
Introduction to the Subject
Lisa F. Berkman
Harvard School of Public Health
Dr. Berkman opened her remarks by citing the six reports of the National Research Council and IOM that inspired this symposium. It is “stunning,” she noted, that despite these reports’ diversity—addressing children, aging, research priorities, training, health promotion, and interventions, among other topics—they all come to similar conclusions. They consistently say that social and behavioral conditions are major determinants of health and that this realization implies new ways to do science in order to improve the health of the public.
“Just as the natural sciences—biology and chemistry and even physics—have reorganized in terms of how they fundamentally teach and train people,” said Dr. Berkman, “today we are building on the same kind of technological advancements and real achievements in the social sciences, and we are at a similar kind of crossroads.”
The reports note the importance of a new concept, “population health,” developed initially by Jeffrey Rose in 1992. He said that it was critical not only to ask why some individual patients get sick but also why this population has its own distribution of risk. He pointed out, for example, the differences in blood pressure patterns between London civil servants and Kenyan nomads; these distributions overlapped only slightly. Similarly, Dr. Berkman noted, virtually everyone in Finland today would have high serum cholesterol levels by Japanese standards (see Figure A).
A major population health issue in the United States, she said, is the epidemic of obesity among children. Three times as many kids in the 1990s
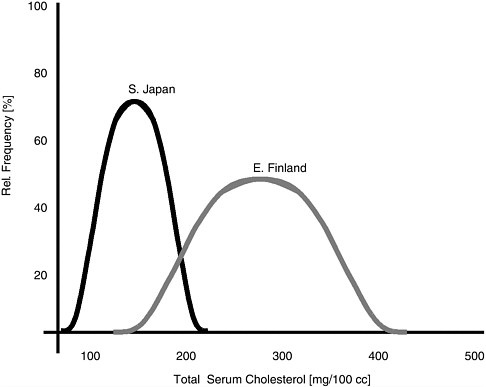
FIGURE A Serum cholesterol levels among populations in Japan and Finland.
were obese by standards set in the mid-1960s (see Figure B). More fundamentally, why has the mean weight of all children in the United States risen over the past 20 or 30 years, causing the percentage of kids in the tails of the distribution to be obese?
Another area of population health in which we have acquired a great deal of evidence, Dr. Berkman said, is social stratification and inequality. For example, between 1969 and 1998, mortality rates dropped dramatically among men in every socioeconomic group. But those in the lower socioeconomic status groups had higher mortality rates, and the gap between the highest and lowest groups actually grew.
There are dramatic health disparities in racial and ethnic groups as well. In Table 1, which shows life expectancy for white men and women and black men and women from 1950 to 1996, life expectancy is improving for everyone. But as black men enter the 21st century they have a life expectancy less than what white men enjoyed 46 years earlier. Black women do only a little better—their rates look like those of white women 36 years earlier.
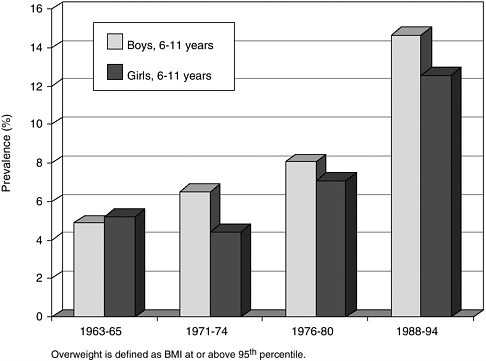
FIGURE B Obesity rates of children in the United States, 1963-1994.
Almost all the data suggest that the lower socioeconomic status of African Americans accounts for much, but not all, of this gradient, said Dr. Berkman. Some of the more important and innovative work in this area is identifying additional factors such as discrimination, which may lead to increased risk among certain racial and ethnic groups. “In a society where
TABLE 1 Life Expectancy at Birth for Blacks and Whites, 1950-1996
|
|
Whites |
Blacks |
||
|
|
Men |
Women |
Men |
Women |
|
1950 |
66.5 |
72.2 |
58.9 |
62.7 |
|
1960 |
67.4 |
74.1 |
60.7 |
65.9 |
|
1970 |
68.0 |
75.6 |
60.0 |
68.3 |
|
1980 |
70.7 |
78.1 |
63.8 |
72.5 |
|
1990 |
72.7 |
79.4 |
64.5 |
73.6 |
|
1996 |
73.9 |
79.7 |
66.1 |
74.2 |
in the next 50 years we expect the minority to become the majority,” she said, “we cannot afford to leave this issue unresolved.”
Another area of research in which we have accumulated a great deal of evidence, Dr. Berkman said, is the importance of social relationships. Literally hundreds of studies now link social isolation to increased mortality, morbidity, and lower survival. And scores of studies identify attachment and caregiving as critical components of early childhood development.
Some of the most far-reaching and innovative research today has been on the “power of place.” While research on neighborhoods has long been a tradition in social science, new findings indicate that work environments, school environments, cultures, and other social contexts also play important roles in determining individuals’ health outcomes.
Given the consistency of such new findings in social science research, Dr. Berkman said, the six National Research Council and IOM reports exhibit several common, and critical, themes. Virtually all recognize that behaviors occur in a social context. If we could characterize earlier waves of behavioral interventions as individualistic—focusing on smoking cessation among individuals, for instance—the new wave of behavioral interventions is built on a recognition that where we live and work and who we talk to, and what kind of resources we have and where we buy our groceries, all shape our behavior.
Another critical theme of these reports is the importance of understanding multiple determinants of health, or multiple levels of influence, simultaneously. Social and economic policies at the upper levels, on down through institutions, neighborhoods, living conditions, social relationships, individual risk factors, genetic/constitutional factors, and pathophysiologic pathways, all contribute to individual and population health.
A third pervasive theme relates to life course and development; issues of cumulative disadvantage, latency, precursors of later resiliency, or disease risk are now central themes in many of these reports. However, this life-course perspective requires substantial new investments in the kinds of studies that we do, said Dr. Berkman. Longitudinal studies, whether they are cohorts starting from birth or young adulthood, or simply cohorts that take us through career trajectories in middle and older age, are profoundly needed in the United States.
The fourth theme of these reports, Dr. Berkman said, revolves around understanding the pathways that link the macro social structure to biologic mechanisms of disease causation. Harmful social experiences, and the cu-
mulative wear and tear on the body through repeated activation of physiologic stress responses, affect a life’s course.
Examples of such stress paradigms based on social conditions include the brain, where we see hippocampal shrinkage and memory loss; endocrine systems, where we see things like diabetes; cardiovascular systems that influence hypertension and coronary heart disease; and reproductive systems that may be related to low birth weight and ovarian function.
The persuasive evidence discussed in the reports has three basic implications for social and behavioral approaches to health, Dr. Berkman said. The first is that theories of disease causation that focus primarily on the individual should be complemented by the systematic patterning of risk across social contexts.
Second, we have new outcomes. No longer is it adequate to think only of mortality or disease-specific morbidity. We are dealing with health in a world where new issues of child development and aging—assessments of functioning from the standpoint of cognitive ability, optimal performance, and disability—are becoming increasingly important.
Third, we need new ways of intervening that integrate what we have recently learned. Ultimately, of course, our goal is not only to understand the determinants of health but to improve health. That means we will also need to develop new methods of training and new partnerships to improve the likelihood that interventions will be successful.
Thus, the next steps need to be really bold ones, Dr. Berkman said. They will require reconfigurations in funding opportunities across National Institute of Health (NIH) and foundations, for example, changes in educating the next generations of scientists and practitioners, and dissemination and press coverage that clearly get out the message that improvements in health depend in large part on changes in the social environment.





