
1
Preterm Birth and Its Consequences*
The Roundtable on Environmental Health Sciences, Research, and Medicine is comprised of key stakeholders in environmental health. They meet on a regular basis to discuss areas of mutual concern in a neutral environment. The purpose is to promote discussion, but not to come to consensus. Sometimes, the Roundtable convenes workshops to explore issues in greater depth and facilitate discussion. This is a summary of a workshop convened by the Roundtable on October 2–3, 2001, to look at the issues surrounding the role of the environment in premature birth. The summary has been prepared by the workshop rapporteur as a factual summary of what occurred at the workshop and should not be construed as consensus by the Roundtable or the Institute of Medicine (IOM).
PRETERM BIRTH
More than 400,000 babies are born prematurely each year in the United States. These early births, defined as those occurring before the thirty-seventh week of pregnancy, result in infants who are small and immature—weighing less than 5.5 pounds—and who are at greater risk of death than those born at full term. Indeed the statistics show the struggle that these children face. Disorders relating to short gestation and low birth weight are among 10 leading causes of infant mortality (Hoyert et al., 2001). Earlier estimates suggest that approximate-
ly 75 percent of all infant deaths in the first month of life occur in premature infants (McCormick, 1985). Premature babies often spend months fighting for survival and struggling to overcome illness, and the impact on families is often long-lasting both emotionally and financially. In economic terms, estimates suggest that in the first year of life alone, a preterm birth costs on average about $59,730 (Rogowski, 1998). Furthermore, approximately 35 percent of all expenditures for newborns and approximately 10 percent of all medical expenditures for children are associated with preterm birth (Lewit et al., 1995). Emotionally, the impact on families is harder to quantify but is reputed to be substantial.
Approximately 35 percent of all expenditures for newborns and approximately 10 percent of all medical expenditures for children are associated with premature birth.
WHAT IS PRETERM BIRTH?
The normal length of pregnancy is 40 weeks (plus or minus 2 weeks) as calculated from first day of the woman’s last normal menstrual cycle. A baby born prior to week 37 of gestation is considered premature. However, it is the 1 percent or less of babies who are born at less than 32 weeks and/or who weigh less than 1,000 grams that account for most of the long-term morbidity and mortality observed in premature infants, according to Robert Goldenberg, University of Alabama at Birmingham.
Of all premature babies, approximately 50 percent are born at 35 and 36 weeks of gestation.
Preterm births are classified into two categories: (1) indicated—those deliveries initiated by the clinician for the benefit of either the fetus or the mother, and (2) spontaneous preterm birth—those that follow either spontaneous preterm labor or spontaneous rupture of the membranes. Approximately 20 percent of preterm births are indicated, usually occurring because the mother is severely ill with a life-threatening condition or the fetus shows signs of deterioration and risk of fetal death. Spontaneous preterm labor accounts for the remaining 80 percent. Approximately 30 percent of total preterm births follow spontaneous rupture of the membranes, while the remaining 50 percent follow spontaneous preterm labor, noted Goldenberg. Spontaneous preterm births are often divided into those that occur early and those that occur later. Early preterm births, occurring at less than 30 week’s gestation, generally are associated with an intrauterine infection or placental hemorrhage. Later preterm births, which occur be-
Later preterm babies, which occur between 35 and 36 weeks gestation, are, for the most part, not associated with infection, placental hemorrhage, or a specific etiologic factor.
tween 35 and 36 weeks gestation, are, for the most part, not associated with infection, placental hemorrhage, or a specific etiologic factor. Instead, these preterm births appear to happen when the normal mechanisms responsible for term labor take place earlier than usual. Women who have a preterm birth at 35–36 weeks gestation often have an increased number of risk factors—they are under-weight, they smoke, and/or they have various psychosocial characteristics—but often no specific precipitating cause is identified for the spontaneous labor or rupture of membranes.
Goldenberg further noted that preterm birth is a heterogeneous entity, with distinctive contributing pathways, which presents a challenge to researchers who study the mechanisms and prevention of preterm birth. Many studies separate spontaneous from medically indicated preterm delivery. Although this is a reasonable strategy, it does not account for the fact that the common indications for medical intervention and early delivery (fetal growth restriction, hypertension) are also independent risk factors for spontaneous preterm birth, stated Goldenberg. Some risk factors may be shared across spontaneous and indicated preterm births, while others are likely to differ. Preterm birth also has been categorized based on clinical presentation (idiopathic preterm labor, preterm rupture of membranes) or on the severity of prematurity as defined by the duration of gestation. More novel approaches to categorization consider the underlying etiologic process—for example, infection/or inflammation and vascular compromise. The challenges related to classification need to be addressed in order to better define end points for epidemiological studies, according to some participants.
INCIDENCE
Preterm birth is not an infrequent event in both the developing and the developed countries. Although the incidence rate is higher in developing countries, the United States and other industrialized countries have seen a steady increase in the incidence of preterm births, noted Goldenberg. From 1981 to 1994, approximately 9 to 10 percent of all births were preterm (see Figure 1.1). This increase continued until 1999 when the incident rate was 11.8 percent (Ventura et al., 2001). For the first time in a decade, a decrease in the number of preterm births was reported for the vital statistics for 2000 (Martin et al., 2002). Most of the increase in preterm birth since 1981 has been among moderately preterm births—those infants born between 32 and 36 weeks of gestation (Ventura et al., 2001). The very preterm birth rate—approximately 1.93 percent (Martin et al., 2002)—has fluctuated little since 1990. Catherine Spong, National
It is better to have a preterm birth at 34, 35, or 36 weeks where the baby lives, than a stillborn baby at full term.
Robert Goldenberg
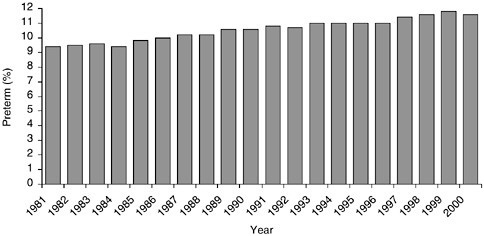
FIGURE 1.1 The incident rate of preterm birth in the United States rose from approximately 9 percent in 1981 to 11.8 percent in 1999. Calendar year 2000 marked the first time in a decade that a decrease in the incidence rate for premature birth was noted.
SOURCE: Martin et al., 2002.
Institute of Child Health and Development, suggested that some of the increase is due to the increased use of assisted reproductive technologies; however, predominantly, the increase cannot be explained.
Similarly in Canada, the preterm birth rates also increased during the same period according to Daniel Krewski of the University of Ottawa. He noted that despite the increase, the infant mortality rate has been steadily decreasing at all gestational ages from what it was a decade ago. While this is good news, Goldenberg cautioned that prematurity or reducing prematurity is not the end point. The major goal is to have both healthy babies and mothers. It is better to have a preterm birth at 34, 35, or 36 weeks where the baby lives, than a stillborn baby at full term.
African Americans in the United States have a higher incidence of preterm birth (17.4 percent) than Caucasians (10.4 percent).
Hidden within the statistics is the disparity among populations, according to several participants. African Americans in the United States have a higher incidence of preterm birth (17.4 percent) than Caucasians (10.4 percent). The demographic differences have led some investigators to characterize preterm birth as a disease of poverty. Interestingly, although African Americans have a higher rate of preterm birth, their incident rate has decreased consistently since 1990. During the same period, the preterm birth rate has remained the same for Hispanics, but the preterm birth rate for non-Hispanic whites has shown a steady
increase from 8.5 to 10.4 percent (Martin et al., 2002). The factors that contribute to the variation in the distribution of preterm birth across the U.S. population, particularly the higher incidence for African-American women, have not been determined. According to Goldenberg, more African-American women have bacterial vaginosis, histologic and clinical chorioamnionitis, postpartum endometritis, and genital tract infection, which may be risk factors. Further, some African-American women also may have a low-grade chronic intrauterine infection before or between pregnancies that may be the cause of repeated spontaneous preterm births. This finding appears to be unrelated to the age of onset of sexual activity or number of sexual partners.
LONG-TERM OUTCOMES OF PREMATURE INFANTS
Numerous advances, both technological and therapeutic, in neonatal intensive care have led to the improved survival of premature infants. Prior to 1940, the deaths associated with a preterm birth occurred either at or immediately following birth, according to Maureen Hack, Rainbow Babies and Children’s Hospital. Those babies who survived generally were born at 32 weeks of gestation (or later). Since the early 1960s, we have seen a steady increase in the survival rates of premature infants weighing between 1,000 and 1,500 grams and similar, albeit not as high, increases for those infants whose birth weight was well below 1,000 grams. Hack reported that when she started following premature children in the late 1970s, babies born at about 29 weeks’ gestation were being treated and some survived. In the 1980s, neonatologists were keeping babies alive at 26 weeks’ gestation, and in the 1990s, babies born at 23 or 24 weeks of gestation were surviving. Today, we still see a high percentage of mortality in infants born at less than 26 weeks of gestation; however, those born after 27 weeks of gestation have a greater probability of survival (Figure 1.2).
Using current methods of neonatal intensive care, we have reached the limits of survival for premature infants.
Maureen Hack
Hack speculated, however, that using current methods of neonatal intensive care, we have reached the limits of survival of premature infant, because there has been no significant change in the survival rates in recent years. Not surprisingly, the increase in survival rate of preterm infants has been associated with an increase in neonatal complications, including brain injury and chronic lung disease, which have been most common among the smallest and least mature infants.
Complications of prematurity include respiratory distress syndrome, brain hemorrhage, jaundice, and infections, according to Hack. Other complications
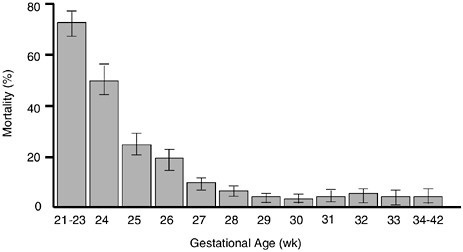
FIGURE 1.2 The percentage of neonatal mortality is inversely related to gestational age. Infants born at or after 27 weeks of gestation have a mortality rate less than 20 percent.
SOURCE: Lemons et al., 2001. © 2001 American Academy of Pediatrics. Reprinted with permission.
such as neurodevelopmental disabilities or chronic lung disease are not diagnosed or discernable at birth or shortly there, however, may extend over the course of a lifetime. These impacts have not been fully investigated. The majority of premature babies do not develop neurodevelopmental disabilities as assessed at birth or shortly thereafter; however, many of the impacts become apparent as the infant reaches school age. Overall, premature children require more services beyond routine care throughout childhood, including counseling, occupational therapy, physical therapy, special education, and special school arrangements.
Currently, health care professionals are reporting fewer incidences of blindness due to the increased use of laser and cryotherapy; however, other complications, such as cerebral palsy, have been on the rise for infants born at less than 28 weeks’ gestation since 1975 (Figure 1.3). These impairments are inversely related to gestational age and birth weight, such that the younger the gestational age, the greater is the likelihood of an infant having a neurological or a developmental impairment. Predictors of poor neurodevelopmental outcomes include the neonatal complications of prematurity as well as socioenvironmental risk factors. In addition, the same socioenvironmental factors that predispose the fetus to preterm birth usually continue after birth and may have deleterious effects on childhood health and development.
Major neurodevelopmental impairments, including cerebral palsy and mental retardation, that may result from preterm birth can be diagnosed in early
childhood. However, more subtle problems in behavior and functioning (such as poor visual–motor functioning, poor gross motor functioning, reduced math abilities, deficient attention skills, and hyperactivity) may be present at later ages even among children who have no overt neurodevelopmental sequelae. Although respiratory and other health problems tend to diminish during childhood and catch-up growth occurs among many of these children, school functioning problems often persist into adolescence. More preterm than term-born children fail grades, and fewer complete a high school education, noted Hack. Differences in intelligence between normal-term and premature children are evident even among premature children who weighed between 3 and 5 pounds at birth and who did not require neonatal intensive care.
Hack noted that studies by Breslau and colleagues (1994) in Detroit have shown that an increase in IQ test scores, both verbal and performance, accompanies increasing birth weight (Table 1.1).
Little research has been done on the health status of premature infants as they reach adulthood. Hack reported that premature infants displayed less deviant behaviors, less sexual activity, and less drug abuse in a cohort she studied until the individuals reached the age of 20. She further found that the low birth weight population had a lower rate of pregnancy (Hack et al., 2002). Some
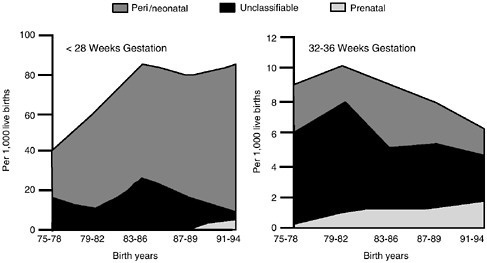
FIGURE 1.3 Since 1975 the prevalence rate of cerebral palsy in infants, whether the result of prenatal, perinatal, or unclassified causes, has been increasing for infants born at less than 28 weeks gestational age compared to infants born at age 32–36 weeks of gestation.
SOURCE: Hagberg et al., 2001. © 2001 Taylor & Francis. Reprinted with permission.
TABLE 1.1 Adjusted WISC-Ra Scores of Children in Three Low Birth Weight Levels and Normal Birth Weight
|
|
|
WISC-R IQ |
||
|
Birth Weight (grams) |
No. of Subjects |
Full scale IQb |
Verbal IQb |
Performance IQb |
|
≤ 1,500 |
76 |
95.8 (1.5) |
97.5 (1.6) |
94.8 (1.6) |
|
1,500–2,000 |
92 |
97.8 (1.4) |
99.2 (1.5) |
96.6 (1.4) |
|
2,000–2,500 |
300 |
102.3 (0.8) |
102.6 (0.8) |
101.5 (0.8) |
|
≥ 2,500 |
348 |
105.2 (0.7) |
105.6 (0.8) |
103.9 (0.7) |
|
aWISC-R Wechsler Intelligence Scale for Children-Revised. bLeast-square means and standard errors estimated in multiple regression analyses with population site, maternal IQ, maternal education, and race as covariates. SOURCE: Breslau et al., 1994. © 1994 American Medical Association. Reprinted with permission. |
||||
additional research has found that when these low-birth rate women have children, they have a greater probability themselves of giving birth to a low birth weight baby. The results of these studies need additional work in order to better understand the long-term and transgenerational effects of preterm birth.
MEASURING PREDICTORS OF PRETERM BIRTH
Preterm birth is a highly complex process influenced by multiple environmental factors, genetic factors, and gene-environment interactions. In fact, less than half of all preterm births are associated with an identifiable risk factor.
Preterm birth is a highly complex process influenced by multiple environmental factors, genetic factors, and gene–environment interactions. In fact, less than half of all preterm births are associated with an identifiable risk factor. Researchers have used epidemiology as the cornerstone for establishing risk factors and determining intervention strategies for preterm birth. Speakers and participants discussed many of these risk factors, which include biological, individual health behavior, and population factors (Box 1.1). Participants stressed the importance of defining risk factors, not just universally for all populations, but also for individuals or specific subgroups. This may allow the development of more targeted intervention strategies. Presently, the strongest predictors of preterm birth are limited to multiple gestation, prior preterm birth, and African-American ethnicity, according to David Savitz, University of North Carolina School of Public Health. However, research has failed to determine a predominant risk factor or factors, which suggests multiple causal pathways. While most previous studies have focused on
|
BOX 1.1
|
socioenvironmental or clinical variables, the role of genetic susceptibility and gene–environment interactions remains largely unexplored (see Chapter 2).
There are distinct issues when researchers characterize preterm birth as a reproductive end point, stated Savitz. He suggested that the idea of dividing preterm birth based on clinical presentation is of potential value but may be misleading in identifying subgroups with differing etiology. Providers often act in practice as though the determinants or risk factors are similar across the spectrum of severity of preterm birth. Just as the consequences of preterm birth vary depending on gestational age, participants considered if the etiologic factors differ and whether subgroups should be considered based on the severity of prematurity. Further, according to Savitz, there is a judgment on the part of the researchers of how inclusive or exclusive to make the outcomes of interest. For example, preterm birth and low birth weight often do not identify the same pregnancies. A high proportion of premature babies are not low birth weight babies; conversely, a high proportion of low birth weight babies are not premature. It is only at the extremes that these two measures predict each other well. As we begin to address these issues from a multidisciplinary approach, we may begin to make further strides in understanding the risk factors and mechanisms underlying preterm birth.
INTERVENTIONS IN PRETERM BIRTH
The goal of any pregnancy is to have labor and delivery occur at an appropriate time to ensure healthy babies and mothers. If premature infants were born with no co-morbidities, the fact that an infant was premature would be of little consequence. However, morbidities do occur in a significant number of preterm births, which has resulted in researchers proposing a number of prevention strategies aimed primarily at spontaneous preterm birth.
Interventions to reduce spontaneous preterm birth are categorized as either general or targeted. General interventions might include providing prenatal care,
improving the general quality of prenatal care, providing across-the-board nutritional supplementation, or providing social support or home visiting. More targeted, experimental interventions may include providing specific aspects of prenatal care—for example, risk screening; nutrition counseling; caloric supplementation; protein supplementation; iron supplementation; labor-inhibit-ing agents; drug, alcohol, and tobacco cessation programs; bed rest; hydration; and home uterine activity monitoring. However, these types of interventions have rarely been shown to be beneficial in reducing the rate of preterm birth. In fact, there is no evidence that any of the numerous strategies currently used to reduce preterm birth, when applied to various populations, are effective, according to Robert Goldenberg of the University of Alabama at Birmingham. This may be because current intervention strategies are often suggested from risk factors that although associated with preterm birth, may not be directly linked to preterm birth. Some participants suggest that additional research may be needed to better understand the processes underlying preterm birth and to develop better inventions. This section reviews the interventions discussed by various speakers and participants.
There is no evidence that any of the numerous strategies currently used to reduce preterm birth, when applied to various populations, are effective.
Robert Goldenberg
Antibiotics
Infections, such as bacterial vaginosis, syphilis, gonorrhea, and periodontal disease, have all been associated with increased rates of preterm birth and may account for the preterm births of unknown etiology. In the 1980s and 1990s, clinicians began to hypothesize that subclinical infections in either the umbilical cord, the deciduous space, or the amniotic cavity may result in a preterm birth, according to James Roberts, Magee-Women’s Research Institute. Romero et al. (1993) cultured amniotic fluid from women in preterm labor. They reported that women with a positive culture were more likely to have a preterm birth, whereas those with a negative culture did not. The mounting evidence of infection as a risk factor suggested that the use of antibiotics may be important for the prevention of preterm birth.
Various attempts at using antibiotics as an intervention for preventing preterm birth have had mixed results. Often antibiotics have been administered to women experiencing preterm labor to prevent or delay delivery. The result of the use of antibiotics in this situation has been inconsistent (see Table 1.2), said Goldenberg, and although two randomized studies, both using metronidazole and ampicillin, suggest that there may be some minimal benefit. Generally, how-
ever, the use of antibiotics alone in women who are in preterm labor has not been successful, and is not likely to have a major impact for women in developed countries.
Bacterial vaginosis is an independent risk factor associated with preterm birth, which is complicated by the fact that many women are asymptomatic. Treating pregnant women with asymptotic bacterial vaginosis with two doses of 2 grams of metronidazole 48 hours apart on two occasions was not effective in reducing preterm birth. However, some studies suggest that antibiotic administration for the treatment of bacterial vaginosis was effective in women who have had a prior preterm birth. Although the use of antibiotics in developing countries has been useful, this administration in developed countries has had mixed results. Since there is an association between preterm birth and infection, it may be possible that, as researchers learn more about underlying mechanisms, specific antibiotics may be useful in some clinical cases.
Prenatal Care
Prenatal care, which involves the provision of social support, home visiting, and nutritional counseling, has been hypothesized to be inversely related to the incidence of preterm birth. However, when studies have examined the data where the amount of prenatal care was increased (e.g., prenatal care was provided to a population that had none, more prenatal care to women who had been receiving little, more prenatal care in a location where only routine care was available), researchers failed to see a reduction in the incidence of preterm birth (Goldenberg and Rouse, 1998). Although prenatal care may not reduce or prevent preterm birth, it does have some benefits. For example, Goldenberg noted that increased prenatal care was effective in decreasing the rate of stillbirths and reducing term mortality in Alabama.
Bed Rest
Bed rest has been used to treat many conditions during pregnancy. It is a recommended treatment for first-, second-, and third-trimester bleeding; prevention of preterm labor in pregnancies with twins, triplets, or higher order multiples; prevention and treatment of preeclampsia; treatment of nonproteinuric hypertension and edema; and treatment of growth retardation. However, randomized studies have shown no improvement in outcomes associated with bed rest in conditions such as first-trimester bleeding; prevention and treatment of preeclampsia; treatment of nonproteinuric hypertension; and treatment of growth retardation, according to Goldenberg. Similarly, randomized studies have failed to show any benefits of bed rest associated with preterm labor (Goldenberg and Rouse, 1998). In the four randomized studies of bed rest as an intervention to reduce preterm delivery in twin studies, no benefit was reported (Harti-
TABLE 1.2 Randomized Controlled Trials of Antibiotics in Women in Preterm Labor with Intact Membranes
|
Author |
Year |
Weeks of Gestation |
Number |
|
McGregor et al. |
1986 |
<34 |
17 |
|
Morales et al. |
1988 |
21–34 |
150 |
|
Newton et al. |
1989 |
24–34 |
95 |
|
McGregor et al. |
1991 |
_34 |
103 |
|
Newton et al. |
1991 |
24–33 |
86 |
|
McCaul et al. |
1992 |
19–33 |
40 |
|
Romero et al. |
1993 |
24–34 |
277 |
|
Norman et al. |
1994 |
26–34 |
81 |
|
Watts et al. |
1994 |
<34 |
56 |
|
Gordon et al. |
1995 |
24–35 |
95 |
|
Cox et al. |
1996 |
24–34 |
78 |
|
Svare et al. |
1997 |
26–34 |
110 |
|
Oyarzun et al. |
1998 |
22–36 |
170 |
|
Kenyon et al. |
2001 |
24–33 |
6295 |
|
SOURCE: Goldenberg, 2002. © 2002 Lippincott Williams & Wilkins. Reprinted with permission. |
|||
kainen-Sorri et al., 1984; Saunders et al., 1985; Crowther et al., 1989; Maclennan et al., 1990).
Nutritional Interventions
Epidemiological studies have found a relationship between women who gain very little weight during pregnancy and the incidence of preterm birth, stated Goldenberg. This suggested that nutritional interventions may help prevent pre-
|
Outcomes |
||||
|
Antibiotics (type) |
Decrease in Delay in Delivery |
Decrease in Perinatal Preterm Delivery |
Mortality and Morbidity |
|
|
Erythromycin |
Yes |
No |
No |
|
|
Erythromycin Ampicillin |
Yes |
Yes |
Not Stated |
|
|
Ampicillin Erythromycin |
No |
No |
No |
|
|
Clindamycin |
Yes |
No |
No |
|
|
Ampicillin Sulbactam |
No |
No |
No |
|
|
Ampicillin |
No |
No |
No |
|
|
Ampicillin Erythromycin Amoxicillin |
No |
No |
No |
|
|
Ampicillin Amoxicillin Metronidazole |
Yes |
No |
Yes |
|
|
Mezlocillin Erythromycin |
No |
No |
No |
|
|
Ceftizoxime Ampicillin Sulbactam Augmentin |
No |
No |
No |
|
|
Ampicillin Metronidazole |
Yes |
Yes |
No |
|
|
Amoxicillin Erythromycin |
No |
No |
No |
|
|
Erythroymcin Amoxicillin, Clavulanic Acid |
No |
No |
No |
|
mature birth. Currently, researchers have found that the majority of the success has occurred in developing countries where evidence suggests that nutritional intervention has substantially improved pregnancy outcomes, including a reduction in preterm birth. This improved outcome was seen in Gambia, where women worked hard in the field and were nutritionally deprived during certain seasons of the year (Prentice et al., 1983). Similarly nutritional benefits were seen in a randomized trial with an HIV population (Fawzi et al., 1998). However, in developed countries, nutritional counseling and caloric supplementation has had
little or no impact on the rate of preterm births, whereas nutritional supplementation has had mixed results. This may be one area where additional research is needed.
PURPOSE AND TIMING OF THIS WORKSHOP
“Mortality is decreasing primarily because of our ability to intervene, but we’ve really not made much of an impact at all on morbidity,” said Donald R. Mattison of Columbia University. Despite research efforts that are complete or ongoing, we still do not understand the many divergent causes of preterm birth, and therefore we lack the interventions needed to prevent it. Many speakers, however, described research findings suggesting that we may be on the verge of understanding the intervening factors of preterm birth at the molecular, individual, and community levels.
Despite research efforts that are complete or ongoing, we still do not understand the many divergent causes of preterm birth, and therefore we lack the interventions needed to prevent it.
Donald R. Mattison
During this two-day workshop, several speakers suggested that a greater understanding of the factors that constitute normal parturition and labor as well as those that contribute to preterm birth is needed. Chapter 2 of this workshop summary focuses on what is known about the normal mechanisms of labor and delivery that might lead to identification of the causes of preterm birth. Chapter 3 provides an overview of the biological causes of preterm birth. Chapters 4 and 5 explore environmental factors, including the social environment, gene–environment interactions associated with preterm birth, and research protocols used by federal agencies that may detect toxicant effects on gestation length. Finally, Chapter 6 presents workshop participants’ proposals for future research directions that are needed to address this major public health concern.














