8
WORKING GROUPS, DAY 2
WORKING GROUP 5: IMMUNOLOGY, ASSAY STANDARDIZATION, AND CORRELATES OF PROTECTION
Chairpersons—Ann Arvin and Brian Murphy
Briefer—Brian Murphy
Rapporteur—Ann Arvin
Focus: The focus of this group will be research needed to improve understanding of the immune response to influenza infection or vaccination; to enhance comparability of results between laboratories; and to identify correlates of protection that will facilitate testing and licensure of candidate vaccines.
Specific Questions:
-
What studies are needed to better assess the role of antibody to neuraminidase in protection against influenza disease or its complications?
-
What studies are needed to assess the importance of cellular immunity following influenza disease or the potential importance of cellular immunity in response to vectored vaccines?
-
What research is needed to develop, validate, and standardize immunological assays to facilitate vaccine evaluation and licensure?
-
What research is needed to evaluate the immune response to influenza vaccine delivered by different routes of administration?
-
What studies are needed to better define or validate proposed immune correlates of protection for different influenza strains and in different populations?
-
What research is needed to better understand mucosal immunology and influenza?
Rapporteur Report—Dr. Ann Arvin
A key priority is to develop, validate, and standardize serologic tools for pandemic preparedness. We focused on improving neutralization assays for antibodies against avian strains; standardizing protocols; engineering an inoculum so it could be used in a Biosafety lab 2 setting; and boosting automation, which might include robotics but also new reagents such as fluorescentated or luciferase tagged inocula.
Improving HAI methods for detecting H5 antibodies is also important.. Developing ELISA methods for a variety of HA subtypes is considered important and includes developing standardized, purified, or recombinant HA and NA proteins, as well as reference serum panels to facilitate the development and use of ELISA-based assays.
We recommend efforts to develop and standardize assays for antibodies to NA, and to evaluate and correlate the subtype ELISAs with a gold standard functional assay, e.g. a neuraminidase inhibition method.
Sero-epidemiology research is important for pandemic preparedness. Such research should include studies to understand pre-pandemic antibody levels in human populations in key areas to HA and NA proteins, and investigating potential cross-protection provided by human anti-HA or anti-NA antibodies against the avian strains.
A longer-term goal is to develop simpler serologic assays for field use. It seems most prudent and practical to do this work on assay development and standardization in centralized reference laboratories, but we ultimately need to develop techniques that can be transferred to field laboratories.
We discussed the need to investigating immune correlates of protection extensively. A much broader and deeper understanding of the human immune response to flu infection in general, as well as to vaccines is needed, based on using modern immunologic techniques. Examples include subtype-specific ELISAs and new assays, focusing on trying to better understand protection and cross-protection by antibodies to these proteins; and the role of IgG and IgA in serum and mucosal sites that have specificity for these proteins in protection.
We conclude that it is important to use the many new methods now available to probe human immune responses against primary and secondary flu infections with non-pandemic strains. These studies would give us a repertoire of methods to apply immediately to evaluate host responses in a pandemic setting. Examples of this kind of work include better characterizing flu-specific memory T cells and B cells, and aspects of trafficking of immune cells that can be studied now, such as lung trafficking and trafficking to mucosal epithelium. What is the role of cross-protective immunity by T cells that recognize various flu proteins? We can now study all of these questions in new ways.
Applying new immunologic assays to understand protective immunity requires their use in the context of prospective studies, using clinical endpoints and viral shedding to define a true correlate of protection, as opposed to just to measuring an immune response in the absence of information about viral replication.
We recommend efforts to improve understanding of the consequences of antigenic drift in H5 strains. New tools should be used to better understand the immunopathogenesis of complex and fatal flu infections, not just in the pandemic setting, where obtaining samples may be difficult, but also during annual epidemics. New tools and a better network for sharing patient samples for testing would enable us to better analyze the mechanisms that lead to these unusual situations.
Additional research to evaluate flu vaccine immunity is necessary. This work should be based on some of the same concepts discussed for assessing the response to natural infection and defining protective immunity. In this case, the goal should be to develop a panel of standardized immunologic assays that can be used as background information for designing pandemic vaccines that would engender the best repertoire of immune responses in the shortest time after vaccination.
In this context, we recommend comparing the capacities of existing inactivated, live attenuated, and vectored vaccines for inducing humoral and cellular and mucosal immunity,
during primary and secondary vaccination, and with varying routes of administration of the vaccines.
These studies should focus on immunogenicity and efficacy in populations at the extremes of age, especially infants and the elderly, including the very elderly. The interval required to induce a protective immune response after immunization is key to understanding the best vaccine for a pandemic setting. Responses that are reliably associated with reduced viral shedding must be defined and persistence of the immune response is another important factor.
Finally, it is important to generate experience with multiple pandemic vaccines to assess reactogenicity, immunogenicity, optimal dose, and route of administration. In our final analysis, gaining a broad understanding of the immune response to both natural infection and vaccines for as many different HA and NA viruses is a priority, as is looking not just at the standard serologic responses but also at cellular immune responses.
WORKING GROUP 6: PANDEMIC VACCINES—ASSESSMENT, DEVELOPMENT AND PRODUCTION STRATEGIES
Chairperson—John Treanor
Briefer—Harry Greenberg
Rapporteur—Regina Rabinovich
Focus: The focus of this group will be to identify research needed to improve the production, evaluation, and use of existing in an influenza pandemic; to improve their immunogenicity; and to decrease the amount of antigen needed per dose through alternative formulations or routes of administration. This group also will define research needs associated with development and evaluation of new vaccines, new approaches to vaccine production, and potential new antigens to target in influenza vaccines such as conserved structural viral proteins.
Specific Questions:
-
What research is needed to better define the potential for common antigen vaccines against heterologous strains including avian influenza strains and for the optimal approach to their development?
-
What studies are needed to identify and study adjuvants that may provide an antigen-sparing effect with influenza vaccines?
-
What studies are needed to assess intradermal administration as an immunogenicity enhancing or antigen sparing measure?
-
What research is needed to develop and assess new devices or strategies for vaccine administration intradermally, transcutaneously, or intranasally?
-
What research is needed to develop and assess new vaccine production strategies?
-
What technologies hold promise and what studies are needed to evaluate candidate influenza vaccines or vaccination strategies?
Rapporteur Report-Dr. Regina Rabinovich
A central theme of the discussion is that a pandemic vaccine needs to use technologies, tools, and processes that are integrated into inter-pandemic influenza vaccines. Otherwise, there is no market for such vaccines, and thus no surge capacity. Improving the efficacy, effectiveness, ease of administration and production, and routine use of all influenza vaccines is the technical framework for influenza pandemic preparedness.
An immediate and long term need is broad access to critical reagents (some which may involve management of intellectual property and know-how), such as influenza isolates, validated assays, serum panels, or platform technologies. Whether collected by government, academic researchers, or developed by the private sector, delayed access to these for either business or academic reasons can slow the development of new influenza vaccines. But much of the funding for collecting and creating these tools comes from the public sector, and we need to ensure their access by the global community. Respect for intellectual property surrounding
platform technologies, a keystone of the U.S. pharmaceutical industry, is not incompatible with this goal, but negotiated agreements to manage this may be necessary.
If we take access to these tools as given, pandemic planning requires a quiet revolution in influenza vaccines, and making the case for industry involvement in manufacturing these vaccines is critical. This effort requires a research program that actually yields a usable product rather than a special vaccine that sits in the freezer awaiting deployment during a pandemic. If it does not, pandemic flu will be akin to orphan diseases such as malaria, where the market is limited and the drivers for investing in the technologies that the research community is developing are somewhat mysterious. A specific concern in pursuing development of novel vaccines along with manufacturing of annual supply is competition between inter-pandemic and pandemic vaccine development and manufacturing, in some instances even at the pilot lot level, because production will require the same facilities and there are relatively few players. Research and product development for influenza need to be managed and integrated. And global challenges in scale and implementation—that is, universal access to some sort of vaccine-based intervention—are the 900-pound gorilla.
In terms of priorities, our first is to improve production. Enhanced understanding of the molecular factors that influence viral growth in any substrate is needed. In the short term, improved egg manufacturing yield and capacity may be possible – although there are clearly enormous regulatory barriers to changing manufacturing processes for licensed vaccines - with greater use of influenza vaccine in the inter-pandemic period as the market driver.
Our medium-term priority is a cell-culture vaccine, which would be a new vaccine from a regulatory perspective and thus would require safety and efficacy data. A cell-culture approach to vaccine production has been plagued by low yields and the technology is still unproven. We identified a couple of cell substrates that are perhaps furthest ahead. One is MDCK, whose safety issues could be evaluated based on specific scientific criteria. Regulatory barriers to using new cell lines for production have apparently been overcome by one European company, with plans to license and produce an influenza vaccine based on MDCK cells in 2006. Data to support this claim were not reviewed.
In the long-term column is a totally new way of producing influenza vaccine based on processes used for other vaccines. A second long-term priority is improving immunogenicity. This goal could include increasing vaccine potency through the use of adjuvants; and new routes, mechanisms, and tools for different formulations and routes of delivery. Achieving this goal will require head-to-head testing of existing vaccines.
Another priority is to generate full dose-response curves for both intradermal and intramuscular delivery, because it is not clear that these that flu vaccine has been optimized for immunogenicity. We also need clinical evaluation of alternate routes that may be dose-sparing, as well as of nearer-term adjuvants and other approaches in the early stages of development. Developing novel adjuvants and formulations is not a minor endeavor, and thus is a medium-term priority.
We also need to improve immunogenicity by improving heterosubtypic potency. One approach that is furthest off and highest risk—but potentially high payoff—is the common protein vaccine, with clinical data from one candidate pending. We also discussed what we know and don't know about heterosubtypic protection following cold-adapted influenza vaccine. An existing trial will probably be informative.
Questions that could be answered in the short-term include more knowledge of the immune response to wild-type H5. Precious samples from that virus are not available, and collecting them needs to become a priority, because we are missing opportunities to evaluate them.
We also discussed the potential of DNA vaccines, vectors, and expressed flu proteins. Recombinant-DNA, protein-based vaccines, which can copy a viral protein without changes, or some new technology could be viable. DNA vaccines deserve special mention because of the mouse data from Margaret Liu, and because they offer so many advantages in yield and the ability to deal with pandemic flu if we can make them work in humans.
Finally, we need to improve clinical evaluation by performing challenge models and head-to-head comparisons, and by improving criteria and methods for assessing safety, efficacy, and immunogenicity. A priority is to create the infrastructure for the human challenge model using pandemic HAs and NAs on the challenge virus, including finding locations, critical reagents, and funding for these studies. We also see validating surrogate markers as a priority, particularly in the context of a priming dose for a population.
Working Group 6 Presentation: Pandemic Vaccines-Assessment, Development and Production Strategies, Dr. Rabinovitch, Rapporteur
|
General Issues
|
TABLE 1 Research Priorities for Vaccine Assessment, Development, and Production
|
Research Areas |
||
|
1. Improved Production of Vaccines—general issues Increased growth Cell substrate Eggs vs. cells Limits to eggs PER.C6 or MDCK Rapidly identify the appropriate flu isolate in accepted cell line |
||
|
|
Short term research priorities - < 2 year |
|
|
• |
Research to enhance understanding of the molecular factors that influence viral growth in any substrate |
|
|
• |
Research to improve egg manufacturing yield or capacity – lack of diversity or assurance of supply of eggs —greater use of influenza vaccine in inter-pandemic years would be a market driver Eggs vs. cells – a “no brainer” but… —Cells still have low yield – yet unproven —European cell based influenza vaccine in 2006 (MDCK) |
|
|
Medium term research priorities – 3 -10 year |
||
|
• |
Research to develop a cell culture vaccine. This would be a “new vaccine” and would require a body of safety and efficacy (could use surrogate) research to support licensure in the US —Cell substrates (such as PER.C6 or MDCK) —Others have advantages of being approved but are not as good candidates than these 2 above —MDCK – safety of cell substrate – can develop scientific criteria rather than a generalized concern |
|
|
• |
Research to facilitate evaluation of characterized cell line in context of new understanding of factors that influence growth |
|
|
Long term research priorities- >10 years |
||
|
• |
Research to develop a totally new way of producing influenza vaccine (i.e., e coli) |
|
|
2. Improve Immunogenicity – general issues Increased potency adjuvant route (intradermally/intramuscularly) formulations head-to-head cold adapted influenza virus (CAIV) vs. trivalent influenza vaccine (TIV) |
||
|
|
Short term research priorities - < 2 year |
|
|
• |
Research that generates full dose response curves - flu vaccine has never been optimized for immunogenicity at the currently accepted dose; (some are ongoing; need to be done for both intradermal (ID) and intramuscular (IM). |
|
|
• |
Research on the clinical evaluation of alternate routes for dose-sparing -should be done up front. |
|
|
• |
Evaluate alum and MF59 and other late stage adjuvants. |
|
|
Medium term research priorities – 3 -10 year |
||
|
• |
Research to develop novel adjuvants are longer term, particularly for US where only alum is licensed in flu vaccine. |
|
|
• |
Research to develop novel formulations (such as adjuvanted patch) |
|
|
3. Improve Immunogenicity: Understanding Heterosubtypic Potency. Increase heterosubtypic potency Mechanisms for crossreaction Cold adapted influenza virus (CAIV) vs. trivalent influenza vaccine (TIV)? Common ag T cell immunity vs. Ab to HA/NA Pre-prime pop with heterosubtypic H5/H9/etc? |
||
|
|
Short term research priorities - < 2 year |
|
|
• |
Research to document that heterosubtypic protection does happen post CAIV – analysis of ongoing trial may suffice. |
|
|
• |
Research to determine if there is a fundamental difference between H5 and H3 or H1. How much of the response is the virus and the immune response? |
|
|
• |
Urgent Research: Need to know more about immune response to wild type H5 |
|
|
• |
Research on role of other proteins in pathogenesis |
|
|
Long term research priorities- >10 years |
||
|
• |
Common protein vaccine —Existing preclinical data more related to severity/death than prevention of infection —lower priority for public sector —Would benefit from reviewing all potential proteins for systematic analysis particularly if role in pathogenesis is not understood |
|
|
4. Research on Totally New Influenza Vaccines—general issues DNA vaccines Vectors Expressed flu proteins or peptides |
|||
|
|
Short term research priorities - < 2 year Issues around anti-vector immunity? rDNA protein based vaccines can copy viral protein – without changes to surface antigens that may be relevant |
||
|
Medium term research priorities – 3 -10 year rHA has been in humans and not DNA vaccine on gold bead: remains a viable approach as a vaccine, new data deserves review – will be a new vaccine |
|||
|
Long term research priorities- >10 years Same as above? Vector: some advantages |
|||
|
5. Improved Clinical Evaluation—general issues Create infrastructure for human challenge models Comparisons head-to-head Criteria and methods for safety, efficacy, and immunogenicity |
|||
|
|
Short term research priorities - < 2 year |
||
|
• |
Create infrastructure for challenge model – using pandemic HAs/NAs on the challenge virus. Could evaluate new candidates. —Places—finding locations —critical reagents —Readouts —funding $$ |
||
|
• |
Research to validate surrogate markers |
||
|
• |
Research to determine the immunologic surrogate for a priming dose for a population |
||
|
• |
Evaluate logistics for vaccination with different approaches above. |
||
WORKING GROUP 7: STRATEGIES TO CONTAIN OUTBREAKS AND PREVENT SPREAD
Chairperson – Harvey Fineberg
Briefer – Neil Ferguson
Rapporteur – Nicole Lurie
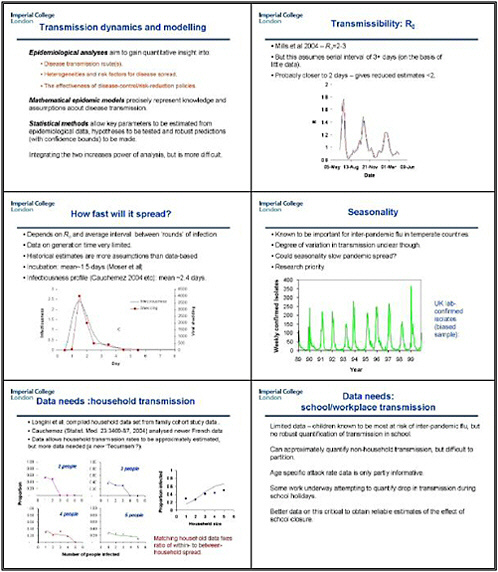
Focus: The focus of this group will be research priorities to define better strategies that may contain an initial outbreak of disease caused by a novel influenza strain or to decrease the spread of infection if containment fails. Issues to consider include priorities related to mathematical modeling; to analysis of existing data from interventions that have been implemented to control the spread of influenza or other infectious diseases; and prospective studies that could be implemented and evaluated in the context of annual influenza outbreaks.
Specific Questions:
-
What research is needed to develop and assess models for pandemic influenza and how can these models be used to identify optimal containment and/or intervention strategies or approaches to decreasing spread of disease? What are the most important questions a model or strategy must answer in containing an influenza outbreak?
-
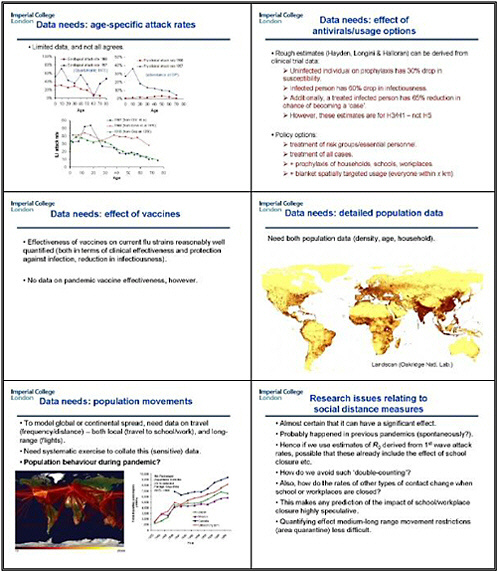
What are the most important model assumptions that must be made and what research is needed to make the assumptions reliable?
-
What research is needed to assess the relative role of model building based analyses of previous epidemics (SARS, previous influenza outbreaks ) and non-model based analyses (communication mobilization, training of health workers, stockpiling of antivirals and vaccines) for strategies to prevent spread?
-
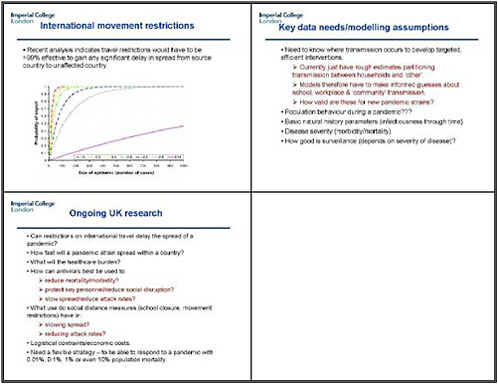
What research is needed to assess the relative effectiveness and interdependence of different control strategies (isolation and quarantine, travel restrictions, physical barriers, masks, use of antivirals, vaccines?
-
What studies are needed to better assess whether a population focus if any (children, elderly, sing, military and other clustered populations) is most important for containing spread?
-
What prospective studies are high priorities to conduct that will help in defining strategies to decrease the spread of influenza? These may include studies of vaccine strategies (e.g., vaccination of children) or use of antiviral agents.
-
What studies can be done to evaluate available data on decreasing the spread of influenza of other viral respiratory infections where results may be applicable to influenza?
Rapporteur Report—Dr. Nicole Lurie
We talked a lot about the promise and perils of models, as well as their assumptions and the need to test those assumptions. We agreed that modeling is most useful in helping us understand gaps in the assumptions and which data we need to fill them. Modeling can also take options for intervention off the table or put them on the table quickly, enabling us to prioritize them differently.
We focused on modeling not only human disease but also the agricultural epidemic, to understand the tradeoffs between “upstream” and “downstream” strategies. Should we put more money, time, and energy into trying to identify and eradicate virus in poultry in Southeast Asia now, and consider the use of antivirals or other strategies, or apply those strategies when until a pandemic hits or the disease spreads to other areas?
We need to caution policymakers not to overuse the numbers that come out of models, as precision can outpace accuracy. Mathematical models make their assumptions much more explicit than some of the mental models.
We also discussed the tradeoffs involved in inputs for the models. Some participants felt that interventions that are not socially practical or acceptable are not worth modeling, with quarantine an example. Other participants felt that if we could better understand the implications of these interventions, those results might drive policymakers and the public to regard those interventions as more doable. Because planning continually shifts during a pandemic, modeling will have a role throughout, and the assumptions underlying the model will also have to change during the pandemic.
We need to be clear that one model can't do it all, and that modeling can serve very different functions. These include not only disease transmission and control but also the vaccine supply chain, helping us understand the consequences of just-in-time delivery, for example.
We also need to model the social consequences of different interventions. For example, what are the implications of closing schools for parents’ ability to work and other social functions? If policymakers instruct people to stay home, how will they obtain food and medicine? A model can address only factors we can conceive of in advance. One aspect we cannot anticipate terribly well is how a pandemic might alter international relations.
This discussion led us to focus on the data we need to better model different outbreak and containment strategies. We recommend more comprehensive community surveillance in the inter-pandemic period, and more studies. We also need to beef up international surveillance and initiate well-placed field trials this season and next to help us both model and understand a future pandemic.
Modeling linear or additive combinations of public health measures is fairly easy, but we don't really understand what synergies among those measures may occur. Creating a good evidence base on these strategies is very important. We also need to better understand human and population behavior during a pandemic.
We wondered whether we could calibrate influenza models to SARS, and determine whether they would predict that we could contain SARS with the strategies that we actually used. Even more important is learning from the social isolation measures used to contain SARS, and from experience with anthrax, smallpox, and other infectious diseases. How do stigmatized populations who don't trust government react to such measures? What happens when different sectors of our government, including civilian and defenses agencies, respond differently?
In the short-term we need better data, and people need to share their knowledge and information with modelers so they can create better models. Input from colleagues in Vietnam and other Asian countries could prove especially valuable. Another priority is designing studies for seasonal influenza, to help us establish research protocols and clarify the kinds of data we
want to collect before a pandemic hits. Widespread use of antivirals and vaccines will require a slightly longer timeframe.
Media hype will ensure major consequences from a pandemic even if it is not the worst in history, and we need to understand the role of media in affecting the outcome. We also urgently need to connect policymakers and public health experts. We would make a plea for a trusted communicator along the lines of C. Everett Koop, who gave the public the straight scoop.
VIRAL TRANSMISSION: UNDERSTANDING AND PREDICTING PANDEMIC RISK
Working Group 8
Chairperson – Richard D. Slemons
Briefer – Daniel Perez
Rapporteur – Peter Palese
Focus: The focus of this working group is to define research needed to better understand the genetic and environmental factors responsible for animal to human and human to human influenza transmission.
Potential issues to consider:
-
What further studies are needed to define the genetic loci important for virus transmission between species?
-
What studies are needed to determine whether changes in the viral RNA polymerase play a role in virus transmission?
-
What studies are needed to define environmental factors that contribute to virus transmission and how they interact with genetic factors?
-
What studies can be done to provide measures to predict intraspecies changes in virus transmission?
-
What studies are needed to identify what measures, if any, can alter intraspecies virus transmission and what the effects of these measures?
-
What studies are needed to determine whether transmission changes can be used to predict pandemic risk?
Rapporteur Report—Dr. Peter Palese
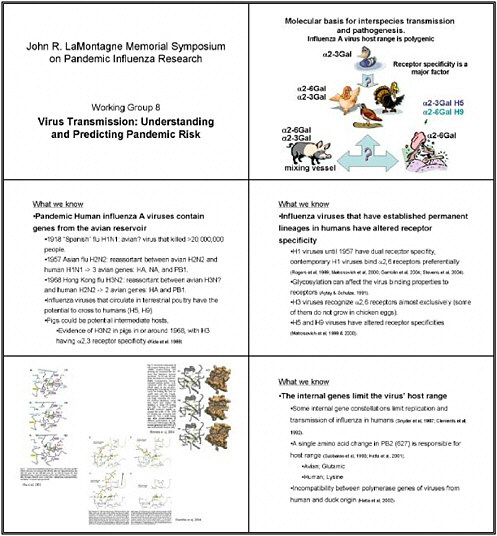
The ability of influenza viruses to be transmitted from animal to animal, from animal to human and from human to human is determined by the genome of the virus as well as by the host.
In the past, animal influenza viruses—or at least genes from animal influenza viruses—have jumped into humans. One example was the 1957 H2N2 virus, where three genes, likely from an avian source, jumped into a human H1N1 virus. This virus, possessing a novel hemagglutinin (H2), neuraminidase (N2) and a new PB1 gene circulated for 11 years in the human population. In 1968, only the hemagglutinin and the PB1 gene came from an avian virus, resulting in the new H3N2 virus. In these two cases, essentially a human virus was spiked with genes from an avian virus and the new viruses were easily transmitted from humans to humans. We don’t know the precise origin of the 1918 virus but it could also have come from birds (at least the hemagglutinin gene appears to derive from an animal influenza virus strain).
The hemagglutinin clearly helps to determine the host range and tissue tropicity. We know a lot about the receptor specificity of influenza viruses: sialic acid which is bound in 2-3 linkage to galactose is preferentially present in avian cells and a 2-6 linkage, in which the sialic acid is bound to the six position of galactose, is the more common structure for receptors of human influenza viruses. Hemagglutinins from avian viruses thus preferentially recognize 2-3
sialic acid receptors and those from human viruses preferentially bind to 2-6 linkages. However, this specificity is not absolute, since most hosts possess cells which carry both receptors. Thus, an avian virus may bind cells in the human host which also carry 2-3 receptors. Furthermore, one (or only a few) amino acid changes may change an avian hemagglutinin into one which recognizes 2-6 sialic acid (human) receptors.
We understand that influenza virus proteins interact with signal transduction pathways such as the interferon pathway. A virus may be able to effectively block the interferon response in one species (and thus grow to high titers) but not do it well in another host species. Thus, many different factors come together to determine the transmissibility (from one species to the other) of influenza viruses.
Given this short introduction, we examined our first question: What further studies do we need to define the genetic loci important for virus transmission between species? Because the hemagglutinin is probably very important, surveillance of the receptor specificity of viruses is an important aspect of understanding viral transmission. But we also need to understand the receptors in the cell. As strange as it may sound to some colleagues, we still don't know exactly which cell protein or glycolipid is the best (the natural) receptor for influenza viruses. They must contain sialic acid, but which carbohydrate-containing glycoprotein or glycolipid is the “real” receptor is still not clear. Some of the specific cells we see in some quail and chicken may actually contain both 2-3 and 2-6 receptors, so one cell may actually be a mixing vessel (for the infection of a human and an avian virus).
Other important studies would look at the molecular changes associated with adaptation. Here we are referring to all of the genes, as they may all contribute to the properties of a virus. Except for the hemagglutinin and the interferon antagonist NS1, there is probably not a good reason to single out one gene over another. We will need to employ classic virologic methods in these studies to identify the gene(s) responsible for transmission, but sequencing will also be important. The NIH is pursuing an influenza virus genome sequencing project, as is the CDC and many other groups, and those studies will prove important in defining the genetic mutations contributing to transmissibility.
We need to use different animal models to try to understand transmission. Mice have been very helpful so far, but ferrets provide another model, and we should not forget about simple systems such as organ cultures, which can shed light on which cells become infected. We can now make influenza viruses that express a green fluorescing protein, so studying animal infections with these reporter viruses will be very important. We feel that it is critical to immediately initiate such studies, although some will be more long-term than others. Human organ culture experiments, for example, are certainly more easily performed than animal studies.
Our third question concerns what studies we need to do in order to define the environmental factors which contribute to virus transmission and how genetic factors weigh in. We clearly need more studies on the environmental survival of different strains. Different viruses may have different stabilities, and some may be transmitted more effectively than others. The duration of shedding may vary among viruses, and modes of transmission may also vary, extending beyond aerosol transmission. Dr. Kilbourne reminded us that the Balb/c mouse is an important animal system for answering some of these questions because it can be standardized from one lab to another. However, we should not forget that the human is basically the best animal model we have. Prospective clinical studies are long-term and expensive, and they require excellent laboratory support. However, human studies will be invaluable in answering questions such as: Are some patients super shedders of influenza viruses? Which influenza virus
strains transmit more easily from one patient to another? At the present time, we do not have enough data to answer such questions.
What studies can provide measures to predict intra-species changes in virus transmission? We will need multiple transmission models. Ferrets are obviously the most advanced model, but other models may also be useful in reducing spread. This aspect has not received much attention, but principles gleaned from intra-species transmission should help us understand inter-species transmission.
Our fifth question—concerning what studies we need to identify measures that can alter intra-species virus transmission, and the possible side effects or consequences of these measures—was probably the most hotly debated. Some colleagues felt that social controls among both animals and humans would be quite useful in reducing spread, while others felt that they would be less effective. One important measure in preventing viral spread is educating small farmers to minimize contact with birds and rely on certain techniques for raising these animals.
Hopefully, better and cheaper vaccines will become available. One consequence will clearly be the need to study whether antigenic changes of strains are selected by the widespread use of vaccination.
Our last question was: what studies are needed to determine whether transmission changes can be used to predict pandemic risk? We were not comfortable giving a definitive answer. One colleague suggested that we will find out only during the next pandemic. As a philosopher in New York (Yogi Berra) said, it's tough to make predictions, especially about the future.
DR. FINEBERG: I understand that Niels Bohr said something very similar, and it sounds so much more elegant coming from him than from Yogi Berra. But the sentiment is exactly right: prediction is always risky. On the other hand, if we do not make the effort, we certainly will not be prepared. The question is how to make the most cogent, effective, and promising effort.