for many people who drink a cup or two of coffee at a time but is aversive—that is, it makes most people feel worse, not better—if they consume the caffeine equivalent of six cups of coffee all at once. Reinforcement for a particular drug also varies from person to person. In the case of caffeine, research indicates that its effects are the most pleasurable for the least anxious people.
Marijuana is indisputably reinforcing to many people. Some have argued that marijuana has a relatively low potential for abuse, based on experiments in which animals—who willingly dose themselves with cocaine —did not self-administer THC. Other studies indicate that THC is rewarding to animals in relatively mild doses but that, like many reinforcing drugs, it is aversive in large amounts. Cannabinoids have also been shown to unleash a surge of dopamine, a chemical generally associated with reinforcement, in rats; however, the mechanism by which cannabinoids exert this effect appears to be different from that of other abused drugs such as cocaine and heroin. It is also important to note that the dopamine “reward” system in the brain responds to a wide variety of stimuli, not all of which are dangerous substances. For example, from animal studies we know that dopamine levels also rise in response to feelings of sexual attraction and when eating sweet foods. Based on similarities in brain structure and function, this is probably true of humans as well.
As people progress from tolerance to physical dependence to drug abuse, their craving intensifies despite mounting problems caused by their behavior. This intense desire for a drug is the toughest part of addiction to overcome. As a result, most recovering addicts suffer a relapse within one year of becoming drug-free. Animal studies suggest that this tendency to relapse results from long-term changes in brain function brought on by addiction. These alterations appear to persist for months or years after the last use of an addictive drug.
Anticraving medications have been developed for nicotine and alcohol, while methadone reduces cravings for heroin as it blocks the drug 's euphoric effects.
Research on cravings has focused on nicotine, alcohol, cocaine, and opiate drugs. It has not specifically addressed marijuana, so it remains unknown whether marijuana induces similar changes in brain function.
MARIJUANA USE AND DEPENDENCE
Another way to look at the risk of marijuana addiction is to examine general patterns of use and dependence. Who uses marijuana? How frequently and under what circumstances do marijuana users become abusers? How do patterns of marijuana abuse compare with those of other abused substances? Social scientists and epidemiologists have addressed several aspects of these questions in recent years.
Millions of Americans have tried marijuana, but most do not use it regularly. According to a U.S. Department of Health and Human Services household survey conducted in 1997, 33 percent of the U.S. population over the age of 12 (some 70 million people) has tried marijuana or hashish at least once. Only 5 percent of respondents reported that they currently use either substance. Marijuana use was most prevalent among people between 18 and 25 and declined sharply in people age 34 and older.
These results fit a long-observed scenario: many people try marijuana as adolescents, but few continue to use it past young adulthood (see Figure 3.1). Peer pressure, as well as the desire to conform or appear mature, typically prompts teenagers to try marijuana for the first time. Different factors, however, appear to influence marijuana use beyond mere experimentation.
In one study of 456 students who tried marijuana while in high school, those who became regular (but not heavy) marijuana users typically said they continued to take the drug to improve their mood, rather than for any social reason.20 This finding is in keeping with additional research on young adults, who tend to use drugs on a regular basis to satisfy psychological needs rather than to impress others.
Only 28 percent of the high school students continued using marijuana after their initial experimentation with the drug. Several who quit did so because they felt that marijuana had harmed either their health or their relationships with other people. Some
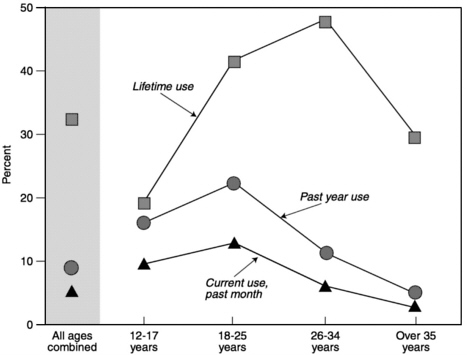
FIGURE 3.1 Age distribution of marijuana users among the general population in 1996. (Adapted from Marijuana and Medicine: Assessing the Science Base. Institute of Medicine. 1999. Washington, DC: National Academy Press.)
said they stopped when they found themselves in positions of responsibility or in less frequent contact with other marijuana users. They also cited parental disapproval more often than peer disapproval as a factor in their decision to give up marijuana.
But people who turn to marijuana to relieve medical symptoms—most of whom are older than 35—face an entirely different set of circumstances than do youthful recreational users. There are no existing scientific studies of the relationship between medical marijuana use and abuse. However, several individual and environmental factors appear to influence whether a particular person is likely to abuse or become addicted to a given drug. Each of these criteria bears consideration in calculating the risks posed by medical marijuana.
Some segments of the population appear to be more susceptible to drug dependence in general than others. For example, national survey results indicate that men are 1.6 times more likely to
become dependent on illicit drugs than are women. The risk of drug dependence for white Americans is approximately double that for African Americans. People between the ages of 25 and 44 are estimated to be more than three times as likely than those over 45 to abuse drugs.
Adolescents are particularly vulnerable to drug dependence since they tend to suffer the behavioral consequences of dependence at lower levels of drug use compared with adults. Young people who are already dependent on other substances—typically alcohol or tobacco —are especially prone to marijuana dependence. In a study of more than 200 patients in a residential treatment program for delinquent youth, participants were found to be dependent on an average of more than three different substances. Of those patients who had used marijuana more than six times, more than 80 percent went on to become dependent on it—a far higher rate of progression to dependence than found among the general population.21
Although parents of children who use marijuana often claim that the drug provokes rebellious behavior, the adolescents in the previous study had all displayed behavioral problems before they began abusing marijuana. Several other reports echo these observations and indicate that the more troubled a child is, the earlier he or she is likely to begin drug use, abuse, and dependence.
People with psychiatric disorders constitute another group at high risk for drug abuse. An estimated 76 percent of men and 65 percent of women classified as being drug dependent suffer from at least one additional psychiatric disorder; most frequently, that disorder is alcohol abuse. In drug-dependent women, phobias and major depression are nearly as common as alcohol abuse. Antisocial personality and its predecessor in children, conduct disorder, also figure prominently in the psychiatric diagnoses of substance abusers.
Genetic factors also appear to influence whether a person will abuse drugs, including marijuana. A study of over 8,000 male twins indicates that people inherit the tendency to enjoy marijuana's effects.22 Presumably, people who try marijuana and find it pleasant are more likely to continue using it—and thus possibly abuse it—than those who do not find it enjoyable. The results of this study and a similar survey of female twins23 indi-
cate that some people who experiment with marijuana may be genetically predisposed to becoming regular users. Whether a person ever tries marijuana, however, appears to be most strongly influenced by one 's family and social environment.
Although marijuana seems to pose an increased risk of abuse for some people, it is generally considered to be only mildly addictive. Compared with users of several other addicting substances, few people who use marijuana become dependent on it (see Figure 3.2). Thus, while many more people try—and use—marijuana than other illicit drugs such as cocaine or heroin, marijuana abuse cases are relatively rare. Two large-scale surveys—the National Comorbidity Survey24 and the Epidemiological Catchment Area Program25—have found that about 5 percent of the U.S. population has been dependent on marijuana at some
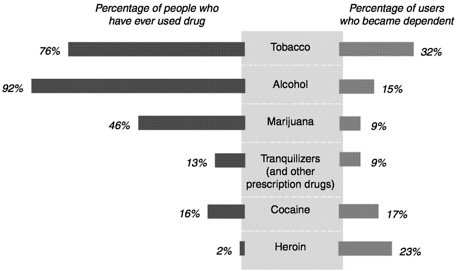
FIGURE 3.2 Prevalence of drug use and dependence in the general population. The higher estimates for marijuana use shown here compared to those reported by the Department of Health and Human Services household survey shown in Figure 3.1 are probably due to differences in how the surveys were conducted. (Adapted from J.C. Anthony, L.A. Warner, R.C. Kessler. 1994. Comparative epidemiology of dependence on tobacco, alcohol, controlled substances, and inhalants: Basic findings from the National Comorbidity Survey. Experimental and Clinical Psychopharmacology 2:244-268.)
point in their lives. By comparison, nearly 14 percent of adults met the criteria for dependence on alcohol and 36 percent met the criteria for tobacco dependence.
Clearly, marijuana use carries a risk of dependence and abuse—a danger that must be taken into account if either the crude plant extract or its active ingredients are to be used for medical purposes. For certain patients—particularly adolescents, people with psychological or social problems, and those with an inherited predisposition to substance abuse—marijuana-based medications may not be worth the risk. On the other hand, compared with alcohol, tobacco, and several prescription medications, marijuana's abuse potential appears relatively small and certainly within manageable limits for patients under the care of a physician.
PSYCHOLOGICAL HARMS
Compared with the physical dangers of marijuana use, its psychological drawbacks are far less well understood. Indeed, some of the psychoactive effects of marijuana—such as anxiety reduction, sedation, and euphoria —can be counted among the drug's potential benefits for certain patients. This paradox, plus the fact that the vast majority of research on the psychological effects of marijuana and cannabinoids concerns intoxication and recreational use, makes it difficult to anticipate the psychological impact of medical marijuana use.
One would expect that people who use marijuana solely as a medicine have very different mental experiences than those of recreational users simply because the circumstances under which people use psychoactive drugs strongly influence their psychological reactions. Most of the existing psychological research on marijuana was conducted on people who had previously used the drug, so very little is known about its potential to cause adverse psychological reactions in first-time or inexperienced users. Moreover, the majority of psychological studies have measured the effects of a single, often large, dose of the drug, rather than the chronic exposure that would be more typical of medical use. Instead, it is the subtler effects of low doses of marijuana and cannabinoids that must be taken into account if they are to be used as
the basis for medications. For even in amounts too small to cause users to feel “high,” marijuana and THC provoke changes in mood, thinking, and performance on tasks that demand a combination of attention and coordination.
Marijuana's popularity as a recreational drug hinges on its ability to induce a temporary sense of well-being or euphoria in most users. Many feel that being high enhances their physical and emotional sensitivity, causing them to become talkative and more engaged with other people. Because it suppresses short-term memory and learning, though, people under the influence of marijuana often have difficulty carrying on an intelligible conversation. Short-term memory loss also causes distortions in their sense of time.
Adverse mood reactions to marijuana also can occur, particularly among inexperienced users after smoking or eating a large dose. The most common among such acute reactions are anxiety and paranoia; others include panic, depression, depersonalization, delusions, illusions, and hallucinations. These symptoms usually disappear within hours and respond well to reassurance and a supportive environment. Seventeen percent of regular marijuana smokers report that they have experienced at least one of these symptoms at some time—typically early in their use of the drug.26
Large doses of marijuana also impair cognition. Using an imaging technique called positron emission tomography to measure the acute effects of marijuana on brain function, researchers have detected blood-flow abnormalities in volunteers after they smoked a single marijuana cigarette; specifically, circulation to the temporal lobe of the brain, which governs auditory attention, was restricted. This effect coincided with diminished performance in listening tasks. Yet smoking marijuana also appears to increase, not decrease, blood flow to the brain's frontal lobes and lateral cerebellum. The frontal lobes control a variety of cognitive functions, including abstract thinking, and are also involved in motor control and emotional reactions; the cerebellum coordinates movement and also governs some types of learning.27 The science of measuring activity in the living brain is still new. It is not entirely clear what these intriguing changes in cerebral blood flow
indicate, but they seem to support the general contention that marijuana impairs thinking.
In the 1970s, reports suggested that heavy marijuana use causes structural changes in the brain, but this finding has not been confirmed when examined with more sophisticated techniques. While more recent studies have found that heavy marijuana users make subtle mistakes in cognitive tasks after they abstain from the drug for 19 to 24 hours, some researchers have questioned the validity of this conclusion because the users may not have been matched against nonusers with comparable cognitive abilities.28
Marijuana has also been shown to affect activities that require a fine balance of attention and muscular coordination, such as driving. Such functions are governed by psychomotor processes, which include the ability to control body and limb movement, sustain attention, and respond to environmental cues with appropriate movements. A study of experienced airplane pilots showed that their performance on flight simulator tests was impaired as long as 24 hours after smoking a single marijuana cigarette. Interestingly, prior to taking the test the pilots told investigators that they were sure their performance would not be affected.29
Clearly, the evidence that marijuana impairs cognitive and psychomotor performance indicates that medical users will need to limit their activities—much as after taking a strong painkiller or drinking alcohol. No one under the influence of marijuana or THC should drive a vehicle or operate potentially dangerous equipment.
One of the most controversial effects that marijuana has been claimed to produce is a so-called amotivational syndrome. Although this syndrome is not a medical diagnosis, it has been used to describe the behavior of young people who lose interest in school, work, and social activities. When heavy marijuana use accompanies this behavior, the drug is often cited as the cause, despite the fact that no convincing data demonstrate that marijuana actually provokes these symptoms.
It is not enough to observe that chronic marijuana users lack drive or ambition. In order to justify such a claim, people's behavior and personality traits must be compared before and after they become regular users. Because it would be unethical to en-
courage a person to use marijuana heavily, such research can only be conducted on people who become users on their own. An epidemiological survey could be used to identify such young people and might shed light on the relationship between motivation and marijuana use. But while such a study might show that marijuana users tend to lose motivation compared with nonusers, it could not be used to establish that marijuana use causes people to become unmotivated.
A major question remains as to whether marijuana can produce severe and lasting psychotic disorders. There are clinical reports of marijuana-induced states that resemble psychoses such as schizophrenia, depression, and mania, with symptoms that last a week or more. Some researchers have argued that the diversity of these symptoms belies the existence of a specific “marijuana psychosis.” Others have concluded that heavy marijuana use—and perhaps even acute use in especially sensitive people—can produce a psychosis characterized by a suite of symptoms such as confusion, amnesia, delusions, hallucinations, anxiety, and agitation. Regardless of which of these interpretations is correct, both camps agree that marijuana use alone—without the influence of additional risk factors—is unlikely to provoke a psychosis that persists longer than intoxication.30
Drug abuse is common among people with mental illness. Thus, it is not surprising that several (but not all) studies have shown that a disproportionately large number of people with schizophrenia use marijuana. The association between marijuana and schizophrenia is not well understood, however. While experts generally agree that heavy marijuana use can provoke schizophrenic episodes in susceptible individuals, they also concur that the drug does not cause the underlying disorder. Additional research indicates that people with schizophrenia prefer the effects of marijuana over those produced by alcohol and cocaine, which they generally use less often than does the general population. The reasons for this preference remain unknown, but it suggests that marijuana might give these patients some relief from their symptoms. But people with schizophrenia or a family history of the disease should understand that using marijuana puts them at a greater than average risk for adverse psychiatric reactions.31
Some of marijuana's psychological effects may prove to be
medically useful. For example, the antianxiety properties of cannabinoids may help relieve conditions worsened by anxiety, such as movement disorders or nausea. It is also possible that the euphoric good feelings of the marijuana high could enhance the benefits of marijuana-based medicines for pain relief or appetite stimulation. On the other hand, cannabinoid-induced euphoria or sedation may simply mask symptoms, leading some users to the false belief that marijuana improves their medical conditions. That is a problem if it causes patients to choose marijuana over more effective conventional medicines that have fewer undesirable side effects. Thus, the IOM researchers recommended that any future clinical trials of cannabinoid drugs include an evaluation of their psychological impact.
MEDICAL MARIJUANA: A DANGER TO SOCIETY?
Almost everyone who spoke or wrote to the IOM study team about medical marijuana's potential harms felt that acknowledgment of marijuana 's possible medical value would undermine its reputation as a dangerous drug, particularly among young people. Yet if marijuana-based drugs were to be developed, they would join a wide variety of effective medications known to be dangerous if misused. While it is important to explore the various ways that medical use of marijuana might encourage drug abuse, it must also be recognized that marijuana is hardly unique among medicines in carrying a burden of risk.
The question is not so much whether marijuana can be both harmful and helpful but whether public perception of its benefits will lead to increased abuse. There is also the concern that experience with marijuana may prompt people to use harder drugs, triggering a general rise in the abuse of illegal substances.
Those who depict marijuana as a so-called gateway drug recognize that other illicit drugs, such as cocaine or heroin, are even more dangerous to both individual health and society as a whole. The gateway concept also reflects strikingly consistent patterns of drug use from adolescence to adulthood. Because it is the most widely used illegal drug, marijuana is predictably the first one that most people encounter, including users who later turn to other illicit substances. Before experimenting with marijuana,
however, most future drug users become well acquainted with alcohol and nicotine—usually when they are too young to do so legally.
Discussions of marijuana as a gateway drug usually refer to—and often confuse—two distinct behavioral scenarios. The first, more often called the “stepping stone” hypothesis, is the notion that marijuana possesses pharmacological properties that compel users to experiment with harder drugs. The second and more common theory is that marijuana opens a door to the world of illegal substances. Once introduced to illicit drug use via marijuana, young people encounter increased peer pressure to try other drugs and gain easier access to them.
The stepping-stone hypothesis applies to marijuana only in the sense that individuals who enjoy marijuana's effects probably have a stronger than average attraction to mood-altering substances. In other words, many of the same factors that induce people to use marijuana are likely to predispose them to use harder drugs as well. Those factors include physiological reactions to drugs, the psychological state of the user, and the social context in which the drug is used. Additional factors are addressed by the gateway theory, which asserts that marijuana, due to its illegal status, serves as a conduit to harder drugs.
People who are most likely to use illicit drugs other than marijuana tend to share several traits, including use of alcohol or nicotine at an early age, heavy marijuana use, and psychiatric disorders. Yet while it appears that people who try alcohol and nicotine earliest are more likely than others to experiment with illegal drugs, they are no more likely to become heavy drug users. Similarly, experimental or infrequent users of marijuana are less likely to progress to harder drug use than those who smoke marijuana on a daily basis. One study of young adult males found that those who had used marijuana between 10 and 99 times in their lives were unlikely to have tried another illicit drug, while more than half of those who had used marijuana more than 100 times had done so.32
Data that have been collected on the gateway phenomenon are frequently overinterpreted. For example, in one study, researchers concluded that “marijuana's role as a gateway drug appears to have increased” based on interviews with drug abusers
who reported using crack cocaine or heroin daily.33 However, only a tiny fraction of the adult population—an estimated one to three per 1,000 people—uses crack or heroin this often. While most of the people interviewed for the study said they had used marijuana before moving on to harder drugs, that trend is not necessarily true among marijuana users in general.
Another drawback of many studies on the gateway theory is that they rely on measurements of drug use rather than drug dependence. Thus, these studies can only demonstrate that, when compared with people who have never used the drug, marijuana users are more likely to try other drugs as well; such studies do not prove that marijuana users tend to become dependent, or even frequent, users of harder drugs. The real value of this type of research is that it can reveal factors that predict whether a person will progress from using a given illegal drug to a harder one.
Marijuana is a gateway drug in the sense that its use typically precedes rather than follows initiation into other illicit substances. On the other hand, marijuana use per se does not appear to be a gateway to the extent that it is a cause, or even a significant predictor, of hard drug abuse. Instead, the most consistent predictors of hard drug abuse appear to be intense marijuana use, psychiatric disorders, and a family history of psychological problems or alcoholism.
It is also important to recognize that research on drug progression has focused exclusively on recreational use. It does not follow that if marijuana were available by prescription for medical use the pattern of subsequent drug progression among medical users would be the same as for recreational users. In fact, a study of nonmedical use of psychoactive prescription drugs—including tranquilizers, antidepressants, and opiate painkillers—failed to find that a clear or consistent sequence of drug use following the abuse of these medications. At present, data on drug use neither support nor refute the assertion that legalizing marijuana for medical purposes would prompt increased drug abuse among medical marijuana users.
A related but distinct concern is whether the use of marijuana for medical purposes would encourage drug use throughout society in general. Unless and until marijuana is approved for medical treatment, we can only speculate about the answer to this
question. However, reasonable inferences can be drawn about the outcome of such a change based on three examples: patterns of abuse for opiate drugs, including painkillers such as morphine and codeine; patterns of drug abuse in the Netherlands and also in some parts of the United States, where marijuana was decriminalized in the 1970s; and the short-term consequences of the campaign to legalize medical marijuana in California in 1996.
Opiates can be considered a “stand-in” for marijuana-based medicines since both classes of drugs have the potential to be abused to great harm as well as to be used for medical benefit. Earlier in this century some physicians raised concerns that liberal use of opiates would cause many patients to become addicted to the drugs. Such worries have proven unfounded, and it is now widely recognized that physicians often needlessly limit doses of opiate medications to patients in pain out of fear of producing addicts. Today, opiates are carefully regulated by medical caregivers and rarely diverted from legitimate use to the black market.
There is no evidence to suggest that the use of opiates or cocaine for medical purposes has increased the perception that the illicit use of these drugs is safe or acceptable. Clearly, some patients may abuse these substances for their psychoactive effects, and others may divert them to recreational users. The same problems have occurred with several other medications, most of which are included in Schedule II of the Controlled Substances Act. Both the dispensation and manufacturing of Schedule II drugs are strictly controlled, and physicians are cautioned to monitor their use by patients who may be at risk for drug abuse.
Two studies designed to probe the effects of marijuana decriminalization have reported somewhat conflicting conclusions. Monitoring the Future, an annual survey of high school seniors, revealed that students in states that had decriminalized marijuana did not report using the drug more than their counterparts in states where marijuana remained illegal between 1975 and 1980.34 Another study, based on drug-related emergency room (ER) cases, concluded that decriminalization had increased marijuana use.35 It indicated that among states that had decriminalized marijuana in 1975-1976, there was a greater increase between 1975 and 1978
in the number of ER patients who had used marijuana than in states that did not decriminalize the drug.
However, the study also found that by 1978 the proportion of marijuana users among ER patients was about equal in states that did and did not decriminalize marijuana; prior to decriminalization, states in which marijuana continued to remain illegal had higher rates of marijuana use than those that eventually legalized the drug. In contrast to marijuana use, rates of other illicit drug use among ER patients were substantially higher in states that did not decriminalize marijuana. Thus, there is more than one possible explanation for the relatively greater increase in marijuana use in the decriminalized states: on the one hand, decriminalization may have led to an increased use of marijuana; on the other hand, where marijuana remained illegal, people may have been less likely to discriminate between it and other illicit substances, a view that would tend to increase the use of hard drugs.
In 1976 the Netherlands adopted a policy making it legal for individuals to possess up to 30 grams of marijuana. Research indicates that little change in marijuana use occurred for seven years following this change in policy; however, in 1984, when “coffee shops” that sold marijuana began to spread throughout Amsterdam, marijuana use started to increase. During the 1990s, marijuana use continued to increase in the Netherlands at the same rate as in the United States and Norway—two countries that strictly forbid the sale and possession of marijuana. Nearly equal percentages of American and Dutch 18 year olds were found to have used marijuana during this period, while Norwegian 18 year olds were about half as likely to have used marijuana. Although these results offer little evidence that the Dutch decriminalization policy itself led to increased levels of marijuana use, it appears that the commercialization of marijuana sales may have done so.
According to the most recent National Household Survey on Drug Abuse, significantly fewer children between the ages of 12 and 17 reported that they perceived marijuana as a “great risk of harm” in 1997 than in 1996.36 At first glance this might seem to validate the fear that the medical marijuana debate of 1996—prior to passage of the California medical marijuana referendum in November 1997—had caused more teenagers to believe that marijuana use is safe. But a closer analysis of the data show that, de-
spite exposure to a statewide advertising campaign in favor of medical marijuana, teens in California were actually an exception to the national trend: their perception of marijuana's harmfulness did not decrease between 1996 and 1997. Thus, there is no evidence that the medical marijuana debate has altered adolescents' perceptions of the risks of using marijuana.37
WEIGHING MARIJUANA'S HARMS
For most people the main adverse effect of acute marijuana use—that is, the immediate effect of a single potent dose—is diminished psychomotor performance. A few people also experience bad feelings that range from uneasiness to profound emotional discomfort. Marijuana and marijuana-based drugs pose a greater danger to people at risk for psychiatric disorders, especially those who are vulnerable to substance dependence. This spectrum of risk for acute side effects lies well within tolerable limits for prescription medications.
An even more important concern about medical marijuana is the drug 's chronic side effects (those that crop up during extended use). These effects fall into two categories: the long-term consequences of smoking and the risks of chronic exposure to THC. Marijuana smoke, like tobacco smoke, is associated with increased risk of cancer, lung damage, and poor pregnancy outcomes. Smoked marijuana is thus unlikely to prove to be a safe medication for any chronic medical condition.
A less prevalent side effect of protracted marijuana use is dependence, which tends to occur only in a vulnerable subpopulation of users, most notably adolescents with conduct disorder. As one might expect, people with psychiatric problems and those vulnerable to substance abuse may be at risk of becoming dependent on medical marijuana.
In addition to the dangers of smoke inhalation, another drawback of using marijuana cigarettes as a drug delivery system is their highly variable composition. Plants grown under different conditions contain variable mixtures of cannabinoids, and their dried leaves may also be contaminated with toxic bacteria and fungus.
As for the notion that the sanctioning of medical marijuana
might lead to an increase in its nonmedical use or to drug abuse in general, no convincing data exist that support this concern. Research suggests that, if marijuana were as closely regulated as other medications with abuse potential, it would pose no special threat of increased abuse; however, no existing study has directly addressed this question. Even if it could be demonstrated that medical use of marijuana would decrease the perception that it can cause harm, this evidence would not be pertinent to the legal regulation of marijuana-based therapeutics. Whether a drug gains federal approval for medical use hinges on its safety and efficacy for individual use, not the perceptions or beliefs it engenders in society at large.
Marijuana is not, to be sure, a completely benign substance. It is a powerful drug that affects the body and mind in a variety of ways. However, except for the damage caused by smoking marijuana, its adverse effects resemble those of many approved medications. While the effectiveness of marijuana-based medicines remains largely to be determined, existing clinical data suggest that marijuana and its component chemicals could contribute to the treatment of numerous disorders. Part II of this book explores the potential of marijuana and cannabinoids to relieve the symptoms of several specific conditions.
NOTES
1. Polen MR, Sidney S, Tekawa IS, Sadler M, Friedman D. 1993. “Health care use by frequent marijuana smokers who do not smoke tobacco. ” The Western Journal of Medicine 158:596-601.
2. Tashkin DP, Coulson AH, Clark VA, Simmons M, Bourque LB, Duann S, Spivey GH, Gong H. 1987. “Respiratory symptoms and lung function in habitual, heavy smokers of marijuana alone, smokers of marijuana and tobacco, smokers of tobacco alone, and nonsmokers.” American Review of Respiratory Disease 135:205-216.
3. Ammenheuser MM, Berenson AB, Babiak AE, Singleton CR, Whorton EB Jr. 1998. “Frequencies of hprt mutant lymphocytes in marijuana-smoking mothers and their newborns. ” Mutation Research 403:55-64.
4. Tashkin DP, et al. 1987.
5. Sidney S, Quesenberry CP Jr, Friedman GD, Tekawa IS. 1997. “Marijuana use and cancer incidence (California, United States).” Cancer Cause and Control 8:722-728.
6. Ammenheuser MM, et al. 1998.
7. Institute of Medicine. 1999. Marijuana and Medicine: Assessing the Science Base. Washington, DC: National Academy Press, pp. 59-68.
8. Ibid.
9. Barbers RG, Gong HJ, Tashkin DP, Oishsi J, Wallace JM. 1987. “Differential examination of bronchoalveolar lavage cells in tobacco cigarette and marijuana smokers.” American Review of Respiratory Disease 135:1271-1275.
10. Institute of Medicine. Marijuana and Medicine, pp. 112-113.
11. Ibid., pp. 121-122.
12. Ibid., pp. 122-125.
13. Dreher MC, Nugent K, Hudgins R. 1994. “Prenatal marijuana exposure and neonatal outcomes in Jamaica: An ethnographic study.” Pediatrics 93:254-260.
14. Fried, PA. 1995. “The Ottawa Prenatal Prospective Study (OPPS): Methodological issues and findings.” Life Sciences 56:2159-2168.
15. American Psychiatric Association. 1994. Diagnostic and Statistical Manual of Mental Disorders (DSM-IV). Fourth edition. Washington, DC: American Psychiatric Association.
16. Haney M, Ward AS, Comer SD, Foltin RW, Fischman MW. 1999. “Abstinence symptoms following oral THC administration in humans.” Psychopharmacology 141:385-404.
17. Childers SR, Breivogel CS. 1998. “Cannabis and endogenous cannabinoid systems.” Drug and Alcohol Dependence 51:173-187.
18. Jones, RT, Benowitz N, Bachman J. 1976. “Clinical studies of tolerance and dependence.” Annals of the New York Academy of Sciences 282:221-239.
19. Dreher MC, et al. 1994.
20. Bailey SL, Flewelling RL, Rachal JV. 1992. “Predicting continued use of marijuana among adolescents: The relative influence of drug-specific and social context factors.” Journal of Health and Social Behavior 33:51-66.
21. Crowley TJ, Macdonald MJ, Whitmore EA, Mikulich SK. 1998. “Cannabis dependence, withdrawal, and reinforcing effects among adolescents with conduct symptoms and substance use disorders.” Drug and Alcohol Dependence 50:27-37.
22. Lyons MJ, Toomey R, Meyer JM, Green AI, Eisen SA, Goldberg J, True WR, Tsuang MT. 1997. “How do genes influence marijuana use? The role of subjective effects.” Addiction 92:409-417.
23. Kendler SA and Prescott CA. 1998. “Cannabis use, abuse, and dependence in a population-based sample of female twins.” American Journal of Psychiatry 155:1016.
24. Anthony JD, Warner LA, Kessler RC. 1994. “Comparative epidemiology of dependence on tobacco, alcohol, controlled substances and inhalants: Basic findings from the National Comorbidity Survey.” Experimental and Clinical Psychopharmacology 2:244-268.
25. Robins LN and Regier DA, eds. 1991. Psychiatric Disorders in America: The Epidemiologic Catchment Area Study. New York: Free Press.
26. Institute of Medicine. Marijuana and Medicine, p. 84.
27. Ibid., p. 106.
28. Ibid., pp. 106-107.
29. Yeasavage JA, Leirer VO, Denari M, Hollister LE. 1985. “Carry-over effects of marijuana intoxication on aircraft pilot performance: A preliminary report.” American Journal of Psychiatry 142:1325-1329.
30. Institute of Medicine. Marijuana and Medicine, pp. 105-106.
31. Yeasavage JA, et al. 1985.
32. Institute of Medicine. Marijuana and Medicine, p. 100.
33. Golub A and Johnson BD. 1994. “The shifting importance of alcohol and marijuana as gateway substances among serious drug abusers.” Journal of Studies on Alcohol 55:607-614.
34. Johnston LD, O'Malley PM, Bachman JG. 1989. “Marijuana decriminalization: The impact on youth, 1975-1980.” Journal of Public Health 10:456.
35. Model KE. 1993. “The effect of marijuana decriminalization on hospital emergency room drug episodes: 1975-1978.” Journal of the American Statistical Association 88:737-747.
36. Substance Abuse and Mental Health Services Administration. 1998. National Household Survey on Drug Abuse: Population Estimates 1997. DHHS Pub. No. (SMA) 98-3250. Rockville, MD: SAMHSA, Office of Applied Studies.
37. Institute of Medicine. Marijuana and Medicine, p. 104.

































