
1
Introduction
ROLE OF BEHAVIORAL AND SOCIAL FACTORS IN HEALTH AND DISEASE
For more than a decade it has been well established that approximately half of all causes of morbidity and mortality in the United States are linked to behavioral and social factors (McGinnis and Foege, 1993; NCHS, 2003a). In fact, the leading cause of preventable death and disease in the United States—smoking—significantly increases the risk of lung cancer and chronic lung disease, as well as the risk of heart disease and stroke (CDC, 1999; Mokdad et al., 2004; NCHS, 2003a). A sedentary lifestyle, along with poor dietary habits, has also been associated with increased risk of heart disease, as well as a myriad of other adverse health conditions, and may soon overtake tobacco as the leading cause of preventable death (Graves and Miller, 2003; Mokdad et al., 2004; Morsiani et al., 1985; U.S. DHHS, 2001). Alcohol consumption is the third leading cause of preventable death in the United States (Mokdad et al., 2004). And although moderate alcohol intake may have some protective effects against heart disease, excessive consumption has been linked to a variety of potentially preventable conditions (Maekawa et al., 2003; Nanchahal et al., 2000; Pessione et al., 2003).
Illnesses related to behavioral factors include, among others, cancer, heart disease, poor pregnancy outcome, chronic obstructive pulmonary disease, type II diabetes, and unintentional injury (Hoyert, 1996; NCHS, 2003a; NHLBI, 2003a,b; U.S. DHHS, 1996). In addition to these adverse health effects of harmful behaviors, psychological and social factors have been shown to influence chronic disease risk and recovery. Psychological factors, such as personality, developmental history, spiritual beliefs, expectations, fears, hopes, and past experiences, shape
people’s emotional reactions and behaviors regarding health and illness. Social factors, including support of family and friends, institutions, communities, culture, politics, and economics, can have profound effects as well. Indeed, scientific evidence is increasing on the effects of psychological and social factors on biology, and recent studies have demonstrated that psychosocial stress may be a significant risk factor for a variety of diseases (Barefoot et al., 2000; Carroll et al., 1976; Everson et al., 1996; Frasure-Smith et al., 1993; Kawachi et al., 1996; Leserman et al., 2000; Mayne et al., 1996; Orth-Gomer et al., 1993). In the case of heart disease, for example, psychosocial stress appears to contribute directly to atherosclerotic processes by narrowing blood vessels, thus restricting circulation (Bairey Merz et al., 2002; Williams et al., 1991).
Theories underlying behavioral interventions aimed at modifying disease course are based on the assumptions that behavioral and psychosocial influences on disease course are modifiable and that curtailing unhealthy practices will slow disease progression or minimize the recurrence of disease following treatment (IOM, 2000). Understanding that behavior can be changed and that proven methods are available to facilitate such change allows physicians to provide optimal interventions—behavioral and nonbehavioral—to improve the health of patients. Identifying personal, familial, social, and environmental factors that may affect a patient’s health enables physicians to provide better, more patient-centered care (IOM, 2001a, 2003a). In addition, physicians must be able to recognize their own personal and social biases and perceptions to best serve the needs of their patients.
Although the scientific evidence linking biological, behavioral, psychological, and social variables to health, illness, and disease is impressive, the translation and incorporation of this knowledge into standard medical practice appear to have been less than successful. To make measurable improvements in the health of Americans, physicians must be equipped with the knowledge and skills from the behavioral and social sciences needed to recognize, understand, and effectively respond to patients as individuals, not just to their symptoms. Sobel (2000:393), an expert in mind–body health care, notes that “more and more studies point to simple, safe and relatively inexpensive interventions that can improve health outcomes and reduce the need for more expensive medical treatments. Far from a new miracle drug or medical technology, the treatment is simply the targeted use of mind–body and behavioral medicine interventions in a medical setting.” Thus, physicians with an understanding of disease causation that extends beyond biomedical approaches are more likely to see better intervention outcomes than have been achieved to date (IOM, 2000).
The limitations of a strictly biomedical approach to health care as described by Engle suggest the need for a model of medical school education designed to provide an integrative and multilevel understanding of how biological, psychological, and social variables interact in health and illness (Engel, 1977). Others have expanded upon and explicated such a biopsychosocial model (Anderson and
Scott, 1999; Evans and Stoddart, 1990). The term “biopsychosocial,” however, appears to imply three separate spheres while omitting other key disciplines, such as the behavioral sciences and economics. A unified approach that is more inclusive than both the biomedical and biopsychosocial models is needed as a curricular framework for medical education (see Figure 1-1 for an example of such a model).
A number of demographic factors in the United States also underscore the need for more attention to the behavioral and social components of health. First, the proportion of the population aged 65 and over is expected to grow by 57 percent by 2030 (U.S. Bureau of the Census, 1996), and with Americans now having an average life expectancy of 77 years (NCHS, 2003b), physicians need the knowledge and skills to care for this aging population. To this end, they must understand the interplay of social and behavioral factors (e.g., diet, exercise, and familial and social support) and the role these factors play in delaying or preventing the onset of disease and slowing its progression. Physicians also need to have been trained in pain management and means of improving quality-of-life measures that are essential to providing patient-centered care. Knowledge and skills in both of these areas are especially critical for the treatment of chronic conditions, common in this population, that require palliative care.
A second demographic change is the rising percentage of minorities in the overall U.S. population. According to U.S. census data, 26 percent of the current
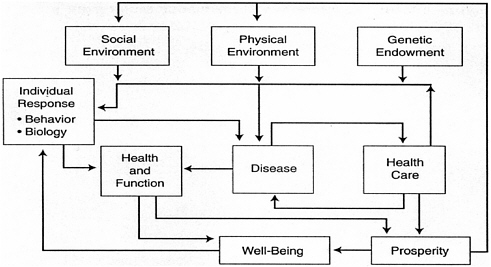
FIGURE 1-1 Model of the determinants of health. This model is a theoretical delineation of the interacting forces that contribute to the health, functional status, and well-being of an individual (or a population). Reproduced with permission from Elsevier Science Ltd.
SOURCE: Evans and Stoddart (1990).
population is nonwhite, a proportion that is expected to increase to almost 47 percent by 2050 (U.S. Bureau of the Census, 1996). The country’s growing cultural and ethnic diversity presents new challenges and opportunities for physicians and other health professionals, who must become culturally competent and better skilled in communicating and negotiating health management with diverse populations (Crawley et al., 2002; IOM, 2003c; Satterfield et al., 2004).
PURPOSE OF THE STUDY
For nearly three decades, persistent calls have been made to formally educate undergraduate medical students in the behavioral and social sciences to help establish a critical foundation for providing good clinical care (Bolman, 1995; Carr, 1998; Engel, 1977; Krantz et al., 1999). Increasingly, medical schools have introduced courses with behavioral and social science content into their curricula. However, current educational practices are uneven in their comprehensiveness and clinical applicability, and all too often, newly trained physicians cannot effectively translate behavioral and social science knowledge, skills, and attitudes into effective patient care. Given that nearly half of all patients present with conditions that are significantly influenced by such factors, continued lack of attention to this aspect of medical school training is no longer acceptable. Applying the behavioral and social sciences to medicine should not be a marginal effort, but a part of mainstream medical education.
STUDY ORIGIN AND TASKS AND ORGANIZATION OF THE REPORT
This study was undertaken to enhance the behavioral and social sciences in medical school curricula in response to a request from the National Institutes of Health (NIH) and The Robert Wood Johnson Foundation. In the fall of 2002, the Institute of Medicine convened a committee to examine the content and effectiveness of behavioral and social science teaching in medical school education. The committee was asked to:
-
Review the approaches used by medical schools that have tried to incorporate behavioral and social sciences into their curricula.
-
Develop a list of prioritized topics from the behavioral and social sciences for possible inclusion in medical school curricula. As an alternative to a numerical list, clustered priorities (e.g., top, high, medium, and low) may be assigned to topic areas.
-
Provide options for how changes in curricula can be achieved, such as encouraging the leadership of medical schools to incorporate behavioral and social sciences, funding opportunities that would achieve this goal, or other novel approaches that would achieve this aim. In developing these options, the barriers
-
to implementing curricula change and approaches to overcoming these barriers should be considered.
To address the tasks described above, the committee met five times between December 2002 and October 2003, and cast a broad net to capture the relevant information. It held public meetings with medical schools and other organizations to explore and discuss relevant information regarding the status of teaching behavioral and social science in medical schools. The committee also reviewed and considered information from the published literature, medical school websites, and a variety of other sources. (See Appendix A for details regarding the methods that the committee used to address the statement of task.)
Each chapter of this report responds to one of the three tasks listed above. Chapter 2 reviews and describes currently available information on the incorporation of the behavioral and social sciences into undergraduate medical education. Included is a brief historical overview of curriculum changes in medical schools. Chapter 3 expands on the importance of including the behavioral and social sciences in medical school curricula. It also presents the 26 priority topics identified by the committee, along with the rationale for their selection. Included as well is a description of the type of content that would enable medical students to demonstrate competency in these areas. Chapter 4 provides an overview of successful strategies for creating and sustaining curriculum change in multiple areas of medical education. These strategies are discussed as they apply to behavioral and social science content and are accompanied by an analysis of the influence of national examinations on curricular content.





