
Summary
In the 50 years since the first successful organ transplant, thousands of recipients of a transplanted kidney, heart, pancreas, liver, or other solid organ in the United States and throughout the world have had their lives extended and their health improved as a result of organ transplantation. Since 1988, more than 390,000 organs have been transplanted, with approximately 80 percent of the transplanted organs coming from deceased donors. In 2005, 7,593 deceased donors provided 23,249 transplanted organs in the United States, and there were 6,896 living donors.
The number of organ donors has increased each year since 1988, with a steady increase in the number of organs recovered (an average of approximately 1,100 more organs are recovered each year than in the previous year). However, the growth of the waiting list has been much more dramatic, increasing by approximately 5,000 transplant candidates1 each year. The net result is a widening gap between the supply of transplantable organs and the number of patients on the waiting list (Figure S-1). The U.S.
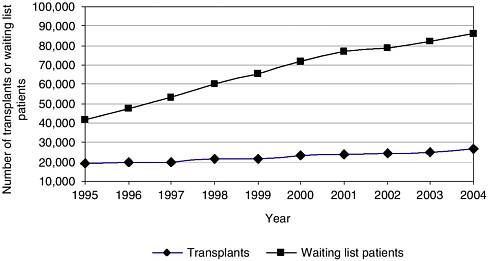
FIGURE S-1 Growth in the number of transplants and in the number of candidates on the transplant waiting list.
waiting list for organ transplants, which listed 16,026 individual candidates for transplantation in 1988, has grown more than fivefold to greater than 90,000 in January 2006. The need for kidney transplants is the major driving force in the increase in the waiting list, with individuals waiting for a kidney transplant constituting more than 70 percent of the individuals on the current transplant waiting list. In 2005, 44,619 transplant candidates were added to the waiting list.
Over the past 10 years, minority populations have donated organs at increased rates. In the past, donation by minority populations has been hindered by mistrust of the healthcare system, inequities in access to transplantation, and failure to request donation. Although donations by minority populations are steadily increasing, several of these matters remain unresolved and need further attention. The donation rates by minority populations are now in proportion to their population distribution in the U.S. census. However, there is an increased need for transplants, particularly kidney transplants, in minority populations because of the higher incidence of end-stage renal disease among the members of these populations. In addition, there is still room for improvement in the rates of consent to organ donation among all ethnic groups.
As the demand for organ donation far exceeds the current supply of available organs, various efforts are under way to determine how best to reduce the gap between supply and demand. In addition to refinements in hospital processes and protocols, several proposals are being discussed that
might further enhance the system or provide incentives for more individuals or families to consent to organ donation.
In 2004, the Health Resources and Services Administration (HRSA) and The Greenwall Foundation asked the Institute of Medicine (IOM) to study the issues involved in increasing the rates of organ donation. This report is the result of a 16-month study conducted by an IOM committee composed of experts in the fields of bioethics, law, health care, organ donation and transplantation, economics, sociology, emergency care, end-of-life care, and consumer decision making.
PERSPECTIVES AND PRINCIPLES
The committee carefully examined the ethical and societal implications of a range of proposals to increase the rates of organ donation by deceased donors in the United States and also considered several of the ethical issues regarding organ donation by living donors.
The committee’s deliberations were undertaken from the perspective of the shared interest that all members of society have in access to organs for transplantation should the need arise. The perspectives and principles guiding the committee’s report are as follows:
-
Common stake in a trustworthy system: Everyone in the national community has a common stake in the creation and maintenance of an effective and trustworthy system for providing timely access to transplantable organs and, if organs are scarce, in increasing the number of organs recovered and distributing them fairly.
-
Acceptable appeals for donations: Policies and practices designed to increase organ donation may properly appeal to a variety of motivations for donation, including altruism, community spirit, and reciprocity.
-
Respect for persons: Policies and practices designed to increase the rates of organ donation and the recovery of organs from deceased individuals must be compatible with four limiting conditions deeply rooted in the cultural, religious, and legal traditions of the United States: (1) respect for the moral worth and dignity of each human being; (2) respect for each individual’s right to govern the disposition of his or her body after death, including the voluntary choice of whether or not to donate organs; (3) respect for the remains of human beings, as represented in particular cultural and religious practices; and (4) respect for the wishes and feelings of families of deceased individuals.
-
Fairness: Policies and practices designed to increase the supply of transplantable organs need to be fair in their distribution of both benefits and burdens, with particular attention to their impacts on disadvantaged groups.
CLARIFYING TERMINOLOGY
Because the concepts and processes of organ donation are so closely intertwined with emotional issues of death and dying, it is of utmost importance to the committee, as it is to the transplantation community, that the terminology used to describe and discuss all aspects of organ transplantation be both as sensitive and as accurate as possible. Terminology in this field has had both positive and negative connotations, which have sometimes changed over time. Terms that have seemed descriptive or useful in the past are now being reconsidered in favor of terms that are more sensitive to the donor family and that affirm the value of individual human life. Table S-1 highlights some of the terms recommended by the committee.
A SYSTEMS APPROACH
The committee considered a number of approaches that have been suggested for increasing the rate of organ donation. The remainder of this summary examines each of these approaches and presents the committee’s recommendations.
Organ transplantation involves a complex, collaborative set of interactions among patients, family members, healthcare professionals, organ procurement and transplant coordinators, the hospital where the donation occurs, the organ procurement organization (OPO) that facilitates the acquisition and the distribution of organs, and the transplant center. The U.S. organ donation system has evolved over the past half century, having been shaped by a series of federal and state laws and regulations, private-sector oversight, and individual hospital policies. The system has focused primarily on deceased donors whose deaths have been determined by neurologic criteria.
This report is being written at a time when many initiatives in the organ donation system have been undertaken to increase rates of organ donation.
TABLE S-1 Recommended Terms
|
Instead of: |
Use the Recommended Term: |
|
Cadaver or cadaveric donor |
Deceased donor |
|
Harvest or procure |
Recover or surgically remove |
|
Life support |
Mechanical support or ventilated support |
|
Cardiac death |
Circulatory determination of death |
|
Brain death |
Neurologic determination of death |
|
Donation after cardiac death |
Donation after circulatory determination of death (DCDD) |
|
Donation after brain death |
Donation after neurologic determination of death (DNDD) |
A major new initiative is the series of Organ Donation Breakthrough Collaboratives. Directed by HRSA, the collaboratives attempt to increase rates of organ donation by encouraging hospitals and OPOs to use methods of continuous quality improvement to enhance the process of deceased organ donation.
The opportunity to decide whether to be an organ donor should be a part of end-of-life decision making. Patients and their families should be offered this opportunity as standard end-of-life care. For the organ donation process to be fully integrated into end-of-life care, a wide range of healthcare professionals need enhanced awareness of and training regarding the organ donation process.
Recommendations:
Sustain Continuous Quality Improvement Initiatives.
HRSA should be sufficiently funded to provide technical assistance to hospitals and OPOs for continuous quality improvement efforts, including the identification and dissemination of best practices. An infrastructure that can support the collaboration, the dissemination of findings, and evaluations of the Breakthrough Collaboratives should be funded. Furthermore,
-
Individual OPOs and hospitals should develop, implement, and evaluate continuous quality improvement processes.
-
Accrediting and monitoring organizations, such as the Association of Organ Procurement Organizations, Joint Commission on Accreditation of Healthcare Organizations (JCAHO), and National Committee for Quality Assurance (NCQA) should require and monitor measures of continuous quality improvement, including process measures as well as conversion rates.
-
HRSA, the Centers for Medicare & Medicaid Services, and private insurers (where appropriate) should ensure that organizational quality improvement efforts are recognized as part of normal healthcare operations and should be reimbursed accordingly.
Increase Research on Innovative System Changes.
HRSA, the National Institutes of Health, and the National Center on Minority Health and Health Disparities should be allocated funds sufficient to increase research efforts to identify further innovative and effective system changes for improving the organ donation process and increasing the rates of organ donation and to evaluate the impacts of such changes on the healthcare system. Research efforts should be evidence based, interdisciplinary, and culturally relevant.
Strengthen and Integrate Organ Donation and Quality End-of-Life Care Practices.
Hospitals, OPOs, and other healthcare entities should consider how best to integrate the organ donation process with quality end-of-life care practices. Interdisciplinary teams should align end-of-life protocols, practices, and guidelines with organ donation protocols.
Enhance Training for Healthcare Professionals.
HRSA, in collaboration with palliative care and other professional associations representing diverse disciplines and specialties (including, but not limited to, critical care professionals, transplantation professionals, social workers, and clergy), should strengthen training in end-of-life practices and organ donation, including processes of communication and decision making, with the goal of establishing a knowledgeable and positive environment that supports organ donation.
EXPANDING THE POPULATION OF POTENTIAL DONORS
Most transplantable organs come from deceased donors who have been declared dead by neurologic criteria. Because many more deaths in the United States are determined by circulatory criteria than by neurologic criteria, there is great potential to expand the number of potential organ donations. The committee acknowledges that donation after circulatory determination of death (DCDD) can be a more complex and less facile process than donation after neurologic determination of death. However, expanding the nation’s capabilities, particularly in large urban areas with excellent emergency medical care, could provide the opportunity for donation to larger numbers of individuals and families. One set of conservative estimates suggests that at least 22,000 of out-of-hospital cardiac arrest deaths annually in the United States could be potential donors if important ethical and practical matters could be resolved. Before proceeding further, demonstration projects to assess the feasibility of undertaking such a strategy within a defined community should be considered.
Recommendations:
Implement Initiatives to Increase Rates of Donation after Circulatory Determination of Death.
HRSA, the National Institutes of Health (NIH), OPTN, OPOs, donor hospitals, transplant centers, and professional societies
should implement initiatives to increase rates of DCDD. Particular emphasis should be given to
-
funding of interdisciplinary research by NIH and HRSA to understand and remove institutional, professional, and community barriers and resistance to DCDD;
-
enhancing public and professional education, disseminating best practices, and monitoring and evaluating DCDD efforts;
-
clarifying required referral regulations to ensure that all potential donors are considered; and
-
adding preparation for organ donation to the end of standard resuscitation protocols.
Encourage and Fund DCDD Demonstration Projects.
The U.S. Department of Health and Human Services, states, and local entities should encourage and fund demonstration projects to determine the feasibility of increasing the rates of uncontrolled DCDD in cities with established and extensive trauma centers and emergency response systems. Such demonstration projects should include extensive public and professional education, including an emphasis on donor registry efforts, and participation by all relevant stakeholders in the development of protocols and processes.
Maintain Opportunities for Organ Donation.
OPOs should work with relevant stakeholders to obtain community authorization for the use of postmortem organ preservation techniques during the time needed to seek family consent for donation when the deceased person’s donation intention is unknown.
Increase Research on Organ Quality and Enhanced Organ Viability.
NIH should request and allocate funds for the purpose of determining the characteristics that modify and define organ quality. NIH should fund further research on enhancing the viability of organs for transplantation, including improved methods of organ preservation and improved criteria (with appropriate point-of-care testing) for determining the viability of organs.
PROMOTING AND FACILITATING INDIVIDUAL AND FAMILY DECISIONS TO DONATE
Making an informed choice regarding organ donation, documenting that decision (by designating the decision on a driver’s license or a donor
card or through a donor registry), and sharing the decision with family members are the key steps in ensuring that individuals are able to exercise their rights to make a determination about the disposition of their organs after death. This decision is a significant expression of personal autonomy, as the individual considers an action that after his or her death has the potential to save lives and improve the quality of life for others.
Many myths surrounding organ donation and transplantations—such as the fear that having a donor card will compromise the extent of health care that the patient receives—often constitute barriers to increased rates of donation. Therefore, public education that is culturally sensitive and that uses effective community education strategies is needed. Public education about organ donation should emphasize that all members of society have a common interest in an adequate supply of organs because all are potential recipients as well as potential donors. Each individual should have multiple opportunities to learn about organ donation and to express his or her desire to donate. Furthermore, mechanisms are needed to ensure that recorded decisions to donate are accessible to the relevant healthcare professionals and OPO staff on a 24-hour-a-day, 7-day-a-week basis.
The committee believes that it would be premature to move toward a policy of mandated choice (which would require an individual to make a decision about donation). To be successful, a mandated-choice model needs an informed citizenry that understands organ donation and what it means for the individual and for the recipient and that sufficiently trusts the system to go on record as an organ donor. Without giving people adequate and accessible information, merely forcing them to choose to be an organ donor or not does not capture the potential of mandated choice and weakens the argument for it. A broad-based and multidimensional educational campaign is needed that confronts issues around death and dying, debunks the myths and misperceptions surrounding organ donation, and emphasizes the benefits of organ donation. Pilot tests of mandated choice could be reconsidered in the future when there is a broader and more accurate understanding of organ donation among all sectors of U.S. society. If public education is successfully intensified, however, mandated choice may prove to be unnecessary.
Recommendations:
Increase Public Understanding of and Support for Organ Donation.
HRSA, NIH, the Centers for Disease Control and Prevention, the United Network for Organ Sharing, OPOs, voluntary health organizations, faith-based organizations, community coalitions, and other interested parties should strengthen their efforts to provide
public education about organ donation through multiple media and educational venues. They should pay particular attention to developing and disseminating culturally sensitive educational materials that can be understood by individuals with different levels of education. Entertainment and media organizations should strive to accurately portray organ donation and transplantation.
Increase Opportunities for People to Record Their Decision to Donate.
HRSA, state and local governments, nonprofit organizations, community coalitions, and other interested parties should provide multiple opportunities for individuals to receive information on organ donation and to record their donation decisions. These opportunities should be provided at the times of driver’s education and licensing and advance care planning, as well as through work-, faith-, school-, and community-based initiatives.
Enhance Donor Registries.
State governments (including departments of motor vehicles), OPOs, and HRSA should work together to:
-
ensure full access to and sharing of donor registration data;
-
ensure that a nationwide networked system of registries that identifies self-declared organ donors is readily accessible to OPOs and healthcare professionals on a 24-hour-a-day basis, and is updated daily.
Mandated Choice Should Not Be Enacted.
At this time, states should not enact legislation requiring people to choose whether or not to be an organ donor (mandated choice).
PRESUMED CONSENT
In the United States, deceased organ donation occurs only with express consent (often in response to an inquiry or request). This consent may be given in advance by the individual while he or she is still alive, or it may be given by the next of kin after the death of the individual. The state laws that govern organ donation thus require opting in (or contracting in). The default option, in the absence of express consent, is nondonation. Proposals to increase the availability of transplantable organs often recommend a policy of presumed consent or opting out. Under such a policy, organs from deceased individuals could be removed for transplantation unless the decedents—or their families, after their deaths—had followed the prescribed
measures for opting out. The default option, in the absence of express objection, would become donation.
The committee believes that it would be premature to attempt to enact presumed-consent policies at this time. Although the committee is supportive of the principles of a presumed-consent approach (namely that under certain clear and well-defined circumstances, in the absence of an individual’s expressed decision, one may presume his or her consent rather than refusal to donate), the first step is to build sufficient social support before introducing presumed consent in the United States. This can be accomplished through intensified public education regarding organ donation, building greater trust in the healthcare system, and encouraging a general shift in societal understanding of the value and moral grounding of donation. The current emphasis on the use of first-person (donor) consent to organ donation can reinforce the importance of individual decision making. Coupling this change with the move towards use of an expected donation approach with families can also strengthen the societal norm of organ donation as a social responsibility and standard practice.
Although conditions essential for a change to a presumed-consent policy do not currently exist and do not appear to be likely in the foreseeable future, it is both appropriate and important to seek to realize them over time. When the necessary conditions exist for a shift to a presumed-consent policy it will be critical to provide clear, easy, nonburdensome, and reliable ways to opt out.
Recommendation:
Presumed Consent.
At this time, states should not replace the existing legal framework, which requires explicit consent for organ donation, with a framework under which people are presumed to have consented to donate their organs after death unless they have declared otherwise. However, it would be appropriate for all interested parties to seek to create over time the social and cultural conditions that would be essential for the adoption of an effective and ethical system of presumed consent.
INCENTIVES FOR DECEASED DONATION
The committee was asked to examine the use of financial and nonfinancial incentives to increase the supply of organs from deceased donors. A financial incentive is the provision of something of material value to motivate consent for organ removal. For example, a direct payment could be
made in exchange for the organ, with the price for the organ determined by the free market or set by regulatory authorities. In either case, the exchange of money for organs would constitute a purchase and sale. Alternatively, financial incentives might be used to induce donations, just as the prospect of a tax deduction is used to induce charitable contributions. Such incentives might be a cash payment usable for any purpose; a cash payment earmarked for a specific purpose, such as funeral expenses or a charitable contribution; or a material good or service, such as bereavement counseling or health insurance. The financial incentive could go to the donor before death or to the donor’s estate after death in exchange for the donor’s agreement to allow his or her organs to be recovered after death. In situations in which the donor’s family makes the decision to donate, the incentive could go to the family. Nonfinancial incentives to donate could take the form of community recognition or preferential access to donated organs.
Every society draws lines separating things that are treated as commodities from things that should not be treated as “for sale.” The committee believes that there are powerful reasons to preserve the idea that organs are donated rather than sold, even in a regulated market.
The committee examined financial incentives within the gift model of donation to determine if they would provide additional increases in the rates of organ donation. Hard data on the impact of incentives are lacking, and it may be difficult to obtain reliable data to address these issues. A pilot study of financial incentives for organ donation may set in motion a societal process that is difficult to reverse even after the pilot study itself is abandoned. For example, if people begin to view their organs as valuable commodities that should be purchased, then altruistic donation may be difficult to reinvigorate.
Additionally, in principle, the provision of anything of material value raises some of the same justice concerns as do payments within a regulated market: although some might consider an incentive to be fair to donors or donor families, there is also the fear that incentives would disproportionately affect those who are poor or marginalized from the system.
Furthermore, there are concerns that the relationship between financial payments and a willingness to donate may not conform to the pattern that applies to ordinary consumer goods; payments may “crowd out” other motivations, and some families who would donate under an altruistic system may refuse to donate.
Much remains to be done to remove disparities in the provision of health care and to build the trust in the medical community. Although incentives might serve to increase donation rates, the committee believes that the actual need for incentives can be determined only after other alternatives have been explored. Promising options are the use of quality im-
provement methods to improve the process of organ donation under a gift model and making medical practice changes that increase the number of deceased individuals who are potential organ donors.
In examining nonfinancial incentives, the committee was concerned that a reciprocity model for receiving a transplant would—at least in the short term—accentuate existing social inequalities and disadvantage those who are uninformed about organ donation. Moreover, reciprocity introduces a criterion for organ allocation that is not related to medical need. Similarly, preferred-status programs risk penalizing uninformed individuals and introduce a nonmedical (non-need-based) criterion into the allocation equation.
Recommendations:
Financial Incentives.
The use of financial incentives to increase the supply of transplantable organs from deceased individuals should not be promoted at this time. (The term “financial incentives” refers to direct cash payments as well as contributions toward funeral expenses or to a charity of choice.)
Preferential Access.
Individuals who have recorded a willingness to donate their organs after their death should not be given preferential status as potential recipients of organs. This recommendation does not imply opposition to the assignment to living donors of additional points for the allocation of organs should they subsequently need a transplant.
ETHICAL CONSIDERATIONS IN LIVING DONATION
Organ donation by living donors clearly saves lives, improves transplantation outcomes under some circumstances, and reduces recipients’ waiting times. It also increases opportunities for patients without living donors to receive organs from deceased donors. However, it raises a series of ethical questions that have not been fully addressed. The transplantation of organs from living donors seems to violate the traditional first rule of medicine—primum non nocere (above all do no harm)—because it involves the removal of a healthy organ from one person for implantation into another person who is already a patient.
Although the committee believes that the whole practice of organ donation by living donors now needs a careful review and assessment on its own, in the interim the committee makes a few specific recommendations, build-
ing on ethical concerns and proposals already present within the transplantation community and drawing on the ethical perspectives that inform this report. These recommendations focus on the need for better information for improved risk-benefit analyses by transplantation teams, donor advocates, and potential donors themselves and on the increased use of independent donor advocate teams committed to the rights and welfare of the donor as patient, before, during, and after the donation.
Recommendations:
Protect Living Donors.
Hospitals that perform living donor transplantations should provide each potential living donor with an independent donor advocacy team to ensure his or her voluntary and informed decision making.
Facilitate Living Donor Follow-Up.
HRSA, OPTN, and transplant centers should work to establish registries of living donors that would facilitate studies of both short-term and long-term medical and other outcomes of living donation.
OPPORTUNITIES FOR ACTION
The recommendations provided in this report set forth a number of actions that the committee believes can have a positive impact on organ donation (Table S-2). Together, these recommendations identify a set of actions that in isolation might have only limited results but that in concert should strengthen ongoing efforts and open up new opportunities to increase the supply of transplantable organs, thereby saving the lives and improving the quality of life of many individuals.
It is the committee’s hope that this report will contribute to the development and implementation of new efforts to increase the rates of organ donation. In addition, the committee hopes that these efforts, along with concurrent actions focused on the prevention of health conditions that lead to the need for transplantation and research to explore alternatives to transplantation, will significantly reduce the size of the organ transplant waiting list in the near future.
TABLE S-2 Actions to Increase Organ Donation
|
Individuals |
|
|
Families |
|
|
Healthcare, emergency care, and transplantation systems |
|
|
|
|
|
|
|
|
|
|
Nonprofit organizations, academia, government, media, employers |
|
|
|
|
|
|
|
|














