
5
Organization- and System-Focused Quality Improvement: The Committee View
James D. Mortimer
I have been honored to be part of this Institute of Medicine (IOM) study committee. I have learned a lot, and I have enjoyed the opportunity to meet and work with fellow panelists and the staff. The IOM report (IOM, 1990) is a comprehensive discussion of quality management in health care. In this brief paper, I will try to provide a picture of how quality improvement fits into this study and then discuss what role quality improvement might play in our proposed strategy.
As we use the term quality assurance in the report it includes quality assessment, quality assurance in a narrow sense, and quality improvement. Those are all terms for which people have varying definitions. In fact, quality improvement ideas are laced throughout the report, starting from the first goal in the committee's second recommendation and continuing through the rest of the report.
QUALITY IMPROVEMENT AND OUTCOMES
In Chapter 2 of the IOM report, we explore patient outcomes and our understanding of the distribution of outcomes (Figure 5.1). This can be visualized as a bell curve of outcomes in any given situation.
On the left tail of the curve we have activity that is less than expected—lower outcomes than desirable—and on the right we have a better-than-expected outcomes. The region for quality assurance in the narrow sense is on the left, in looking at causes of less-than-expected outcomes. Here quality assessment and detection, the disciplinary kind of corrective measures, are contemplated as part of the report. On the other end, we have superior results, and we talk about studying these things, finding out why they happen, and rewarding the people involved in achieving these better-
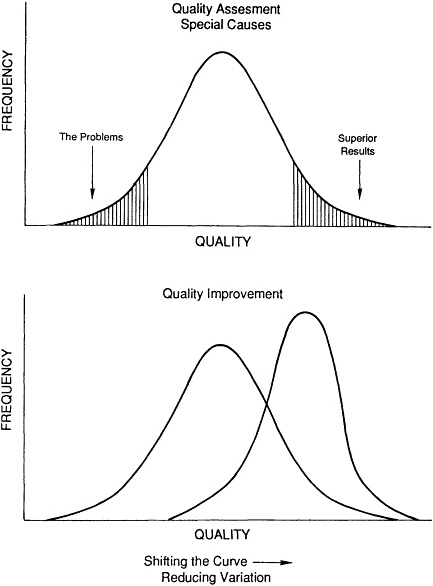
than-expected results. Those have been the more traditional domains of quality assurance as we have used the term.
The middle of this distribution is the domain in which we focus on improving the basic processes of health care. Quality improvement ideas pertain here. As discussed by Leo Cooney (1991), much in the IOM report is based on professionalism; we are looking for professionalism to improve the process.
Using the terminology of quality improvement, we need another kind of understanding of the left tail of the curve—what we call "special causes." These are problems or disturbances that are not random and not part of a stable process. They are things that occur because of certain situations. They may be caused by an individual. They may be caused by an event. They are correctable or observable as individual episodes or as individual transactions.
Things that happen in the middle of the distribution curve are part of the normal process, that is, the way the system actually works. Seeing health care as a system, as a combination of stable and unstable processes, is also part of this new understanding. Variations in stable processes are random and cannot be corrected by working on specific incidents. Quality improvement techniques are used to change the shape of this curve. By moving it to the right, quality improvement leads to better results on the average, and makes the curve narrower by reducing variation. This is the conceptual structure that we wrestled with in Chapter 2 of the IOM report.
Committee members' views on quality improvement were divided. Some members said, "Quality improvement is new to health care, and we are not sure that it has a role." Others said, "It is not new to health care. We have been doing it all along—quality improvement is part of quality assurance. And so there is really nothing new here. Is it relevant? Is it effective outside administrative areas where it is first taking root? Is it a fad? Is there proof of results? Does it have staying power?" These are some of the areas of uncertainty with which the committee wrestled.
THE ROLE QUALITY IMPROVEMENT PLAYS
I would like to show how we see the role of quality improvement in our proposed strategy for the Medicare program.
We talked in the later part of the report about three levels of quality assurance: the Medicare Program to Assure Quality (MPAQ) level, the Medicare Quality Review Organization (MQRO) level, and the provider level. These are shown in Table 5.1.
At the bottom of Table 5.1—the local provider level—we see quality improvement activity beginning. We anticipate that health care provider organizations will pursue quality improvement activities. The idea is that
TABLE 5.1. Relationships and Responsibilities of Main Constituents of the Medicare Program to Assure Quality
|
Responsible Entity |
Component Organizations |
Information Flow |
Quality Policy Deployment |
|
Congress of the United States |
Quality Program Advisory Commission (QualPAC) |
Advise Congress on strategies for quality assurance in Medicare and report on issues relating to quality of care for the elderly. |
Policy development and formation of goals and strategies |
|
Department of Health and Human Services (DHHS) |
National Council on Quality Assurance |
Advise the Secretary of DHHS, the HCFA Administrator, and others on all aspects of MPAQ implementation, strategy, program planning, and operations. |
|
|
|
Technical Advisory Panel (TAP) |
Advise the Secretary of DHHS, the HCFA administrator, and others on public oversight and regular, formal evaluation of the MPAQ. |
|
|
Health Care Financing Administration (HCFA) |
Medicare Program to Assure Quality (MPAQ) |
Long-and short-term program planning (MPAQ) (e.g., of MQRO activities). Monitoring and evaluation of MQRO operations and performance. Aggregation, analysis, and reporting of quality-of-care data. |
Program management |
|
|
Medicare Quality Review Organizations (MQROs) |
Obtain, analyze, use, and feed back quality-related processes and outcome data to internal quality assurance programs of practitioners, agencies, and facilities providing care to the elderly. Report information to MPAQ. Initiate quality recognition interventions and sanctions as appropriate. |
Information resources |
|
|
Technical assistance contractors |
Give expert assistance in methods of quality assessment and assurance to MQROs and to internal quality assurance programs. |
Training and facilitation resources |
|
Participating health care providers |
Quality assurance department, quality support department |
Collect and report clinical and financial information to MQRO. |
Quality improvement team selection and management |
the whole process should be very "permissive," that is, very supportive of quality improvement activity at the provider level. Both quality assurance and quality assessment activities will be conducted by the institution, and some interaction between quality assurance and quality improvement may occur. In other words, the problems and the difficulties that are detected in quality assurance may, in fact, become agenda material for improving the normal process of care delivery.
Moving up in the table to the Medicare Quality Review Organizations, we see data collection and data sharing where larger data sets and larger samples are being pulled together. We see risk-adjusted outcomes. This kind of information is produced for the health care provider organization, resulting in a feedback system. For quality assurance and quality improvement, we think that having that outside source of data is useful. There may be at this level some selection of diagnoses for study. Certain topics will be picked on a regional level and become selected input to the institutional level activity. Moving to the top of the table we see the major elements of the Medicare Program to Assure Quality. They are located in the U.S. Congress, the Department of Health and Human Services, and the Health Care Financing Administration. Their goals and activities are predicated in a definition of quality that does not exist today in the Medicare program in the explicit form we are recommending: Quality of care is the degree to which health services for individuals and populations increase the likelihood of desired health outcomes and are consistent with current professional knowledge. We also recommended capacity building, that is, training in quality assurance and quality improvement, and research in quality improvement effectiveness being mounted as national activities. Thus, many quality improvement activities are laced through the structure that we have envisioned in the proposed quality assurance strategy.
Looking at this table from the top, I could make the argument that this is a "quality policy deployment." At the federal level is a quality policy being put together—a definition, goals, attention to improving outcomes, and a customer (or patient) focus. At the MQRO level is quality management, where people are organized for, and decisions are made among, alternative kinds of activities. Deploying this quality policy down to the institutional level we have quality implementation, for example, quality improvement teams organized in a hospital.
How will this structure, in fact, work? Can it capture the favorable attention of the provider community? Those are key questions. As we gathered data in the study we found that much of what goes on today between government and health care does not have the favorable attention of the health care community. There is, in fact, defensiveness and a negative chemistry.
For quality improvement to work there needs to be a positive connection
—a partnership. Can this organizational structure form a partnership with the patient? Can it form one with the health care provider organization? These are the challenges: bringing this program closer to the needs of the patient, bringing it closer to the providers so that it is a positive connection.
This is, therefore, a major change in direction—one of several the report recommends. Indeed, "new directions" are the theme of this conference. As we wrestle with implementation of this strategy, we will begin to understand the full potential of the quality improvement model in health care.
REFERENCES
Cooney, L.M. More Professionalism, Less Regulation: The Committee View. Pp. 18-21 in Medicare: New Directions in Quality Assurance. Donaldson, M.S., Harris-Wehling, J., and Lohr, K.N., eds. Washington, D.C.: National Academy Press, 1991.
Institute of Medicine. Medicare: A Strategy for Quality Assurance. Volumes I and II. Lohr, K.N., ed. Washington, D.C.: National Academy Press, 1990.






