
4
Prevention of Developmental Disabilities
The term developmental disabilities was introduced in the late 1960s to describe clinical disorders and diseases that cause disability, begin early in life, and require supportive services. This generic term covers a broad spectrum of impairments, ranging from mild to serious, and includes conditions characterized by mental retardation, cerebral palsy, epilepsy, and serious sensory impairment, as well as other childhood chronic illnesses associated with significant developmental delay.
In 1970 the term was given a narrower legal definition in Public Law 91-517 for the purposes of public planning and policy. This definition was subsequently altered and given its current form in the Developmental Disabilities Act of 1984 (P.L. 98-527). Here, Developmental Disabilities (using uppercase letters) were legally defined solely as severe, chronic conditions attributable to a mental or physical impairment, manifest before age 22, and likely to continue indefinitely, resulting in substantial limitations in a prescribed set of activities and requiring special interdisciplinary care. This restrictive definition generally has been interpreted to include only the most serious conditions.
This chapter will address developmental disabilities in the broader sense of the term, focusing on clinical disorders and diseases that can cause developmental delay. The concepts of prevention discussed here apply to all chronic health conditions that potentially can cause disability in childhood.
PUBLIC HEALTH SIGNIFICANCE
The scope of developmental disabilities is broad. An estimated 2 million to 4 million persons of all ages have such disabilities. The upper estimate is derived from the 1.7 percent prevalence rate in a study by Wistar and Vernon
(1986). The lower estimate is based on national survey data by LaPlante (1989a) and Sirrocco (1987). The two most common developmental disabilities, mental retardation and cerebral palsy, rank first and fifth as chronic conditions causing major activity limitation among persons of all ages (Table 4-1) (LaPlante, 1989a) and rank ninth and eighth, respectively, as conditions that create a need for assistance in carrying out basic life activities.
Disability years, a measure introduced by Houk and Thacker (1989), represents the number of years people survive with disabilities and thus provides an estimate of the public health impact of disability. By this measure, developmental and other childhood disabilities accounted for 35 percent of all disability years in 1986 (Table 4-2). This highlights the importance of preventing childhood disabilities, because significant gains in this area will have a ''multiplier effect," substantially decreasing the number of disability years.
The national costs of caring for children with developmental disabilities are substantial. Data from the 1980 National Medical Care Utilization and Expenditure Survey (NMCUES) indicate that children who experience limitations in normal activities use more medical services than other children, resulting in significantly higher health costs for this group (Newacheck and McManus, 1988).
Of an estimated total of $40.5 billion spent on health care for all children under the age of 21 in 1988 (based on updated 1980 National Medical Care Utilization and Expenditure Survey data), approximately $4.4 billion was spent on children with chronic disabling conditions. Thus an average of $1,406 was spent on each child with a chronic disabling condition, compared with an average of $487 for other children. Four percent of those under the age of 21 accounted for nearly 11 percent of total health care expenditures for that population (Newacheck and McManus, 1988). However, these cost figures underestimate the individual and total charges because of the significant changes in medical care costs and out-of-pocket expenditures since 1980.
A 1986 study of state, local, and federal government expenditures on institutionalization, income maintenance, and special education revealed combined spending of $16.5 billion in 1984, a 23 percent increase over 1979. These figures represent $7.28 billion in federal expenditures, $6.08 billion in state expenditures, and $3.12 billion in local expenditures (Braddock and Hemp, 1986).
The following section provides a descriptive epidemiology of developmental disability.
Epidemiology of Developmental Disabilities
Clinical disorders and diseases associated with developmental disability can be categorized by time of onset as follows: hereditary disorders, early
TABLE 4-1 Conditions with the Highest Risk of Disability, All Ages: United States, 1983-1986
|
Chronic Conditions |
Number of Conditions (thousands) |
Percent Causing Activity Limitation |
Rank |
Percent Causing Major Activity Limitation |
Rank |
Percent Causing Need for Help in Basic Life Activities |
Rank |
|
Mental retardation |
1,202 |
84.1 |
1 |
80.0 |
1 |
19.9 |
9 |
|
Absence of leg(s) |
289 |
83.3 |
2 |
73.1 |
2 |
39.0 |
2 |
|
Lung or bronchial cancer |
200 |
74.8 |
3 |
63.5 |
3 |
34.5 |
4 |
|
Multiple sclerosis |
171 |
70.6 |
4 |
63.3 |
4 |
40.7 |
1 |
|
Cerebral palsy |
274 |
69.7 |
5 |
62.2 |
5 |
22.8 |
8 |
|
Blind in both eyes |
396 |
64.5 |
6 |
58.8 |
6 |
38.1 |
3 |
|
Partial paralysis in extremity |
578 |
59.6 |
7 |
47.2 |
7 |
27.5 |
5 |
|
Other orthopedic impairments |
316 |
58.7 |
8 |
46.2 |
8 |
14.3a |
12 |
|
Complete paralysis in extremity |
617 |
52.7 |
9 |
45.5 |
9 |
26.1 |
6 |
|
Rheumatoid arthritis |
1,223 |
51.0 |
10 |
39.4 |
12 |
14.9 |
11 |
|
Intervertebral disk disorders |
3,987 |
48.7 |
11 |
38.2 |
14 |
5.3 |
— |
|
Paralysis in other sites (complete/partial) |
247 |
47.8 |
12 |
43.7 |
10 |
14.1a |
13 |
|
Other heart disease/disordersb |
4,708 |
46.9 |
13 |
35.1 |
15 |
13.6 |
14 |
|
Cancer of digestive sites |
228 |
45.3 |
14 |
40.3 |
11 |
15.9a |
10 |
|
Emphysema |
2,074 |
43.6 |
15 |
29.8 |
— |
9.6 |
15 |
|
Absence of arm(s)/hand(s) |
84 |
43.1 |
— |
39.0 |
13 |
4.1a |
— |
|
Cerebrovascular disease |
2,599 |
38.2 |
— |
33.3 |
— |
22.9 |
7 |
|
a Figure has low statistical reliability or precision (relative standard error exceeds 30 percent). b Heart failure (9.8 percent); valve disorders (15.3 percent); congenital disorders (15.0 percent); all other and ill-defined heart conditions (59.9 percent). SOURCE: LaPlante, 1989b. Reprinted with permission. |
|||||||
TABLE 4-2 Estimated Effect of Disability in the United States, in Terms of "Disability Years"
|
|
|
|
|
Years of Disability |
|
|
Age of Onset |
Number of Persons (millions) |
Percent of Persons with Disability |
Survival (years) |
Number (millions) |
Percent |
|
Birth-15 years |
5.6 |
20 |
50 |
280 |
35 |
|
16-34 years |
7.0 |
25 |
40 |
280 |
35 |
|
35-54 years |
6.4 |
23 |
25 |
161 |
20 |
|
55 years and older |
8.7 |
31 |
10 |
87 |
10 |
|
SOURCE: Houk and Thacker, 1989. |
|||||
alterations of embryonic development, late pregnancy or perinatal conditions, acquired childhood conditions, and conditions of unknown etiology. Table 4-3 presents these categories of origin, associated causes or pathologies, and some examples of conditions and their estimated prevalences in the United States. This is a slightly modified scheme from that of Crocker (1989) in that there is no category for environmental problems and behavioral syndromes; these have been primarily subsumed under the acquired childhood condition category. The following sections present general descriptions of these categories and some examples.
Hereditary Disorders
Some conditions originate prior to conception in the genotype of the parents. These conditions often have multiple somatic effects, but variation in expression is common as a result of single-gene interactions with other genic and environmental forces. The underlying causes or pathologies of these conditions are metabolic disorders, single-gene abnormalities, chromosome abnormalities, and polygenic familial syndromes.
Fragile X Syndrome Fragile X syndrome, a hereditary disorder caused by a chromosomal abnormality, is a common cause of mental retardation among males (Friedman and Howard-Peebles, 1986). Estimates of fragile X prevalence in males range from 0.5 to 0.9 per 1,000 (Blomquist et al., 1983; Froster-Iskenius et al., 1983; Herbst and Miller, 1980; Sutherland, 1982). Diagnosis is made by laboratory identification of the characteristic fragile site on the X chromosome or by inference from the pedigrees of affected family members.
TABLE 4-3 Category of Origin, Associated Cause/Pathology, and Examples (with Prevalence Estimates) for Developmental Disabilities
|
Category of Origin |
Cause/Pathology |
Examplesa (prevalence per 1,000) |
|
Hereditary |
Metabolic disorders |
Tay-Sachs disease (>0.01)1 |
|
|
|
Phenylketonuria (0.08)2 |
|
|
|
Maternal phenylketonuria (0.08)3 |
|
|
|
Congenital hypothyroidism (0.33)1 |
|
|
|
Hurler syndrome (0.01)2 |
|
|
Other single-gene abnormalities |
Neurofibromatosis (0.02)2 |
|
|
|
Tuberous sclerosis (0.6)4 |
|
|
|
Muscular dystrophy (0.02 - 0.10)4 |
|
|
Chromosomal abnormalities |
Fragile X syndrome (0.7)4 |
|
Early alterations of embryonic development |
Chromosomal changes |
Down syndrome (1.0)1 |
|
|
Intrauterine toxicity |
Fetal alcohol syndrome (1.4)1 |
|
|
|
Lead exposure toxicity |
|
|
Intrauterine infection |
Congenital rubella syndrome (<0.1)2 |
|
|
|
Congenital cytomegalovirus infections (3.0)2 |
|
|
|
Congenital syphilis (0.2)2 |
|
|
Structural malformations |
Absence of or shortened limbs (0.5)1 |
|
|
|
Hydrocephalus (1.8)1 |
|
|
|
Microcephalus (0.5)1 |
|
|
|
Spina bifida (0.4)1 |
|
Late pregnancy or perinatal conditions |
Premature birth |
Very low birthweight, < 1,500 grams (12)1 |
|
|
|
Central nervous system hemorrhage (6)5 |
|
|
|
Retrolental fibroplasia (0.07)2 |
|
|
Perinatal hypoxia |
5-minute Apgar < 4 (6)1 |
|
|
Infection |
Perinatally acquired human immunodeficiency virus infection (0.4)2 |
|
Acquired childhood conditions |
Postnatal infection |
Bacterial meningitis (0.8)2 |
|
|
|
Measles encephalopathy (<0.1)4 |
|
Category of Origin |
Cause/Pathology |
Examplesa (prevalence per 1,000) |
|
|
Childhood injury |
Spinal cord injury (0.04)6 (0.4)7 |
|
|
|
Traumatic brain injury (2.2)4 |
|
|
|
Near drowning (1.0)4 |
|
|
Environmental toxicity |
Lead encephalopathy (>0.1)4 |
|
|
|
Low-lead toxicity (not available)4 |
|
|
Psychosocial disadvantage |
Mental retardation of deprivational causes (3-5)4 |
|
Unknown |
|
Autism (0.4)4 |
|
|
|
Cerebral palsy (2-4)4 |
|
|
|
Epilepsy (3.5)4 |
|
|
|
Mental retardation of unknown cause (3-5)4 |
|
|
|
Learning disorders (50-100)4 |
|
a Superscript numbers indicate the age group used in determining the prevalence estimates, as follows: 1, at birth; 2, early childhood; 3, of all births; 4, childhood; 5, newborn period; 6, age 10; and 7, age 20. SOURCE: Adapted from Crocker, 1989. |
||
Early Alterations of Embryonic Development
Circumstances in early gestation can affect mitosis and embryogenesis. Generally, the resulting conditions are relatively stable after birth. The underlying causes or pathologies of these conditions are chromosomal changes, intrauterine toxicity, intrauterine infection, and structural malformation.
Fetal Alcohol Syndrome Fetal alcohol syndrome (FAS) is a condition caused by intrauterine toxicity. FAS is diagnosed when infants have characteristic dysmorphic features and when a history of maternal alcohol use in early pregnancy is determined. Infants with FAS have prenatal onset growth deficiency, facial abnormalities, and mental retardation. Congenital malformations, especially microcephaly, are common (Goodman and Gorlin, 1983; Smith, 1976). The national prevalence of FAS is estimated to be 1.4 per 1,000 live births. FAS rates among blacks are as much as six times higher than those for whites; among Native Americans the prevalence is 30 times greater (Chavez et al., 1988).
FAS is only one of a number of adverse outcomes associated with alcohol use in pregnancy. Mental retardation, in the absence of FAS, and learning disorders are other disabling conditions that become apparent in the school-age years (Streissguth et al., 1989).
The cause of mental retardation and learning disorders in children of women who use alcohol during pregnancy is often not clear. More study is needed to determine the contribution of maternal use of illicit drugs (especially cocaine)—often associated with heavy alcohol use—in the etiology of central nervous system impairment. Children of parents who use alcohol and illicit drugs have an increased risk for child abuse or neglect (Orme and Rimmer, 1981), which can also cause central nervous system impairment. Additional work is needed in the area of postnatal parental behavior that increases the vulnerability of this group of children.
Down Syndrome Children with Down syndrome, a condition caused by chromosomal changes, have a characteristic facies and almost always have mental retardation (Cicchetti and Sroufe, 1976; Dahle and McCollister, 1986). The presence of a third chromosome 21 is diagnostic for the condition. The risk of Down syndrome increases with the age of the mother from rates of less than 1 per 1,000 pregnancies among women in their twenties, to more than 10 in 1,000 among women over 40 years old (Hook and Lindsjo, 1978). In the United States today, the prevalence of the condition is 1 per 1,000 live births (Centers for Disease Control, 1988b), a decrease from the prevalence rates of more than 2 per 1,000 observed in earlier decades. Eighty-seven percent of children with Down syndrome survive to at least age 5 years; most deaths are due to heart malformations (Masaki et al., 1981). Persons with Down syndrome are at risk for developing hypothyroidism (Cutler et al., 1986) and instability of the neck (Van Dyke and Gahagan, 1988), as well as Alzheimer disease (Miniszek, 1983) for those living into their forties.
Late Pregnancy or Perinatal Conditions
During gestation and after morphogenesis, fetuses undergo a relatively long period of growth and development. If this growth period ends prematurely, the result is small, low-birthweight babies with increased vulnerabilities. The underlying causes of these conditions are prematurity, perinatal hypoxia, and infection.
Perinatally Acquired Human Immunodeficiency Virus Infection Data from the Centers for Disease Control (CDC) national serosurveys suggest an HIV seroprevalence rate of 1.5 per 1,000 among women delivering liveborn babies in the United States. Approximately one-third of these pregnancies
result in HIV infection of the infant as well. Thus, in 1990, between 1,500 and 2,000 infants (0.5 per 1,000 live births) are expected to develop perinatally acquired HIV infection.
The clinical course of HIV infection in children is varied. Belman and colleagues (1985) report that 90 percent of infants with HIV infection had central nervous system involvement including developmental delay, loss of developmental milestones, microcephaly, and encephalopathy.
Acquired Childhood Conditions
Many postnatal hazards can modify the body's development during childhood and do damage, from which varying degrees of recovery are possible. The underlying causes of these conditions are postnatal infection, childhood injury, environmental toxicity, and psychosocial disadvantage.
Traumatic Brain Injury It has been estimated that 2.2 per 1,000 children (birth through 19 years) each year have traumatic brain injury (Centers for Disease Control, 1990a). Approximately 40 per 1,000 persons sustain a traumatic brain injury in the first 19 years of life (based on annual age-specific rates). The major consequence of traumatic brain injury is death. Other outcomes such as intellectual, motor, and emotional/behavioral impairment have not been adequately studied. Existing data suggest that loss of consciousness and motor and sensory impairments are usually only short-term sequelae, but intellectual limitation, especially loss of memory and concentration, is an important long-term complication (Bruce, 1983; Klonoff et al., 1977; Lange-Cosack et al., 1979). It has also been reported that about a third of children who remained unconscious for more than one week had IQ scores less than 70. Some children, however, have long-term intellectual limitation/mental retardation after comas lasting only three to four days (Heiskanen and Kaste, 1974). However, Haas and colleagues (1987) report that 50 percent of persons with head injury had a record of poor academic performance before their injury.
Lead Toxicity Lead toxicity, an acquired childhood condition caused by environmental lead exposure, is the most common environmental disease of young children. Lead is a toxicant that affects every system in the body and is particularly harmful to the developing brain and nervous system. It has been estimated that in 1984, more than 3 million U.S. children (ages 6 months to 5 years) had lead levels high enough to cause clinical or subclinical effects (U.S. Department of Health and Human Services, 1988a). Children in the inner cities, who are already disadvantaged by poor nutrition and other factors, are particularly vulnerable.
Recent prospective studies have shown that adverse effects on the fetus and child probably begin at blood lead levels of 15 micrograms per deciliter (µg/dl) and below. These effects include decreases in IQ (Grant and Davis, 1989), delays in reaching developmental milestones (Bellinger et al., 1987; Vimpani et al., 1989), decreases in birthweight (Bornschein et al., 1989) and in postnatal stature (Schwartz et al., 1986), and shorter gestation (McMichael et al., 1986). There may be no threshold for some of the adverse effects of lead.
Conditions of Unknown Origin
There are a significant number of developmental disabilities for which the etiology remains obscure. These conditions include epilepsy, autism, and much cerebral palsy and mental retardation.
Cerebral Palsy Cerebral palsy (CP) is a group of disorders in which a disease of the brain causes impairment of motor function (Ingram, 1984). Although mobility limitation is the most common result of CP, coexisting mental retardation also occurs in about half of all cases (McDonald and Valmassey, 1987). In a review of CP prevalence studies in industrialized countries, Paneth and Kiely (1984) estimate that 2 per 1,000 school-aged children require services. About half of all occurrences of CP are associated with underlying prenatal conditions such as intrauterine infection, perinatal anoxia and maternal metabolic disease, and postnatal events such as trauma, infection, toxic exposure, and vascular problems. In the other half of CP cases, no underlying health problem can be identified.
There is a common misconception that most CP results from perinatal hypoxia. Blair and Stanley (1988) have shown that perinatal hypoxia was a possible cause of CP in less that 10 percent of children with the disorder.
Learning Disorders Learning disorders occur in persons who do not have mental retardation and include conditions such as hyperactivity and attention deficit disorder, along with specific "disabilities" of reading, writing, and mathematics. These learning disorders are usually not recognized until the child is academically challenged in school. A prevalence range of 50 to 100 per 1,000 children was found in studies reviewed in a 1987 report (U.S. Interagency Committee on Learning Disabilities, 1987). A few factors, such as very low birthweight (Calame et al., 1986; Nickel et al., 1982), fetal alcohol effects (Streissguth et al., 1989), low-lead-exposure syndrome (Needleman et al., 1990), and neurofibromatosis (Stine and Adams, 1989), are known to be associated with learning disorders, but in most cases the underlying cause is unknown.
There is both a need and a high potential for the prevention of developmental disabilities. The most readily preventable conditions include fetal alcohol syndrome, lead toxicity, many premature births, intrauterine and postnatal infection, and disabling conditions related to psychosocial disadvantage. Although more research is needed to improve interventions, current knowledge is adequate to warrant the expansion of existing prevention programs.
Employing the New Model
The terms impairment, functional limitation, disability, and handicap are commonly used to describe developmental disabilities. But their use has not been consistent, leading to some conceptual confusion. The committee's model of the disabling process (Figure 3-3) provides a new perspective for assessing and evaluating developmental disability. The model is useful in identifying similarities between developmental disabilities and other disabling conditions and in improving understanding of developmental disabilities as nonstatic disabling conditions. As a result, this model should facilitate the development of preventive interventions.
The clinical conditions described above correspond generally to the first two stages of the model of the disabling process, that is, pathology and impairment. Thus the prevalence of developmental disability does not equal the prevalence of functional limitation and disability according to the committee's model; other measures are needed to describe the prevalence of functional limitation and disability.
Functional limitations associated with developmental disabilities can be described as occurring in three categories: intellectual limitation/mental retardation, mobility limitations, and sensory and communication limitations. (Note that the committee's definition of functional limitation differs from that used in the Apt Associates report that provided terminology for federal legislation on developmental disabilities.) Examples of measurements that can be used for these categories of functional limitation appear below. It is important to note that functional limitations in childhood are caused not only by Developmental Disabilities but also by other potentially disabling conditions such as congenital heart defects, asthma, cystic fibrosis, and sickle cell anemia.
As described earlier, disability is the expression of a functional limitation in a social context, that is, a limitation in performing socially defined roles and tasks. Disability estimates can be made using activity limitation data (as measured by the National Health Interview Survey) and school-related limitation data (as measured by the use of special education services).
Functional Limitations
As noted above, developmental disabilities cause three major types of functional limitation: intellectual limitation/mental retardation, mobility limitation, and sensory and communication limitation. Some of the disabling conditions that can cause these functional limitations are discussed below. Monitoring their prevalence, in relation to the categories of origin, should be useful in developing intervention strategies and evaluating their effectiveness.
Intellectual Limitation/Mental Retardation Mental retardation (MR) is often divided into two categories: serious MR (IQ of less than 50) and mild MR (IQ 50 to 70). Serious MR is more likely than mild MR to be associated with discernible pathology. Susser and colleagues (1985) cite a range of reported prevalence for serious MR between 2.9 and 3.5 per 1,000 children. In the studies they examined, about 35 percent of the serious MR was associated with chromosomal changes, between 15 and 20 percent with late pregnancy or perinatal conditions, and between 15 and 25 percent of unknown causes (Figure 4-1).
Children reared in psychosocially disadvantaged family settings are at greater risk for MR (Butler et al., 1984; Broman et al., 1987; Shonkoff, 1982), but the relationship between socioeconomic risk and mental retardation is complex and not well understood. Subtle neurological abnormalities and minor obstetrical risk factors (Zigler and Cascione, 1984) are thought not to be sufficient cause (Breitmayer and Ramey, 1986).
Comprehensive day care programs have been developed in response to observed differences between homes with and without psychosocial disadvantage (Ramey and Campbell, 1984). A 13-point improvement in IQ scores of low-birthweight children has been reported in a recent trial of such programs (Infant Health and Development Program, 1990).
Mobility Limitation The prevalence of mobility limitation among children under 18 years of age was 1.5 per 1,000 (LaPlante, 1989b). Walker and colleagues (1988) studied the underlying health conditions of children using crutches and wheelchairs and reported that 43 percent have cerebral palsy, 12 percent have spina bifida, and 8 percent have muscular dystrophy (Figure 4-1). Prevalence estimates for these disorders are 2 per 1,000 for cerebral palsy (Kudrjavcev et al., 1983), 0.4 per 1,000 for spina bifida (Centers for Disease Control, 1988b), and between 0.02 and 0.1 per 1,000 for muscular dystrophy (Gardner-Medwin and Sharples, 1989; Tangsrud and Halvorsen, 1989).
Sensory and Communication Limitation A range of prevalence between 0.93 and 2.3 per 1,000 has been reported for childhood hearing impairments
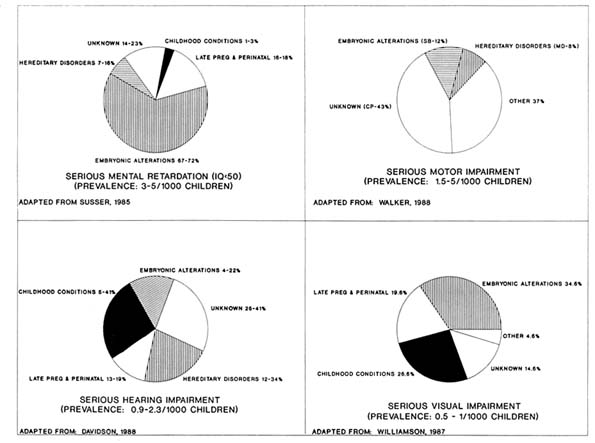
(Figure 4-1) (Davidson et al., 1988). Hereditary and other prenatal causes accounted for between 31 and 52 percent of all hearing limitation; late pregnancy and perinatal causes for between 13 and 19 percent; and postnatal causes for between 5 and 41 percent. The underlying disorder (cause/pathology) was unknown in between 25 and 41 percent of the subjects.
In a population-based study of infants and toddlers, Williamson and colleagues reported that 1 child per 1,000 under age three had a severe vision impairment that could not be corrected (Figure 4-1) (Williamson et al., 1987). Twenty-five percent of these cases were attributable to prenatal disorders, 20 percent to late pregnancy/perinatal conditions, and 25 percent to postnatal infection or injury. The cause was unknown in 15 percent of the cases.
Multiple Impairments and Functional Limitations A person who has a serious impairment that causes functional limitation in one area may have additional impairments causing other functional limitations. For example, a child with mental retardation may also have mobility limitations caused by cerebral palsy. About two-thirds of all children with developmental disabilities have more than one clinical disorder. Of children with mental retardation, 10 percent have cerebral palsy (and mobility limitation), 3 percent have serious hearing impairment, 1 percent have visual loss, and 40 percent have emotional or behavioral disorders (Accardo and Capute, 1979). Children with more serious mental retardation are more likely to have additional functional limitations.
Disability
At least two survey indicators are useful in determining childhood disability: activity limitation (measured in the National Health Interview Survey) and use of special education services (measured by public education agencies). Based on the 1983-1985 National Health Interview Surveys, 40.2 children per 1,000 aged 5 through 17 were limited in their major activities (LaPlante, 1988). The prevalence of children who needed help to carry out activities of daily living (ADL) was 3.3 per 1,000. Of the 15 per 1,000 children aged 5 through 17 who were found to have mental retardation, 90 percent (13 per 1,000) were limited in their major activity (school), and 6 percent (0.9 per 1,000) needed help in ADLs. Of the 2.4 per 1,000 children who had cerebral palsy, 74 percent (1.8 per 1,000) had activity limitations, and 13 percent (0.3 per 1,000) needed help in ADLs. Children with mental retardation and cerebral palsy accounted for 26 and 10 percent, respectively, of all children needing help in ADLs.
The prevalence of children aged 3 through 21 who received special educational services in 1987-1988 was 66 per 1,000 (U.S. Department of
Education, 1989b). Forty-seven percent of these children were categorized as learning disabled, a prevalence of 31 per 1,000 children. Fourteen percent were labeled mentally retarded, a prevalence of 9.6 per 1,000 children.
Secondary Conditions
When more than one potentially disabling condition is present in the same individual, it is important to determine whether the conditions had different origins or whether one led to the other. This distinction has important implications for prevention. If one condition, such as mobility limitation, is an antecedent to another, such as decubitus ulcers, then elucidating the causal mechanism can help to identify effective interventions to prevent development of the secondary condition. In children with cerebral palsy and mobility limitations, for example, muscle contractures that further limit mobility are secondary conditions and can be prevented. Data are limited, however, on secondary conditions, and it is often difficult to differentiate between dependent and independent conditions. The Centers for Disease Control (CDC) is attempting to identify and classify preventable secondary conditions associated with cerebral palsy. Five types have been tentatively identified: neuromusculoskeletal, health maintenance, psychosocial, communication, and quality of life (see Table 4-4) (M. Pavin, Centers for Disease Control, personal communication, 1990).
An improved understanding of the relationships that exist between clinical conditions and the model for the disabling process is needed to facilitate the development and evaluation of improved intervention strategies. Prevalence data on functional limitations and disabilities need to be evaluated in relation to the categories of origin of developmental disability, the progression in the disabling process, and the interactions with risk factors and quality of life. Research should include assessments of risks associated with socioeconomic and psychosocial disadvantage, the effectiveness of habilitative services, and the identification of secondary conditions.
APPROACHES TO PREVENTION
The development of successful prevention strategies in recent decades is illustrated by the history of the prevention of kernicterus and cerebral palsy from Rh hemolytic disease. Prior to the Second World War, there was virtually no understanding of the cause of the hemolytic anemia and severe jaundice that produced some cases of cerebral palsy. Progress in understanding blood types during the war led to the discovery that the hemolytic anemia was caused by a genetic incompatibility between the mother and the
TABLE 4-4 Secondary Conditions, Their Associated Risk Factors, and Interventions in Persons with Cerebral Palsy
|
Secondary Condition |
Risk Factors |
Recommended Interventions |
|
Neuromusculoskeletal |
|
|
|
Deformities of hip, knee, spine |
Poor positioning |
Range of motion exercises; positioning; wheelchair type |
|
Falls |
Deconditioning |
Treatment selection that recognizes short- and long-term consequences |
|
Health maintenance |
|
|
|
Respiratory problems |
Dysphagia |
Food selection; oral/swallowing therapy |
|
Skin breakdown |
Compromised skin integrity |
Nutrition, positioning |
|
Psychosocial |
|
|
|
Low self-esteem, depression |
Inadequate modes of communication; limited community integration |
Augmentive communication devices; access and training; peer interaction at all ages |
|
Limited communication |
Unintelligible expressive language |
Speech and language skills therapy; use of augmentive communication devices; access and training |
|
Quality of life—limited integration, independence, and productivity |
Lack of employment opportunities; lack of community access (e.g., inadequate transportation and architectural barriers) |
Supported employment; community education policy; legislation and regulation |
fetus. Subsequently, exchange transfusions after birth became a common procedure to prevent toxic brain effects that caused cerebral palsy.
The late 1960s and early 1970s saw further advances in the prevention of hemolytic anemia that resulted from several factors: an understanding of the biology of blood types, the development and use of an Rh immune globulin, and a change in reproductive patterns (women began to have fewer babies). The condition is now virtually eliminated. Thus the battle against this genetically caused developmental disability has progressed from treating a condition to prevent the impairment to preventing the underlying pathology.
Many types of interventions reduce the incidence of potentially disabling conditions among infants and children. As seen in Table 4-5, genetic interventions are the prime method when the underlying condition is a hereditary
disorder. Immunization and avoidance of prenatal toxic exposures are important measures to prevent early alterations in embryonic development. Programs that reduce the rate of prematurity prevent some disabling conditions associated with the perinatal category of origins. Medical care, injury control, and family support services are examples of interventions to reduce disabling conditions associated with acquired childhood conditions. The types of interventions are ranked in three categories according to their effectiveness: those proven to be effective (such as immunizations to prevent congenital rubella); those showing promise (such as prenatal care to prevent prematurity); and those requiring further research (such as periconceptional multivitamin supplementation).
Effective secondary preventive strategies include corrective surgery for congenital anomalies, newborn metabolic screening, early detection of serious hearing impairment, and habilitation to reduce limitations in communication. Tertiary prevention includes habilitation, peer support, and prevention of secondary conditions in persons with existing disabilities.
Preventive interventions can be grouped into four general categories: health care, education, environmental control and adaptive assistance, and peer support. Some examples of each of these categories are presented below.
Health Care Interventions
Health care before pregnancy (preconception care) can ameliorate disease, improve risk status, and help prepare a family for childbearing (Institute of Medicine, 1988c). The components of preconception care include health promotion activities and interventions to reduce risk. Such care for women with known medical conditions may prevent anomalies or illnesses in the newborn. A discussion of other health care interventions follows.
Prenatal and Well-Child Care
Preventive interventions have been developed for normal health care practices in pregnancy, during the prenatal and perinatal periods, and during childhood. Recommendations on the content of such programs, including specific risk assessment and health promotion activities, have been developed by the Institute of Medicine (1985) and the U.S. Public Health Service (1989), among others. Risk assessment is done by evaluating an individual's medical history and conducting a physical examination. Pertinent elements of history, such as prematurity in a previous pregnancy or genetic disease in a family member, can be indications for special care. During the physical examination, blood pressure, weight gain, and pelvimetry findings can also signal the need for intervention.
TABLE 4-5 Known Risk Factors and Types of Interventions That Reduce the Incidence and Severity of Certain Conditions
|
Condition |
Risk Factor |
Type of Intervention |
|
HEREDITARY DISORDERS |
||
|
Metabolic disorders |
|
|
|
Maternal phenylketonuria |
Maternal diet |
Program to inform young women with phenylketonuria of preventive dieta |
|
Hurler syndrome |
Family history Laboratory marker |
Genetic interventionsb |
|
Tay-Sachs disease |
Family history Laboratory marker |
|
|
|
Ashkenazi Jews |
|
|
Other single-gene abnormalities |
|
|
|
Muscular dystrophy |
Family history Laboratory marker |
Genetic interventionsa |
|
Cystic fibrosis |
Family history Laboratory marker |
Genetic interventionsa |
|
Sickle cell anemia |
Family history Laboratory marker |
Genetic interventionsb |
|
Hemophilia |
Family history Laboratory marker |
Genetic interventionsb |
|
Chromosomal abnormalities |
|
|
|
Fragile X syndrome |
Family history Laboratory marker |
Genetic interventionsa |
|
|
|
Population screening and pregnancy planningc |
|
EARLY ALTERATIONS OF EMBRYONIC DEVELOPMENT |
||
|
Chromosomal changes |
|
|
|
Down syndrome |
Maternal age Laboratory markers |
Genetic interventionsb |
|
Toxic exposure syndromes |
|
|
|
Fetal alcohol syndrome |
Maternal alcohol use |
Parenting supportsa |
|
|
|
Child placementa |
|
|
|
Family planninga |
|
|
|
Addiction treatment programsa |
|
Kernicterus |
Rh hemolytic disease |
Rh immune globulinb |
|
Condition |
Risk Factor |
Type of Intervention |
|
Accutane embryopathy |
Maternal exposure |
Labeling and patient informationa |
|
|
|
Counselinga |
|
Intrauterine infection |
|
|
|
Congenital rubella syndromes |
Rubella exposure |
Immunizationb |
|
Congenital syphilis |
Maternal infection |
Prenatal detection and maternal treatmentb |
|
Congenital malformations |
|
|
|
All types |
Maternal diabetes |
Prenatal medical managementa |
|
Spina bifida |
Family history Laboratory marker |
Genetic interventionsb |
|
|
No maternal vitamin use |
Periconceptional vitamin supplementationc |
|
LATE PREGNANCY AND PERINATAL CONDITIONS |
||
|
Premature birth |
Lack of prenatal care |
Prenatal carea |
|
|
Adolescent pregnancy |
Adolescent pregnancy prevention programsa |
|
Perinatal hypoxia |
High-risk pregnancy |
Prenatal carea |
|
|
|
Tertiary perinatal carea |
|
Infection |
|
|
|
Perinatally acquired HIV infection |
Maternal infection |
Counselingb |
|
Congenital herpes |
Maternal infection |
Family planninga |
|
|
|
Cesarean deliverya |
|
ACQUIRED CHILDHOOD CONDITIONS |
||
|
Postnatal infection |
|
|
|
Bacterial meningitis |
HFlu immunity |
Immunizationa |
|
Poliomyelitis |
Immune status |
Immunizationb |
|
Measles encephalopathy |
Immune status |
Immunizationb |
|
Mumps encephalopathy |
Immune status |
Immunizationb |
|
Childhood injury |
|
|
|
Unintentional head trauma and spinal cord injury |
Seat belts and child safety seats |
Child safety seat legislationb |
|
Condition |
Risk Factor |
Type of Intervention |
|
|
|
Child safety seat programsa |
|
|
Motorcycle helmets |
Helmet legislationb |
|
|
Bicycle helmets |
Bicycle helmet programsa |
|
|
Unsafe diving |
Health educationa |
|
|
Playground hazards |
Surface modificationb |
|
Child abuse (physical) |
Family history of violence |
|
|
|
Impoverished family environment |
See deprivational syndromes below |
|
|
Parental alcohol and drug addiction |
Addiction treatment programsa |
|
|
Adolescent parents |
Adolescent pregnancy prevention programsa |
|
|
Childhood disability for all above risks |
Respite carea |
|
Near drowning |
Unsupervised swimming |
Health educationa |
|
|
Unfenced home pools |
Local ordinancesa |
|
|
No caretaker CPR skills |
CPR training programsa |
|
Burns |
Hot water temperature |
Health educationa |
|
|
|
Local ordinancesa |
|
Environmental toxicity |
|
|
|
Lead exposure toxicity |
Environmental lead in paint, dust, and air |
Abatement in housinga |
|
|
|
Low-lead gasolinesa |
|
|
|
Lead-free paintsa |
|
|
|
Protection in workplaceb |
|
Deprivational syndromes |
Impoverished family environment |
Head Startb |
|
|
|
Comprehensive day carea |
|
|
|
Food supplementation for women and childrena |
|
|
|
Housing programsa |
|
|
|
Social servicesa |
|
a Interventions that are promising and should be implemented, but that should also be monitored closely and evaluated. b Interventions that have been proven effective and that should be implemented and monitored. c Interventions that require further research. |
||
Guidelines on preventive measures in labor and delivery procedures, infection control in nurseries, and other areas have been issued by the American Academy of Pediatrics and the American College of Obstetricians and Gynecologists (Frigoletto and Little, 1988). A recent report by the U.S. Preventive Services Task Force (U.S. Department of Health and Human Services, 1989a) also includes sections on care during the prenatal period, at birth, and during childhood.
There is a need to increase the use of preventive measures in prenatal care and well-child care. This could be accomplished by increasing public awareness of the need for family planning and prenatal care and by ensuring that every child who has, or is at risk of developing, a developmental disability has access to continuous, comprehensive preventive and acute health services.
Genetic Interventions
Major advances in genetic screening during the past 20 years have allowed families and physicians to recognize hereditary and other genetic disorders at very early stages, thereby facilitating preventive and treatment decisions for patients earlier in the course of the condition. During the next decade, genetic interventions are likely to play a major role in reducing the incidence and severity of developmental disabilities.
Genetic screening has reduced the birth incidence of Down syndrome, other chromosomal aberrations, and inborn errors of metabolism such as Tay-Sachs disease. The success of these interventions highlights the responsibility of health care providers to counsel potential parents about test results and discuss with them a range of possible options. Some tests can give a definitive diagnosis for a disease, whereas others, such as maternal serum alpha-fetoprotein screening, can give only an indication of risk. Clinicians must be able to provide sufficient detail about risk and therapy to provide couples with a range of reproductive options. In certain circumstances, the availability of pregnancy termination may be an important option to some parents. It is important to note, however, that this option in health care delivery does not prevent the occurrence of disabling conditions—only their birth incidence.
Continued success with genetic technology opens the way for rapid gains in carrier screening for hundreds of genetic diseases known to cause developmental disabilities, and probably for the many genetic diseases that are yet to be discovered as causes of developmental disabilities. Understanding the genetic basis for these diseases may one day lead to primary prevention or true cures through gene therapy.
Newborn screening for metabolic conditions also shows promising developments for secondary prevention. For example, genetic technology is currently
used to identify children who will develop mental retardation upon exposure to phenylalanine. The next decade is likely to see a growing list of conditions that are caused by susceptibility of the rare individual to common environmental exposures. Interventions will be developed to provide early identification and appropriate avoidance of exposures.
Genetic interventions, as part of preconception counseling and prenatal care, can play a major role in reducing the birth incidence of disabling conditions. Genetic screening and counseling, with associated services, should be accessible to all who choose to use them. Using sensitivity and care, physicians should discuss all possible interventions with prospective parents.
Multidisciplinary Care
A 1987 report by the U.S. surgeon general emphasized that health care for children with disabling conditions should be delivered in a family-centered, community-based system. The Association for the Care of Children's Health and the Maternal and Child Health Bureau have developed specific recommendations to ensure that health care delivery is flexible, accessible, and responsive to family needs (Shelton et al., 1987). Moreover, parents should be involved in all health care decision making, and physical therapists, speech therapists, orthopedic surgeons, and other involved health professionals should coordinate the delivery of care.
State systems of services for children with, or at risk of developing, chronic and disabling conditions must be expanded to provide adequate multidisciplinary care for the prevention of developmental disabilities and associated secondary conditions.
Education
Head Start and Comprehensive Day Care
Head Start programs are designed to provide educational opportunities to three- and four-year-old children from low-income families (Barnett, 1985; Lazar et al., 1982). Children in Head Start programs are better prepared for school, demonstrate less need for special education, and have less chance of being retained in a grade. Success in school was associated with lower rates of delinquency, teenage pregnancy, and welfare usage, and with higher rates of high school completion and employment.
Comprehensive day care programs for disadvantaged children younger than age three also show promise. The Infant Health and Development Program
(1990) reported that such programs improved the developmental outcomes of low-birthweight and premature infants. Infants from one to three years old who were assigned to the intervention, which included attending a child development center five days a week, showed improved IQ scores.
Positive effects from these programs are possible if they are adequately funded and staffed with well-trained, competent teachers (U.S. Department of Health and Human Services, 1985; Schweinhart and Weikart, 1986).
Head Start and comprehensive day care programs have been shown to be effective interventions in reducing the incidence of school failure. Early educational interventions should continue to be implemented but should be evaluated further.
Community Educational Priorities
Communities can promote prevention in a broad variety of settings, such as clinics in public schools. Community leaders also have successfully used public school curricula, newspapers and other media, churches, and the business sector to promote information in priority areas. Health promotion and disease prevention education should be an integral part of the curriculum in public schools and should include the rationale for preventive measures such as immunization and newborn metabolic screening.
Recent efforts to evaluate the effectiveness of school-based health education will enhance the quality of the prevention science base (Kolbe, 1986), and the National Cancer Institute's program to assess the impact of school curricula on student health behavior provides a useful model for evaluating prevention in the developmental disabilities area. In addition, several of the Health Objectives for the Year 2000 (U.S. Department of Health and Human Services, 1990) focus on increasing instruction in specific prevention activities. Many of these objectives are relevant to developmental disabilities prevention.
The effectiveness of school-based programs in health education should be reviewed and improved as necessary to educate children about prevention including the prevention of disability.
Access to Public Education
Landmark 1975 legislation (P.L. 94-142) mandated the education of children with disabilities in the least restrictive environments and required the provision of special education services to make school completion possible. Although there is considerable variability in placement policies among school districts, on average, 27 percent of ''students with handicaps" were placed
in regular classrooms in 1986-1987 (U.S. Department of Education, 1989b). Special resource rooms were provided for another 43 percent, 25 percent were placed in separate classes, and 4 percent were placed in separate schools. Less than 2 percent of special educational services were provided in homes, hospitals, residential facilities, or correctional facilities.
Sixty percent of "handicapped students" aged 16 to 21 graduated with a diploma or certificate. Twenty-five percent dropped out. The highest dropout rates were reported among the "emotionally disturbed" (42 percent) and the "learning disabled" (26 percent) (U.S. Department of Education, 1989a).
In 1986, amendments to the 1975 legislation (P.L. 99-457) encouraged states to identify children with disabling conditions as early as possible and provide early intervention services (Smith, 1976; DeGraw et al., 1988). States are now discussing how to implement these programs.
Environmental Interventions
Environmental Control
Environmental control programs are designed to protect children from exposure to toxicants such as lead and asbestos. With respect to lead, prevention strategies focus on efforts to identify major environmental sources of lead exposure (such as house paint, automobile emissions, and water) and to identify children with elevated blood levels of lead (Centers for Disease Control, 1985). Federal, state, and local regulations are directed at keeping environmental exposures at safe levels.
Childhood lead exposure is an important cause of preventable developmental disability, and screening programs in high-risk areas should be expanded. Surveillance also should be established to monitor childhood lead poisoning more closely, and governmental health, housing, and environmental agencies should work together to increase the removal of lead paint and dust in high-risk areas.
Accessibility and Adaptation
Methods of adaptive assistance that reduce secondary conditions are evolving, including personal care attendants, respite care, and a vast array of assistive technology. Communication devices, feeder plates, computers, and electric wheelchairs are among the most widely used assistive technologies, but devices also can be customized for individuals with unique needs. The impact of some environmental obstacles, such as curbs and buildings, has been lessened, but many obstacles remain, including inadequate transportation in rural areas.
Environmental modification and adaptive assistance are essential components of a prevention program focused on developmental disability.
Peer Support Groups
Organizations such as local Parent to Parent groups, Associations of Retarded Citizens groups, United Cerebral Palsy Associations, and Independent Living Centers provide community-based peer support for individuals with disabling conditions and their families. These groups provide an invaluable resource for emotional support and information. For example, support groups are the major source of referrals to professionals who specialize in care for persons with disabling conditions, and to systems of health care reimbursement. In addition, support groups are excellent sources of advice on career alternatives, training, and job opportunities.
Peer support groups also play a major advocacy role. Through the concerted efforts of several such groups, legislation has been adopted to improve access to public buildings and transportation. These groups also have been instrumental in developing many state-based disability prevention programs.
Persons with disabling conditions, their families, personal attendants, and advocates need improved access to information and training in disability prevention. In particular, there is a need for enhanced disability advocacy, information, and support in many rural communities where physical distances limit group interactions.
OPPORTUNITIES AND NEEDS
Current efforts in the prevention of developmental disabilities as described above provide numerous opportunities. There is much room for improvement, however. Some of the opportunities and needs that have been identified are described below, organized into five categories: organization and coordination, surveillance and epidemiology, research, access to care and preventive services, and professional education.
Organization and Coordination
The vast array of disability-related activities in both the public and private sectors is evidence in itself of the need for coordination. There are numerous examples of duplicate and underutilized services. Efforts are under way at national and state levels to better coordinate prevention programs. Some of these are briefly described below.
National Coordination
National Council on Disability The National Council on Disability is a presidentially appointed council that has made prevention of disability one of its highest priorities. Its efforts include promoting the development of a national disabilities prevention plan. In addition, the council has worked with the Office of Disease Prevention and Health Promotion to cosponsor a federal task force to coordinate disability prevention planning.
The National Coalition for the Prevention of Mental Retardation The National Coalition for the Prevention of Mental Retardation comprises representatives from the President's Committee on Mental Retardation, the American Academy of Pediatrics, the American Association on Mental Retardation, the Association for Retarded Citizens of the United States, and the American Association of University Affiliated Programs. This group meets regularly to discuss major activities in the area of developmental disabilities prevention.
The Office of Disease Prevention and Health Promotion In coordinating the development of the Health Objectives for the Year 2000 (U.S. Department of Health and Human Services, 1990), the Office of Disease Prevention and Health Promotion has promoted objectives that address disability prevention. These objectives will prescribe measurable improvements in health status, risk factor reduction, health education, and preventive services related to the prevention of disabilities.
State-based Coordination
States that accept planning money under federal legislation (P.L. 99-457) must establish interagency coordinating councils. Under the direction of a state agency (usually the department of education or health), representatives of state government divisions dealing with childhood disability interventions must meet regularly to discuss the design of intended service programs.
A new systematic approach to the prevention of developmental disabilities has been launched under recent federal legislation (P.L. 100-102). This approach involves cooperative agreements between the CDC and the respective states to develop coordinated state disability prevention programs. A major goal of this effort is to develop a scientific data base on incidence, prevalence, and relative effectiveness of intervention strategies.
The many disability-related activities in the public (federal, state, and local levels) and private sectors need to be coordinated with additional emphasis on prevention.
Surveillance and Epidemiology
The creation of effective preventive measures requires an informed analysis of data on the types and prevalences of disabling conditions and their underlying conditions. Surveillance data on younger children can be used to estimate their potential needs in subsequent years. Surveillance data also provide the basis for epidemiologic research to evaluate preventive measures and to discover more causes of developmental disabilities. Analysis of community-and state-based surveillance data can provide the basis for etiologic research (Thacker and Berkelman, 1988). The systematic collection of surveillance data should always be examined with the goal of spreading knowledge about the availability of health services. Several sources of nationally published data are described below to illustrate the variety of available data and the need to coordinate data collection and analysis.
Centers for Disease Control
CDC has an established program in epidemiologic research and birth defects surveillance and is building on this experience to study other developmental disabilities such as mental retardation and cerebral palsy. The birth defects surveillance program has two elements: the Metropolitan Atlanta Congenital Defects Program (MACDP), and the national Birth Defects Monitoring Program (BDMP). Developmental disabilities are being studied in the Metropolitan Atlanta Developmental Disability Study (MADDS).
Metropolitan Atlanta Congenital Defects Program MACDP is a population-based active surveillance program in metropolitan Atlanta designed to provide reliable prevalence estimates of several hundred types of birth defects. Because many prevention programs and environmental agents that exist in Atlanta are also found throughout the country, this program has served as a source of data for national policy decisions.
Reports based on MACDP data have shown no increased risks for birth defects associated with maternal Bendectin exposure (Cordero et al., 1981) or with paternal opportunity for exposure to Agent Orange (Erickson et al., 1984). Another study showed that women who took multivitamin supplements prior to pregnancy were only half as likely as unsupplemented women to have an infant with spina bifida (Mulinare et al., 1988).
Birth Defects Monitoring Program The BDMP provides a national perspective on birth defects, using hospital discharge diagnoses from large numbers of hospitals. Comparison of BDMP birth defect rates with those obtained from MACDP is helpful in interpreting national findings and monitoring trends over time. Patterns discerned from these data include decreasing trends of anencephaly and spina bifida (Edmonds and Windham, 1985) and
increasing trends in renal agencies and ventricular septal defect (Centers for Disease Control, 1988b).
These and other data gained from birth defects surveillance programs potentially can be used to inform eligible families of the availability of clinical services. Iowa and Colorado are investigating the feasibility of using surveillance data to refer families to early intervention programs.
Metropolitan Atlanta Developmental Disabilities Study Birth defects are a major component of developmental disabilities and are easier to ascertain on a population basis than are non-birth defect developmental disabilities. Surveillance methods are now being developed in this more difficult area. MADDS is a prevalence survey of five developmental disabilities (mental retardation, cerebral palsy, severe hearing and vision impairments, and seizure disorders) in metropolitan Atlanta. In addition, cases and controls are being studied to search for causes.
There is a need for a national surveillance system to monitor the incidence and prevalence of developmental disabilities. The CDC surveillance systems for birth defects and developmental disabilities represent an important base from which to develop this capacity.
National Center for Health Statistics
In addition to its birth defects and developmental disabilities surveillance efforts, the CDC has several other programs for collecting information on health status. These programs, directed by the National Center for Health Statistics (NCHS), which also compiles vital statistics data, can be a rich source of information on disability. The most important of the NCHS surveillance efforts are the National Health Interview Survey (NHIS), the 1980 National Medical Care Utilization and Expenditure Survey (NMCUES), the National Maternal and Infant Health Survey, and the National Health and Nutrition Examination Surveys (NHANES).
National Health Interview Survey The NHIS has been conducted annually since 1957, with approximately 50,000 households providing information in a personal interview. A core questionnaire solicits data on perceived health status, limitation of activity, disability days, the incidence of acute conditions, prevalence of selected chronic conditions, and health care utilization. Conditions such as mental retardation, cerebral palsy and sensory impairment are included in the core data, but no information on underlying clinical disorders is gathered. A Child Health Supplement to the NHIS, added in 1981 and 1988, solicits information on childhood conditions.
1980 National Medical Care Utilization and Expenditure Survey NMCUES was a 1980 study that collected data on disability, health status, acute and
chronic conditions, use of health services, and source of expenditures from 17,000 noninstitutionalized civilians. NMCUES was replicated, in part, by the 1987 National Medical Care Expenditures Survey conducted by the National Center for Health Services Research.
National Maternal and Infant Health Survey Ten thousand mothers of liveborn babies were interviewed in this 1988 survey. A longitudinal follow-up study of this group is planned in 1990. This study will help establish expected distributions of health status measures, but the sample size will not allow adequate statistical description of individual developmental disabilities.
National Health and Nutrition Examination Surveys Data on hearing, vision, and intelligence were collected in three cycles of NHANES studies beginning in 1971, providing another source of normal descriptive data. The samples studied in NHANES I, NHANES II, and Hispanic HANES were approximately 20,000 (1971-1974), 20,000 (1976-1980), and 12,000 (1982-1984), respectively.
National Institutes of Health
National Institute of Child Health and Human Development NICHD, part of the National Institutes of Health (NIH), has supported research on the genetic and environmental causes of mental retardation, autism, epilepsy, and cerebral palsy (National Institutes of Health, 1989). NICHD-funded investigators in 12 mental retardation research centers carry out biomedical and behavioral studies of these issues. Biomedical research has focused on applications of new genetic approaches to investigate a variety of developmental disabilities. NICHD Mental Retardation Research Centers have also provided a setting for longitudinal studies of environmental and social factors, along with research on secondary conditions and quality of life issues. NICHD also houses the new National Center for Medical Rehabilitation Research (see Chapter 8).
National Institute of Neurological Disorders and Stroke Another branch of NIH, NINDS funds biomedical research on brain development during infancy and childhood and on disorders that influence cognition, learning, behavior, and performance (NIH, 1989). NINDS-supported investigators study conditions that damage the central nervous system early in life and contribute to mental retardation.
Bureau of Maternal and Child Health and Resources Development
To complement their health service delivery program, the Health Resource Services Administration's BMCHRD administers a grant program
for research (BMCHRD, 1989). These grants support a broad spectrum of studies, ranging from descriptive epidemiology to evaluation of major preventive interventions. Evaluation of interventions to reduce the incidence and severity of secondary conditions is also a priority in the BMCHRD research program.
Department of Education
National Institute on Disability and Rehabilitation Research The NIDRR administers two grant programs: one to support research and training centers, and a second to promote individual research. The research and training centers, which are principally university based, recently have focused on the identification and treatment of secondary conditions. The NIDRR is also promoting the development of assistive technology and is cofunding (with the National Institute of Mental Health) a study of service systems used by children with emotional disorders.
Office of Special Education Programs The U.S. Department of Education supports research activities on the effectiveness of special education and publishes annual data on the use of special educational services. The State/Federal Evaluations Studies Program funds studies of the effectiveness of programs implemented under the Education of the Handicapped Act.
The Department of Education publishes special education statistics in an annual report to Congress. Use of services is categorized by type of impairment (e.g., mental retardation, learning disorders, hearing and visual impairment). National data are difficult to interpret because case definitions may vary greatly among local school districts.
State- and Local-level Data Bases
Disability data are collected at the state and local level by a number of health and education agencies. Some states have begun interagency collaboration to share data to improve planning and inform families of available services. For the most part, however, data are used only within the agency that collected them.
There is a great potential for increasing the applications of these data for both service and research purposes. More complete discussions of these varied data sets are provided by Gortmaker and Walker (1984) and by Crocker (1986) in his widely used unpublished article, "Data Collection for the Evaluation of Mental Retardation Prevention Activities: The Fateful Forty-three."
Birth and death records are usually maintained by the state health agency. The number of annual births, by state and region, is often used with established prevalence rates to calculate the expected number of persons with specific potentially disabling conditions. Such synthetic estimates can provide a basis for evaluating the comprehensiveness of service programs.
State- and local-level data can provide the foundation for epidemiologic research in selected regions. National surveillance for developmental disabilities could benefit from such epidemiologic research.
Other Important Data Bases on Developmental Disabilities
Several other valuable data bases document important aspects of developmental disabilities. These include surveys by the National Center for Health Services Research, the Social Security Administration, the Health Care Financing Administration, and the Bureau of the Census.
Public access data bases are available from the Collaborative Perinatal Study of 50,000 pregnancies in the early 1960s and the Child Health and Development Studies of 20,000 infants in the mid-1970s. Both studies include follow-up data on cognitive and other neurological development of the children studied.
Research
Preventive interventions are directed at reducing risk factors. For developmental disabilities, the interactions of biologic, behavioral, and environmental (social and physical) risk factors in pregnancy and early childhood are of obvious importance. However, because many children with congenital anomalies are born to parents who practice healthy lifestyles, there is a clear need for identifying risk factors that remain unknown.
Maternal use of alcohol during early pregnancy clearly can cause mental retardation. But it is not known why some infants with heavy alcohol exposure during early pregnancy have no discernible impairment. Understanding these differences may provide clues for prevention. The belief that the nutritional status of the mother is an important determinant of infant health provides the basis for the Women, Infants, and Children (WIC) food supplementation programs. More can be learned about how to maximize the impact of this intervention.
Recent studies show that women who use multivitamin supplements prior to conception and throughout early pregnancy have a lower risk of having an infant with spina bifida (Smithells et al., 1983; Mulinare et al., 1988; Milunsky et al., 1989). It is not clear whether this protective effect is attributable to vitamin supplements or to some other maternal behavior. More definitive studies are needed in this important area.
Expanded surveillance and epidemiologic research can greatly improve our ability to prevent developmental disabilities. A national surveillance program is needed to establish the magnitude of the problem, to measure our success in reaching prevention goals, and to determine gaps in prevention stemming from poorly implemented programs or services. Epidemiologic
research is also needed to identify the causes of the large proportion of developmental disabilities with unknown origins and to find the basis for the excess of developmental disabilities observed among the socioeconomically disadvantaged.
Improved and expanded surveillance, epidemiology, and applied research is needed as part of a coordinated research program on the prevention of developmental disabilities.
In summary, the goal of these efforts is to prevent developmental disabilities and reduce the incidence and severity of secondary conditions. To reach this goal, effective preventive measures must be implemented. The scientific base of known preventive interventions should be expanded by further evaluating promising strategies and by identifying the preventable risk factors that may underlie disabilities of unknown origin and etiology.
Comprehensive, coordinated services in health care, education, environmental control, and peer support are encouraged at the federal, state, and community levels. In addition, efforts to monitor prevention programs and establish uniform definitions and data collection methods will advance program coordination and accountability.
Access to Care and Preventive Services
The financing of health care and preventive interventions in the United States is complex, involving contributions from public programs, private insurers, and families (Table 4-6). This complicated strategy makes it increasingly difficult for all citizens to have equal access to health care and preventive services.
Inadequate insurance coverage is the single greatest barrier to equal access to health care, according to a Robert Wood Johnson Foundation study (1987). Lack of insurance coverage for preventive care services for women of childbearing age is a particular problem. More than 14 million women in this category (ages 15 to 44) do not have prenatal or other maternity coverage, 9 million are completely uninsured, and 5 million have private insurance coverage that excludes maternity care (Alan Guttmacher Institute, 1987).
The cost of immunizations and other pediatric preventive care is a strong disincentive for uninsured families who might otherwise obtain these services. Nineteen percent of children under 18 (10.6 million) had no insurance coverage in 1986 (Chollet, 1988). Thirty-three percent of all uninsured children had family incomes below the poverty level. In 1987, children under age 21 represented 52 percent of all Medicaid recipients and only 19 percent of expenditures. The average payment per child was $742, compared with $3,362 for adults (U.S. Health Resources and Services Administration, 1989).
TABLE 4-6 Various Normal and Special Care Prevention Activities for Developmental Disabilities and Their Usual Sources of Funding
|
|
Usual Source of Funding for Prevention Activities |
|
|
|
Type of Care |
Private Funds (third-party reimbursement) |
|
Public Funds (programs of state, city, and volunteer agencies) |
|
Normal care |
|
|
|
|
Prior to pregnancy |
|
|
Family life education: Avoidance of teen pregnancy; Improved parenting; Role of alcohol in pregnancy; AIDS education Family planning |
|
Prenatal |
Maternal serum alpha-fetoprotein; Ultrasound and amniocentesis as needed |
a Appropriate prenatal care |
|
|
Perinatal |
Hospital delivery |
a Newborn screening PKU, thyroid, etc. |
|
|
Childhood |
A medical ''home" for each child; Immunization; Automobile restraints |
|
Lead screening; Developmental screening |
|
Special care |
|
|
|
|
Prior to pregnancy |
Genetic counseling; Carrier testing |
|
Family assistance |
|
Prenatal |
Prenatal diagnosis as needed |
|
Family assistance |
|
Perinatal |
Regional newborn intensive care |
|
|
|
Childhood |
|
a Early intervention programs |
|
|
|
|
a Effective services for child progress; family support |
|
|
a Usual sources of funding for these activities are both public and private. |
|||
To help redress these inequities, governmental programs have been established to provide preventive services to two groups: persons with disabilities, and families with socioeconomic disadvantage. Because socioeconomic disadvantage is a risk factor for disability, persons may be members of both groups.
Public Programs for Persons with Developmental Disabilities
The major federal programs for persons with developmental disabilities are coordinated by the Administration for Developmental Disabilities (ADD) of the Department of Health and Human Services. ADD supports councils in each state that plan and coordinate services and advocate changes to reduce the disadvantage associated with developmental disabilities. ADD also awards grants to state offices providing legal and administrative assistance to individuals with developmental disabilities. Special project grants are awarded to encourage innovative work that will help integrate persons with disabling conditions into the community. ADD also supports the University Affiliated Programs, which offer clinical evaluation for children and training for providers in the field.
In addition to ADD-sponsored programs, the Medicaid and Supplemental Security Income (SSI) programs provide medical insurance and income assistance for persons with developmental disabilities. Guidelines are expected to be revised soon that will make more children eligible for SSI support.
Several other federal departments offer assistance to persons with developmental disabilities, including the Department of Education (special education and vocational education, among other programs), the Department of Transportation (grants to improve access to public transportation), and the Department of Housing and Urban Development (housing construction loans).
Public Programs for Families with Socioeconomic Disadvantage
Many preventive services programs for families with socioeconomic disadvantage are jointly financed by federal and state funds. At the federal level, the Departments of Health and Human Services, Education, and Agriculture are responsible for directing these programs. Agencies at the state and local levels manage the programs. Table 4-7 contains a partial list of existing programs for the prevention of developmental disability.
Within the Department of Health and Human Services, the Maternal and Child Health Bureau (Health Resources and Services Administration) administers block grants that provide major support for state prenatal care programs, newborn intensive care units, newborn screening, genetic services,
TABLE 4-7 Partial List of Existing Programs for the Prevention of Development Disabilities
|
Program |
Activity |
|
FEDERAL PROGRAMS |
|
|
Maternal and Child Health Bureau (Health Resources and Services Administration) |
MCH block grants include major support for states in public prenatal care programs, newborn intensive care units, newborn screening, services for children with special health care needs, etc. Additional elements are provided for genetics programs, AIDS education and prevention, and special projects. |
|
Centers for Disease Control |
Disabilities Prevention Program, epidemiologic studies; injury control program, lead poisoning prevention; childhood immunization, school health, AIDS prevention programs |
|
Office of Special Education and Rehabilitative Services |
P.L. 94-142, P.L. 99-457, and special projects |
|
Office of Disease Prevention and Health Promotion |
Health Objectives for the Year 2000 |
|
Office of Human Development Services |
Head Start, Administration on Developmental Disabilities |
|
Health Care Financing Administration |
Early Periodic Screening, Diagnosis, and Treatment, Medicaid |
|
National Institute of Child Health and Human Development |
Studies in causation, pathophysiology, and intervention; Mental Retardation Research Centers |
|
National Institute on Disability and Rehabilitation Research |
Studies of interventions to reduce secondary conditions in persons with disabilities; assistive technology research |
|
National Council on Disability |
National advocate for federal civil rights legislation for persons with disabilities and for a national disabilities prevention program; introduced concept of prevention of secondary conditions in persons with disabilities |
|
President's Committee on Mental Retardation |
Guidelines for state prevention planning, convenes National Coalition on Prevention of Mental Retardation |
|
Program |
Activity |
|
STATE PROGRAMS |
|
|
Department of Health |
Prenatal care clinics, standards of obstetric care, newborn screening, services for children with disabilities, special chronic disease programs, supports for immunization, lead screening and lead poisoning prevention, developmental screening, genetic counseling, family planning, AIDS programs, automobile restraints, education of the public, professional awareness |
|
Departments of Mental Retardation, Developmental Disabilities, and/or Mental Health |
Early childhood services, family support, counseling |
|
Department of Social Services |
Family support, child protection, respite, foster care, adoption |
|
Departments of Welfare, Public Assistance |
Family support, care coordination, Medicaid |
|
Department of Education |
Family life curricula, school health services, and early intervention programs |
|
Office for Children |
Standards, certification, advocacy |
|
Office for Prevention |
Prevention planning, monitoring, collaborative efforts |
|
COMMUNITY PROGRAMS |
|
|
City health departments |
Immunization, prenatal care, AIDS work, lead programs |
|
Other city agencies |
Recreation, youth programs, transportation |
|
Health care centers |
Screening, counseling, supports |
|
Neighborhoods |
Education, lead poisoning prevention |
|
PRIVATE PROGRAMS |
|
|
Voluntary and consumer organizations |
Education of public, counseling services, family planning, parent-to-parent services, screening, case-finding, advocacy, pressure on state agencies, and research (March of Dimes, Associations for Retarded Citizens, National Tay-Sachs Allied Diseases Association, National Mucopolysaccharidosis Society, Epilepsy Foundation of America, and United Cerebral Palsy Association) |
|
Program |
Activity |
|
Professional organizations |
Member education, advocacy, studies, standard development, data collection (American Association on Mental Retardation, American Association of University Affiliated Programs, American Academy of Pediatrics, Association of Maternal and Child Health Programs) |
|
University centers |
Genetic counseling and services, other services, technical assistance, education of public, advocacy, and research (teaching hospitals, pediatric departments, and University Affiliated Programs) |
|
Private philanthropy |
Special projects, all types |
|
COORDINATION OF SERVICES |
|
|
Interagency coordinating councils |
These coordinating groups are required in all states that accept planning money under Part H of the Amendments to the Education for Handicapped Children's Act (P.L. 99-457). Under direction of the specified lead agency (usually Education or Health) all the elements of state government participating in the early education effort for children at risk of or with disability must meet regularly to share in the design of intended services |
|
State advisory committees |
The states participating in the awards from the Disability Prevention Program of the Centers for Disease Control are required to establish advisory committees with multiagency and consumer membership that monitor the progress of local efforts. |
|
Program |
Activity |
|
Citizen organizations |
Many states that have created state prevention plans derive their original proposals under the stimulation and leadership of a special task force, study group, or governor's panel, with prominent representation by members of the Developmental Disabilities Council or Association for Retarded Citizens. Such committees usually remain in effect even after the state's Office for Prevention is operational and serve a valuable watchdog function in a voluntary setting |
and services for children with special health care needs. The programs of the Centers for Disease Control include injury control, lead poisoning prevention, childhood immunization, school health, and AIDS prevention. The new CDC Disabilities Prevention Program supports the planning, coordination, and evaluation of prevention services.
The Office of Human Development Services supports Head Start programs, state Developmental Disabilities Councils, and University Affiliated Programs for persons with developmental disabilities. The Health Care Financing Administration administers the federal contribution to Medicaid programs, which provide health care reimbursements for persons meeting state financial eligibility criteria.
Reimbursement for services in the Early Periodic Screening, Diagnosis, and Treatment Program is also managed by this agency.
Access to medical care and preventive services is an essential component of the prevention agenda. Persons who are socioeconomically disadvantaged need access to programs providing family planning information and comprehensive prenatal care. In addition, the private sector needs to be more active in programs to prevent developmental disabilities, as in the model to provide a "medical home" to children with disabilities that was developed by the Tennessee chapter of the American Academy of Pediatrics.
Professional Education
The rapid development of new technology makes continuing education of health professionals a challenge. University-based research groups supported by NIH, CDC, NIDRR, and MCH provide training settings for developmental disabilities researchers. Despite these programs, there is great need for additional epidemiologists with expertise in developmental disabilities. More leadership is needed in schools of public health to encourage program participants to enter this field. Development of coherent career tracts in universities and state health agencies is needed to keep capable researchers in the field.
Special professional educational programs are needed for practitioners and researchers in the area of developmental disabilities.






































