
4
Sexual Behavior and HIV/AIDS
This chapter discusses what we know about sexual behavior and HIV/AIDS in Africa. Given that the epidemic is being sustained by heterosexual transmission (see Chapter 3), information on sexual behavior is needed to help project the future course of the HIV/AIDS epidemic, to develop more effective prevention strategies, and to provide baseline data for evaluating the effectiveness of alternative prevention strategies. Consequently, this chapter provides important background information for the next chapter, which deals with prevention.
Published papers on sexual behavior and HIV/AIDS in sub-Saharan Africa show a remarkable uniformity in their point of departure and their destination. They tend to begin with the observation that in the absence of a vaccine or cure, changing sexual behavior is the only way to halt the spread of the HIV/AIDS epidemic in the region, and they end with a call for more research. What lies between diverges widely in methodology, focus, presentation of results, and conclusions. This chapter reviews some of this literature, attempting to identify common threads and define the boundaries of what we know. It concentrates on work dealing with general populations, although reference is made to some of the larger body of work on high-risk groups, such as commercial sex workers. The sections that follow address sources of information on sexual behavior in Africa, patterns of sexual activity, sex-related risk factors for HIV/AIDS, sexual practices and beliefs, AIDS awareness, the role of condoms, and behavior change. The chapter ends with conclusions and a set of recommendations for future research.
SOURCES OF INFORMATION
Researchers have often noted the dearth of studies on sexual behavior in sub-Saharan Africa. According to Larson (1989:9), "data on actual practice [of extramarital sex] are extremely rare and probably worthless." What little was known about sexual behavior in Africa at the time was exhaustively reviewed by Standing and Kisekka (1989). Accordingly, while some mention is made here of the early ethnographic work they reviewed, this chapter focuses on work published subsequently.
This chapter relies heavily on the results of a series of nine surveys coordinated by the World Health Organization/Global Programme on AIDS (WHO/GPA) that were carried out in 1989 and 1990. Eight of the surveys were national in coverage, while the ninth was conducted in Lusaka, Zambia. These surveys provide information on age at sexual initiation; broad patterns of sexual activity within and outside of stable unions; levels of commercial sex; and many other issues, such as perceived risk.1
QUESTIONS OF METHODOLOGY
The two principal sources of information about sexual behavior are ethnographic accounts and survey methods. Ethnographic accounts typically focus on sexual behavior only insofar as it relates to family, marriage, and kinship. Anthropological research uses primarily qualitative methods and participant observation for data collection. The goal usually is not to quantify the behaviors, but to understand their intent and meanings. This research is important to the design of interventions, but says little about the number of times an event occurs, its duration, or other factors of concern to disease transmission models. Large-scale surveys are designed to provide information that is comparable across cultures, but are forced to use sweeping, standardized definitions for complex and highly varied concepts such as marriage. Increasingly, researchers are designing studies that aim to bridge the gap between detailed observation of particular societies and broad characterizations of patterns and trends, for instance by combining survey data with diaries and in-depth interviews.
The principal danger with using survey methodology to collect data on sexual behavior is that respondents may simply say what they think researchers want to hear and that without elaborate probing, such methods may lead to a serious undercount of the true situation (Bleek, 1987). Women are believed to be particularly prone to giving normative answers. Indeed, women are sometimes excluded from surveys altogether for fear that their responses will be worthless
(Hogsborg and Aaby, 1992; Orubuloye et al., 1992). Nevertheless, there is also evidence that people are not entirely swayed by social norms when reporting their own behavior. For instance, several studies report a large gap between proportions expressing disapproval of premarital sex (typically high) and those reporting virginity at marriage (frequently low) (see, for example, Anarfi, 1993).
Public health researchers, independent of discipline, use both qualitative and quantitative methods to improve our understanding of behaviors. In an effort to verify independently the WHO/GPA estimates of sexual behavior, the WHO/GPA survey material is therefore supplemented here, as the authors of those studies urge, with less-generalizable surveys and information derived from ethnography, observational studies, serosurveys, and focus group interviews. Study designs differ substantially; those of the principal papers used in this chapter are summarized in Table 4-1. The following subsection makes some general observations about difficulties common to several studies.
Concerns about large-scale comparative survey research include the selection, operationalization, and validation of responses to items in the questionnaire. For example, researchers frequently need to use broad and sometimes arbitrary categories for comparability across research sites (e.g., partner categories such as regular and casual). Many of the difficulties that arise in conducting survey research are compounded when one is conducting research about intimate topics such as sexuality (Bleek, 1987). In the quest for comparability, large-scale surveys sacrifice information that may help explain local differences in sexual networking. Nor are international surveys likely to contribute much to our understanding of motivations for behavioral change. However, such surveys can be useful in highlighting patterns that link sociodemographic variables and personal behavior. As the editors of the WHO/GPA volume observe, single-round surveys are also good at describing the climate of public opinion and measuring the incidence of certain behaviors (Cleland and Ferry, 1995). Moreover, repeated over time, nationally representative surveys can help track behavior change.
Sampling proved problematic in many of the WHO/GPA studies reviewed. Although the WHO/GPA surveys covering the Central African Republic, Côte d'Ivoire, Guinea-Bissau, Togo, Burundi, Kenya, Lesotho, and Tanzania sought to be nationally representative, sampling difficulties appear to have led to an overrepresentation of women and urban residents in some cases. The remaining WHO/GPA survey in mainland sub-Saharan Africa, that in Lusaka, Zambia, leaned heavily toward the more educated.
Family formation norms vary widely throughout the African continent, and marriage in many African societies has often been described as being more akin to a process than a discrete event. It has proved difficult to develop easily understood definitions for sexual partners, and many of the subtleties of various forms of marriage are lost when all forms of unions are coded using a small number of standardized categories. For example, the WHO/GPA surveys make no distinction between regular partnerships and marriages, "regular" partnership
TABLE 4-1 Details of Some Studies of Sexual Behavior Cited in This Chapter
|
Reference |
Study Population |
Sample Size |
Main Methodology |
Limitations |
|
Anarfi (1993) |
Ghana, rural, urban |
1,360 |
Cross-sectional survey |
Unclear reference periods |
|
Anarfi and Awusabo-Asare (1993) |
Ghana, various lineal groups |
360 |
Cross-sectional survey |
Interviewers known to respondents; no clear definitions of marriage |
|
Hogsborg and Aaby (1992) |
Guinea-Bissau, urban (both sexes, but diary respondents all male) |
422 25 |
Cross-sectional survey Diaries |
Diary men purposively chosen |
|
Hunter et al. (1994) |
Nairobi, Kenya, prenatal clinic attenders |
4,401 |
Serosurvey |
|
|
Irwin et al. (1991) |
Kinshasa, Zaire, male factory workers |
1,796 |
Serosurvey, focus groups |
|
|
Kisekka (no date) |
Hausa groups, Nigeria; Baganda, Uganda |
n.a. |
Focus groups |
|
|
Konde-Lule (1993) |
Rakai, Uganda |
35 groups of 8-12 respondents |
Focus groups |
|
|
Lindan et al. (1991) |
Kigali, Rwanda prenatal clinic attenders |
1,458 |
Serosurvey |
|
|
Meekers (1994) |
DHS data, 7 African nations |
n.a. |
Survey data analysis |
|
|
Messersmith et al. (1994) |
Ile-Ife, Nigeria (men aged 18-59, women aged 18-49) |
1,149 |
Cross-sectional survey |
Excludes adolescents |
|
Meursing et al. (forthcoming) |
Bulawayo, Zimbabwe, sexually abused children |
54 |
Clinical examination, record review, focus groups |
|
|
O'Toole Erwin (1993) |
Ado-Ekiti, Nigeria, prenatal clinic attenders |
113 455 |
Clinical examination Cross-sectional survey |
|
|
Ogbuagu and Charles (1993) |
Calabar, Nigeria |
500 |
Cross-sectional survey |
High nonresponse rate; partnerships not clearly defined |
|
Orubuloye et al. (1991) |
Ekiti, Nigeria, urban and rural |
400 |
Cross-sectional survey |
Unclear reference periods, denominators, and partner definitions; no cross-checking of spousal replies possible |
|
Orubuloye et al. (1992) |
Ekiti, Nigeria |
488 |
''The lawyer's cross-examination method of investigation by exhaustion" |
|
|
Pickering et al. (1992) |
The Gambia, prostitutes (p) and clients (c) |
248p 795c |
Prospective survey, diaries |
|
|
Preston-Whyte (1994) |
Kwazulu/Natal, adolescents |
n.a. |
Focus groups, intervention |
All mixed-sex focus groups |
|
Schopper et al. (1993) |
Moyo, Uganda |
1,486 |
Cross-sectional survey |
|
|
Serwadda et al. (1992) |
Rakai, Uganda, trading towns, rural |
1,292 |
Serosurvey |
|
|
n.a. = not available DHS = Demographic and Health Surveys |
||||
being any union that continues or is expected to continue, however sporadically, for at least a year. "Casual" is anything outside that, and any partnership that lasts under a year and involves the exchange of money, gifts, or favors in exchange for sex is classified as "commercial." In the standard partner relations questionnaire,2 it is frequently difficult to distinguish one category from another, and secondary regular partners may be double-counted as casual, unless the interviewers were very skillful. In a study designed to test the validity of the WHO/GPA survey instrument, Schopper et al. (1993) showed that among 392 women whose answers could be cross-checked with those of their partner, 12 percent reported they had co-wives when their husbands declared themselves monogamously married, thus illustrating the difficulty of watertight categorization. Other surveys use entirely different definitions, so that even comparing data on premarital sex becomes fraught with difficulty.
Discrepant reference periods do little to clear the confusion. Without defining the term "current," several West African studies make a distinction between current partners and partners within the previous week (e.g., Orubuloye et al., 1991; Anarfi, 1993). As documented by Orubuloye et al. (1991), consistently more men and women in both urban and rural areas reported abstinence in the last month (and, except for rural males, in the last 12 months) than reported abstinence currently, which leaves us with a puzzle for interpretation. That respondents are confused by definitions emerges also from a study by Ogbuagu and Charles (1993). In that study, 55 percent of women reported more than one current partner. However, when asked directly if they kept other partners outside their regular partnership, 66 percent answered no.
Sources of bias are sometimes incompletely documented. Often studies state or imply significant levels of nonresponse, but give no information on possible refusal bias (Ogbuagu and Charles, 1993; Omorodion, 1993; Oyeneye and Kawonise, 1993). Bias can also arise from the injudicious or unclear use of denominators; for instance, excluding virgins from the denominator will bias downward the mean age of onset of sexual activity in the youngest cohorts (Konings et al., 1994).
The question of age cut-offs is relevant to almost every study. Although overwhelming evidence of early sexual activity is provided in existing sources such as the Demographic and Health Surveys (DHS) series, the successor to the World Fertility Surveys (WFS), very few studies include people under age 15. Indeed, some investigate only the behavior of people over age 18 (e.g., Messersmith et al., 1994), and many exclude women after they reach age 50.
Other shortcomings common across studies are a lack of information about economic status (education is often the only proxy for socioeconomic status) and a failure to include information about the content of public education campaigns, data that might help us understand local knowledge and attitudes.
The Issue of Validity
Self-reported data on sexual activity are of course more or less impossible to verify absolutely. But other checks can be made. For example, are study results consistent with what we know from other sources? The answer would appear to depend on the context. The age at first intercourse reported in the WHO/GPA surveys does not differ strikingly from the available DHS data (Schopper et al., 1993; Meekers, 1994). On occasion, however, reported condom use differs greatly, appearing much higher for a given country in the WHO/GPA surveys than in subsequent DHS surveys (Cleland and Ferry, 1995). This discrepancy may occur because people's answers differ according to the intent of the survey.
Are data mutually consistent? In the WHO/GPA surveys, consistency is difficult to check because there is no device for linking two halves of a couple when each individual has been randomly selected. Since questions are not repeated within the same interview, internal consistency checks are difficult as well. There is, however, broad aggregate agreement between the sexes on coital frequency and number of regular partners. In Schopper et al. (1993), a study using the WHO/GPA survey instrument, 392 couples were identified among the 1,486 individuals randomly selected for interview. Although it was confirmed that results were good on an aggregate basis, there were significant disparities on the individual couple level in reports of coital frequency between monogamous couples reporting no outside partners.3 Similar results are cited by Rutenberg et al. (1994) using Tanzanian DHS data for 1991/1992; men reported on average 35 percent more sexual contacts than women. That study shows further that women are just as likely as men to report higher frequency than their partner.
Studies on sexual behavior consistently find that men report more partners than women. For instance, Konings et al. (1994) show men reporting around 10 times as many partners as women. This discrepancy may occur because men overreport their partners, because women underreport theirs, or because a large number of men network with a small number of women who have a high turnover of partners. Many researchers point out that their study populations are unlikely to capture sex workers; few indicate whether they include men likely to be clients
of sex workers, such as truck drivers or the military—highly mobile groups that might escape the sampler's net.
One way of teasing bias out of a single-round survey is to supplement it with other methods. Repeated interviews at short intervals and respondent diaries have been shown to be effective in this regard. Using this method, studies in Guinea-Bissau and Senegal suggest overreporting of coital frequency in surveys, but underreporting of numbers of partners (Hogsborg and Aaby, 1992; Enel et al., 1994). Similarly, Pickering et al. (1992) used diaries to show that prostitutes in The Gambia consistently gave higher totals of client contacts in surveys than when reporting daily; comparison with questionnaires administered to clients emerging from their rooms showed that the women also overreported condom use in surveys.
More cross-referencing of questions might help identify bias in normative responses. In focus group interviews of schoolgirls in Zimbabwe, most denied they had sugar daddies, that is, older men as boyfriends who gave them presents or money for sex; however, in answer to a later question, half volunteered ways of keeping presents from sugar daddies hidden from parents, indicating that their earlier responses may have been less than wholly honest (Vos, 1994). Individual interviews might have avoided this discrepancy. Ethnographic models may also be applied to resolve discrepancies in single-round survey results (Stone and Campbell, 1984).
It is clearly premature to reach any firm conclusions about the reliability or validity of survey data on sexual behavior in developing countries. However, after a review of the evidence, Dare and Cleland (1994) are guardedly optimistic that the information gathered in most surveys is solid enough to allow broad conclusions to be drawn.
PATTERNS OF SEXUAL ACTIVITY
This section examines patterns of sexual activity in sub-Saharan cultures, including sexual initiation and premarital intercourse, sex within marriage or a stable union, extramarital and casual sex, and commercial sex.
Sexual Initiation and Premarital Intercourse
Marriage has long been considered a proxy for the onset of sexual activity. In cultures where female sexuality is strongly proscribed, an increase in premarital sex is often believed to be synonymous with the amoralizing influence of modernization. In premodern times, marriage for most sub-Saharan African women took place around puberty. Now, in some African societies, changes associated with modernization, such as increasing urbanization and greater emphasis on formal education for women, have led to an increase in the age at first marriage for women.
In some sub-Saharan African civilizations (although by no means universally), marriage has been an unfolding process rather than a salient event (Meekers, 1992). As Bledsoe (1990:118) writes:
The first problem is that of defining when marriage begins and ends. African marriage is often a long, ambiguous process rather than a unitary event. It may extend over a period of months or even years, as partners and their families work cautiously toward more stable conjugal relationships. A girl, sometimes with her family's implicit permission, may test out potential relationships with several young men before establishing a more permanent one.
This ambiguity presents researchers with an additional problem of interpretation, since the answer to the question "Were you a virgin at marriage?" clearly depends on how the respondent dates marriage. If a union turned out to be successful, the respondent may in retrospect date the marriage from the start of that union, even though it was at the time a tenuous and potentially transitory liaison (van de Walle, 1993).
A substantial body of work addresses the question of premarital sex. Inevitably, definitions vary widely. In the WHO/GPA surveys, for instance, the term refers to any sex before first regular partnership. Other surveys define the term as any sexual activity before legally or traditionally sanctioned marriage, thus including early sex between people who subsequently go on to marry. Table 4-2 gives some of the findings reported by the various studies.
As mentioned earlier, several studies show a discrepancy between a persistent ideal of virginity at marriage and actual levels of premarital activity, both now and in the past. In Anarfi (1993), three-quarters of both men and women said they believed women should be virgins at marriage, but barely 1 in 10 of either sex maintained that he or she was. Further, two-thirds of ever-married men and half of ever-married women reported having had two or more premarital partners. Some 40 percent of respondents in Ogbuagu and Charles' (1993) study in Calabar, Nigeria, said they hold virginity at marriage as an ideal, but fewer than half that proportion could report no sex before marriage. While Botswana and Kenya display strong evidence of a rise in premarital sex, Meekers (1994), using data from a variety of DHS studies, shows that there is generally a substantial fall in the proportions of single women currently reporting sexual activity as compared with the proportions of married women saying they experienced sex before marriage. While the figures are distorted by the fact that many single women who are still virgins may go on to have premarital sex, this observation also hints that it may be easier to report socially dubious behavior after the fact than at the time of its occurrence.
Several researchers note that women sometimes feel under pressure to prove they are fertile by getting pregnant in order to increase their chances of marriage (e.g., Standing and Kisekka, 1989). Because of a ubiquitous age difference at marriage between men and women, any decline in polygyny—as long as populations
TABLE 4-2 Percentage of Respondents Reporting Premarital Sex in Various Studies
|
|
|
|
|
Percent Reporting Premarital Sex |
|
|
Reference |
Country |
Population |
Study Period |
Women |
Men |
|
Cleland and Ferry (1995) |
Burundi |
singles (15-19) |
12 months |
3 |
10 |
|
Meekers (1994) |
Burundi |
all single |
ever |
5 |
n.a. |
|
Meekers (1994) |
Burundi |
all ever-married |
ever |
20 |
n.a. |
|
Balépa et al. (1992) |
Cameroon |
all single |
ever |
57 |
n.a. |
|
Cleland and Ferry (1995) |
CAR |
singles (15-19) |
12 months |
56 |
69 |
|
Cleland and Ferry (1995) |
Côte d'Ivoire |
singles (15-19) |
12 months |
28 |
43 |
|
Anarfi & Awusabo-Asare (1993) |
Ghana |
all respondents |
ever |
75 |
90 |
|
Anarfi (1993) |
Ghana |
all respondents |
ever |
87 |
n.a. |
|
Meekers (1994) |
Ghana |
all single |
ever |
47 |
n.a. |
|
Meekers (1994) |
Ghana |
all ever-married |
ever |
60 |
n.a. |
|
Cleland and Ferry (1995) |
Guinea-Bissau |
singles (15-19) |
12 months |
30 |
51 |
|
Cleland and Ferry (1995) |
Kenya |
singles (15-19) |
12 months |
44 |
54 |
|
Meekers (1994) |
Kenya |
all single |
ever |
50 |
n.a. |
|
Meekers (1994) |
Kenya |
all ever-married |
ever |
61 |
n.a. |
|
Cleland and Ferry (1995) |
Lesotho |
singles (15-19) |
12 months |
16 |
33 |
|
Meekers (1994) |
Liberia |
all single |
ever |
81 |
n.a. |
|
Meekers (1994) |
Liberia |
all ever-married |
ever |
59 |
n.a. |
|
Meekers (1994) |
Mali |
all single |
ever |
6 |
n.a. |
|
Meekers (1994) |
Mali |
all ever-married |
ever |
13 |
n.a. |
|
Kourguéni et al. (1993) |
Niger |
all single |
ever |
10 |
n.a. |
|
Messersmith (1994) |
Nigeria |
all respondents |
ever |
53 |
85 |
|
Ogbuagu and Charles (1993) |
Nigeria |
all respondents |
ever |
82 |
83 |
|
Federal Office of Statistics (1992) |
Nigeria |
all single |
ever |
41 |
n.a. |
|
Barrère et al. (1994) |
Rwanda |
all single |
ever |
12 |
n.a. |
|
Cleland and Ferry (1995) |
Tanzania |
singles (15-19) |
12 months |
24 |
37 |
|
Rutenberg (1994) |
Tanzania |
all single |
ever |
44 |
72 |
|
Cleland and Ferry (1995) |
Togo |
singles (15-19) |
12 months |
3 |
18 |
|
Meekers (1994) |
Togo |
all single |
ever |
61 |
n.a. |
|
Meekers (1994) |
Togo |
all ever-married |
ever |
65 |
n.a. |
|
Cleland and Ferry (1995) |
Lusaka, Zambia |
singles (15-19) |
12 months |
10 |
16 |
|
Meekers (1994) |
Zimbabwe |
all single |
ever |
26 |
n.a. |
|
Meekers (1994) |
Zimbabwe |
all ever-married |
ever |
48 |
n.a. |
|
n.a. = not available CAR = Central African Republic |
|||||
are growing—would increase the pool of available women of marriageable age relative to potential husbands in older cohorts. This increase would be likely to intensify competition for husbands, reinforce pressures to prove fertility, and erode lingering disapproval of premarital sex.4 Already, 1 in 10 urban respondents in Ado-Ekiti, Nigeria thinks that no one is a virgin at marriage these days, and some men and women report that virginity is considered antisocial (Orubuloye et al., 1991). Qualitative work with teenagers in Kwazulu/Natal, South Africa, led Preston-Whyte (1994) to observe that whatever parents preach, they will usually help care for offspring of their unmarried teenage daughters. Social sanctions on premarital pregnancy do not run deep, although perhaps deep enough to make sexual education and services targeted at young teens politically difficult.
WHO/GPA survey data show that education is associated with an increase in premarital sex in the teen years, particularly in societies with generally low levels of sexual activity. However, in data analyzed by Meekers (1994), the association more or less disappears when age is held constant. The implication is that since extra years of schooling are likely to delay marriage, they increase exposure to premarital sex. Any observed increase in premarital sexual activity may thus be a function more of later marriage (or changing definitions of marriage) than of earlier first sexual experience.
If we look at sexual initiation regardless of marital status, rates of sexual activity recorded in the WHO/GPA surveys for men and women converge dramatically. In West Africa, sexual initiation tends to occur relatively early: in Côte d'Ivoire and the Central African Republic, 45 to 60 percent of both sexes are sexually active by the age of 15 (see Table 4-3). In Calabar, Nigeria, Ogbuagu and Charles (1993) report lower figures: over one-third of men and 17 percent of women have had sex by the time they are 15. In East and Southern Africa, WHO/GPA surveys show that sexual activity starts slightly later, with a wider gap between the sexes. In some studies (e.g., Anarfi and Awusabo-Asare, 1993, Ghana), people recall that they first had sex when as young as 8 or 10. This young age at sexual debut is important when targeting populations for intervention, particularly in light of the work by Konings et al. (1994) showing a correlation between the early onset of sexual activity and large numbers of partners.
Sex Within Marriage or a Stable Union
It appears that marriage may have been a relatively informal concept in many African societies throughout much of history, becoming more narrowly defined only in response to the dictates of colonial administrators and missionaries. Some
TABLE 4-3 Approximate Percentage of Those Currently Aged 15 Already Sexually Active
|
Study Area |
Male |
Female |
|
Burundi |
27 |
7 |
|
Central African Republic |
46 |
43 |
|
Côte d'Ivoire |
47 |
60 |
|
Kenya |
24 |
29 |
|
Lesotho |
36 |
6 |
|
Tanzania |
29 |
29 |
|
Togo |
19 |
15 |
|
Lusaka, Zambia |
43 |
24 |
|
SOURCE: Cleland and Ferry (1995). |
||
suggest that formalization is currently being reversed, although, as Guyer (1994) points out, there are no clear data to support this conclusion that many anthropologists have reached by observation.
Certainly, informal unions are very common. In some cities in the developing world, nearly half of all adults are living in unions not formally legitimized (Caraël, 1995), so distinguishing between marital and extramarital relations can be problematic. What emerges clearly from the WHO/GPA data is that multiple concurrent partnerships are frequent in Africa. In Lesotho, with low organized polygyny but high rates of migrant labor, over half of men and two in five women report more than one current regular partner. In Côte d'Ivoire, over one-third of men are in two or more unions simultaneously, but no women report more than one regular partner, while in Lusaka, Zambia, twice as many men as women have two stable relationships. In general, women are aware of their partners' other partners; the surveys show a very high correlation between men reporting more than one partner and women reporting the same of their husbands.
The WHO/GPA surveys report high levels of abstinence within marriage or regular partnership (Table 4-4), in part the consequence of either long periods of abstinence following the birth of a child or terminal abstinence following the birth of a grandchild. One-quarter of married women in Togo reported no sex with their regular partner in the 12 months preceding the study. (Figure 4-1 shows that women in Togo also average more months of postpartum abstinence than most other women in Africa.) In most countries, 4 to 8 percent of currently
TABLE 4-4 Percentage of Currently "Married" Men and Women (15-49) Reporting Sex with Their Regular Partner and Mean Coital Frequency in the Last Month
|
|
Burundi |
Côte d'Ivoire |
Lesotho |
Tanzania |
Togo |
Lusaka, Zambia |
||||||
|
Percent Reporting |
M |
F |
M |
F |
M |
F |
M |
F |
M |
F |
M |
F |
|
No sex this year |
6 |
8 |
4 |
8 |
4 |
6 |
6 |
8 |
11 |
24 |
2 |
2 |
|
Sex this year but not this month |
27 |
26 |
38 |
42 |
46 |
54 |
28 |
28 |
31 |
34 |
42 |
43 |
|
Sex this month |
68 |
66 |
58 |
50 |
50 |
41 |
66 |
64 |
58 |
42 |
56 |
55 |
|
Mean coital frequency |
5.5 |
5.7 |
2.9 |
2.0 |
3.0 |
1.9 |
4.9 |
4.4 |
2.9 |
1.5 |
3.4 |
3.7 |
|
Sample size |
735 |
826 |
865 |
1,136 |
356 |
805 |
1,119 |
1,642 |
811 |
961 |
594 |
738 |
|
SOURCE: Cleland and Ferry (1995). |
||||||||||||
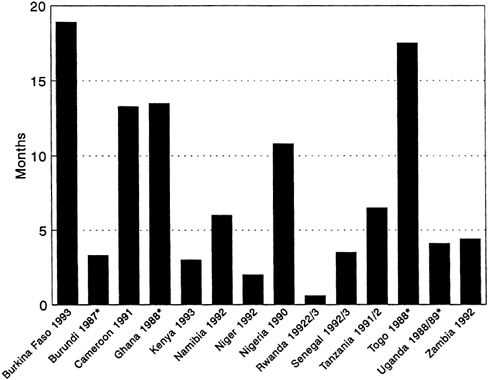
FIGURE 4-1 Average Number of Months of Postpartum Abstinence. NOTE: Asterisk indicates mean number of months of postpartum abstinence. All other figures are median number of months. SOURCES: Burkino Faso: Konaté et al. (1994); Burundi: Segamba et al. (1988); Cameroon: Balépa et al. (1992); Ghana: Ghana Statistical Service (1989); Kenya: National Council for Population and Development (1994); Namibia: Katjiuanjo et al. (1993); Niger: Kourguéni et al. (1993); Nigeria: Federal Office of Statistics (1992); Rwanda: Barrère et al. (1994); Senegal: Ndiaye et al. (1994); Tanzania: Ngallaba et al. (1993); Togo: Agounké et al. (1989); Uganda: Kaijuka et al. (1989); Zambia: Gaisie et al. (1993); Zimbabwe: Central Statistical Office [Zimbabwe] (1989).
married respondents reported not having sex with their regular partners for a year or more. In a single month, 35 to 45 percent typically had no sexual contact with their spouse or regular partner.
Extramarital and Casual Sex
Given that marriage is difficult to define, defining what constitutes extramarital sex is also problematic. A woman may consider her husband's relationship with another woman to be an extramarital affair, while the man may see it as a stable union of some emotional significance. What a researcher considers it to be will vary from study to study.
Much of the nonquantitative literature assumes that extramarital sex must have a primarily economic underpinning, with women accepting material support, gifts, or money from their lovers. ''African women do not trust their boy-friends and believe that several are needed as a financial insurance," declare Awusabo-Asare et al. (1993:71). Indeed, two out of three rural women in a Nigerian study justified their extramarital affairs on the basis of economic security, although half of all extramaritally active urban women said they had sex outside marriage just for fun (Orubuloye et al., 1991). Even among market traders, a group often thought highly likely to supplement their income through sexual relations (e.g., Orubuloye et al., 1992), nearly one-quarter said they had affairs for pleasure (Omorodion, 1993). In-depth interviews in Uganda suggest that the most common reaction by men to their wives having extramarital affairs was to try to avenge oneself by sleeping with the wife of the offending man—a powerful push toward extramarital sex (Obbo, 1993a).
An interesting variation on the theme of extramarital sex as a survival strategy is proposed by Guyer (1994). She maintains that easily dissolved marriages and increasingly common informal unions may be insufficient to ensure support for women, who are instead turning to childbearing as a survival strategy. Because men in most of sub-Saharan Africa are happy to claim paternity, and extended families are happy to absorb additional members, bearing a child may give a woman a stake in a man's family resources, regardless of whether she has married into the family or not. Bearing several children to different men will potentially allow the woman a claim to the resources of several families. Where conception and childbirth are the prime goal of a union, the prognosis for condom use as an AIDS-prevention strategy cannot be good.
It appears that a woman's postpartum abstinence may well be a strong motivation for men to seek sex outside marriage. Messersmith et al. (1994) show strong aggregate agreement between the sexes when reporting their own or their partner's pregnancy and lactation; but while only 12 percent of breastfeeding women reported having sex in the last 4 weeks, the proportion was three times as high among men who declared that their main partner was lactating.5 Hogsborg and Aaby (1992) report that 68 percent of women observing postpartum abstinence or their male principal partners said the male partner had sex with others during that time.
Levels of extramarital sex with nonregular partners vary, though once again comparisons are difficult because of differences in definition. 6 WHO/GPA surveys
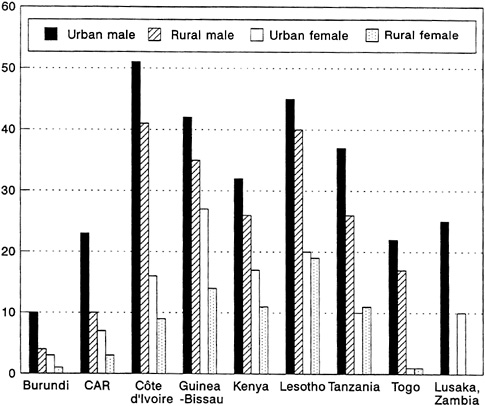
FIGURE 4-2 Percentage of All Men and Women Reporting Nonregular Sex in the Last Year, by Residence.
SOURCE: Cleland and Ferry (1995).
show proportions of men reporting nonregular sex ranging from 51 percent in urban Côte d'Ivoire to 4 percent in rural Burundi (a figure the researchers regard as surprisingly low in view of the area's high HIV seroprevalence). Women tend to report less than half of male levels of nonregular sexual activity (Figure 4-2). In a study that looked only at most recent sexual partners in Ghana, around two-fifths of women, and a slightly higher proportion of men, reported that their most recent partner was not their spouse, although only a fraction of those relations would be defined as extramarital by the WHO/GPA surveys (Anarfi, 1993). Beliefs about partners can be revealing: in high-HIV-prevalence Rwanda, nearly 9 women in 10 said they believed most married men are unfaithful, and 44 percent said they believed most married women are, too (Lindan et al.,
1991). It may also be noted that women are far more likely to have extramarital lovers if they are the younger wives in a polygynous marriage than if they are the only wife (Orubuloye et al., 1991).
With whom are the men having sex? In Ekiti, Nigeria, Orubuloye et al. (1992) report that two-thirds of men's extramarital partners are single, and, perhaps disturbingly, one-third are described as schoolgirls.7 This pattern is confirmed by Hogsborg and Aaby (1992), who conclude that in Guinea-Bissau, single women under age 26 appear to constitute the pool of nonmarital partners for men of all ages.
And who are the men? The WHO/GPA surveys show a strong aggregate correlation between men reporting casual sex in the last year and men reporting more than one regular partner. This finding would suggest that where overall levels of sexual activity are high, women who have no sex outside regular partnerships will still be at increased risk for HIV. Stronger still is the correlation between men reporting casual sex and men not cohabiting with their regular partner (a figure that reaches 43 percent in Côte d'Ivoire and is lowest in Tanzania at 11 percent). Not surprisingly, men reporting more than five casual partners in the last month are disproportionately likely to live in countries with generally high levels of sex outside regular partnerships. Interestingly, there is no apparent correlation between levels of commercial sex reported and the proportion of men with five or more casual partners, though this surprising result may perhaps be explained by the imprecise definition of "commercial" sex in the surveys.
Commercial Sex
The WHO/GPA survey instruments defined "commercial" sex as any sex in which money, gifts, or favors are exchanged in partnerships lasting under a year. Interviewers were told that the term did not include relationships in which the exchange was not the prime motive or reason for sex. Use of this definition once again led to the possibility that the same sexual experience would be classified differently by the man and woman involved. In terms of overall proportions reporting commercial sex, men dominated everywhere, though the gender gap was narrower in Côte d'Ivoire than elsewhere. However, in most sites, a higher proportion of all nonregular sex was classified as commercial by women than by men. The incidence of commercial sex during the past year. ranged from 3 percent of all men in Burundi to 25 percent of all men in Tanzania (Figure 4-3A)
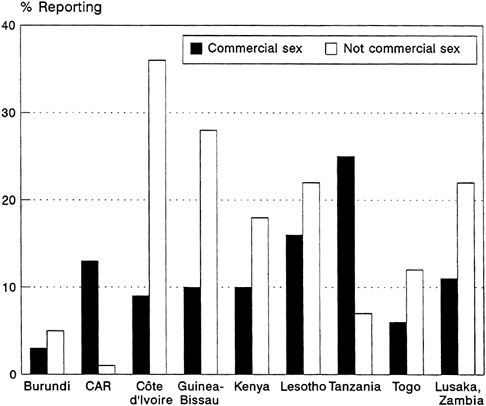
FIGURE 4-3A Percentage of Men who Reported in the Last Year (1) Commercial Sex and (2) Nonregular but Not Commercial Sex. SOURCE: Cleland and Ferry (1995).
and from 0.2 percent of all women in Burundi and Togo to 11 percent of all women in Tanzania (Figure 4-3B).
The confusion surrounding transactional sex is apparent elsewhere. In Ekiti, Nigeria, Orubuloye et al. (1992) note a profusion of sex workers incompatible with the low levels of commercial sex reported by men. Only 1 percent of extramarital partners of men surveyed were reported to be sex workers, but 38 percent were classified as street traders, whom the authors describe as an important source of commercial sex. Further, the authors note that when a man visits a sex worker regularly, the relationship may cease, in his mind, to be one of commercial sex. Indeed, such sex would not have been classified as commercial in the WHO/GPA surveys if the relationship lasted more than one year. In another Nigerian study, a far higher proportion of men (14 percent) reported having paid for sex with a sex worker (Messersmith et al., 1994). Relatively high proportions (16 percent) of schoolboys in Zimbabwe surveyed by Wilson et al. (1989) reported sex with a prostitute.
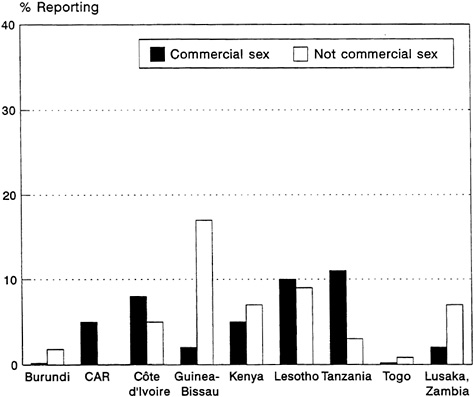
FIGURE 4-3B Percentage of Women who Reported in the Last Year (1) Commercial Sex and (2) Nonregular but Not Commercial Sex. SOURCE: Cleland and Ferry (1995).
Many authors comment that economic hardship, particularly that caused by structural adjustment programs, has increased the need for and incidence of transactional sex (e.g., Larson, 1989; Caldwell et al., 1993). Although the spectrum of women engaging in transactional sex is broad, commercial sex workers are often portrayed as hapless victims of extreme poverty and family breakdown in surveys and focus group interviews (Pickering et al., 1992). However, in an extremely thorough prospective study of prostitutes and their clients in The Gambia that led to invitations to the commercial sex workers' family homes, the researchers reported that many of the women were from well-off families; their work appeared to be a life-style choice. A concurrent study (Pickering and Wilkins, 1993) calls into question the common assumption that many widowed, divorced, or separated women, shorn of their partner's support, are obliged to turn to sex as a means of generating income. Through income/expenditure diaries, formerly married women were shown to generate two-thirds of their income by providing services, such as laundry and cooking, that require few skills, but are commonly required in cities in which men greatly outnumber women. That these women
had discovered viable alternatives to casual transactional sex was supported by the fact that levels of syphilis among formerly married women were found to be nearly identical to those among currently married women, and one-third those among a well-defined group of professional prostitutes.
SEX-RELATED RISK FACTORS
In examining which sociodemographic, behavioral, or attitudinal characteristics might be linked to an elevated risk of contracting HIV/AIDS, studies fall into two categories. In the first, the HIV status of study participants is known, usually only after information on explanatory variables has been collected. In the second, analysts must rely on proxy markers of risk that have been determined by clinical studies of the first kind; these markers include high numbers of partners, unprotected sex with commercial sex workers, and the presence of STDs.
This section examines sex-related risk factors associated with HIV/AIDS, including a high number of partners/commercial sex, perceived risk, age, education, marital status, residence, migration, STDs, circumcision and traditional medical practices, and alcohol.8
High Number of Partners/Commercial Sex
In analyzing the WHO/GPA survey data, researchers define "risk behavior" as having one or more nonregular partners in the last 12 months, while "high-risk behavior" is having "commercial" sex in that time period. Although the definitions may appear to capture a wide range of behavior, they are lent credence by serostudies. Lindan et al. (1991) show that in Kigali, Rwanda, while one-quarter of the women reporting only a single lifetime partner were seropositive, the proportion rose to 47 percent for women reporting more than one lifetime partner. In Nairobi, Kenya, where overall prevalence is much lower, Hunter et al. (1994) found a strong positive association between the number of lifetime partners and seropositivity, even at low number of partners. Lindan et al. (1991) also found that 42 percent of Rwandan women reporting that their partner had visited commercial sex workers tested HIV-positive, as compared with 30 percent of those who answered negatively or did not know.
The risk inherent in the rate of partner exchange is of course affected by the background prevalence of HIV infection. While the odds of being HIV-positive increase with the number of sexual partners in various urban and rural locations,
the danger at any given level of sexual activity is greater where HIV is more prevalent (Serwadda et al., 1992).
Perceived Risk
Surprisingly, there does not seem to be a strong correlation between perceived risk and risk behavior. People who report risk behavior do not seen to feel more threatened by HIV than people who do not, and in the WHO/GPA data, no relationship between the two appears when the effects of other factors are simultaneously controlled. Conversely, Lindan et al. (1991) report that those who perceive themselves to be at risk of AIDS (62 percent of them through their partner's sexual behavior rather than their own) are actually no more likely to be seropositive than those who feel less threatened. It does, however, emerge from that study that women who feel powerless to prevent HIV/AIDS are more likely to be infected.
The WHO/GPA data suggest that risk behavior is itself positively correlated with AIDS awareness and knowledge of its lethality and sexual transmission routes. While this finding may dim hopes that knowledge will lead to behavior change, the relationship may be spuriously caused by the fact that formal schooling leads simultaneously to better AIDS awareness and a socioeconomic status that makes it easier to acquire more partners.
Age
In the WHO/GPA surveys, risk behavior is associated with age. In some African societies, for example, Central African Republic, Guinea-Bissau, and Kenya, over half of all those aged 15 to 19 are already sexually experienced (Caraël, 1995). In contrast, in other societies such as Burundi, around 90 percent of those aged 15 to 19 are still virgins (Caraël, 1995). However, by age 20, the level of sexual experience is close to 90 percent among most of the populations studied in the WHO/GPA surveys. Never-married men aged 15 to 19 reported that in the last 12 months they had had between 1.6 and 2.5 partners; women in the same age range reported between 1.0 and 1.9 partners.
Condom use for sexually experienced men aged 20 to 24 varies from under 20 percent in Lesotho, Tanzania, and Togo to over 50 percent in Guinea-Bissau and Lusaka, Zambia (Mehryar, 1995). Reported condom use for women in this age range was significantly lower. Only in Lusaka, Zambia, did more than 20 percent of sexually experienced women in this age range report ever using a condom, and in Central African Republic, Togo, and Lesotho, fewer than 10 percent of women in this age range reported ever having used a condom (Mehryar, 1995).
Education
In the comparable national WHO/GPA studies, more education is associated with more casual sex everywhere except Lesotho. The effect, which is most powerful when secondary education and primary or no schooling are compared, remains when the effects of other variables are controlled. 9 However, the WHO/GPA analyses do not include economic status. It is likely that the effect of education is confounded by the fact that for men, education opens the door to resources, and resources can make it easier to acquire access to commercial or casual sex. In Rakai, Uganda, seropositivity shows a linear rise with education and with occupational status for both sexes, with the exception of female bar and hotel workers (Kivumbi, 1993).
Marital Status
Lindan et al. (1991) report that among women, the unmarried were found to be far more likely to be seropositive than the married, with the monogamously married safest of all. In Rakai, Uganda, and Nairobi, Kenya, the same pattern was found (Serwadda et al., 1992; Hunter et al., 1994). In Nairobi, single sexually active women were found twice as likely and formerly married women three times as likely as married women to be HIV-positive. The high rates among the formerly married are not altogether unexpected. In high-prevalence areas, the formerly married may well be AIDS widows and therefore at extremely high risk of exposure. Alternatively, some women may have been divorced because they were suspected to be HIV-positive.
In terms of risk behavior, Rutenberg et al. (1994) used DHS data to show that in Tanzania, single women have the highest rate of partner change, with the formerly married just behind, while for men the two groups are roughly the same. In the WHO/GPA surveys, formerly married women were typically more likely to report casual sex than married women, with single women being intermediate. Among the three surveys for which multivariate analyses were performed, however, a significant effect of marital status was found only in Côte d'Ivoire. Among men, marital status in these three countries appears to be a less important influence on risk behavior.
Residence
The WHO/GPA surveys in every case reported more casual sex in urban than in rural areas, though the data show an extremely strong correlation between
urban and rural rates of casual sex within each country. There was little difference across place of residence in the percentage of men who reported having commercial sex in the last 12 months, although among men reporting commercial sex, the mean number of partners was higher in urban areas (Caraël et al., 1994). In a result that surprised researchers, however, the effect of residence evaporated in multivariate analysis, suggesting that it is greatly confounded by other variables, such as education, marital status, and age (Cleland and Ferry, 1995). Thus there is little support for the hypothesis that sexual life-styles are divided merely across urban-rural lines. Instead, sexual behavior in towns and cities appears culturally linked to sexual behavior in rural areas, and risky behavior is present in both urban and rural areas (Caraël et al., 1994).
Orubuloye et al. (1991) report astonishingly similar levels of multiple partners in rural and urban areas of southwest Nigeria. Rutenberg et al. (1994) report that in Tanzania, single men who were not virgins were far more likely to have multiple partners if they lived in rural areas, but, perhaps because of lower levels of polygyny, married men were more likely to have extramarital partners in town. Anarfi (1993) reports earlier sex in urban than in rural areas of Ghana. In multivariate analysis of DHS data for several sub-Saharan African countries, Meekers (1994) shows little effect of urban/rural residence on age at first intercourse, although when asking retrospective questions in cross-sectional surveys, it is difficult to determine where first sex took place, or if onset of sexual activity might be linked in some way to migration.
Migration
A widening rural-urban gap in income and availability of social services and a subregional variability in development have generated large movements of people in Africa. Increasing urbanization is associated with a lower proportion of customary marriages relative to consensual unions (Caldwell et al., 1989; Orubuloye et al., 1990). Such conjugal situations often weaken the financial security of women and their children. Because migrants are most often young adult men, one outcome of migration is a very high ratio of men to women at the points of destination. Most West and Central African cities (except Abidjan, Côte d'Ivoire) have sex ratios close to parity, in contrast to the situation in East and Southern Africa (see above). In such settings, high sex ratios in favor of men have generated growing demand for commercial sex, which is often satisfied by widowed, divorced, and single women because of their bleak economic situation (Anarfi, 1993). Mining or industrial centers often have particularly high concentrations of young men who have migrated to seek employment; these sites are highly vulnerable to the spread of HIV infection. Lesotho, Swaziland, and several other countries in Southern Africa face the dual challenge of sustaining economies that are largely dependent on their export of labor to South Africa and
reducing the consequent vulnerability of migrant workers and their families to HIV/AIDS (Phits'ane, 1994).
Migration in Africa commonly takes the form of people leaving their villages on a seasonal or temporary basis in search of work, hoping to move back eventually to their place of origin. In this pattern of migration, an infected individual may spread HIV/AIDS to others at both the sending and the receiving ends of the cycle. In Ghana, the risk is heightened in rural areas by a tendency among returning migrants to flaunt wealth and acquire partners (Anarfi, 1993). The same study showed that international migrants are more likely than internal migrants to report high numbers of partners (Anarfi, 1993). Rutenberg et al. (1994) show that migration in the last 3 years (presumably largely within Tanzania, although this implication is not stated) makes no substantial difference in levels of sexual activity.10 The issue of migration as a factor in the spread of HIV/AIDS is discussed in further detail in Chapter 2.
Sexually Transmitted Diseases
As discussed in Chapter 3, there is a strong relationship between STDs and HIV. Lindan et al. (1991) report that HIV infection among women with a history of STDs in the previous 5 years is twice as high as among women with no STD history.
Responses about symptoms of STDs over the last 12 months in the WHO/GPA surveys show a strong correlation between reported risk behavior and venereal infections. In many nations, those reporting STD symptoms are two or three times as likely to report casual sex as those apparently unaffected. The correlation grows stronger as partner numbers increase, and stronger yet with a history of contact with commercial sex workers. Messersmith et al. (1994) report a 12-fold increase in STD history for respondents with five or more lifetime partners and previous contact with a prostitute as compared with those having a single lifetime noncommercial partner.
Treatment (often of both partners) can be crucial in limiting the importance of STDs as a cofactor for HIV transmission. Although high proportions of those reporting STD symptoms in the WHO/GPA survey said they obtained treatment, only half reported telling their regular partner. In Cameroon, one-quarter of STD patients in one study continued sexual relations during their illness, and of those nearly two-thirds stated that they used condoms on every occasion (IRESCO, 1994). Caldwell et al. (1993) assert that much sex in sub-Saharan Africa takes place in the dark without hand-to-genital contact, making it difficult for people to ascertain whether their partner is infected with an STD.
|
10 |
Doubtless other large-scale movements of refugees, such as those associated with famine, civil unrest, and military coups, also contributed to the rapid spread of the epidemic, but such situations rarely lend themselves to careful study (see Chapter 2). |
In a Nigerian study, a sizeable majority of STD sufferers said they had sought treatment in hospitals or with private doctors, though turning to traditional healers and self-medication was not uncommon. In Nigeria, abstention and effective treatment were much more common among women who knew their illness to be sexually transmitted than among those who thought it ''natural" (O'Toole Erwin, 1993).
Where levels of STD-induced sterility are high and the connection between the two is well known, single women may refrain from seeking treatment for fear of being stigmatized and jeopardizing their chances of marriage. The high cost of treatment, lack of available services, and the attitude of the staff toward the client may also be further reasons to deter women from attending STD clinics. In a society where fertility is an all-important key to family support and resources, barrenness may drive women to towns and to commercial sex work (Southall, 1961, cited in Standing and Kisekka, 1989). Where barrenness is the product of chronic or untreated STDs, the implications for HIV transmission are clear.
Circumcision and Traditional Medical Practices
Generally, male circumcision is thought to be protective against HIV transmission and female circumcision a risk factor, although some dispute these claims. Female circumcision continues to be widely practiced among some groups throughout Africa (Kouba and Muasher, 1985). In the most recent DHS in northern Sudan, 86 percent of women aged 15 to 19 were circumcised and/or had experienced infibulation (Ahmed and Kheir, 1992). There have been no studies that have actually attempted to examine the relationship between female circumcision and HIV transmission, although the practice may put women at risk if unsterile instruments are used; it is also likely to increase the risk of bleeding during intercourse and therefore of HIV transmission.
Lack of male circumcision has been associated with some sexually transmitted diseases, including chancroid, syphilis, and gonorrhea (Cook et al., 1994), but there has been a good deal of debate in the recent literature on the link between lack of male circumcision and the risk of HIV infection. On one side, Bongaarts et al. (1989), Moses et al. (1990, 1995), and Caldwell and Caldwell (1993) have argued that there is a statistically significant positive association between estimates of the extent to which ethnic groups in various regions traditionally do not practice circumcision and the prevalence of HIV, so that absence of male circumcision may be a crucial factor in the spread of HIV in Africa. Using micro-level data, Hunter et al. (1994) show in a multivariate analysis that having an uncircumcised partner is a risk factor for seropositivity for women even when other factors, including number of partners, are held constant. Adopting a more cautious tone, others argue that the causal relation is far from proven, and that confounding factors such as behavioral differences may account for these findings (de Vincenzi and Mertens, 1994; Conant, 1995). For instance, a study of
rural Uganda revealed that circumcised men tend to be Moslem traders concentrated in high-prevalence trading towns (Serwadda et al., 1992). Although circumcision is found to be protective, the authors do not investigate whether there are behavioral factors associated with being Moslem that might also be protective. Further research is required to illuminate not only the association between male circumcision status and acquisition of HIV, but also the causal factors and specific mechanisms involved (Mertens and Caraël, 1995).
Alcohol
Drinking is often thought to be associated with lower self-control and greater risk-taking behavior with regard to sex. However, few studies have examined the effects of alcohol consumption on sexual behavior in sub-Saharan Africa, although some income expenditure studies show that a significant portion of disposable income is spent on the consumption of various forms of alcoholic beverages. Bars and nightclubs that sell alcohol are often popular meeting places and are frequented by people looking for commercial or casual sex. Six of the nine WHO/GPA surveys in sub-Saharan Africa included a module on drinking habits (Central African Republic, Côte d'Ivoire, Guinea-Bissau, Lesotho, Tanzania, and Lusaka, Zambia). Analysis of these data established that alcohol consumption is common in these countries and that it is positively associated with risk behavior, even when other factors are held constant (Ferry, 1995b).
In Uganda, alcohol and sexual activity are linked in both commercial and social spheres (Olowo-Freers and Barton, 1992). The brewing of various forms of alcoholic beverages is a major source of cash income for may women, particularly in urban slum areas. The alcohol trade is closely intertwined with commercial sex activity. Many women who make and sell beer are also known as prostitutes (Olowo-Freers and Barton, 1992). In Kampala, beer gardens are popular places for finding casual sexual partners. Drinking is particularly heavy among students and urban slum dwellers. In one study of urban slum dwellers in Kampala, over 60 percent of heads of households drink daily (Kayobosi, 1988, cited in Olowo-Freers and Barton, 1992).
SEXUAL PRACTICES AND BELIEFS
While quantitative studies are useful in defining the incidence of common practices, they will never identify all of the beliefs and practices that, albeit far from universal—indeed sometimes apparently at odds with survey data—may help indicate acceptable interventions with the potential for having some impact on behavior. This section reviews some of the beliefs and practices examined by the literature on sexual behavior in sub-Saharan Africa, particularly qualitative studies.
The Notion That Men Need Sex
It is widely held in sub-Saharan Africa that men have an all-but-insatiable need to copulate (what Anarfi [1993:47] calls "the repetitive and overpowering nature of the sexual appetite in males") and that this need must be satisfied if they are to remain in good health. The idea that retained semen is somehow poisonous and dangerous to health is frequently expressed. Caldwell et al. (1993) state that African cultures hold frequent sex to be healthy and strengthening, and some researchers contend that men measure their health status by their ability to achieve multiple orgasms. Poewe's 1981 study in Zambia (quoted in Standing and Kisekka, 1989) reports the belief that sexual deprivation may cause emaciation and madness.11 In focus groups in Zimbabwe, men and women agreed that men must find a way to release their sexual tensions, and may even be "forced by nature" to rape (Meursing et al., forthcoming), and women immodestly dressed are considered by both sexes to be provoking just such a situation and to deserve what they get (Vos, 1994).
Coercive Sex
Coercive sex or rape is a behavior that no quantitative survey will ever adequately describe. But there is no shortage of evidence that it is present in all societies and even common in some, particularly during periods of intense ethnic conflict. As documented by Orubuloye et al. (1992), 4 percent of Nigerian men reported themselves guilty of rape or coercion at first intercourse, while 3 percent of women in a Ghanaian study reported that they were forced into first sex and a further 8 percent that they were lured or deceived (Anarfi, 1993). Standing and Kisekka (1989) quote many anthropological papers giving accounts of ritual or commonplace violence in marital and sexual relations. The authors also detail rape cases, often involving very young victims.
In a study of the rape of children in Bulawayo, Zimbabwe, Meursing et al. (forthcoming) show a linear rise in reported rape cases in recent years. Over half of the 54 child victims of rape (the youngest 2 years old) referred to central hospitals in the city in the final 6 months of 1992 contracted STDs. Although this high proportion may partly reflect the increased likelihood that a rape resulting in an STD will be reported, the risk for a young girl to be subjected to violent sex must be high in a population where STDs are common. Since STDs are a cofactor for HIV transmission, HIV, too, is a potential consequence of rape.
Health Beliefs
Some women who report knowingly having sex with an STD-infected partner say they did so because of a belief that sex could cure venereal diseases (Awusabo-Asare et al., 1993). This belief apparently extends to AIDS. Blue-collar respondents in Ugandan focus groups reported a belief that frequent sex could diminish the viral load of the HIV-infected. Focus groups in Uganda reported a belief that young girls were "safe"; adolescents reported that infected men bribed young girls for sex or raped them (Konde-Lule, 1993; Obbo, 1993b). In Zimbabwe, female traditional healers reported that their male counterparts sometimes encourage men to have sex with young women (especially family members) to "cleanse" themselves of HIV (Meursing et al., forthcoming).
Dry Sex
There are a number of reasons "dry sex" practices intended to decrease vaginal secretions might be associated with an increased probability of HIV transmission. The insertion of crushed leaves, powders, or mineral infusions into the vagina can lead to tearing, lesions, or inflammation in the vagina, increasing the likelihood of transmission of STDs and HIV. Lesions or inflammation may also mask symptoms of ulcerative or non-ulcerative STDs (Sandala et al., 1995). Dryness alone may lead to abrasive sex and lesions, with the same effect. Finally, strong preferences for dry sex may interfere with condom effectiveness or acceptability of vaginal microbicides (Kisekka, no date; Dallabetta et al., 1995).
Dry sex practices have been reported in many countries in sub-Saharan Africa, including Nigeria, Zaire, Zambia, Malawi, Zimbabwe, and South Africa (see Sandala et al., 1995 and references therein). In one study in Ghana, schoolchildren of both sexes said that they preferred the vagina dry and tight, and most could describe drying agents (Bleek, 1976, quoted in Standing and Kisekka, 1989). The same was also true for older women (but not schoolgirls) in focus groups in Zimbabwe (Vos, 1994). Among some teenagers in Natal, South Africa, wetness is thought to indicate promiscuity (Preston-Whyte, 1994).
In a thorough study in Zaire, men and women alike expressed a preference for a dry, tight vagina during intercourse (Brown et al., 1993). All men and women studied could contribute at least 1 of a total of 30 drying methods spontaneously mentioned, and over two-thirds of the women said that they had used such a method themselves. Although most of the women said that the procedure increased their sexual pleasure, some complained of inflammation and itching. Clinical examination showed that many of the methods had led to lesions or swellings in the vagina.
In Blantyre, Malawi, a study of women attending an antenatal clinic, designed to assess the prevalence of dry sex practices and its association with HIV infection, found that 34 percent of the women had used an intravaginal agent for
treatment of discharge and itching, while 13 percent had used traditional drying agents exclusively for tightening the vagina. The study found that a significantly higher proportion of HIV-infected than uninfected women had used intravaginal agents for treatment purposes, but no difference was found in HIV status among women who used these agents for tightening (Dallabetta et al., 1995). In Lusaka, Zambia, 50 percent of women attending an STD clinic reported having ever engaged in dry sex behavior (Sandala et al., 1995). A variety of practices was reported, including drinking an elixir or "porridge" before having sex. There was no evidence of a strong relationship between these practices and HIV infection (Sandala et al., 1995).
Oral/Anal Sex
Conventional wisdom holds that oral and anal sex are uncommon among most sub-Saharan African groups. However, this belief may reflect the fact that studies rarely investigate levels of nonvaginal sex. IRESCO (1992), studying sexual practices among commercial sex workers and their clients in Cameroon, found that 26 percent of commercial sex workers and 28 percent of their clients reported experience with anal intercourse, while over one-third of men and one-quarter of women in the group reported having experienced oral sex. In focus group studies in Uganda, some heterosexuals said they engaged in anal sex while women were menstruating (Standing and Kisekka, 1989). In a study of 329 women attending an STD clinic in Lusaka, Zambia, 8 percent of women reported ever engaging in anal intercourse (Sandala et al., 1995).
Homosexuality
Although very little sound research appears to have been done on homosexuality in sub-Saharan Africa, its existence is overwhelmingly denied in academic publications. This claim may result because "homosexuality" as a lifelong sexual identity is rare or unknown, rather than because men never have sex with men.
Ahmed and Kheir (1992) report homosexual behavior to be common though clandestine in northern Sudan. The authors express a concern that a recent government crackdown on female commercial sex workers may increase the incidence of homosexual sex, thus perhaps increasing the spread of HIV. Male-with-male sex featured prominently in focus group discussions among the Hausa in Nigeria (Kisekka, no date). Other studies give evidence of homosexual behavior among the Kikuyu in Kenya, the Hausa in Nigeria, and mine-workers in South Africa (Standing and Kisekka, 1989). According to D. Moodie et al. (1988, quoted in Standing and Kisekka, 1989), the mine-workers most likely to have boys acting as "mine-wives," that is, performing domestic and sexual services for them, were Mozambican migrants who also had the highest HIV prevalence.
Postpartum and Other Abstinence
Postpartum abstinence probably evolved simply as a means of birth spacing, but became ritually sanctioned so that it would be maintained. In Bamako and Bobo-Dioulasso, two cities of the Sahel region, the prevailing belief among women interviewed in 1983 was that women must not have sex while they are breastfeeding because the ingestion of semen will spoil the mother's milk (van de Walle and van de Walle, 1991). As was pointed out earlier, it is common for men to seek other partners during the postpartum period; indeed, many researchers believe postpartum abstinence is a principal prop of high levels of sexual networking, and call for the promotion of condoms to breastfeeding women as a means of eliminating the danger of "dirty milk" (e.g., Hogsborg and Aaby, 1992). Anarfi (1993) suggests that a possibly related dynamic is under way in Ghana: women are limiting their postpartum abstinence in an attempt to keep husbands from seeking other sexual partners. He reports an average of 12.4 months of abstinence in Ghana, where, he says, the taboo period was much longer in the past.12 Half of the women in his sample reported contraceptive use, versus a national average of 13 percent among currently married women (Ghana Statistical Office and IRD/Macro Systems, 1989). However, repeated surveys sometimes contradict the conventional wisdom that postpartum abstinence is everywhere on the wane. In Cameroon, the average length of postpartum abstinence remained at 13.9 months between 1978 and 1991 according to WFS and DHS data, while in Kenya the mean number of months rose from 2.9 in 1977/78 to 5.9 in 1989. The median length of postpartum abstinence measured by the 1993 DHS in Kenya was 3.0 months (Figure 4-1).
Couples may abstain from sex for other reasons, such as during a woman's menstrual period or in times of mourning. Researchers report that in some contexts, the definition of "abstinence" may be flexible, extending to situations that include sleeping with a person only on a single occasion. Such misconceptions, if common, would diminish health educator's recommendation of "abstinence" as a protection against HIV/AIDS.
Levirate Marriage
Standing and Kisekka (1989) report that passing on wives to the brothers or family members of dead husbands remains common in some societies, particularly
in Uganda (see also Olowo-Freers and Barton, 1992). The practice also remains quite common in parts of West Africa. In East African patrilineal societies, such as the Masai, Nandi, Kikuyu, Kisii, and Meru in Kenya, widow-inheritance used to be the rule, and widows had limited rights of appeal (Lesthaeghe, 1989). Nowadays, widows often have more choice in the matter (Lesthaeghe, 1989; Olowo-Freers and Barton, 1992). They may choose among the potential heirs or even choose not to remarry at all (Olowo-Freers and Barton, 1992).
AIDS AWARENESS
Almost all studies report a very high awareness of the existence of HIV/AIDS, with the WHO/GPA surveys recording that over 9 out of 10 people know of the disease everywhere except Francophone West Africa (Table 4-5). The lowest awareness recorded in any study was in Togo, where just under two-thirds of respondents had heard of AIDS, and where the sex differential in knowledge was also greatest. In multivariate analysis, media exposure and education appeared as major predictors of AIDS awareness. Controlling for education diminished the independent effect of age. This section reviews levels of AIDS awareness with respect to the specific issues of modes of transmission, asymptomatic transmission, severity and perceived threat, attitudes toward sufferers, and testing.
Modes of Transmission
Most studies concur that among those aware of AIDS, the overwhelming majority are aware of actual modes of transmission and genuine risk behaviors (Irwin et al., 1991; Lindan et al., 1991; Hogsborg and Aaby, 1992; Messersmith et al., 1994). In most sub-Saharan Africa WHO/GPA surveys, sex with prostitutes was recognized as risky by over 90 percent of those respondents who were aware of AIDS, although in Guinea-Bissau, nearly 3 in 10 respondents did not think of the practice as dangerous (Ingham, 1995). However, in a Nigerian study reporting very high awareness of sexual transmission, just 29 percent of women and 17 percent of men mentioned the route of sex with prostitutes spontaneously (Messersmith et al., 1994). The suggestion here of deliberate denial—especially in this case by men who were broadly more educated and aware than women—was reinforced in the same study by the sex differentials in answers to questions about prevention. Of those who knew of AIDS, women were nearly twice as likely as men to mention condom use and avoidance of sex workers, and were also slightly more likely to mention partner reduction. Men who had a history of contact with sex workers were less likely than those who did not to regard sex workers as a source of danger, and the proportion of men saying fewer partners could reduce the risk of HIV infection fell as their number of partners over the
TABLE 4-5 Awareness of AIDS and Accuracy of Knowledge of Suggested Routes of Transmission
|
|
Percent Aware of AIDS |
Among Those Aware of AIDS, Percent Responding Accurately on Routes of Transmission |
|||||
|
Study area |
Male |
Female |
Prostitute (Yes) |
Touch (No) |
Mosquito (No) |
Vertical (Yes) |
Curable (No) |
|
Burundia |
96 |
|
94 |
77 |
38 |
89 |
97 |
|
CAR |
87 |
78 |
93 |
60 |
26 |
78 |
95 |
|
Côte d'Ivoire |
94 |
86 |
n.a. |
51 |
23 |
n.a. |
n.a. |
|
Guinea-Bissau |
77 |
72 |
69 |
45 |
71 |
86 |
84 |
|
Kenya |
90 |
89 |
78 |
75 |
51 |
68 |
95 |
|
Lesothoa |
98 |
|
93 |
67 |
n.a. |
86 |
83 |
|
Tanzaniaa |
96 |
|
92 |
66 |
41 |
81 |
97 |
|
Togo |
73 |
56 |
92 |
40 |
11 |
80 |
71 |
|
Lusaka, Zambiaa |
98 |
|
77 |
88 |
n.a. |
88 |
93 |
|
a Both sexes. Prostitute = having sex with a prostitute Touch = touching someone with AIDS Vertical = mother-to-child transmission Mosquito = transmitted by mosquito bite Curable = AIDS is curable CAR = Central African Republic n.a. = not available SOURCE: Cleland and Ferry (1995). |
|||||||
last years rose. Moreover, in every survey, respondents demonstrated a high propensity to respond positively to questions on biomedically erroneous modes of transmission, and even to report spontaneously that HIV could be transmitted, for example, by the wind or by eating chicken (Messersmith et al., 1994).
In a regression analysis of WHO/GPA survey data, education was the strongest predictor of accuracy about ways of contracting HIV, both correct and incorrect. Despite fears that a belief in casual transmission will act as a disincentive to protect oneself from contracting HIV sexually, such erroneous beliefs do not seem to be independently associated with a lack of behavior change.
Asymptomatic Transmission
Some investigators report that local concepts of disease may not encompass the idea of a healthy carrier (Irwin et al., 1991; Hogsborg and Aaby, 1992). Among women questioned by Lindan et al. (1991), 70 percent believed that everyone infected with HIV was clinically ill, and one in five thought one could tell if someone was seropositive by looking at him or her. A study of AIDS-related knowledge in Zimbabwe, undertaken in 1994, revealed that while virtually all Zimbabwean men and women have heard of AIDS, 15 percent of men and 26 percent of women do not believe that a healthy-looking person can carry the AIDS virus (Central Statistical Office [Zimbabwe] and Macro International Inc., 1995). It is surprising, then, to find such high levels of awareness of asymptomatic transmission among respondents to the WHO/GPA surveys. This awareness, however, may be more apparent than real as a result of bias in the question.13
Severity and Perceived Threat
Although most people who know of AIDS consider it a dangerous disease, a substantial proportion believe it is curable. This is the case even in countries such as Lesotho, where there is broad access to AIDS information. In Kigali, Rwanda, one of the highest HIV-prevalence areas in the world, over one-third of women said they thought AIDS was curable or possibly curable (Lindan et al., 1991), while in Zaire, the vast majority of subjects in a study of factory workers said they thought a cure was available (Irwin et al., 1991). The WHO/GPA surveys show that high proportions of those who think most people infected with AIDS will die of it also think that a cure is available, presumably because most people will not be able to get access to it.
A large proportion of respondents in most WHO/GPA survey countries spontaneously mentioned AIDS as a major health threat to both the world and their nation. Some respondents thought the problem less pressing in their own regions. High proportions in Guinea-Bissau and Burundi said AIDS was a national threat, but only around 1 person in 10 in those countries thought it an immediate threat to his or her community, although more thought the danger would grow over the next few years. Respondents in some heavily afflicted areas (e.g., Tanzania and Lusaka, Zambia), though very much aware of the immediate threat AIDS poses to their community, appeared not to fully understand the implications of the epidemic; lower proportions saw it as a medium-term rather than a current concern.
Such optimism is unlikely to be warranted. People's perceptions may change rapidly once vaccine trials begin. It is possible that a mass vaccination campaign would induce negative changes in risk behavior. In particular, there is concern that those vaccinated would believe themselves to be at reduced risk of acquiring HIV, and consequently increase their rate of acquisition of new partners or decrease their use of condoms (Lurie et al., 1994; Chesney et al., 1995).
What emerges from these responses is that ordinary people are genuinely concerned about AIDS as a public health problem. Those governments concerned with the opinions of their citizens would appear to have nothing to lose and much to gain by putting the epidemic high on their national agendas.
Beyond the public threat, to what extent do individuals feel they themselves are at risk? Here expected relationships fail to emerge. To return to a point made earlier, we might expect, assuming an understanding of HIV transmission and accurate reporting, to find that people with several partners feel themselves most at risk. The WHO/GPA data show that this expectation often does not hold. In Francophone countries, for example, many people who reported no intercourse for 12 months still felt themselves to be at risk. Only in Lusaka, Zambia, did a clear majority of respondents say they did not consider themselves to be at risk of contracting HIV. This majority included half of the men who reported five or more casual sex partners. Nonusers of condoms with "commercial" sex partners also frequently reported that they felt in no danger of infection.
These discrepancies cannot be neatly reconciled by pointing to erroneous beliefs about modes of transmission. In multivariate analysis, belief in casual transmission was associated with higher perceived risk only among men in Lusaka, Zambia, and women in Côte d'Ivoire. That finding might explain why women in Côte d'Ivoire who were apparently not at risk perceived that they were, but it does not explain why men in Lusaka who did report high-risk behavior felt safe.
In sites surveyed under the auspices of WHO/GPA, there were few differences between men and women in perceived personal vulnerability to HIV infection. Multivariate analysis of a subset of these surveys showed that marital status was related to perceived personal risk for women, but not for men. In two surveys, married women reported significantly higher risk than unmarried women, and in the third the difference was in the same direction, though not significant. However, in a study of sexually active women in Kigali, Rwanda, 84 percent of women who lived alone felt at risk of HIV infection, as compared with just one-quarter of monogamously married women (Lindan et al., 1991). In fact, this was exactly the fraction of monogamously married women that turned out to be seropositive, a potent reminder that women are probably more at risk from their partner's behavior than from their own. That awareness is evident from the responses of women living with men who had other wives: 9 in 10 felt at risk of infection.
Even in high-prevalence Kigali, Rwanda, 56 percent of women reporting at
least one factor shown in the HIV-seropositivity study to be an HIV/AIDS risk still thought themselves to be in no danger of contracting the disease. Astonishingly, the WHO/GPA surveys showed that proportions feeling themselves vulnerable to the disease were generally much lower in the higher-prevalence areas of East and central Southern Africa than in lower-prevalence West Africa.
Perhaps the explanation for the weak links between behavior and risk perception can be found in Hogsborg and Aaby (1992). Respondents reporting feelings of vulnerability in that study were also liable to report that ''it depends on God." This fatalism was taken one step further by focus group participants who were aware of modes of transmission and risk reduction. Kisekka (no date) and Obbo (1993a) report that the sentiment "after all, you have to die of something" has become a common justification for continued high-risk behavior. 14
Attitudes Toward Sufferers
In heavily affected Rakai district, Uganda, Konde-Lule (1993) found that AIDS patients were little stigmatized except by adolescents, who thought that since the means of transmission were known, people had only themselves to blame if they fell ill. This feeling was among the most sympathetic attitudes expressed elsewhere, however. Factory workers in Kinshasa, Zaire, stated that anyone known to be HIV-positive would be shunned by his or her neighbors (Irwin et al., 1991), while many respondents in the WHO/GPA survey in the Central African Republic thought AIDS patients deserved no care, and nearly one in five stated flatly that they should be killed. Anarfi (1993) found similar sentiments in Ghana: "The general opinion is that sufferers of the disease must be killed or at best confined" (Anarfi, 1993:65).
The extent of variation even within countries is illustrated in two reports on AIDS from different regions of Tanzania. Kaijage (1994a:15) states that in Kagera, AIDS stigmatization is declining:
Although the problems raised above are still fairly widespread, denial and stigma are less prevalent now than they used to be in the earlier days of the epidemic. … [A]lmost every family, especially in Bukoba, Muleba, and to some extend Karagwe, has been affected by AIDS. People are therefore generally more sympathetic to persons with AIDS (PWAs) than used to be the case. And, for a PWA in Kagera, having AIDS is no longer such a peculiar experience. AIDS is less a disease of shame than it used to be. It is now euphemistically referred to as "this disease," which suggests familiarity with it.
|
14 |
See also Chapter 5 for further discussion of the underreaction to the AIDS epidemic. |
However, Kaijage (1994b:14) comments as follows about Arusha:
Stigmatization of AIDS patients in Arusha is far worse than it is in Kagera. The reason is that the disease is not so prevalent in Arusha, and lots of myths still surround it.
Testing
If some of the attitudes described above are indeed common, there is a real risk that HIV/AIDS will be driven underground, and its spread will become yet more difficult to control. One might expect the above rather harsh views on HIV/AIDS-infected individuals to translate into a reluctance to be tested, or at any rate a desire not to have test results known. Surprisingly, the WHO/GPA surveys indicate no such fear of testing. Around 90 percent of respondents in all areas except Lusaka, Zambia, said they would undergo testing and would want to know the results, and the vast majority also said they would want their families to know the results.
Similar responses were found in another survey in Guinea-Bissau (Hogsborg and Aaby, 1992), but the authors observe that the professed willingness to share information with partners was at odds with actual behavior. In a serosurvey in the same area, all people testing positive were invited to bring their partners back for free counseling. Not one did. The likelihood that survey results reflect what respondents feel to be the "correct" answer rather than the truth is supported by focus group discussions. While participants in Zaire said they would want to know test results, many men said they would not want their wives or partners to be told (Irwin et al., 1991). In Uganda, the majority of those discussing the issue said flatly that they did not want to know their HIV status (Konde-Lule, 1993). And in a recent study of female partners of AIDS patients in a hospital in Kampala, Uganda, only 12 percent of women correctly identified their husbands' diagnosis as "slim" or AIDS (Baingana et al., 1995). Most women (54 percent) thought that the disease was tuberculosis. Others thought that it was some other disease or simply did not know. Furthermore, although just over half of the women felt that they needed to be tested for HIV, only 5 percent had actually done so at the time of the survey (Baingana et al., 1995).
THE ROLE OF CONDOMS
Knowledge of condoms varies widely both across countries and, in many surveys, between the sexes.15 More men than women knew of condoms in every country surveyed by WHO/GPA, a disparity that remains even after holding
media exposure, education, and residence constant. Of those who said they knew of condoms (including answering affirmatively to prompting), a high proportion could not say where they might be obtained. In the WHO/GPA surveys, a maximum of 38 percent (males, Côte d'Ivoire) knew of a source and lived or worked within 30 minutes of it.
Some surveys have found that people's declared knowledge of condoms depends on the context of the questioning. Messersmith et al. (1994) report that in their study of sexual behavior and condom use in Ile-Ife, Nigeria, condoms were known as a means of family planning by more people of both sexes than as a means of protecting against STD transmission, although more actually used condoms for the latter purpose.
Condom Use
Perhaps the same dynamic is at work with reports of condom use: people asked in the context of STD prevention whether they have ever used condoms may underreport their use as contraceptives. Condom social marketing projects in many African countries have been remarkably successful in the recent past, and the number of condoms sold has increased dramatically (see Chapter 5). Nevertheless, it is clear from all surveys (including the fertility-based DHS series) that use of condoms is still low throughout sub-Saharan Africa (Tables 4-6A and 4-6B).
In multivariate analysis of WHO/GPA data, age is negatively related to condom use, while use rises with both education and level of risk behavior. However, knowing that HIV is transmitted sexually and feeling personally vulnerable to infection16 are not associated with condom use. Messersmith et al. (1994) confirm the negative correlation with age and the positive correlation with risk behavior (including contact with sex workers). They show a linear rise in condom use with the number of lifetime partners. They also show positive associations with knowledge of AIDS and a history of STDs. Using DHS data for Tanzania, Rutenberg et al. (1994) show that although condom use is scanty, it is concentrated among those with multiple partners.
Although around one-quarter of men reporting "commercial" sex in Burundi and Lusaka, Zambia, claim always to use a condom in such encounters, proportions recorded in the other WHO/GPA surveys are far lower. A consistently higher proportion of women than men reporting "commercial" sex said they never used a condom. These women are not likely to be full-time sex workers. A study of just such women in The Gambia (to whom condoms are freely distributed)
TABLE 4-6A Percentage of Sexually Active Men Who Have Ever Used Condoms
|
Age |
Burundi |
CAR |
Côte d'Ivoire |
Guinea-Bissau |
Kenya |
Lesotho |
Tanzania |
Togo |
Lusaka, Zambia |
|
15-19 |
18 |
34 |
42 |
46 |
10 |
23 |
14 |
9 |
55 |
|
20-24 |
29 |
34 |
45 |
50 |
28 |
17 |
11 |
18 |
59 |
|
25-39 |
21 |
16 |
33 |
47 |
18 |
19 |
17 |
17 |
38 |
|
40-49 |
9 |
11 |
13 |
20 |
17 |
19 |
12 |
12 |
15 |
|
50+ |
n.a. |
12 |
3 |
7 |
2 |
9 |
10 |
12 |
3 |
|
All |
18.5 |
21.0 |
30.3 |
33.0 |
16.4 |
16.1 |
14.0 |
14.8 |
36.3 |
|
n.a. = not available CAR = Central African Republic SOURCE: Cleland and Ferry (1995). |
|||||||||
TABLE 4-6B Percentage of Sexually Active Women Who Have Ever Used Condoms
|
Age |
Burundi |
CAR |
Côte d'Ivoire |
Guinea-Bissau |
Kenya |
Lesotho |
Tanzania |
Togo |
Lusaka, Zambia |
|
15-19 |
11 |
10 |
16 |
21 |
11 |
9 |
5 |
8 |
31 |
|
20-24 |
10 |
8 |
15 |
11 |
12 |
7 |
10 |
9 |
29 |
|
25-39 |
8 |
5 |
7 |
14 |
9 |
10 |
10 |
6 |
20 |
|
40-49 |
4 |
3 |
1 |
4 |
6 |
5 |
8 |
2 |
14 |
|
50+ |
n.a. |
n.a. |
n.a. |
n.a. |
3 |
5 |
2 |
3 |
n.a. |
|
All |
7.3 |
6.8 |
9.3 |
12.3 |
8.7 |
8.0 |
8.5 |
5.9 |
24.2 |
|
n.a. = not available CAR = Central African Republic SOURCE: Cleland and Ferry (1995). |
|||||||||
gives limited grounds for hope (Pickering et al., 1992). Although in urban areas women reported using condoms with four clients out of five (a higher rate than that reported by the clients themselves), condom use fell as the number of clients per woman rose. At peak periods such as holidays, when women were recording over 11 clients a night, condom use fell below 50 percent (Pickering et al., 1992).
Condoms and STD and HIV Prevention
Notwithstanding Messersmith's finding that more people knew of condoms as a contraceptive, a substantial majority also knew of their properties in preventing STDs. The proportions of the latter were highest for single men and for single and separated women. Even in multivariate analysis, men with five or more partners were far more likely than those with fewer partners to know that condoms could prevent STD transmission. The number of partners was not an independent predictor of that knowledge in women (Messersmith et al., 1994).
For both sexes, there was a strong correlation between those who had heard of AIDS and those who knew that condoms could prevent the spread of STDs. This result is not, however, necessarily a cause for great optimism. A range of studies show that if a person knows of AIDS, knows that it is sexually transmitted, and knows that condoms can protect against STDs, it does not seem to follow that he or she will also believe that condoms protect against HIV. Indeed, the STD connection may be a dangerous one. Kisekka (no date) notes that commercial sex workers in Nigeria dismiss the need to adopt condoms because they already self-medicate to protect themselves from STDs. In fact, fewer than half of those who reported knowing of condoms in the WHO/GPA surveys in all the countries except Guinea-Bissau believed condoms were effective in preventing HIV transmission. In focus groups, people frequently scoffed at the idea that something as flimsy as a condom could protect against a disease as deadly as AIDS (Irwin et al., 1991; Konde-Lule, 1993; Kisekka, no date). Orubuloye et al. (1991) report that in Nigeria this view was common even among bar girls. It is worth considering whether this perception arises from overkill in AIDS awareness campaigns. Virologists have shown that HIV is not very infectious; while it is important to stress that, once contracted, AIDS is lethal, it would be wrong to suggest that it is all-powerful and cannot be kept at bay by fairly simple precautions.
Attitudes Toward Condoms
In strongly pronatalist societies, the fact that condoms prevent conception may weigh heavily against their use to prevent transmission of STDs and HIV/AIDS. Other barriers to condom use, expressed both in surveys and more clearly in qualitative studies, are rife. The single most common feeling expressed was
that condoms reduce sexual pleasure. Both sexes surveyed in WHO/GPA study areas were more likely to say that condoms made sex less enjoyable if they had used them than if they had no experience of condom use. In all countries but one, over half of all men who had ever used a condom said doing so made sex less fun (Mehryar, 1995). The exception was Lesotho, the country with the highest prevalence of condom use among those who had ever heard of the device.17 Annoyances such as the interruption of spontaneity, especially among those professing a habit of serial ejaculation, and the problem of disposal contributed to a distaste for condom use (Konde-Lule, 1993; Kisekka, no date; Preston-Whyte, 1994).
There is a general association of condoms with prostitutes and promiscuity (possibly engendered by AIDS awareness campaigns). Both men and women say that asking a partner to use a condom is tantamount to admitting one's own promiscuity or accusing one's partner of sleeping around (Irwin et al., 1991; Hogsborg and Aaby, 1992; Kisekka, no date; Preston-Whyte, 1994). Konde-Lule (1993) reports that some bar girls in Uganda said they were loath to suggest condom use for fear of getting a reputation as a prostitute. Although reports of condom use with "commercial" partners were infrequent in the WHO/GPA surveys, over three-quarters of men who reported ever using condoms said they thought them appropriate for casual partners (Figure 4-4A). Women with a history of condom use and male respondents who knew of condoms but had never tried them were only slightly less likely to agree. Not surprisingly, the percentage of people reporting that condoms were suitable for use within marriage or a regular partnership was correspondingly low, not rising much higher than one-third of male condom users; the exception was Lesotho, where over three-quarters of respondents were happy to use condoms with their wives (Figure 4-4A). Those who had never used condoms were consistently less likely to think use with a regular partner appropriate.
Women did not differ substantially from men in their views except in Togo and Burundi, where female users (Figure 4-4B) and nonusers were both substantially more willing than men to contemplate condom use with their spouses. However, women in Togo were also far more likely than men to think that their regular partners would be offended by condom use; in all other study areas, men were more likely than women to think condom use would offend their partners. The results suggest that there is substantial lack of communication between regular partners on the issue of condom use.
Some people also reported in group discussions that they believed condom use might encourage promiscuity, especially among the young (Irwin et al., 1991;
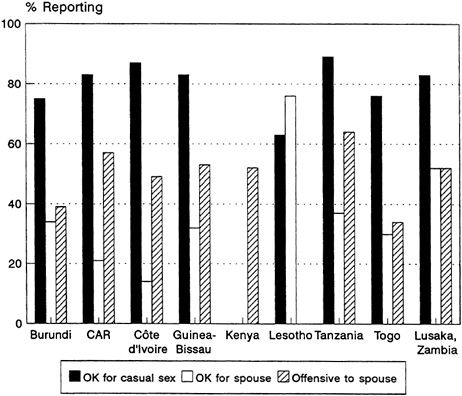
FIGURE 4-4A Attitudes Toward Condoms Among Men Who Have Used Them.
SOURCE: Cleland and Ferry (1995).
Preston-Whyte, 1994). It will be important to address these concerns when designing socially and politically acceptable programs targeted at adolescents.
Concerns over the safety of condoms, particularly for women, surfaced in study after study (Irwin et al., 1991; Lindan et al., 1991; Kisekka, no date; Hogsborg and Aaby, 1992; Konde-Lule, 1993). In focus groups, people frequently tell the story of a friend or local woman known to have died because of a wayward condom. The WHO/GPA surveys showed that a high proportion of people who had used condoms still believed they could "climb up into the womb or stomach." In Côte d'Ivoire, for instance, 61 percent of condom users believed this myth, while in Togo the figure was 46 percent (Mehryar, 1995). Orubuloye et al. (1991:71) report that in Ekiti district in Nigeria, "many believe they [condoms] are as dangerous as AIDS."
Erroneous health concerns aside, the social stress on fertility and the consequent quest for pregnancy can be important in determining women's propensity to disdain condoms. In areas where STDs are common, women may have to choose between not using condoms and exposing themselves to STDs (and
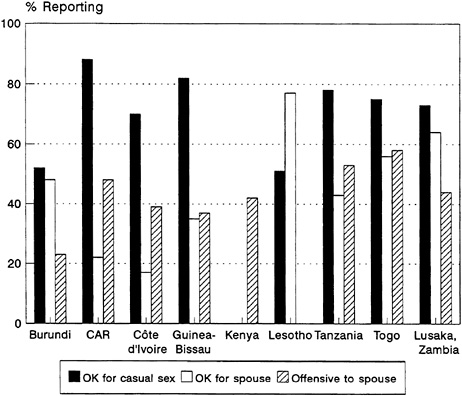
FIGURE 4-4B Attitudes Toward Condoms Among Women Who Have Used Them.
SOURCE: Cleland and Ferry (1995).
thereby the possibility of sterility) or using condoms and foregoing the chance of pregnancy in the short term (O'Toole Erwin, 1993; Preston-Whyte, 1994).
Obviously, condoms are useful only if they are within people's means. In the WHO/GPA surveys, cost was considered a barrier to regular use by fewer than one-quarter of men who had ever used them, except in Côte d'Ivoire, where two-fifths thought them too expensive. In most study areas, female users were slightly more likely than men to consider regular use financially out of reach; this differential may be a reflection on women's relatively lower earning power in the areas in question. In Rakai district, Uganda, the availability and affordability of condoms have been shown in four annual surveys to have little effect on the decision to use them (Kivumbi, 1993).
BEHAVIOR CHANGE
As this chapter demonstrates, measuring sexual behavior is no straightforward matter and is a science in its infancy. Without a large body of evidence
accumulated by measuring current behavior over several years, it is almost impossible to determine what changes have taken place.
The WHO/GPA surveys represent a step in establishing such a body of evidence. Although they do include questions on changes in behavior, single-round cross-sectional surveys are singularly inappropriate for establishing the causality of any changes that may have taken place in the past. Given that the section on behavior change in the WHO/GPA surveys comes after a long section focusing on the threats and dangers of AIDS, replies are quite likely to reflect what respondents perceive the interviewers want to hear. That said, the answers may give some indication of the types of behavioral change that people consider most plausible.
Over half of all men in every country surveyed by WHO/GPA (and up to 90 percent in the Central African Republic and 70 percent in Côte d'Ivoire) reported having changed their sexual behavior in response to the HIV/AIDS epidemic. Women reported lower levels of change in all populations but Lesotho. No clear link emerges between a sense of personal vulnerability and reported behavior change. Cleland (1995) maintains that risk reduction is usually incomplete, so some risk behavior will remain, and a positive correlation should be expected. It might equally be argued, however, that people would bother to reduce their risk behavior only if they thought doing so would be effective and would in consequence feel less vulnerable. The survey data show a positive correlation between risk behavior and reported risk reduction over the last 12 months. If this association were interpreted as a change from previous higher levels of sexual activity to a level still considered high risk in the survey classification, it would provide support for Cleland's hypothesis. An alternative explanation of the empirical evidence might be that behavior changed very recently and was thus not fully captured in the 12-month reference period.
Of behavior changes reported, few were related to casual transmission beliefs, with reduction of partners the most frequently reported measure. Nowhere except Guinea-Bissau was condom use reported as a specific change by more than 7 percent of those who reported any change.18 However, some of these respondents had reported earlier in the survey that they had never used a condom. Certainly the level of potentially effective behavior change reported is not reflected in other markers of safer sexual activity, such as a decrease in the prevalence of STDs.
In-depth interviews conducted in Guinea-Bissau revealed that only two of seven men who had reported in surveys that they had started using condoms because of AIDS turned out to have done so (Hogsborg and Aaby, 1992). The
researchers further reported that men who said they would use condoms with casual partners did not in fact do so, explaining in each case that the circumstances were special because the woman was respectable. The researchers concluded that focusing campaigns on condom use with unknown partners who are assumed to be strangers is useless in a context in which people do not consider any partners to be unknown.
In focus group interviews conducted in Rakai district, Uganda, after several years of vigorous campaigns to promote AIDS awareness and behavior change, people in rural areas did believe that risky sexual activity was on the wane. Optimists might think this finding reflects a new, lower-level, post-AIDS norm. In urban areas, however, people thought their neighbors were just as active as ever but more discreet, a change that might also translate into an increasing tendency to underreport the numbers of partners in surveys (Konde-Lule, 1993). Adolescent groups were especially unlikely to think sexual activity had diminished. Working in the same area, Obbo (1993b) reports an interesting attempt to ''map" sexual networks.19 The work shows that even if people reduce their partner numbers to a small band of people they know well, such as old classmates, they are still at considerable risk of infection. Of 15 people in two interlinked urban networks in 1989, only 2 had survived by 1992.
The failure of awareness programs and interventions to effect more substantial change in condom use should be judged in context. Despite initial willingness among adolescents in Durban, South Africa, to try condoms with their partners, few had positive experiences, challenging widely held notions of male sexual prowess, love, and accepted patterns of interpersonal communication between the sexes (Preston-Whyte, 1994). In a culture where condoms are uncommon and have a rather sordid image, such an outcome is hardly surprising.
Focus groups illuminate the frightening possibility that behavior change may be in the wrong direction. An overwhelming majority of schoolchildren involved in an essay-writing exercise in Uganda thought it likely that those who found out they were seropositive would deliberately go out and spread the disease (Obbo, 1993a). Konde-Lule (1993) reports similar findings, and IRESCO (1995) describes the same dynamic in relation to STDs in Cameroon.
Authors frequently observe that knowing how to reduce risk effectively is not in itself enough to change behavior; people must have the power to make the required changes. Ulin (1992) suggests that the failure of AIDS campaigns to recognize this fact can be fatal to their impact. The WHO/GPA surveys attempted to determine how "empowered" people felt by asking whether they believed AIDS could be avoided by behavior change. Consistently high proportions
of those who had heard of AIDS said yes. However, since the question was asked impersonally, a positive response does not tell us whether people felt they were in a position to make those changes themselves, much less whether they felt able to urge changes on their partners.
In the HIV/AIDS literature, the discussion of power within a relationship usually turns on women's ability to refuse sex or enforce condom use. Women may have more chance of taking either action where a strong tradition of postpartum abstinence allows them to refuse sex at certain times, such as in West African societies, where a woman can rely on her natal kin for support if her insistence on behavior change results in the breakdown of the relationship (Awusabo-Asare et al., 1993; Orubuloye et al., 1993; O'Toole Erwin, 1993). Women are often in a fairly strong position to refuse sex with regular partners if they know their partner has contracted an STD, but attempts to "punish" men for infidelity are viewed with less sympathy. For instance, for women in Zambia, a husband's infidelity is not grounds for divorce, but women can and do seek divorce if they contract an STD from their husbands (Parapart, 1988, quoted in Standing and Kisekka, 1989). Women who rely on sex or sexual attachments for all or most of their income are among those who have least leverage over their partners. If they are commercial sex workers, they are also those most frequently exposed to the risk of infection.
CONCLUSIONS
What, then, have we learned from the WHO/GPA surveys and other work on sexual behavior in sub-Saharan Africa, and what are the implications? The following conclusions can be drawn:
-
There is considerable diversity among African countries in reports of nonmarital sex.
-
Multiple partnerships remain common, and marriages are in many places inherently unstable. A high proportion of regular partnerships are noncohabiting, even at older ages; noncohabitation is associated with casual sexual contacts.
-
While there is generally more casual sex occurring in towns and cities than in villages, levels of sexual activity are remarkably similar across the urban/rural divide in a given country, and rural areas should not be neglected in planning campaigns to arrest the spread of HIV.
-
AIDS is widely known and feared, and governments should not assume they will encounter opposition if they put the issue high on the national agenda.
-
People know that HIV is sexually transmitted, but many still believe that mosquitoes and social contact can spread the disease as well. The concept of infection by an apparently healthy person is poorly understood and should be stressed in educational campaigns.
-
From the point of view of program planners, health beliefs fall into three categories: those that are likely to prove supportive to interventions and behavior
-
change, those that are merely benign or neutral, and those that are dangerous. An example of this last category is the belief that links sex with a "cleansing" of sexual diseases. If such views are determined to be common, ways must be found of eroding them without spreading them further through suggestion.
-
Levels of condom use are low and access is limited in many countries, although this picture is changing rapidly across the continent as governments and international organizations commit more resources to social marketing, family planning, and the control of STDs. Where condoms are known, their image is often still poor, sometimes for reasons that are inherent to the product and sometimes based on misconceptions. One of the most common of the latter, that condoms are dangerous to women, should be urgently redressed.
-
AIDS awareness campaigns have focused on use of condoms with strangers and casual partners. This focus may jeopardize their use with regular partners, as well as with acquaintances who may belong to high-risk groups.
-
There is no shortage of evidence that coercive sex, including rape, takes place and that schoolgirls are especially likely to be victims. As a human rights issue, this should stand alone; in areas where STDs and HIV/AIDS are prevalent, it is also a public health issue. Work should be initiated to determine the magnitude of the problem and address the forces that promote it, including silence.20
-
Women consistently report fewer sexual partners than do men. Ways must be devised of discovering whether this discrepancy is the result of normative underreporting; if so, alternatives to survey methods of data collection for quantification of women's sexual activity must be developed.
RECOMMENDATIONS
The discussion in this chapter and the conclusions offered above lead to the following recommendations for future research related to sexual behavior and HIV/AIDS.
Recommendation 4-1. Research on sexual networks is critical.
Population-based research is needed to collect and analyze data on both the variables that describe individual sexual behavior and the possible socioeconomic determinants of the decision to have sex with a new partner or forgo protection. Since the details of interconnected sexual networks are difficult to
deduce from the answers to individual questionnaires, there is also an important role for social network research.
Recommendation 4-2. Researchers need to develop more reliable ways of collecting information on sexual behavior and to find ways of testing its validity.
There appears to be a much greater willingness to report sexual behavior than was believed until recently, but this field of research requires sensitivity. The challenge is to develop definitions and appropriate vocabulary, such as for categories of relationships, that are both specific enough to be clear to respondents and generalizable enough to be useful to analysts and program planners. The challenge is likely to grow as information about high-risk behavior spreads, increasing the likelihood that respondents will seek to give the "right" answers on questionnaires and in interviews. Hybrid research strategies involving both qualitative and quantitative approaches are essential. Where appropriate, and when both privacy and confidentiality can be ensured, biological markers of sexual activity (such as HIV or STD status) should periodically be incorporated into behavioral surveys to allow assessment of the validity of questionnaire responses and the extent to which the latter provide adequate information on risk.
Recommendation 4-3. Research is needed on patterns of sexual initiation and on the formation of sexual norms and attitudes.
The sexual habits of a lifetime may well be influenced by a socialization process that starts at or before puberty, often before sexual activity begins. A better understanding of the early influences on sexual norms and attitudes and of patterns of sexual initiation may prove essential to promoting safer behavior. For this recommended research to be successful, studies must include children and prepubescent youths, as well as sexually active adolescents and their partners. Recognition that sexuality is socially constructed and changing rapidly is essential to broadening the research agenda and improving interventions.
Recommendation 4-4. More work is needed to clarify the frequency of specific sexual practices.
Because the epidemic in sub-Saharan Africa is being sustained by heterosexual transmission, information on sexual behavior is needed to help develop more effective prevention strategies, as well as to provide baseline data to evaluate their effectiveness. Specific sexual practices—dry sex, oral sex, and anal sex being but a few examples—may impede the success of particular interventions,
yet information about such practices is necessary for encouraging behavioral change.
Recommendation 4-5. Research on coercive sex, especially among adolescents, is critical.
The magnitude of the problem of coercive sex is all but unknown, as are the circumstances under which forced sex or rape takes place. How frequently does it happen and why? Do the aggressors or the victims share characteristics that might suggest a path for preventive or protective interventions? Research on community attitudes, mores, and gender expectations that may serve to encourage or inhibit coercive sex is urgently needed in order to determine how to enlist community support for the curtailment of such practices.
Recommendation 4-6. Research aimed at achieving a better understanding of perceptions about the dual roles of condoms is required.
Condoms help prevent the spread of HIV/AIDS; they also prevent pregnancy. How aware are people of these dual roles, and what weight do they give each when deciding whether to use condoms? How often are these roles in concord and how often in conflict? Do partners discuss this issue, and if so, what are the negotiating mechanisms used?
Recommendation 4-7. Research on attitudes and beliefs about and behavioral responses to sexually transmitted diseases is required.
To develop effective strategies for the treatment of STDs, understanding is needed about social and cultural responses to STDs, including stigmatization. Much more knowledge about the health-seeking behaviors of people infected with STDs, and whether their sexual habits are altered by knowledge of infection, is also needed.
Recommendation 4-8. Research on acceptance of and behavioral responses to HIV vaccination is urgently needed.
Because vaccine trials are likely to begin with vaccines of limited efficacy, there is an urgent need to learn whether individuals who are vaccinated increase their exposure to HIV through riskier behavior, and if so, to determine how to mitigate this response.


















































