
CHAPTER 3
Health Status and Adjustment
The health of children in immigrant families and the extentto which they adapt successfully to American society are very broad topics. Because few surveys or health monitoring systems in the United States use a generational perspective to distinguish among foreign-born children, U.S.-born children with immigrant parents, and U.S.-born children with U.S.-born parents, the scientific evidence is limited. Nevertheless, on the basis of available data, it appears that, along a small number of important dimensions, children in immigrant families experience better health and adjustment than do U.S.-born children in U.S.-born families. This relative advantage tends to deteriorate with length of time in the United States and from one generation to the next. Moreover, as we discuss in this chapter, children in immigrant families may be at particular risk for certain health conditions.
Care must be taken not to overgeneralize, because children from different countries of origin differ greatly, the variation among children from the same country of origin is often substantial, and the available evidence for preliminary conclusions is quite limited. This chapter reviews what is known about the physical and mental health and adjustment of children in immigrant families. It identifies areas in which more research is needed, as well as areas in which children in immigrant families may face risks to healthy development and adjustment.
BIRTHWEIGHT AND INFANT MORTALITY
The two most commonly used indicators of infant health are the rate of infants born with low birthweight (defined as less than 2,500 grams) and infant mortality (defined as deaths before age 1 per 1,000 births) (Institute of Medicine, 1985; U.S. Department of Health and Human Services, 1986). A number of studies report significantly lower rates for these two indicators among the immigrant population than among U.S.-born mothers of the same ethnicity, a phenomenon that is referred to as the epidemiological paradox.
Initial studies of this phenomenon focused on the Mexican-origin population (Guendelman, 1995; Guendelman and English, 1995; Guendelman et al., 1995; Markides and Coreil, 1986; Scribner and Dwyer, 1989; Ventura, 1983, 1984; Williams et al., 1986).1 Subsequent research has documented a similar pattern for other ethnic groups, although the differences in rates of low birthweight and infant mortality in these groups have often been smaller than they are for Mexican immigrants. For example, in an analysis conducted for the committee, based on single births in the 1989-1991 Linked Birth/Infant Death Data Sets (Landale et al., 1998), the percentages of foreign-born and U.S.-born mothers with low-birthweight infants are, respectively, 4.1 and 5.4 percent for Mexicans, 4.4 and 4.7 percent for Cubans, and 4.8 and 5.2 percent for Central and South Americans. The more favorable measures hold for most Asian immigrants as well (Figure 3-1).
Although it is well documented that prenatal care contributes to positive birth outcomes, the more favorable health outcomes of immigrants often occur in the context of lower utilization of pre-
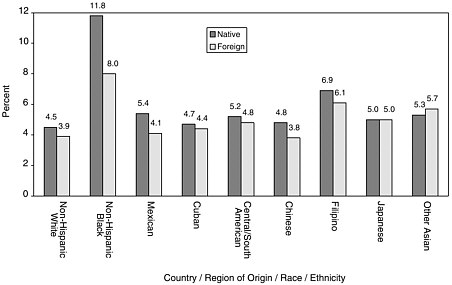
FIGURE 3-1 Percent with low birthweights among births to immigrant and native-born women by country or region of origin and race or ethnicity: 1990. Source: Landale et al. (1998).
natal care. There are indications that other factors may be of equal or greater importance. The role of lifestyle, for example, is only beginning to be documented and understood. More detailed studies of previously unmeasured lifestyle differences, such as nutrition and stress, that compare immigrants and natives, coupled with greater attention to alternative sources of information for pregnant immigrant women, could shed light on the precise role of formal medicine in protecting the health of children in immigrant families during infancy.
Consistent with the pattern for low birthweight, infant mortality rates are also lower for children of immigrants than for U.S.-born children of U.S.-born women, although sometimes the differences are slight. Among Hispanics, the infant mortality rates for single infants born to foreign-born and U.S.-born women are, respectively, 5.3 and 6.6 percent for Mexicans, 4.7 and 5.3 percent for Cubans, and for 5.0 and 5.2 percent for Central and South Americans. For Asians, infant mortality rates for infants of foreign-born and U.S.-born mothers are 4.3 and 4.6 percent for Chinese, 4.8 and 6.8 percent for Filipinos, 3.7 and 3.7 percent for Japa-
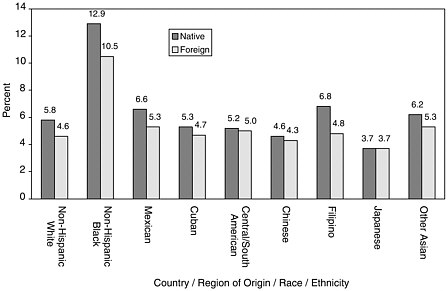
FIGURE 3-2 Infant mortality rate for children of immigrant and native-born women by country or region of origin or race or ethnicity: 1990. Source: Landale et al. (1998).
nese, and 5.3 and 6.2 percent for other Asians and Pacific Islanders. The infant mortality rates for non-Hispanic whites and blacks are also lower for foreign-born than for U.S.-born mothers (4.6 and 5.8 percent for whites, and 10.5 and 12.9 percent for blacks) (Figure 3-2) (Landale et al., 1998).
The pattern is less consistent for neonatal mortality rates (deaths at less than 28 days of age). The rate is lower for infants of foreign-born than for U.S.-born mothers for some groups (non-Hispanic whites, non-Hispanic blacks, Mexicans, Cubans, Filipinos), and higher for others (Central and South Americans, Chinese, Japanese, other Asians and Pacific Islanders). In contrast, the post-neonatal mortality rates (deaths between 28 days and 1 year of age) are lower for all immigrant groups except for Cubans, for whom the rates are somewhat higher (Landale et al., 1998).
A number of factors may contribute to these positive outcomes for infants in immigrant families. The relatively high levels of educational and occupational attainment among Asian immigrants may explain their superior infant health outcomes.
However, most immigrants from Latin America (particularly from Mexico) are neither affluent nor well educated; alternative explanations take into consideration the possible protective influence provided by their cultures of origin. For example, there is convincing evidence that cigarette smoking during pregnancy, a well-recognized cause of low birthweight, is substantially lower among immigrant women; statistically excluding the effect of that single factor substantially reduces the differential rates (Landale et al., 1998).
With regard to infant mortality, a nurturing and protective prebirth environment for the mother is most important. Along these lines, immigrant women of Mexican origin are less likely to use alcohol and drugs and may have a healthier diet than U.S.-born women (Cabral et al., 1990; Guendelman and Abrams, 1995). These healthful behaviors may be reinforced by strong family bonds among immigrant groups and communities that sustain cultural orientations that lead to healthful behavior, factors that become diluted with duration of residence in the United States. As we look to the future, however, it is possible that the increasing size and the geographic concentration of the immigrant population, especially from Mexico, will act to sustain these protective factors.
Additional study will allow researchers to identify the protective factors that contribute to the epidemiological paradox and to determine why, for some groups, acculturation leads to deteriorating health outcomes for infants. Such research should assess another possible explanation, as well: that women who are especially healthy may be more likely to immigrate to the United States than women who are less healthy; that is, that immigrant women are self-selected from among the more healthy women in their countries of origin, and they continue to have comparatively good health after they immigrate.
CHILDREN'S GENERAL HEALTH
Very little is known about the health of school-age children in immigrant families, and much of what is known derives from parental and self-reports. The 1994 National Health Interview Survey (NHIS) and the 1996 National Health and Nutrition Ex-
amination Survey (NHANES III) provide some health status parameters for children in immigrant families,2 as reported by parents.
However, these data must be interpreted with caution for several reasons. The NHIS responses are not categorized by families' country of origin (across which there may be significant variations); the responses to both surveys reflect parental awareness of conditions rather than medically confirmed diagnoses; immigrant parents may be more hesitant than U.S.-born parents to reveal the existence of health problems to an interviewer, or they may have health expectations that differ from native-born parents, because they come from different cultures; and only the NHANES III has standardized translations of the survey instruments into Spanish and uses bilingual, bicultural interviews. For all these reasons, inconsistencies between parental reports of general health and of the prevalence of specific conditions should be treated as preliminary, and subject to additional study.
In the NHIS, first- and second-generation children and adolescents up to 17 years of age were reported by their parents to have fewer acute and chronic health problems (except for certain respiratory conditions) than third- and later-generation children in the same age range. This was reported for all age subcategories (i.e., 0 to 2, 3 to 5, 6 to 11, and 12 to 17).
Parents of first- and second-generation children surveyed by the NHIS also reported fewer health problems that limited the children's activity (4 percent for the first and second generations compared with 7 percent for the third and later generations), and they reported that children were less often placed in special classes or unable to attend school because of health problems (2 percent for the first and second generations compared with 5 percent for the third and later generations).
Paradoxically, despite reporting significantly fewer individual health problems, immigrant parents reported in the NHIS that their first- and second-generation immigrant children have somewhat less favorable health status than did parents of third- and later-generation children: 75 percent of immigrant parents com-
pared with 81 percent of U.S.-born parents reported their child to be in ''excellent" or "very good" health. Comparable percentages (3 percent compared with 2 percent) reported their child to be in "fair" or "poor" health.
Parents were asked to rate their children's health as excellent, very good, good, fair, or poor in NHANES III. A clear difference was seen between all generations of Mexican-origin children and third- and later-generation white children in this measure of health. Mexican-origin children were more likely to be rated in fair or poor health by their parents than were third- and later-generation white children. Moreover, this difference was greatest for the first generation and declined with each generation (Mendoza and Dixon, 1998) (see Table 3-1).
Among first-generation Mexican-origin children, about 1 in 4 was rated by their parents to be in poor health. This compares to 1 in 25 for third- and later-generation white children. Third- and later-generation Mexican-origin children had similar rates as third- and later-generation black children, and both were twice as likely to be rated in fair or poor health compared with third- and later-generation white children. Mexican-origin children in all generations are therefore 2 to 9 times more likely to have parents who express concerns about their health than third- and later-generation white parents.
Data on migrant farmworker children, who are primarily second-generation children, provide more detail about parents' perceptions of their children's health and other aspects of health status. In a study of preschool children enrolled in the Migrant Head Start program, 56 percent of Hispanic parents considered their children to be in "excellent" or "very good" health, 34 percent to be in "good" health, and 9 percent in "fair" or "poor" health. The parents' impressions were consistent with a review of the children's health records, which indicated that 7 percent had "frequent" health problems, principally repeated upper respiratory infections (Aguirre International, 1997). Among the migrant population, it is likely that those children enrolled in Head Start have better health status than those not enrolled. Although this study did not collect data on health hazards posed by parental working conditions, particularly from pesticide residues on par-
TABLE 3-1 Percent with Selected Reported Health Conditions for First- and Second-Generation Children by Generation and for Third- and Later-Generation Children by Race and Ethnicity: 1996
|
Percent with Reported Conditiona |
First-Generation Mexican American |
Second-Generation Mexican American |
Third-Generation Mexican American |
|
Perceived health to be fair or poor as assessed by parent |
|||
|
< 5 yrs. |
23.9 (3.33) |
16.8 (1.05) |
6.3 (0.83) |
|
6-11 yrs. |
27.6 (7.70) |
20.0 (2.28) |
6.6 (1.43) |
|
12-16 yrs. |
28.7 (4.99) |
15.4 (2.52) |
6.8 (1.63) |
|
Asthma |
|||
|
< 5 yrs. |
2.2 (1.20) |
5.2 (0.88) |
8.1 (1.72) |
|
6-11 yrs. |
3.8 (2.74) |
9.8 (2.71) |
15.0 (4.09) |
|
12-16 yrs. |
3.1 (1.77) |
6.6 (1.91) |
8.5 (1.92) |
|
Possible active infection on physical examination at time of surveyb |
|||
|
< 5 yrs. |
8.3 (2.68) |
9.1 (1.42) |
12.3 (1.93) |
|
6-11 yrs. |
8.6 (3.66) |
5.3 (1.43) |
5.9 (1.57) |
|
12-16 yrs. |
4.0 (1.13) |
2.1 (1.12) |
4.7 (1.49) |
|
Ever had anemia |
|||
|
< 5 yrs. |
9.7 (2.18) |
14.5 (1.09) |
11.0 (1.60) |
|
6-11 yrs. |
9.2 (3.14) |
11.7 (2.08) |
2.8 (0.93) |
|
12-16 yrs. |
8.7 (2.64) |
7.2 (1.88) |
4.3 (1.12) |
|
Past 12 months any accidents, injury, or poisoning |
|||
|
< 5 yrs. |
3.7 (1.65) |
5.5 (0.58) |
10.0 (1.16) |
|
6-11 yrs. |
4.2 (3.26) |
5.0 (1.16) |
8.1 (1.95) |
|
12-16 yrs. |
3.6 (1.58) |
7.5 (1.40) |
10.7 (2.63) |
|
Condition of Teeth - Fair to Poor |
|||
|
< 5 yrs. |
39.3 (5.10) |
26.0 (2.49) |
21.0 (1.80) |
|
6-11 yrs. |
60.1 (8.15) |
42.6 (2.92) |
23.5 (3.68) |
|
12-16 yrs. |
50.8 (4.65) |
36.3 (3.24) |
16.4 (1.99) |
|
Problems seeing |
|||
|
< 5 yrs. |
0.2 (0.24) |
1.1 (0.35) |
0.7 (0.30) |
|
6-11 yrs. |
6.8 (2.42) |
13.2 (2.42) |
7.9 (1.19) |
|
12-16 yrs. |
18.8 (2.97) |
15.2 (1.86) |
13.3 (2.05) |
|
a Parental reported condition from Household Youth Questionnaire NHANES III. b Assessed by survey physicians by standardized physical examinations. |
|||
ents' clothing and accidental contamination of the water supply, they are an additional health risk that warrants examination.
In a random sample of migrant farmworker women in Wisconsin with children age 16 or younger traveling with them, children ages 3 to 5 had immunization levels for DPT, polio, measles, and rubella roughly comparable to kindergarten children in the state (Slesinger et al., 1986). Children of migrant farmworkers had lower levels of immunization for mumps, and only half of the children under the age of 12 had received an annual checkup. The study also reported that children of migrant farmworkers were less likely to receive dental care than the general population of children in the United States. It should be noted that the sample size in this study was relatively small (330 children) and the children were primarily Mexican-origin.
Any overall conclusion from these studies about the general good health and well-being of children in migrant farmworker families must be tempered by the fact that the farmworker and migrant subpopulations are extremely heterogeneous. Factors such as ethnicity, recency of immigration, cultural and linguistic barriers to health care, widely varied living and working conditions, and availability and quality of health care make generalizations difficult. Moreover, inappropriate generalization could obscure significant health problems in specific subpopulations of migrant farmworkers.
CHRONIC HEALTH CONDITIONS
An accurate assessment of the prevalence of chronic health conditions and disability among children in immigrant families does not exist for the most part. But there is little reason to expect chronic conditions among them to differ from those for other children who belong to the same racial, ethnic, or income groups.
Children in the United States with chronic conditions often face significant financial and other barriers that complicate the provision of comprehensive services, and the barriers are likely to be more formidable for immigrants. Chronically ill children may require multiple diagnostic and therapeutic services from the medical, educational, and social service systems. These resources are often located in different institutions, each with spe-
cific and sometimes complex and changing eligibility criteria. As a result, providing for and coordinating the provision of care for a chronically ill child usually falls heavily to the family. That responsibility can be particularly difficult for the immigrant family, for whom differences in culture, language, access to care, and financial resources can complicate the process (Lequerica, 1993; Smith and Ryan, 1987).
Asthma is the most common severe chronic physical condition of children, and the rates of the disease have increased in the past few decades. It is a single condition influenced by several key factors, including access to care, utilization of medical and support services, housing conditions (notably cleanliness), and the influence of cultural values on the pattern of care provided. Asthma also provides measurable and meaningful outcomes for both short- and long-term morbidity and health care costs. Additional careful study of asthma in the immigrant population may serve as a valuable indicator of the health and well-being of immigrant children.
The prevalence of childhood asthma varies substantially across ethnic groups for reasons that reflect a combination of biological, cultural, and socioeconomic differences, although the mechanisms by which these factors work are not well understood. Children in immigrant families with asthma often have additional complicating factors. For some with pollen-sensitive forms of asthma, attacks may be exacerbated by the move from a tropical to a temperate climate with higher and more seasonably varying pollen rates (Echechipia et al., 1995; Sin et al., 1997). In addition, infection by viral pathogens to which children have not been exposed previously can trigger acute asthma episodes (Sokhandan et al., 1995). Cultural beliefs among immigrant families about the etiology and treatment of asthma may differ from the general U.S. population as well. For example, studies in the Puerto Rican community have demonstrated that the degree of acculturation is directly related to the likelihood of compliance with medically prescribed asthma therapy for children (Pachter and Weller, 1993).
New analyses conducted for the committee from NHANES III indicate that, among Mexican-origin children, the prevalence of asthma as reported by parents increased between the first, second, and third and later generations (Mendoza and Dixon, 1998)
(see Table 3-1). By the third generation, parental reports of asthma among Mexican-origin parents exceeded those of U.S.-born white parents for children ages 0 to 12, but were lower for adolescents. Since these prevalences are based on parental reports, knowledge of the condition is essential. This knowledge, in turn, is most likely to be accurate for children who have been diagnosed by a health care professional. The possibility of generational differences in access to health care among children of Mexican origin may, as a result, be a factor in these results (with either underreporting or overreporting among the first generation). Clinical data are important to further assess the generational differences in the prevalence of asthma among immigrant Mexican-origin children.
Comprehensive and culturally sensitive care may be particularly important in the care of asthma, because access appears to be problematic for immigrant and minority populations. In one study, black and Hispanic children were less likely than white children to leave the hospital with appropriate home nebulization services, a cornerstone of chronic asthma therapy (Finkelstein et al., 1995).
INFECTIOUS DISEASES
The primary infectious diseases associated with significant morbidity and mortality among infants, children, and adolescents in the United States are perinatal infections, some of which are preventable with adequate prenatal care; human immunodeficiency virus (HIV) infection; vaccine-preventable illnesses among those inadequately immunized; tuberculosis among infants and children exposed to adults with tuberculosis; sexually transmitted diseases (other than HIV) among adolescents; and a range of respiratory and gastrointestinal infections responsible for minimal mortality but significant morbidity and expense.
These diseases occur among children of all racial and ethnic origins, but children of recently arrived immigrants are at particularly high risk of harboring or acquiring several of them. Rates of infection vary considerably by country of origin and socioeconomic status and are compounded if there is lack of access to health care in the United States. Furthermore, the infectious
disease problems of children in immigrant families present a challenge to U.S. physicians, who may be inexperienced in diagnosing and treating conditions such as malaria, amebiasis, schistosomiasis and other helminthic infections, congenital syphilis, hepatitis B, and tuberculosis (American Academy of Pediatrics, 1997b). Tuberculosis, hepatitis B, and parasitic infections are of particular concern for the children in immigrant families, with implications for the health of the entire U.S. population.
In 1995, immigrants accounted for 7,930, or 35 percent, of total U.S. tuberculosis cases. Tuberculosis in the foreign-born population is concentrated geographically, both in terms of country of origin and state of residence. In 1995, two-thirds of immigrants with tuberculosis were from seven countries: Mexico (22 percent), the Philippines (13 percent), Vietnam (12 percent), China (5 percent), Haiti (5 percent), India (5 percent), and Korea (4 percent). Nearly 70 percent of those immigrants resided in four states: California, New York, Texas, and Florida (Binkin et al., 1996). Foreign-born people are at particular risk for drug-resistant tuberculosis infection, an important reason to identify these cases and ensure that they are provided appropriate care in order to minimize the risk of spread to the entire U.S. population (American Academy of Pediatrics, 1997a).
A diagnosis of tuberculosis infection in a child is a sentinel event, because it represents recent transmission in the community and therefore merits intensive investigation by public health authorities to identify the source. Control of this disease requires a combination of strategies, including a vigorous and adequately funded public health effort, improved policies and procedures for overseas screening of potential immigrants, and careful surveillance of cases once in the United States. It is of importance to the entire population as well as to immigrants with tuberculosis that immigrants are ensured access to appropriate health services.
Hepatitis B infection is highly endemic in China, Southeast Asia, Africa, the Pacific Islands, parts of the Middle East, and the Amazon Basin. In these areas, 8 to 15 percent of the population become chronically infected with the virus, which is a major cause of acute and chronic hepatitis, cirrhosis, and primary hepatocellular carcinoma. Universal hepatitis B vaccination is now recommended for all children born in the United States, and for chil-
dren younger than 11 living in households of first-generation immigrants from countries with intermediate or high endemic rates of hepatitis B.
Parasitic infection rates ranging from 10 to 55 percent have been reported for immigrant pediatric populations in the United States, with Trichuris and Giardia the most frequently isolated parasites (Starke et al., 1994). Most intestinal parasites do not present a significant public health hazard in the United States, because effective sewage disposal and hygienic practices interrupt transmission. However, many immigrants live in crowded areas with poor sanitation, and transmission within households may occur. Intestinal parasites may be the cause of chronic or recurrent abdominal pain, diarrhea, anemia, and growth failure in children. Physicians should be particularly alert for their possible occurrence in children from Central and South America, Mexico, the Caribbean, Southeast Asia, and Africa.
One of the few measures of children's physical health status in the NHANES III that is determined by physician report is the assessment of a possible active infection in the child at the time of the survey. As seen in Table 3-1, comparisons between all generations of Mexican-origin children and third- and later-generation white children show no significant differences in the frequency of active infections (Mendoza and Dixon, 1998). There were also no differences in active infections between generations of Mexican origin nor between them and third- and later-generation black children. These data need to be interpreted with caution, given that they represent only one point in time and should not be generalized beyond immigrants of Mexican origin; however, they suggest that there may not be a significant difference in active infections between this group of foreign-born and U.S.-born children.
ENVIRONMENTAL TOXINS
High levels of lead in the blood pose a risk to brain development, particularly during the second and third years of life, and have been associated with hyperactivity, diminished intellectual ability, and impaired academic performance in school-age children.
National estimates of blood lead levels are not available for children from specific countries of origin, but it is evident that children in immigrant families may have a higher incidence of lead poisoning than third- and later-generation children for several reasons, including poverty, exposure to lead in their countries of origin, use of lead-containing products from their country of origin, and a higher likelihood of residing in lead-contaminated housing (Bellinger et al., 1989). One estimate from the most recent National Health and Nutrition Examination Survey (NHANES III) found elevated blood lead levels among Mexicanorigin children, and a study of Mexican-born children in Santa Clara Valley, California, found lead levels above 10 µg/dL among 20 percent of the children, compared with 7 percent of third- and later-generation children (Snyder et al., 1995).
Although few countries sending large numbers of immigrants to the United States gather data from nationally representative samples, mean blood lead values from selected studies of children in those countries are considerably higher than the current U.S. mean of 3.5 µg/dL for 1- to 5-year-old children. For example, contemporaneous surveys of children in Mexico City indicate mean lead levels of 12.0 µg/dL in 2- to 4-year-olds (Salazar-Schettino et al., 1991) and 9.9 µg/dL in 1- to 5-year-olds (Romieu et al., 1995). Children residing in urban areas in China were reported to have mean lead levels of 21 µg/dL (Shen et al., 1996), and the mean cord blood lead level of Indian children born in Lucknow in 1990 was 17.0 µg/dL (Saxena et al., 1994).
An important source of lead exposure in Mexico is the leaded glaze on earthen pottery cookware (Rojas-Lopez et al., 1994), and elevated blood lead levels have been reported in Mexican-origin children from the same source (Gellert et al., 1993). In addition, in countries where gasoline still contains lead (including most developing countries), lead levels in children remain high, and most of this elevation is attributed to airborne lead from gasoline (Romieu et al., 1995; Shen et al., 1996). Elevated blood lead levels have been reported in children in immigrant families from the Middle East, India, and Pakistan from the use of eye cosmetics with high lead content (Al-Kaff, 1993; Sprinkle, 1995). Folk remedies that contain lead and are used to treat childhood illnesses have been reported for families of Mexican, Saudi Arabian, and
Hmong and other Asian origins (Baer and Ackerman, 1988; Yaish et al., 1992).
In an analysis of 136 Rhode Island census tracts, lead levels greater than 10 µg/dL were reported in 30 to 60 percent of children residing in census tracts with a high proportion (20 percent) of Hispanic immigrants, compared with elevated levels in less than 10 percent of children in census tracts with few immigrants (Sargent, 1997).
For migrant farmworkers, pesticides are an ever-present danger, with 1.2 billion pounds of pesticides used in U.S. agriculture annually. The Environmental Protection Agency estimates that as many as 300,000 farmworkers suffer from pesticide-related illnesses or injuries each year (U.S. General Accounting Office, 1992). One New York study found that one-third of the children interviewed who had worked in agriculture the previous year had been injured by pesticides during that time period (U.S. General Accounting Office, 1992). As harvesters, children encounter pesticide residues on crops. When children and adolescents eat, drink, or smoke in the fields, they ingest additional pesticides. And youngsters often are exposed to direct spray or drift while working in the fields or at home in adjacent migrant labor camps. These chemicals may cause acute ailments such as skin rashes, eye irritation, flu-like symptoms, and sometimes even death. They may also cause chronic harms such as birth defects, sterility, neurological damage, liver and kidney disease, and cancer (Wilk, 1993). Children are more likely to be harmed by pesticide exposures than are adults because they have lower body weight, higher metabolism, and immature immune and neurological systems (National Research Council, 1993).
NUTRITIONAL STATUS
Nutritional status is determined by measurements of children's height, weight, and dietary intake, as well as by biochemical parameters such as serum iron (Dwyer, 1991). Overall, the nutritional status of foreign-born children upon entering this country is directly related to their socioeconomic circumstances in the country of origin. Those who were better off in their home countries grow appropriately, and those who were living in pov-
erty grow less well and proportionately to their degree of impoverishment. Given improved economic, nutritional, and health conditions, improved growth can be expected. Conversely, if poverty is unalleviated, it will continue to limit a child's growth.
There are currently only partial data on the nutritional status of children in immigrant families. For Hispanic and Asian immigrant groups, some information is available, but children from other countries, such as Eastern Europe, the former Soviet Union, Africa, and the Middle East, are for the most part invisible in the literature (Mendoza and Dixon, 1998).
For Mexican-origin immigrants, analyses of the Hispanic Health and Nutritional Examination Survey data for 1984 by Mendoza and Dixon (1998) found that, as a group, first-generation children tended to be shorter than their U.S.-born counterparts, an outcome that appeared to be the result of differences in poverty between the two groups. Weight was found to be less deviant than height from the U.S. median for both first- and second-generation children.
The greater deviation from the norm of height than weight resulted in obesity in a greater number of Mexican-origin children and adolescents in both the first and second generations. Although these children appear to have their stature affected by poverty, suggesting stunting due to poor nutrition and health, the increase in obesity would suggest the counterargument of adequate or overnutrition. Similar findings have been reported for some Asian children in immigrant families as well (Himes et al., 1992). The mechanism of this process, obesity in the face of poor linear growth, is not well understood, but one hypothesis proposes that hormonal changes during pregnancy as a result of a nutritional insult in utero may lead to changes in long-term linear growth (Popkin et al., 1996).
To explore further the issue of obesity and problems with linear growth, Mendoza and Dixon (1998) examined the daily intake of the four food groups by first- and second-generation Mexican-origin children. These data showed that consumption of the basic four food groups was similar or better for first-generation children than for second- and third- and later-generation children. In fact, for the age group 6 to 11 years, first-generation children appeared to have more balanced diets. However, the dietary in-
take data did not determine total caloric intake or serving size and therefore need to be viewed cautiously and confirmed by other studies.
Another way to confirm the adequacy of children's diets is by determining the prevalence of iron deficiency anemia. Iron deficiency anemia is the most commonly measured nutritional biochemical abnormality. There are other causes of anemia, but iron deficiency anemia is the most common among children, particularly for those under age 3 (Florentino and Guirriec, 1984; Looker et al., 1997; Lozoff et al., 1997).
Data on Mexican-origin children in general and reports of anemia by mothers of first-generation children suggest that high prevalences of anemia are not present, and for the most part are less than 3 percent (Looker et al., 1997; Mendoza and Dixon, 1998). Data from NHANES III show that parental reports of their children ever having anemia was about 9 percent for first-generation Mexican-origin children of all ages (see Table 3-1). For children less than age 5, there were no significant differences between first- generation Mexican-origin and third- and later-generation white children; there were also no significant differences between first- and either later-generation Mexican-origin children or third- and later-generation black children in this age group.
Data about the nutritional status of Asian children in immigrant families are limited and complicated by the diversity of Asian countries that send children to the United States. As a result, an understanding of the economic, nutritional, and health conditions of the countries of origin is essential to assessing the condition of these children.
In the 1980s, several studies reported on the growth parameters of children in immigrant families from Southeast Asia. Dewey reported significant stunting for age among Vietnamese, Hmong, Mien, and Laotian first-generation preschoolers (Dewey et al., 1986); 39 percent were below the fifth percentile for height, but only 7 percent were below the fifth percentile for weight, suggesting the presence of stunting but not wasting. In fact, Dewey found that children who had been in the United States longer were heavier but not taller. Other studies have similarly reported stunting among Southeast Asian children in immigrant families (Barry et al., 1983; Brown et al., 1986; Peck et al., 1981). Some
evidence shows that, with improved economic, nutritional, and health conditions, these children have exhibited significant catch-up growth (Yip et al., 1992a, 1992b, 1993). But others have found persistent growth problems among them, including among second-generation children, which have been attributed to persistent health and nutritional problems related to poverty (Baldwin and Sutherland, 1988; Himes et al., 1992; Hyslop et al., 1996).
The limited data on the dietary intake of Asian children in immigrant families indicate that they initially consume traditional diets, but then make a transition to American foods (Story and Harris, 1988, 1989; Thuy et al., 1983). Southeast Asian mothers have been observed to reduce the practice of breastfeeding, apparently as a result of the need to work, the desire for convenience, and the sense that baby formula is superior (Serdula et al., 1991; Tuttle and Dewey, 1994). For Southeast Asians there are also findings of high levels of anemia—in some studies, among 18 to 36 percent of new immigrants (Goldenring et al., 1982; Peck et al., 1981). The prevalence of anemia indicates not only poor intake of iron-rich foods, but also possible loss of iron from gastrointestinal bleeding, commonly associated with active parasitic infections (Juckett, 1995; Sarfaty et al., 1983; Weissman, 1994; Wiesenthal et al., 1980). However, in addition to anemia from iron loss, Southeast Asian children in immigrant families also have a high prevalence of hemoglobinopathies (Craft et al., 1983; Hurst et al., 1983). It has been estimated that as many as 40 percent of Southeast Asian refugees (Vietnamese, 62%; Laotian, 22%; and Cambodian, 16%) have one or more congenital anemias (Glader and Look, 1996).
One of the few longitudinal studies of school-age children in immigrant families was done by Schumacher et al. (1987) in a Newcomers school in San Francisco. A group of 835 children from Mexico, El Salvador, Nicaragua, Honduras, Guatemala, Peru, China, Taiwan, Hong Kong, Philippines, Vietnam, Cambodia, and Laos were followed every 3 months for a year. All the children in immigrant families showed improved growth velocities that were either at or above the median for third- and later-generation white children. That is, they grew at a faster rate than the third- and later-generation children, implying that they were experiencing catch-up growth. By subgroup, 60 to 90 percent of the children,
even those who started at two standard deviations below the median, showed significant catch-up growth (Schumacher et al., 1987).
OTHER HEALTH PROBLEMS
There are a number of other conditions for which children in immigrant families may be at increased risk, based on current prevalence rates among low-income U.S. ethnic groups. These include unintentional injury, the most important cause of mortality and serious disability for American children and adolescents; child maltreatment; and poor vision and dental health. Given higher rates of these conditions among children living in poverty, one might expect higher rates among children in immigrant families. However, parental report information from the NHANES III seen in Table 3-1 shows that the prevalence of accidents, injury, and poisoning among all ages of Mexican-origin children is significantly lower than that of third- and later-generation white children of similar ages (Mendoza and Dixon, 1998). Rates increase from the first to the third and later generations but remain lower than those reported by parents of third- and later-generation white children.
The opposite pattern is found for dental health. Parents of first-generation Mexican-origin children are significantly more likely to report that their children's teeth are in fair to poor condition than are parents of second- and third- and later-generation Mexican-origin children or parents of third- and later-generation white and black children (Mendoza and Dixon, 1998) (see Table 3-1). The third- and later-generation children of Mexican origin were more likely, however, to be reported as having fair to poor teeth than were third- and later-generation white children. For first-generation Mexican-origin youth and second-generation Mexican-origin 6- to 11-year-olds, vision problems were also reported at levels that exceed those of third- and later-generation children.
ADOLESCENT HEALTH
The 1995 National Longitudinal Study of Adolescent Health (called Add Health) provides estimates, based on new analyses
conducted for the committee, of the perceived health status and health risk behavior of first- and second-generation adolescents compared with third-generation adolescents (Harris, 1998). Data are available for adolescents in families from countries of Central and South America, Mexico, Asia, Africa, and Europe.
As shown in Table 3-2 and Figure 3-3, overall and for most specific countries of origin, first-generation adolescents were less likely than second or third and later generations to consider themselves in poor health (specifically with neurological impairment, obesity, or asthma) or to have school absence due to health or emotional problems. By the third generation, reports of poor health often exceed those of third- and later-generation white adolescents. First-generation adolescents also reported less delinquent or violent behavior and less substance abuse than did later generations (see Table 3-2 and Figure 3-4). Among the first generation, those living in the United States for longer periods of time tended to be less healthy and to report increases in risk behaviors. (Figures 3-5 and 3-6 provide additional information by ethnic group and immigrant status.)
The Add Health survey also found that first-generation immigrant adolescents were older at age of first intercourse and had a lower probability of having had intercourse than later generations. However, first-generation adolescents were less likely to use birth control at first intercourse. These generational differences remained after statistically excluding the effects of family income, family composition, and neighborhood factors (Harris, 1998).
Other research addresses the influence of acculturation to American society among adolescents, particularly in regard to reproductive patterns and contraceptive use in the Hispanic population. A review by Brindis (1997) indicates that, with increased acculturation, Hispanic girls engage in sexual activity at earlier ages and are more likely to give birth outside marriage and to leave school. Moreover, Hispanic adolescents who consider themselves (or aspire to be) highly acculturated to American society report increased use of alcohol, tobacco, and illicit drugs (Brindis et al., 1995). Among the general population, relatively early childbearing is a common occurrence among young Hispanic women, with those age 18 to 24 almost twice as likely as white women (though less likely than black women) to have had
TABLE 3-2 Health Indicators for First- and Second-Generation Adolescents by Generation and for Third- and Later-Generation Adolescents by Race and Ethnicity: 1995 (means)
|
|
First Generation |
Second Generation |
Non-Hispanic White, Third and Later Generations |
|
Physical Health |
|||
|
General health fair or poor |
9.2 |
10.7 |
8.1 |
|
Missed school due to a health or emotional problem |
33.5 |
36.5 |
33.6 |
|
Learning difficulties |
9.3 |
12.5 |
16.9 |
|
Obesity |
17.0 |
26.7 |
23.4 |
|
Asthma |
4.8 |
8.1 |
12.2 |
|
Health and school problems index |
0.74 |
0.94 |
0.93 |
|
Emotional Health |
|||
|
Psychological distress |
1.54 |
1.52 |
1.45 |
|
Positive well-being |
2.85 |
2.87 |
3.06 |
|
Health Risk Behavior |
|
|
|
|
Ever had sex |
31.3 |
33.9 |
36.7 |
|
Age at first intercoursea |
15.1 |
14.9 |
14.8 |
|
Birth control/first intercoursea |
56.2 |
57.3 |
67.1 |
|
Four or more delinquent acts |
15.8 |
25.0 |
21.9 |
|
Three or more acts of violence |
14.6 |
21.3 |
19.4 |
|
Use of three or more substances |
8.3 |
17.4 |
25.1 |
|
Risk behavior index |
0.7 |
0.98 |
1.03 |
|
N |
1,651 |
2,526 |
10,248 |
|
NOTE: With the exception of age at first intercourse and emotional health, all differences are statistically significant at the .001 level. Non-Hispanic Asians are not included because of small sample size. a These outcomes are based on the sample of adolescents who had ever had sex (N = 8,226). Source: Harris (1998). |
|||
|
Non-Hispanic Black, Third and Later Generations |
Non-Hispanic Other, Third and Later Generations |
Hispanic, Third and Later Generations |
Total |
|
11.5 |
14.3 |
13.1 |
9.7 |
|
37.1 |
40.2 |
41.1 |
35.4 |
|
14.3 |
15.6 |
18.3 |
15.4 |
|
29.9 |
31.5 |
31.0 |
25.3 |
|
13.5 |
14.9 |
15.7 |
11.8 |
|
1.05 |
1.17 |
1.2 |
0.97 |
|
1.52 |
1.54 |
1.54 |
1.49 |
|
2.99 |
2.89 |
2.89 |
2.99 |
|
54.8 |
39.2 |
45.3 |
40.4 |
|
13.8 |
14.4 |
14.2 |
14.5 |
|
64.2 |
60.5 |
29.6 |
21.6 |
|
27.2 |
26.4 |
31.5 |
21.9 |
|
8.6 |
24.3 |
25.3 |
19.4 |
|
1.09 |
1.17 |
1.32 |
1.03 |
|
4,312 |
456 |
1,429 |
20,622 |
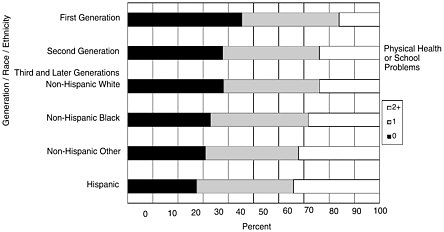
FIGURE 3-3 Percent with physical health or school problems for first- and second-generation adolescents by generation and third- and later-generation adolescents by race and ethnicity: 1995. Source: Harris (1998).
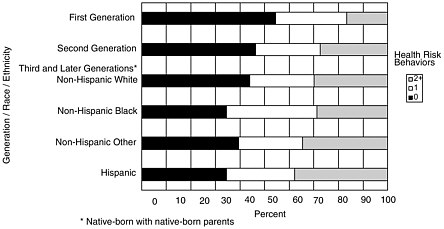
FIGURE 3-4 Percent engaging in health risk behavior for first- and second-generation adolescents by generation and third- and later-generation adolescents by race and ethnicity: 1995. Source: Harris (1998).
children. However, there are considerable differences in fertility rates among different Hispanic groups, with Mexican-origin women consistently having the highest and Cuban-origin women the lowest fertility rates.
Among adolescents in grades 7 through 12 in 1995, health risk behaviors involving early sexual activity, nonuse of birth control,
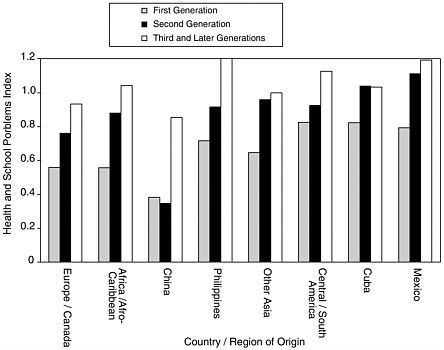
FIGURE 3-5 Mean physical health and school problems index for adolescents by generation and by country or region of origin: 1995. Source: Harris (1998).
delinquency, use of violence, and substance use tended to increase with each generation for adolescents from all countries of origin taken together (Table 3-2) (Harris, 1998). These risk behaviors also increased for each generation for children with origins in Mexico, Cuba, Central and South America, China, the Philippines, Japan, Vietnam, Africa and the Caribbean, and Europe and Canada, although the differences are not always statistically significant (Harris, 1998). For most of these behaviors, the third- and later-generation rates approach and even exceed those of third- and later-generation white children.
MENTAL HEALTH AND ADJUSTMENT
In general, the mental health and adjustment of children and youth in immigrant families appears to be similar to, if not better, than that of U.S.-born children and youth in U.S.-born families, in
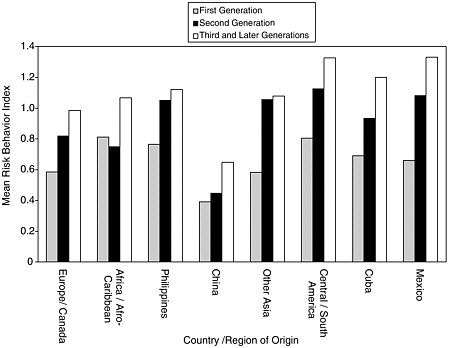
FIGURE 3-6 Mean risk behavior index for adolescents by generation and by country or region of origin: 1995. Source: Harris (1998).
most respects. There is, however, little systematic evidence available in this domain. Among the factors that have been measured with samples of children in immigrant families are acculturative stress, psychological adjustment, and academic achievement.
Acculturative Stress
A key factor in understanding psychosocial distress among children and youth in immigrant families is acculturative stress (Aronowitz, 1984; Gil et al., 1994; Gil and Vega, 1996; Zambrana and Silva-Palacios, 1989). Acculturative stress is an aspect of children's adaptation to the cultures and social structures of a new host country. The kinds of problems associated with acculturative stress include:
-
Language problems as children and their families negotiate a new social system in which their native languages may not
-
be understood and in which they may not know the language of the host country;
-
Perceived discrimination from the larger society because of differences such as language, skin color, clothing, food habits, and other physical features;
-
Perceived cultural incompatibilities between the home culture and the host culture resulting from different family values, interaction styles, social roles, and socialization practices; and
-
Increasing gaps between the cultural affiliations of adults and children and their adherence to home country or host country cultural values and norms.
A study examining acculturative stress among Hispanic teenage boys found that second- and third- and later-generation Hispanics from low acculturation backgrounds who were primarily Spanish speaking and who experienced little family pride, high levels of language conflicts, and perceived discrimination from the larger society were at greatest risk for psychological distress. For first-generation adolescents, higher levels of acculturation corresponded with increased family conflict and decreased family pride. Bicultural individuals born in the United States experienced less acculturation stress, more family pride, and the most positive outcomes (Gil et al., 1994).
In general, mental health researchers have begun to establish that bicultural individuals are more likely to be better adjusted in a new society. This is due to the fact that they not only maintain the strengths of their home culture, but also retain supportive social links to that culture while they develop the language and social skills needed to successfully negotiate their new cultural setting (LaFromboise et al., 1993; Pawliuk et al., 1996). However, more research is needed to further validate these relationships.
Other studies have focused on the context of the receiving host communities and their impact on children's adjustment. One study differentiated the reception of Cuban and Nicaraguan immigrants in Miami (Gil and Vega, 1996). In this study, Cubans were more actively supported by the U.S. government, for example, in obtaining refugee status, work permits, and other supports; these supports were not as broadly extended to the Nicaraguans. The results of this study emphasized that supporting the
family was more important than supporting an ethnic enclave. This research also established that adolescents acculturated more quickly than their parents, particularly with respect to English language acquisition, and that boys acculturated more quickly than girls. A key finding of this study was that, at equivalent stages of adjustment, the Nicaraguans experienced more acculturation conflicts and perceived more discrimination than the Cubans. Differences in the supports provided to these two Hispanic communities and differential response from the broader society in support of these groups were particularly reflected in the adolescents' adjustment.
Others have found that the degree of acceptance provided by the ethnic enclave may also affect the adjustment of children in immigrant families. McKelvey and Webb (1996) examined the expectations of Vietnamese Amerasian adolescents and young adults (born to Vietnamese mothers and American fathers) before they left Vietnam and the actual support they received from the Vietnamese community upon arrival. In general, the established Vietnamese community in the United States was not very supportive of the Amerasian Vietnamese.
The investigators found that the adolescents who had higher expectations for support from the U.S. Vietnamese community and did not receive it had the highest depressive symptoms when they were assessed several months after arrival. The investigators also discovered other factors that may have contributed to the worsening mental health of the Amerasian youth following immigration, including traveling alone or with only partial family support, close identification with other youths from whom they were separated upon arrival in this country, limited education, and little or no knowledge of English. This study underlines the importance of the local ethnic community to the mental health and adjustment of children in immigrant families. The study also provides important cautions about decisions concerning the determination of ethnicity, the appropriate ethnic community of resettlement, and the response from the local community and national government.
Although the family is the nexus of the growth and development of immigrant children, as it is for all children, differential rates of acculturation by parents and children have been associ-
ated with family problems and conflicts. Variable rates of acculturation have also been linked with psychological distress among children in immigrant families (Aronowitz, 1984; Chiu et al., 1992; Gil and Vega, 1996; Zambrana and Silva-Palacios, 1989). Common family problems include illness of a key adult, difficulties maintaining the family's financial well-being, spousal conflict, and parental drinking. Such family problems have been predictive of higher rates of adolescent distress (Zambrana and Silva-Palacios, 1989). In particular, girls seem to respond more strongly to family conflicts than boys, perhaps due to the fact that girls are thought to place more emphasis on social relations in developing their sense of self (Zambrana and Silva-Palacios, 1989). Boys may be buffered from family conflicts because they tend to spend more time outside the home. However, their tenuous family ties place them at risk for developing other kinds of problems.
In general, very little is known about the effect of the migration experience itself on children and adolescents in immigrant families. Migration from one country to another and from rural to urban areas has been found to be stressful for adults (Desjarlais et al., 1995; Hull, 1979; Kasl and Berkman, 1983; Kuo, 1976; Portes and Rumbaut, 1996; Sanua, 1970), but little is known about the sources of the stress and its manifestations at the individual level. A study by McKelvey and Webb (1996) illustrates and other research confirms that the health and well-being of children in immigrant families may be influenced by the circumstances surrounding the decision to migrate, the resources of the family, and the response of the receiving community to the immigrants (Cervantes and Castro, 1985; Portes and Rumbaut, 1996; Portes et al., 1992; Rogler, 1994; Rogler et al., 1989, 1991).
The stages of family adjustment over the course of the immigration experience also affect the psychological health of children and adolescents (Aronowitz, 1984; Gil and Vega, 1996; Pawliuk et al., 1996), although some research indicates that immigrants present fewer behavioral problems than native-born children (Gibson and Ogbu, 1991). Often, the family's first year in the United States may be characterized by feelings of euphoria over the success of their immigrating. However, the second year tends to be the most stressful, as the impact of acculturative stress is completely experienced. The third and subsequent years vary
greatly psychologically, depending on the interplay of family factors and contextual variables. The response of the host community to the family may be particularly critical to the psychological well-being of children in immigrant families in the third and subsequent years.
Psychological Adjustment
Some have speculated that during adolescence the stresses of immigration are likely to be expressed as identity problems pertaining to views of the self, issues of control and efficacy, and fit into the peer group, with the school being a particularly critical context for development (Aronowitz, 1984; Gil et al., 1994; Munroe-Blum et al., 1989; Phinney, 1990; Phinney and Chavira, 1995; Rousseau et al., 1996; Rumbaut, 1998b). Aronowitz (1984) notes that children in immigrant families face a challenging double bind: if they maintain their cultural heritage over time, they risk greater discrimination and alienation from the host culture; if they abandon their cultural heritage, they risk alienation and rejection from family and friends, with no guarantees of acceptance from the wider society. Features like racial differences accentuate the differences between the immigrant child and the host society and heighten this dilemma (Phinney and Chavira, 1995).
Psychological adjustment was studied in research conducted for the committee using the National Educational Longitudinal Survey (NELS) of 1988 for 8th graders from China, the Philippines, Mexico, and other Hispanic countries (Kao, 1998) and the 1995 National Longitudinal Study of Adolescent Health (Add Health) for adolescents in grades 7 through 12 in 1995 with origins in Mexico, Cuba, Central and South America, China, the Philippines, Japan, Vietnam, Africa and the Caribbean, and Europe and Canada (Harris, 1998). The constructs assessed in Add Health were psychological distress and psychological well-being; NELS measured self-efficacy (feelings of having control over the direction of one's life), self-concept, and alienation (feelings of being unpopular among school peers).
The NELS analyses (Kao, 1998) indicated that first- and second-generation youth had significantly lower feelings of self-effi-
cacy and higher feelings of alienation from their schoolmates than third- and later-generation white youth. In contrast, the immigrant youth and their white counterparts with U.S.-born parents did not differ in their self-concepts. The Add Health analyses (Harris, 1998) found no differences between first- and second-generation immigrant youth and third- and later-generation white youth in psychological well-being and distress (see Table 3-2). Taken together, these results may suggest that immigrant youth are able to maintain positive feelings about themselves and their general well-being, despite perceiving that they have relatively less control over their lives and are less well accepted by their school peers.
After the effects of socioeconomic status are statistically excluded, the NELS data continue to show relatively lower self-efficacy among first- and second-generation youth who are Hispanic and Asian compared with third- and later-generation white youth (see Figures 3-7 and 3-8). Black youth in immigrant families and third- and later-generation white youth, however, no longer differ significantly. With respect to alienation, after controls are added, first- and second-generation Asian youth continue to show higher feelings of alienation than third- and later-generation white youth. Among Hispanics, however, only the second generation continues to differ significantly from third- and later-generation white youth; among black youth, only the third generation shows significant differences. It is also important to note that, especially for Hispanic youth in immigrant families, low socioeconomic status is an important explanatory factor, leading to reports of lower self-efficacy and greater alienation.
When controls for socioeconomic influences such as family and neighborhood poverty are added in the Add Health data, differences in psychological well-being and distress emerge as well, but they are in the opposite direction from those found in the NELS data. When differences are found, first- and second-generation immigrant youth demonstrate better psychological well-being than third- and later-generation white youth. There is one exception, however: adolescents from the Philippines, among the most Americanized of the immigrant groups studied and a group speaking English as its native language, experienced higher psychological distress in every generation than third- and later-
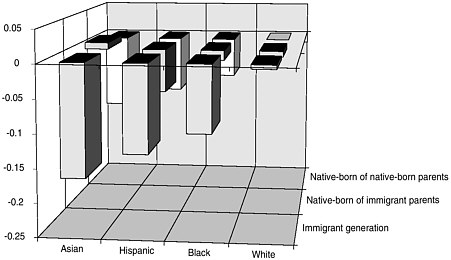
FIGURE 3-7 Estimates of adolescent self-efficacy. Note: The baseline is the score of white third-generation youths (native-born children of native-born parents). Source: Kao (1998).
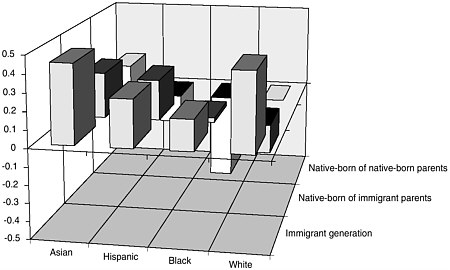
FIGURE 3-8 Estimates of adolescent alienation at school. Note: The baseline is the score of white third-generation youths (native-born children of native-born parents). Source: Kao (1998).
generation white adolescents. Family and neighborhood poverty were among the most influential predictors of psychological stress and well-being for all children. Harris (1998) interprets the data as demonstrating the protective influence of immigrant status among youth that emerges once the effects of greater exposure to poverty and inner-city neighborhoods are eliminated.
Some evidence of a protective function of immigrant status is also found in recent studies of suicide. A study of suicide trends among adolescent immigrants and ethnic groups in California found that first-generation immigrant adolescents were at a slightly lower risk of suicide, regardless of age, than third- and later-generation adolescents. The suicide rate for immigrants was the same as that of lifelong residents among third- and later-generation white and black adolescents, but the rates for Mexican-origin adolescents were lower than those for all third- and later-generation adolescents (Sorenson and Shen, 1996). A similarly low rate of suicide among Mexican-origin adolescents, compared with the third- and later-generation adolescent population, was found throughout the Southwest. In Miami, a longitudinal study of Cuban, Nicaraguan, other Hispanic, black, and non-Hispanic white adolescent boys found the highest rate of suicide attempts among Nicaraguans and other Hispanics. In that study, higher levels of acculturation among minority groups were associated with an increase in suicide attempts.
The Children of Immigrants Longitudinal Study, conducted in Southern California (San Diego) and South Florida (Miami and Fort Lauderdale), is the first large-scale survey of changes in the family, community, and educational experiences of children and youth in immigrant families from nine countries of origin in the Western hemisphere and Asia (see Portes, 1996; Portes and MacLeod, 1996; Portes and Rumbaut, 1996; Rumbaut, 1994b, 1995, 1997b, 1998b). Although it does not provide nationally representative estimates for children from these countries of origin and does not include comparative data from U.S.-born children and youth in U.S.-born families, the survey is a rich source of psychological data and provides insights into the processes that might underlie patterns in the psychological well-being of immigrant youth. For example, Rumbaut (1998b) has recently identified the rise of a reactive ethnicity among immigrant youth. That is, some
youth—notably those of Mexican and Filipino descent—increasingly identify themselves by their foreign nationality (e.g., ''Filipino") or with a pan-ethnic (e.g., "Asian") label. He speculates that this pattern points to a growing identification of immigrant youth with U.S. minority groups that, if sustained, may have important implications for their later development. At the same time, the vast majority of youth in this sample agree that "there is no better country to live in than the United States."
Research was conducted for the committee based on data from this survey, focusing on children and youth in immigrant families living in San Diego who were from Mexico, the Philippines, Vietnam, Cambodia, and Laos (Rumbaut, 1998a). This study assessed possible risk and protective factors for low self-esteem and depressive symptoms, including gender, country of origin, intra-family and extra-family contexts and stressors, educational aspirations and achievement, language preference and skills, and physical looks and popularity with the opposite sex.
The study found lower self-esteem and higher depressive symptoms among youth in immigrant families for girls and for children experiencing high parent-child conflict, low family cohesion, recent serious illness or disability in the family, a high proportion of English-only spoken in the neighborhood, a school perceived as unsafe, dissatisfaction with physical looks, and lack of popularity with the opposite sex. 3 Also associated with low self-esteem were being of Filipino or Vietnamese origin, a recent family move to another home, low grades and educational aspirations, current limited English proficiency, and limited English proficiency in 1991 (see Table 3-3). Subsequent analyses of the Children of Immigrants Longitudinal Study (Rumbaut, 1998b) also found that self-reports of experiences of racial and ethnic discrimination were associated with a higher incidence of depressive symptoms. Self-esteem, in turn, is significantly associated
with the school performance and ambitions of these youth in immigrant families. Interestingly, the NELS data discussed above also revealed the importance of language factors and school experiences for feelings of self-efficacy among Hispanic and black youth in immigrant families, but not for Asian youth in immigrant families (see Kao, 1998).
Despite the potential importance of these factors for enhancing or reducing self-esteem and depression among children in immigrant families, national estimates of the prevalence of their experience with most of these factors are not available (exceptions are educational aspirations and achievements, as measured by NELS, and language proficiency, as measured by the decennial census).
Academic Achievement
Children from immigrant families face many potential challenges to their educational success. Many of them come from homes in which English is not the main spoken language. Parents are often unfamiliar or uncomfortable with avenues for participation in their children's schooling, and some have received little formal education. Immigrant families tend to settle in large urban areas that have troubled school systems (Fuligni, 1998). It follows that these children may experience difficulties at school—yet a handful of recent studies have begun to question this assumption.
Achievement Scores
Students in immigrant families appear to exceed prevailing assumptions about their school performance. In fact, some researchers have found that adolescents in immigrant families perform just as well if not better in school than their U.S.-born peers with U.S.-born parents (Fletcher and Steinberg, 1994; Fuligni, 1997; Kao and Tienda, 1995; Rosenthal and Feldman, 1991; Rumbaut, 1995, 1998b). Analysis commissioned by the committee from the National Educational Longitudinal Survey of 1988 corroborated this broad conclusion (Kao, 1998). Specifically, first- and second-generation children nationally have slightly higher
TABLE 3-3 Predictors of Self-Esteem and Depressive Symptoms Among Children of Immigrants: 1995-96a
|
|
Self-Esteem (Mean = 3.298) |
CES-D Depression (Mean = 1.681) |
||||||
|
Predictor Variables |
Beta |
T-ratio |
p |
ΔR2 |
Beta |
T-ratio |
p |
ΔR2 |
|
Gender, Age at Arrival, Ethnicity: |
|
|
|
.033*** |
|
|
|
.032*** |
|
Gender (O=male, 1=female) |
-.056 |
(-3.12) |
** |
|
.165 |
(7.72) |
*** |
|
|
Age at arrival in the U.S.b |
|
|
NS |
|
.044 |
(1.93) |
* |
|
|
Filipino |
-.075 |
(-3.85) |
*** |
|
|
|
NS |
|
|
Vietnamese |
-.065 |
(-3.49) |
*** |
|
|
|
NS |
|
|
Intra-Family Contexts and Stressors: |
|
|
|
0147*** |
|
|
|
.127*** |
|
Intact family |
|
|
NS |
|
-.048 |
-(2.36) |
* |
|
|
Parent-child conflict |
-.180 |
(-9.15) |
*** |
|
.200 |
(8.52) |
*** |
|
|
Family cohesion |
.091 |
(4.85) |
*** |
|
-.050 |
(-2.24) |
* |
|
|
Family economic situation worse |
|
|
NS |
|
.055 |
(2.70) |
** |
|
|
Family moved to another home |
.068 |
(3.97) |
*** |
|
|
|
NS |
|
|
Seriously ill or disabled since T1 |
-.056 |
(-3.34) |
** |
|
.045 |
(2.21) |
* |
|
|
Extra-Family Contexts and Stressors: |
|
|
|
.026 *** |
|
|
|
.024 *** |
|
English-only in neighborhood |
-.046 |
(-2.57) |
** |
|
.067 |
(3.13) |
** |
|
|
School perceived as unsafe |
-.086 |
(-4.77) |
*** |
|
.042 |
(1.97) |
* |
|
|
Teaching quality and fairness |
|
|
NS |
|
-.042 |
(-1.97) |
* |
|
|
School stress events experienced |
|
|
NS |
|
.050 |
(2.18) |
* |
|
|
Friends' no-college plans |
|
|
NS |
|
.058 |
(2.61) |
** |
|
|
Discrimination trumps education |
|
|
NS |
|
.054 |
(2.58) |
** |
|
grades and math test scores than third- and later-generation children, but their reading test scores are somewhat lower than those of third- and later-generation children (Kao and Tienda, 1995).
The relationship between achievement and generational status is not uniform, but varies with country of origin. As Table 3-4 shows, Mexican-origin children in every generation have similar grades and math test scores, although later generations have better reading test scores. Mexican-origin children in every generation also have substantially lower educational achievements than third- and later-generation white children; most of the difference for each generation is explained by lower parental education and family income among the Mexican-origin children (Kao, 1998).
Children in Chinese-origin immigrant families, especially the second generation, exceed third- and later-generation Chinese-origin children in grades and math test scores. However, only the second generation exceeds the third and later generations in reading test scores. First- and second-generation Chinese-origin children also exceed third- and later-generation white children in grades and math test scores; the second generation has higher reading scores as well. The superior grades and math test scores of first-generation Chinese-origin children are not explained by socioeconomic status, psychological well-being, or other school experiences. For the second generation, however, one-third to one-half of the superior performance is explained by these factors, particularly parental education and family income (Kao, 1998).
Among Filipino-origin children, the second generation also achieves better grades and math and reading test scores than the first or third and later generations (Table 3-4). Compared with third- and later-generation white children, first- and second-generation Filipino-origin children achieve higher grades. The second generation achieves higher math and reading test scores (Kao, 1998).
In the San Diego study, children in immigrant families at every grade level had higher grades than the district-wide average, and their school dropout rate was lower, even among Mexican-origin children, despite significant socioeconomic and linguistic handicaps. Factors contributing to these outcomes were these children's greater amount of time spent doing homework, lesser
time spent watching television, and the higher educational aspirations of the children and parents in immigrant families (Rumbaut, 1998a).
Family and School Support for Educational Success
The National Household Education Survey was used in analyses conducted for the committee to estimate exposure to risk factors for first- and second-generation children ages 3 to 8 for Hispanics, Asians, and whites (Nord and Griffin, 1998). Estimates for specific countries of origin are not possible because of the limited sample size and lack of information on countries of origin.
Among children generally, it has been found that family members can foster school success by engaging in various activities with their young children, including teaching them letters and numbers, reading to them, and working on projects with them (Table 3-5). For seven different activities of this type in 1996, among third- and later-generation white children, the proportion of children with parents engaged in such activities during the past week ranged from 75 to 93 percent; the proportions for children in immigrant families were about the same to no more than 11 percentage points smaller. Among children in immigrant families, the proportions were usually higher for second-generation children than for the first generation, and the proportions tended to be 10 to 15 percentage points lower for Hispanic children than for Asians (Nord and Griffin, 1998).
It has also been found that, among parents generally, they can foster school achievement by taking their children on a variety of educational outings (Table 3-5). Estimates of the proportion of children whose parents took them on six different types of outings in 1996 ranged widely from 12 to 65 percent and did not vary systematically between immigrant and U.S.-born children, between first- and second-generation immigrants, or between Hispanic and Asian children in immigrant families (Nord and Griffin, 1998).
Parental involvement in their children's schools is a third set of activities that has been found for children generally to foster school achievement (Table 3-5). Among third- and later-generation children in 1996, 68 percent of whites had parents highly in-
TABLE 3-4 Descriptive Characteristics of 8th Grade Youth
|
|
CHINESE |
FILIPINOS |
||||
|
|
Immigrant Generation |
Native-born of Foreign-born Parents |
Native-born of Native-born Parents |
Immigrant Generation |
Native-born of Foreign-born Parents |
Native-born of Native-born Parents |
|
Self-efficacy, or locus of control |
-0.241c |
0.011 |
0.073 |
-0.156 |
0.011 |
-0.006 |
|
|
-0.591 |
-0.567 |
-0.757 |
-0.631 |
-0.553 |
-0.806 |
|
Self-concept |
-0.115 |
-0.021 |
-0.058 |
-0.043 |
0.023 |
-0.33 |
|
|
-0.644 |
-0.709 |
-0.659 |
-0.578 |
-0.641 |
-0.561 |
|
Alienation, or unpopularity |
0.349c |
0.283b |
0.192 |
0.207 |
0.198 |
0.312 |
|
|
-0.479 |
-0.453 |
-0.402 |
-0.407 |
-0.4 |
-0.479 |
|
Middle school grade point average |
3.356c |
3.447c |
2.992 |
3.203b |
3.247c |
3.013 |
|
|
-0.654 |
-0.568 |
-0.957 |
-0.687 |
-0.689 |
-0.74 |
|
Math test scores |
56.802c |
61.363c |
53.077 |
50.736 |
56.085c |
53.651 |
|
|
-9.35 |
-8.531 |
-13.564 |
-9.6 |
-9.888 |
-11.786 |
|
Reading test scores |
49.480b |
58.204c |
49.797 |
49.181b |
54.587a |
55.297 |
|
|
-10.166 |
-7.887 |
-10.538 |
-9.219 |
-9.239 |
-9.983 |
|
Parents' education |
14.045a |
15.944c |
14.923 |
15.426c |
15.896c |
13.875 |
|
|
-2.758 |
-3.252 |
-2.607 |
-1.973 |
-2.214 |
-1.147 |
|
Family income (in $10,000) |
3.353c |
6.160c |
4.708 |
3.912 |
5.558a |
3.797 |
|
|
-3.49 |
-4.481 |
-4.247 |
-3.044 |
-4.165 |
-1.382 |
|
Home language use Non-English language only |
0.201c |
0.111c |
0.038 |
0.139c |
0.217c |
0 |
|
|
-0.403 |
-0.316 |
-0.196 |
-0.347 |
-0.414 |
0 |
|
MEXICAN |
OTHER HISPANICS |
WHITES |
||||
|
Immigrant Generation |
Native-born of Foreign-born Parents |
Native-born of Native-born Parents |
Immigrant Generation |
Native-born of Foreign-born Parents |
Native-born of Native-born Parents |
Native-born of Native-born Parents |
|
-0.282c |
-0.151c |
-0.113c |
-0.086b |
-0.049a |
-0.068b |
0.056 |
|
-0.619 |
-0.626 |
-0.633 |
-0.62 |
-0.684 |
-0.685 |
-0.605 |
|
-0.148b |
-0.098b |
-0.025 |
0.012 |
0.003 |
-0.025 |
-0.016 |
|
-0.62 |
-0.649 |
-0.663 |
-0.656 |
-0.642 |
-0.683 |
-0.662 |
|
0.288c |
0.263c |
0.140a |
0.219 |
0.166 |
0.20 |
60.17 |
|
-0.454 |
-0.441 |
-0.348 |
-0.416 |
-0.373 |
-0.405 |
-0.376 |
|
2.707c |
2.760c |
2.743c |
2.853 |
2.796b |
2.803b |
2.959 |
|
-0.734 |
-0.7 |
-0.743 |
-0.746 |
-0.681 |
-0.747 |
-0.751 |
|
45.393c |
45.639c |
46.383c |
46.970c |
48.547c |
46.674c |
52.547 |
|
-8.721 |
-7.891 |
-8.903 |
-10.121 |
-9.844 |
-9.103 |
-9.837 |
|
43.420c |
45.772c |
47.671c |
47.662c |
48.484c |
47.613c |
52.355 |
|
-8.59 |
-8.575 |
-9.193 |
-9.732 |
-9.591 |
-9.658 |
-9.717 |
|
11.200c |
11.887c |
13.066c |
13.512c |
14.000b |
14.033b |
14.546 |
|
-2.071 |
-2.165 |
-1.997 |
-2.968 |
-2.984 |
-2.4 |
-2.433 |
|
1.796c |
2.239c |
2.773c |
2.990c |
3.783b |
3.290c |
4.648 |
|
-1.869 |
-2.037 |
-2.103 |
-3.324 |
-4.008 |
-2.446 |
-3.9 |
|
0.251c |
0.169c |
0.112c |
0.187c |
0.218c |
0.045c |
0.007 |
|
-0.435 |
-0.375 |
-0.315 |
-0.391 |
-0.414 |
-0.208 |
-0.085 |
|
|
CHINESE |
FILIPINOS |
||||
|
|
Immigrant Generation |
Native-born of Foreign-born Parents |
Native-born of Native-born Parents |
Immigrant Generation |
Native-born of Foreign-born Parents |
Native-born of Native-born Parents |
|
School experiences Ever repeat |
0.121 |
0.029b |
0.208 |
0.119 |
0.027c |
0.2 |
|
|
-0.327 |
-0.167 |
-0.415 |
-0.325 |
-0.164 |
-0.414 |
|
Currently enrolled in bilingual program |
0.144c |
0.037 |
0.043 |
0.091b |
0.009 |
0 |
|
|
-0.353 |
-0.191 |
-0.209 |
-0.289 |
-0.096 |
0 |
|
N |
134 |
107 |
25 |
108 |
114 |
16 |
|
a p<.05 b p<.01 c p<.001 Source: The National Education Longitudinal Study of 1988. Kao (1998). |
||||||
volved in school, somewhat more than the 59 percent for Hispanics and 56 percent for blacks. Among children in immigrant families, the proportion with parents highly involved in school was 57 percent, although most of the difference between these children and third- and later-generation white children was accounted for by the higher proportion with a moderate level of parental involvement. Parental involvement was greater for the second generation than the first (58 versus 50 percent highly involved). Among children in immigrant families, Hispanics were less likely then Asians to have highly involved parents (49 versus 57 percent) (Nord and Griffin, 1998).
Early childhood programs prior to kindergarten help children prepare for school. The proportions attending early childhood programs among third- and later-generation children were 58, 66, and 47 percent, respectively, for whites, blacks, and Hispanics, compared with 42 percent for children in immigrant families. The
|
MEXICAN |
OTHER HISPANICS |
WHITES |
||||
|
Immigrant Generation |
Native-born of Foreign-born Parents |
Native-born of Native-born Parents |
Immigrant Generation |
Native-born of Foreign-born Parents |
Native-born of Native-born Parents |
Native-born of Native-born Parents |
|
0.273c |
0.214c |
0.214c |
0.184 |
0.18 |
0.212b |
0.148 |
|
-0.447 |
-0.41 |
-0.41 |
-0.39 |
-0.386 |
-0.409 |
-0.355 |
|
0.141c |
0.067c |
0.047 |
0.147c |
0.062a |
0.069b |
0.034 |
|
-0.349 |
-0.25 |
-0.212 |
-0.356 |
-0.242 |
-0.254 |
-0.182 |
|
215 |
578 |
763 |
121 |
195 |
242 |
13952 |
second generation was more likely than the first to attend such programs, and Hispanic children in immigrant families were slightly less likely than Asians to attend such programs (Nord and Griffin, 1998).
Children generally have been found to learn better if the schools they attend are well-disciplined and parental participation may be encouraged by a variety of school practices that foster such involvement. In parental ratings of children's schools along 10 dimensions, the proportion with favorable or very favorable parental responses was 45 to 67 percent for third- and later-generation white children. The proportions with favorable ratings were 2 to 10 percentage points lower along most dimensions for third- and later-generation blacks and Hispanics. These proportions varied between about 15 percentage points less and 15 percentage points more for third-generation children. They also varied substantially but in no specific direction for first- and
TABLE 3-5 Percent with Parents Reporting Selected Family Educational and School Experiences for Children Ages 3 to 8 by Generation and for Third- and Later-Generation Children by Race and Ethnicity: 1996
|
|
|
First and Second Generations |
|
|
Characteristic |
Children 3-8 Years |
Total |
First Generation |
|
Total (thousands) |
22,959 |
3,213 |
430 |
|
Family Involvement at Home |
|
|
|
|
In the past week, someone in family: |
|
|
|
|
Taught child letters, words, or numbersa |
93% |
92% |
86% |
|
Taught child songs or musica |
76 |
73 |
68 |
|
Took child along while doing errandsa |
95 |
91 |
97 |
|
Number of times read to child:b |
|
|
|
|
Not at all |
7 |
11 |
13 |
|
Once or twice |
20 |
26 |
34 |
|
3 or more times |
28 |
25 |
23 |
|
Every day |
44 |
37 |
31 |
|
Told child a story |
77 |
76 |
74 |
|
Worked on arts and crafts project with child |
72 |
65 |
59 |
|
Played a game, sport, or exercised with child |
92 |
86 |
82 |
|
Involved child in household chores |
95 |
86 |
83 |
|
Worked on a project with child like building, making or fixing somethingc |
67 |
56 |
51 |
|
In the past month, someone in the family: |
|
|
|
|
Visited the library with child |
44 |
38 |
32 |
|
Went to a play, concert, or other live show with the child |
30 |
26 |
21 |
|
Visited an art gallery, museum, or historical attraction with child |
20 |
20 |
17 |
|
Visited a zoo or aquarium with child |
17 |
23 |
21 |
|
Talked with child about family history or ethnic heritage |
52 |
55 |
60 |
|
Attended an event with child sponsored by a community, ethnic, or religious group |
50 |
41 |
39 |
|
Attended an athletic or sporting event in which child was not a player |
33 |
22 |
12 |
|
|
|
|
|
Third and Later Generations |
|||
|
Second Generation |
Hispanic |
Asian |
White |
Total |
White |
Black |
Hispanic |
|
2,782 |
1,734 |
239 |
837 |
19,746 |
14,166 |
3,326 |
1,652 |
|
93% |
90% |
97% |
94% |
94% |
93% |
96% |
91% |
|
73 |
70 |
72 |
78 |
76 |
76 |
83 |
69 |
|
90 |
88 |
79 |
99 |
95 |
96 |
94 |
94 |
|
11 |
14 |
6 |
7 |
7 |
6 |
8 |
8 |
|
25 |
32 |
18 |
17 |
19 |
17 |
25 |
24 |
|
26 |
25 |
25 |
24 |
29 |
28 |
30 |
29 |
|
38 |
29 |
51 |
51 |
45 |
48 |
37 |
39 |
|
77 |
71 |
83 |
84 |
77 |
78 |
73 |
79 |
|
66 |
59 |
74 |
74 |
73 |
75 |
66 |
72 |
|
87 |
81 |
92 |
94 |
93 |
94 |
92 |
87 |
|
86 |
84 |
74 |
90 |
96 |
97 |
95 |
92 |
|
58 |
47 |
59 |
69 |
68 |
70 |
63 |
67 |
|
38 |
27 |
54 |
51 |
45 |
47 |
40 |
39 |
|
27 |
21 |
34 |
33 |
30 |
29 |
36 |
27 |
|
20 |
15 |
24 |
27 |
20 |
19 |
22 |
20 |
|
23 |
20 |
32 |
26 |
16 |
14 |
23 |
21 |
|
54 |
52 |
50 |
61 |
51 |
47 |
65 |
54 |
|
41 |
35 |
38 |
51 |
51 |
52 |
52 |
43 |
|
24 |
18 |
19 |
30 |
35 |
36 |
33 |
27 |
|
|
First and Second Generations |
||
|
Characteristic |
Children 3-8 Years |
Total |
First Generation |
|
Family Involvement at School |
|
|
|
|
Parents' involvement in schoold |
|
|
|
|
Low |
15 |
17 |
17 |
|
Moderate |
21 |
26 |
33 |
|
High |
64 |
57 |
50 |
|
Parent attended a general school meeting |
83 |
82 |
78 |
|
Parent attended class or school event |
67 |
61 |
60 |
|
Parent volunteered at school |
51 |
38 |
24 |
|
Parent attended parent-teacher conference |
79 |
82 |
84 |
|
NOTE: Hispanic children are designated as such. They are not included in any of the other racial or ethnic categories. The Total columns include all children. Because of rounding, percents may not sum to 100. |
|||
second-generation children and for Hispanic and Asian children in immigrant families (Nord and Griffin, 1998).
Educational Aspirations and School Problems
Analyses conducted for the committee based on the National Education Longitudinal Survey of 1988 (Kao, 1998) indicate that children in immigrant families, both the first and second generations, have higher educational aspirations and are more likely to aspire to graduate from college than are third- and later-generation adolescents. Among Chinese, Filipino, and Mexican children, although small sample sizes require that the findings be viewed as preliminary, educational aspirations are highest among Chinese and Filipinos in immigrant families, somewhat lower among third- and later-generation children generally, and still lower for
third- and later-generation Chinese and Filipino children and all generations of Mexican-origin children.
Consistently, the most common school problems identified among youth in immigrant families are behavioral problems and learning difficulties (Aronowitz, 1984; Gil et al., 1994). When asked to assess children in immigrant families, teachers tend to identify more behavioral problems than do parents. It is difficult to assess from the literature whether these higher rates of behavioral problems and learning difficulties that teachers report are due to their misinterpretation of normatively different behavior or the effects of acculturative stresses, such as language difficulties and perceived discrimination at school. It is likely that both of these factors not only are present, but also interact in the school setting. In addition, the negative evaluations that teachers make
may have a negative effect on the self-esteem of children in immigrant families, especially among adolescents.
Smaller-scale studies present a more complex picture of achievement motivation and school problems among different groups of youth in immigrant families. For example, Gil and colleagues (1994) found that, among second- and third-generation Hispanic adolescents, high acculturation was associated with high academic motivation. They also found that second- and third- and later-generation adolescents with low acculturation who perceived significant discrimination from the host society were most likely of all the adolescents studied to experience low self-esteem and poor school performance. Research by Rousseau and colleagues (1996) in Montreal illustrated that the school's perceptions of different immigrant groups may also interact with student motivation to produce worse outcomes for some groups of children than others. In this study, although the school performance of first-generation Southeast Asian and Central American immigrant children did not vary significantly, teachers identified more learning problems in the Central American children. They also subscribed to the stereotype of Asians as a ''model minority" in their differential perceptions of these groups of students.
In another study of Canadian children, Munroe-Blum and colleagues (1989) highlighted the effect of social status on the school performance and mental health of children in immigrant families. In this large study, immigrant status was not associated with either poor school performance or more mental health problems. However, children in immigrant families were more likely to be poor, but less likely to have access to welfare and other social services. The paradoxical nature of the findings was that, given the worse social status of children in immigrant families, there were no overall statistical differences in outcomes, suggesting resilience among these children, an emerging theme in the research literature.
What cannot be ascertained from this cross-sectional study is the effect of enduring social disadvantage on children. Other studies indicate that, in the United States, the persistence of disadvantage is structured along racial lines, with black children experiencing more serious problems (Kao and Tienda, 1995;
Phinney and Chavira, 1995) and Asian children fewer problems. Better statistical analyses are needed to look more closely at different ethnic populations within these broad groupings. However, there are anecdotal indications that Hmong and other tribal people from Southeast Asia are not faring as well as other Asians; that the Cuban experience is quite different from that of Nicaraguans and Salvadorans; and that Jamaicans, Haitians, and blacks also have divergent experiences.
SUMMARY
Although we reiterate that conclusions based on the committee's analysis must be considered preliminary, many measures reported for children in immigrant families indicate that they are healthier than U.S.-born children in U.S.-born families. This relative advantage tends to decline with length of time in the United States and from one generation to the next. In addition, children in immigrant families are at particular risk for certain health problems.
Specifically, children in immigrant families experience fewer specific acute and chronic health problems than do U.S.-born children in U.S.-born families, according to parent reports, including acute infectious and parasitic diseases; acute ear infections; acute accidents; chronic respiratory conditions such as bronchitis, asthma, and hay fever; and chronic hearing, speech, and deformity impairments. For children of Mexican origin, parents in immigrant families report fewer acute injuries and poisonings and fewer limitations on major activities than U.S.-born parents in U.S.-born families. First-generation immigrant adolescents also report lower levels of neurological impairment, obesity, and asthma, and fewer health risk behaviors such as early sexual activity; use of cigarettes, alcohol, marijuana, or hard drugs; delinquency; and use of violence. Many of these health problems and risk behaviors tend, however, to increase with length of residence in the United States or from one generation to the next.
Similarly, second-generation infants are less likely to have low birthweight or to die in the first year of life than are third- and later-generation infants. Comparatively low levels of cigarette
smoking and alcohol consumption during pregnancy among immigrant mothers contribute substantially to their more favorable birth outcomes; additional potentially important factors include lower levels of drug use and a healthier diet.
Perhaps as we look to the future, protective factors that lead to comparatively favorable outcomes for first- and second-generation children will be reinforced, or more easily maintained, as a result of the increasing size and the geographic concentration of the immigrant population, especially from Mexico, providing greater opportunities to retain positive cultural characteristics.
Not all indications are favorable, however. Children in immigrant families from Mexico, for example, are more likely to be reported by parents as being in fair to poor health and as having teeth in only fair to poor condition. They are also more likely to exhibit elevated blood lead levels. In addition, parents in immigrant families are, paradoxically, somewhat less likely than those in U.S.-born families to report their child's health as excellent or very good, despite the fact that they report their children to have fewer specific acute and chronic health problems. Tuberculosis, hepatitis B, parasitic infections, and elevated levels of lead in the blood are also of particular concern for children in immigrant families from certain high-risk countries of origin.
The paradoxical finding that children in immigrant families have better health than U.S.-born children in U.S.-born families on most available measures—despite their overall lower socioeconomic levels, higher poverty rates, and racial or ethnic minority status—suggests that strong family bonds among immigrants may act to sustain cultural orientations leading to healthful behavior, or that other unknown social or cultural factors may serve to protect them. Thus, children may be protected by key aspects of culture brought from their home country. It is important to also keep in mind that most of these findings (with the exception of the infant outcomes) are based on parental and self-report data, which are themselves likely to be affected by cultural factors.
The apparent deterioration of the health of children in immigrant families the longer they reside in the United States and from one generation to the next suggests that protective aspects of immigrant culture may fade as assimilation into the mainstream American culture occurs, allowing deleterious effects of low so-
cioeconomic status, high poverty, and racial or ethnic stratification to emerge. A more complete understanding of the health situation of children in immigrant families and the reasons for change through time will depend on additional study of these children in the United States that is informed by knowledge about the health of children in countries of origin, and hence providing an explicitly cross-national comparative perspective.
Firm conclusions about similarities and differences between adolescents in immigrant and U.S.-born families regarding psychological well-being, academic success, and other measures of successful adaptation to American society are difficult to draw for reasons that include the small immigrant samples in available studies. However, adolescents in immigrant families appear to sustain positive feelings about themselves and their well-being while also perceiving that they have relatively less control over their lives and are less popular with their peers at school. They also report having higher educational aspirations, although these may deteriorate across generations.
At early ages, parents can foster school success among their young children by teaching them letters and numbers, reading to them, working on projects with them, taking them on educational outings, and getting involved in the children's school. Young children also learn better in well-disciplined schools and if parental participation is encouraged by the school. Early childhood programs prior to kindergarten help children prepare for school. Children do not differ systematically along most of these dimensions, with the exception that children in immigrant families are much less likely to be enrolled in early childhood programs or attend Head Start if they are eligible.
Children in immigrant families nationally have somewhat higher middle school grade point averages and math test scores than do U.S.-born children in U.S.-born families, although reading test scores among the first generation are lower than for later generations. Differences across children with various countries of origin appear quite large, however. For example, adolescents in Chinese-origin immigrant families have grade point averages and higher math test scores than third- and later-generation Chinese-origin or white children. In contrast, Mexican-origin children of all generations have grade point averages and math test
scores that are similar to each other, but that are much lower than for third- and later-generation white children. Corresponding to the declines in educational aspirations across generations, however, there is evidence that, among Chinese-origin and Filipino-origin children, the especially strong achievement records of the second generation are not sustained.




















































