
2
Physicians in Public Health: Their Roles, Knowledge Needed, and Numbers
This chapter examines the roles of physicians in public health, describes the knowledge that they need to practice public health, and estimates the number of physicians needed to maintain an adequate public health physician workforce.
ROLES AND LEVELS OF ENGAGEMENT
Since the inception of organized public health programs, physicians have been seen as essential to the delivery of good public health services. In any list of the multiple professions needed for the high-quality practice of public health, physicians are included with nurses, dentists, veterinarians, environmental health specialists, laboratorians, epidemiologists, health educators, and others. In the early years of the 20th century, statutes that established public health departments at the state and local levels required that the public health official (the public health officer or health commissioner) be a duly licensed physician. The size and complexity of the public health workforce have grown over the intervening century, many statutes have been rewritten without specifying the professional discipline of the agency leadership that is required, and the unique role of physicians in public health has become more difficult to describe.
Many more physicians than are currently recognized engage in public health activities at some point in their careers. First, all physicians intersect with public health in many activities of their practice and can be viewed as participating in public health activities. Second, the practices of
some physicians include some public health elements. These physicians include infectious disease physicians investigating health care-associated disease outbreaks, pediatricians working in school health, and emergency medicine specialists serving as the medical directors of emergency medical services. Beyond their day-to-day duties, the stories that they can tell of prevention efforts that have not been practiced may be a critical factor in public policy making. It was the voice of a practicing pediatrician, for example, that launched the national effort to place every child in an appropriate restraint when the child was traveling in a moving vehicle.
Finally, some physicians have careers in public health; that is, they can be identified as specializing in public health, whether they practice this specialty for their entire career or enter it as a change in specialty at some point in their career. These public health physicians work in a variety of settings, including nongovernmental organizations, managed care organizations, occupational medicine, aerospace medicine, academia, public hospitals, and governmental agencies. Figure 2.1 illustrates these different levels of physician engagement with public health. Movement upward in the figure, as indicated by the arrow, indicates the need for higher levels of public health knowledge and practice.
A public health physician policy maker involved in the development of population health policies might work with legislators to ensure that
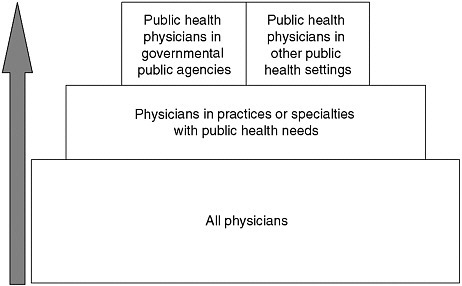
FIGURE 2.1 Physician involvement in public health.
they understand the health implications of proposed legislation, present the health implications of public health programs to the public, or ensure that public health programs are structured to use the best emerging public health science. A public health physician leader or manager may be found to be the head of a managed care organization, a director of a state health department, or the manager of epidemiological surveillance in a hospital. At each of these levels the public health physician leader and manager is responsible for developing clear goals, using resources efficiently and effectively, and ensuring that the workforce for which he or she is responsible is well trained and well organized to fulfill its responsibilities.
Public health physicians also play a key role in a number of practice areas that require both public health perspectives and extensive clinical expertise. Mental health, occupational health, and corrections health are a few of these. At least at the level of leadership, these require the participation of well-trained public health physicians.
As described above, all physicians are a part of the public health system; for a smaller number of physicians, a portion of their practice involves public health, while career public health physicians practice in a wide range of settings, including governmental public health agencies.
WHAT DO PHYSICIANS NEED TO KNOW?
Concurrently with the Institute of Medicine (IOM) study examining the public health system discussed earlier (IOM, 2003a), IOM undertook a study to develop a framework for strengthening education, training, and research to improve population health. That report (IOM, 2003b) discussed the need for an ecological approach to addressing health problems1 and identified several key content areas for public health professionals during their training. Public health professionals come from a wide variety of disciplines including nursing, dentistry, social work, pharmacy, law, epidemiology, laboratory sciences, and, of course, medicine. Physicians are a key component of the public health professional workforce and, as such, must be as well prepared as other public health professionals to meet the challenges of public health practice in the 21st century. Therefore, the current committee endorses the recommendations of the earlier report, agreeing that physicians must be prepared to base their actions on an ecological approach to problem solving, as well as be educated in the
key content areas identified for training public health professionals. Table 2.1 lists the content areas recommended for public health professionals (IOM, 2003b). These content areas have been expanded by this committee to identify how each area applies to physicians. These essential areas are epidemiology, biostatistics, environmental health, health services administration, social and behavioral sciences, informatics, genomics, communication, cultural competence, community-based participatory research, global health, policy and law, and ethics. Again, endorsing the recommendations of the 2003 report (IOM, 2003b), the introduction of this content to all physicians should occur in medical school. The mechanisms for preparation beyond that basic introduction are discussed in Chapter 3.
In reflecting more deeply on the demands facing the United States today (e.g., public health preparedness in the face of natural and human-made disasters), the committee believes that certain responsibilities may fall more directly on physicians and require knowledge and skill in three additional areas not included in the prior report that are crucial to preparing effective public health physicians. These areas are leadership, public health emergency preparedness, and clinical and community preventive service provision. Each of these areas is described in detail in the following sections.
Leadership
Physicians involved in the health of the public require leadership skills that allow analysis and planning for complex threats to the health of small groups, neighborhoods, and entire populations. Medical schools, however, generally prepare their students only for clinical medicine and medical research, with the learning of management skills and leadership taking place through on-the-job experience or during the postgraduate period. Physicians provide leadership, for example, in the rapid responses to industrial explosions or spreading infections, as well as in immunization, health promotion, disease prevention, nutrition, tobacco control, and violence prevention programs. Indeed, policy makers, the public, and other health care professionals look to physicians to be well-informed resources, guides, spokespeople, and leaders.
Leadership development has several elements, including, as John Gardner (1990) commented, “Envisioning goals, affirming values, motivating others, managing, achieving workable unity, explaining things in appropriate settings, serving as a symbol, representing the group, and in the important task of self-renewal.” In the complicated world of public health, these tasks must be carried out by leaders who also demonstrate global awareness, cultural competence, respect for others, humor, per-
TABLE 2.1 Public Health Content Areas for Physician Training
|
Area |
Description |
Application for Public Health Physicians |
|
Biostatistics |
Collection, storage, retrieval, analysis, and interpretation of health data; design and analysis of health-related surveys and experiments; and concepts and practice of statistical data analysis |
Development of commentary to clarify statistical information for clinicians; accurate interpretation of statistical information in publications and reports; understanding the strengths and weakness of studies when their findings are applied to diverse communities; and ability to explain these to professionals, policy makers, and the general public |
|
Epidemiology |
Distributions and determinants of disease, disabilities, and death in human populations and the characteristics and dynamics of health and illness in human populations |
Development of clinically sound case definitions for investigations and surveillance; teaching and encouraging clinicians to ensure their participation in reporting and investigations; and assessing, describing, and developing interventions for health issues in communities |
|
Environmental health sciences |
Environmental factors, including the biological, physical, and chemical factors that affect the health of a community |
Accurate interpretation of environmental influences on health in responding to illnesses or outbreaks; consultation with environmental health professionals; assisting with development of programs and policies that prevent or mitigate environmental health hazards; and articulating the human health aspect of environmental issues |
|
Health services administration |
Planning, organization, administration, management, evaluation, and policy analysis of health programs |
Providing assurance that health policy and management do not misuse medical information or neglect important clinical insights; developing and managing governmental or community programs; and working with governmental, hospital, and other health care systems |
|
Area |
Description |
Application for Public Health Physicians |
|
Social and behavioral sciences |
Concepts and methods of social and behavioral sciences relevant to the identification and the solution of public health problems |
Integration of health promotion and health information in program planning and delivery and development of multifaceted approaches to community health issues |
|
Informatics |
Systematic application of information, computer science, and technology to public health practice, research, and learninga |
Policy contribution to the development of informatics to ensure utility for the intersection of medicine and public health |
|
Genomics |
Application of basic public health sciences to genomic issues and studies |
Interpretation of genomic information relevant to problems of public health importance and accurate provision of this information to other physicians |
|
Communication |
Skills required to interact with different groups within the public health system, including policy makers, health care providers, media, and lay citizens |
Use of best practices in communication to act as a bridge between public health professionals in general and physicians from all settings and in communicating information about public health to the public, working with media, presenting information to diverse communities and to policy makers; and addressing professionals |
|
Cultural competence |
Communicating and adapting public health messages and methods in ways that respect the values, opinions, beliefs, and practices of people in various communities |
Demonstration of the highest possible level of competence in dealing with the multiple cultural groups in the community, effectively identifying and responding to the needs and concerns of diverse populations, and working to address health disparities |
|
Community-based participatory research |
Research methods that emphasize communities as research coequals, collective visioning, incorporation of social ecology approaches, and using multiple data collection methods |
Provide assurance that when public health engages in research, it does so as a partner with the community; sharing this perspective with medical researchers using more traditional approaches to studies |
spective, and up-to-date knowledge of the basic and clinical sciences, biostatistics, epidemiology, and other fields.
In a white paper developed for the CDC Leadership Summit of the Centers for Disease Control and Prevention in 2006, Rowitz (2006) called this approach to leadership “ecological leadership.” Ecological leaders are committed to the development of their leadership skills and competencies throughout their professional careers, while at the same time they are committed to the appropriate application of these skills to their community’s changing health priorities. In addition, ecological leaders are able to balance the needs of the day-to-day practice of public health in
their organizations and communities with the special skills and applications necessary to address public health emergencies.
Within organizations, physicians need to work across programs and departments. As physicians move into public health leadership positions, they must work not only within organizational settings, but also collaboratively across organizations to address population-based programs. This requires learning to operate in terms of systems and strategies rather than the detail orientation typical of clinical work which tends to have a more linear focus (i.e., symptoms, then diagnosis, treatment, and recovery). In recent years this type of leadership, in which multi-sectoral collaboration occurs, has been called meta-leadership.
Rowitz (2001) discussed the complexities involved in leadership and pointed out that individuals learn to be leaders at the personal, team, organization, community, and professional levels. To be effective, leaders need to take a systems perspective and view the view health and illness in a comprehensive way. The physician who understands the biology of health and illness brings a special expertise to the public health field. He or she understands that what happens at a clinical level can provide much useful information about disease prevention at the community level and the importance of these issues in promoting the core public health functions of assessment, policy development, and health assurance (IOM, 1988).
Public Health Emergency Preparedness
As the nation has become more aware of the need for effective emergency preparedness and the response to emergencies in general, professionals in the medical and public health communities have also identified the need for them to pay increased attention to these special areas of practice. Although all physicians have some emergency-related responsibilities (early detection and reporting of potential problems, implementation of public health directives in patient care, and the accurate communication of risk to patients), public health physicians play a particularly important role in population-based activities in response to emergencies and disasters.
The overall management of emergency preparedness and the response to an emergency does not require medical knowledge; but almost any emergency has the potential to threaten the public’s health, such as the risk of foodborne disease when power supplies are cut for extended periods, waterborne disease if water supplies are contaminated by flood waters, or hyper- and hypothermia at temperature extremes. Medical expertise may be essential to interpreting the degree of risk and ensuring that appropriate communications to the public and protective actions are
taken. Beyond these more common challenges, epidemic diseases, chemical exposures, and other human-caused or naturally occurring threats to health require attentive physicians in the community and medical expertise on the public health response team to ensure that threat detection is handled well and the best possible interventions are put to use. Furthermore, in public communication during an emergent event with health implications, the voice of a well-prepared public health physician can be the key to the community understanding of the risks and the steps to be taken for harm reduction and a return to normal function.
Public health professionals are involved in emergency responses in a number of ways. For example, the responsibility for the regulation of state and local emergency medical services has been located in public health agencies and has always included medical oversight. Most governmental emergency preparedness and disaster plans give the responsibility for planning for and response to the health component of the plan to state and local public health entities. In addition, public health officials have specific legal authorities and police powers that they can use under emergency conditions, particularly conditions in which the potential for the transmission of a disease from person to person is encountered. The use of disease-specific information on which to base the use of such powers requires sound medical interpretation.
Over the past decade, agencies and associations in public health have developed clear statements of the competencies in emergency preparedness and response required by any clinician in a position to identify a problem early (which would include all physicians)2 and all public health workers (including public health physicians).3 These competencies go beyond the clinical information about the treatment of individual patients in cases of natural disasters; disease epidemics; or biological, chemical, or radiological emergencies. The competencies applicable to a physician practicing in public health include the management and operational skills essential for the individual to make a successful contribution within the context of the National Incident Management System.
Clinical and Community Preventive Services
One component of the effective practice of public health is ensuring the delivery of the appropriate public health clinical services by practicing
clinicians. Practicing clinicians should be able to look to the public health community for relevant guidelines, professional and technical expertise, and reliable knowledge and opinions, often on a case-by-case basis.
Public health physicians are routinely required to provide advice to the practicing physician in a number of clinical domains. Among the most common are immunizations and vaccines, the diagnosis and treatment of diseases of public health importance, clinical preventive guidelines, community preventive services relevant to the clinical domain, and guidelines and precautions for international travel.
Immunizations and Vaccines
The public health system generally sets recommendations for vaccine use, and public health physicians are often viewed as the “vaccine experts” in communities. In this area, public health physicians require expertise in general vaccinology and vaccine use information, routine childhood and adult immunization schedules, knowledge and assessment of the possible adverse reactions from vaccines, and use of vaccines in special settings, such as a hepatitis A virus outbreak.
Diagnosis and Treatment of Diseases of Public Health Importance
The public health system generally sets the recommendations for the appropriate diagnosis and treatment of diseases of public health importance. Traditionally, these have included endemic infectious diseases of public health importance, such as tuberculosis and sexually transmitted diseases, as well as emerging infectious diseases at the time of first recognition (e.g., severe acute respiratory syndrome and Legionnaires’ disease). In epidemic settings, for example, a cluster of cases of meningococcal meningitis or an outbreak of Escherichia coli O157:H7 infection, public health physicians will be called on to establish appropriate diagnostic and treatment guidelines. An additional area of public health physician expertise relates to the diagnosis and treatment of conditions not commonly seen by practicing clinicians, for example, suspect botulism, lead poisoning, malaria, or rabies.
Clinical Preventive Guidelines
Screening for a wide range of preventable conditions or conditions that are treatable if they are caught early (mammography and breast cancer, for example) is a key element of public health that is conducted by the practicing clinician. The creation and promulgation of screening guidelines are often viewed as the domains of public health, and public
health physicians play a key role in these efforts. In addition to the establishment of clinical screening guidelines, clinicians are often asked to provide patient counseling for selected public health concerns (e.g., tobacco use reduction, firearm safety, and sexual practices), and the development and encouragement of the use of effective counseling messages by practitioners are key elements of public health physician practice.
Community Preventive Services Relevant to the Clinical Domain
Community preventive services are services delivered to populations rather than individual patients. Public health physicians should be knowledgeable and capable of providing advice to clinicians and health systems regarding relevant community preventive services, for example, strategies that can be used to improve immunization rates or the rates of diabetes detection in a patient population.
Guidelines and Precautions for International Travel
Public health physicians are responsible for developing appropriate guidelines and precautions for international travel (malaria prophylaxis recommendations, for example). Although practicing clinicians specializing in travel medicine are becoming increasingly common, individual clinicians still seek public health physicians when they apply these guidelines to individual patients and groups of travelers. Knowledge of travel precautions is thus a core expertise required of public health physicians.
Because there are indications that the current public health workforce is inadequately trained in many respects (see Chapter 1), it is important not only to look at training future public health physicians but also to ensure that those currently engaged in public health careers are adequately trained.
NUMBER OF PUBLIC HEALTH PHYSICIANS
Given the lack of any single database that identifies public health physicians and the lack of any common definition of the term “public health physician” used across more limited data sets, it is difficult to determine accurately the number of physicians engaged in public health careers today. As discussed earlier, all physicians contribute to the practice of public health some of the time, and that number is known. Physicians whose practices require public health knowledge and skills in order to make successful contributions to health promotion or disease prevention can be identified within most medical specialties, although they are not
the major focus of this report. Under current circumstances, however, it is impossible to estimate the number of physicians in other than governmental health settings who are true public health physician specialists (or who work in positions that should require that level of public health specialization). The most reliable data are available only for physicians in governmental agencies.
Both because of the importance and centrality of governmental public health in assuring the health of the public, and because available data focus on physicians in governmental agencies, estimates of the current number of public health physicians focuses on those in governmental agencies. However, it is also difficult to estimate the numbers of physicians currently engaged in governmental public health careers, because information about physicians specializing in public health is incomplete. A number of different groups have, however, attempted to determine that number. For example,
-
A National Association of City and County Health Officials 2005 survey identified up to 2,500 physicians in local public health agencies (NACCHO, 2006). This information was gathered by use of an electronic survey. It did not ask for any details about the specialty certification of the physicians and asked only for information about full-time equivalents. The survey thus underestimates the actual number of physicians involved in public health, and there is no way to extrapolate such a number from the data from that survey. The resulting information is only about the single, official local public health agency and thus excludes information about the numbers of public health physicians in local mental health or substance abuse agencies.
-
The Enumeration 2000 report, commissioned by the Health Resources and Services Administration, estimated that approximately 6,000 physicians worked in federal and state health agencies in 2000, with 4,000 of these at the federal level (HRSA, 2000). The report was based on an analysis of existing data sets from state and some local health departments and was supplemented by information from the federal Office of Personnel Management and the U.S. Department of Defense. At the state level, only one state was able to report on workers throughout the state government. Categorization was by job title, when such information was available. Physicians were likely undercounted in that report for several reasons:
-
Many physicians in state and local public health are employed in job categories such as commissioner or director of health, epidemiologist, program manager, or some other generic term and could not be separated.
-
For some jurisdictions, a general category such as “professional”
-
-
-
was all that was available, with no specification of the individual’s training.
-
For some jurisdictions, even that level of clarity was lacking, and only a single number covering all workers was available.
-
-
Data from the American Medical Association (AMA) identified 1,400 physicians working in public health and preventive medicine (AMA, 2005). These data are drawn from a variety of sources and are not associated with board certification; therefore, there was no way to verify that the category of practice is consistent with the categories used in other systems. The extremely small number of public health and preventive medicine physicians identified from the AMA data compared with the numbers from the two previous reports suggests that these data reflect only those physicians seen as full-time employees in a public health setting and leaves out all or most of those who do not specialize in public health but practice in public health part of the time.
-
Bureau of Labor Statistics (BLS) data show that 22,000 physicians work for governmental agencies, including in all specialties and for all types of agencies (BLS, 2006). These are data from employer systems used for the identification of the types or categories of worker. The BLS data include all physicians working on governmental payrolls, including those in public hospitals and community clinics, employee health clinics, and clinical research settings, as well as public health agencies. For this reason, it cannot be considered an accurate source of information about the numbers of physicians working in official public health agencies or other governmental agencies with public health functions, such as environmental, mental health, and agricultural functions.
-
The American College of Preventive Medicine estimates that 1,654 preventive medicine physicians work in official health agencies (Parkinson, 2006). This represents the proportion of physicians who are known to the specialty board most relevant to public health and who can be identified as working in an official health agency. It can be considered an undercount of physicians working in public health for two reasons:
-
It does not include those physicians working in other governmental agencies with public health responsibilities, a problem common to several of these reports.
-
It does not include physicians with board certification in other specialties working in public health agencies, a group that includes many with specialty certification in pediatrics, infectious diseases, emergency medicine, and more.
-
The tremendous differences in the data sources, time frames, and definitions used in these various reports prohibit any meaningful integration or interpretation of the numbers of public health physicians; challenges
to any one of the methods used can easily be developed and thus prohibit the arbitrary use of any one of them. In determining the size of the current public health physician workforce, the committee relied most heavily on Enumeration 2000 and BLS data since they are most complete. These two most useful resources provide widely divergent numbers: Enumeration 2000, approximately 6,000; BLS, 22,000. Because the BLS data include physicians in other than public health positions and physicians with other than public health specialization, the committee determined this was an overestimate. However, the Enumeration most likely undercounted because categorization was by job title, and physicians are employed under titles such as commissioner, director, supervisor, epidemiologist, and surveyor as well as physician and public health physician. Taking into account the number and size of agencies at all levels of government, staffing patterns both reported and known to members of the committee, and indications from agencies about levels of vacancies, the committee’s considered opinion is that an estimate of 10,000 is reasonable, and could be used until such time as an improved data system is in place.
HOW MANY PUBLIC HEALTH PHYSICIANS ARE NEEDED?
If the estimated number of physicians currently employed in public health was reasonably accurate and reflected fully met need and if these physicians followed a typical work career, it would be relatively simple to estimate the number of replacement physicians who need to be trained for public health careers over the coming decades. Representatives of the U.S. Department of Defense described to the committee the annual planning that the department performs to determine the number of physicians to be recruited and trained in each specialty area and how it establishes a pipeline of physicians in specialty training programs (Mott, 2006). Although knowledge of such efforts is useful, the civilian public health world is not such a closed system with known population demands and specified resources.
Two other major caveats to estimating the national need for public health physicians exist: the current number of public health physicians does not reflect the need being met at present, and it is not clear that the career path for physicians in public health is a typical one.
Reports from public health agencies regarding the recruitment and retention of staff indicate that there are serious gaps in the current supply of public health physicians. Furthermore, according to Glass (2000), the numbers of physicians in public health and preventive medicine is decreasing.
Table 2.2 presents the committee’s estimates of both the current number of public health physicians and the number needed to achieve an
TABLE. 2.2 Estimated Present and Future Numbers of Physicians in Governmental Public Health Agencies
|
Agency |
Present |
Future |
|
Federal (public health and other) |
4,000 |
4,500–5000 |
|
State (public health and other) |
2,000 |
2,500–3,500 |
|
Local |
|
10,000–15,000 |
|
Nonspecified |
4,000 |
|
|
Total |
10,000 |
17,000–23,500 |
adequate supply. The committee bases its estimates on the assumption that public health would be served best by physician participation in the public health leadership team, both at the agency level and in major programmatic areas. The committee believes that these figures present conservative estimates, given the continuing increase in public health-related knowledge and the demands for a high level of public health practice that cannot be accomplished without an adequate public health physician presence throughout the governmental public health system. The estimates take no account of the potential need for increases in the numbers of public health physicians in other areas of medical practice.
The committee’s best estimate of the current number of physicians in state and local public health agencies is in excess of 2,000, or approximately 40 per state. Separation of the numbers of public health physicians at the state and the local levels is not possible at present. Furthermore, the current number of public health physicians working in state and local governmental positions is likely greater than 2,000 because of the large number (4,000) of public health physicians reported to work in positions not specified by level of government. Some of these physicians likely work in official public health agencies.
It is likely, however, based on the minimal data available regarding understaffing presented earlier in this report and on the committee’s expert opinion, that state public health agencies, except for those serving very small populations, need more physician participation, perhaps as many as 10 more in key leadership positions in the state agency (38 states × 10 physicians = 380).4 An additional 10 physicians might be needed in specialized programs in health departments (for example, in clinical services programs) in these same states (38 states × 10 physicians = 380).
|
4 |
The committee chose to designate states with populations of less than 1.5 million as states that serve “very small populations.” Of the 50 states in the United States, 12 have populations of less than 1.5 million (Infoplease. 2007. Population by state. http://www.infoplease.com/ipa/AOOO4986.html [accessed March 1, 2007]). |
Finally, a further 10 or more would be needed in other agencies in these states that perform public health functions, such as mental health and environmental health agencies (38 states × 10 physicians = 380). This would bring the estimated total number of physicians needed for state public health agencies to 3,140 (2,000 current physicians + 1,140 additional physicians). Given that these figures are not exact, the committee has chosen to adopt a range for estimated need of 2,500 to 3,500.
For local health agencies, it may be that very small health agencies might successfully be served by fewer physicians. For example, the 1,800 local health departments (LHDs) serving less than 100,000 people might have only one to two physicians (1,800 LHDs × two physicians = 3,600). However, the 500 local health departments serving larger populations might well have a need for the same 5 to 10 physicians in leadership positions needed by states (500 LHDs × 10 physicians = 5,000), as well as an additional 10 in programmatic areas (500 LHDs × 10 physicians = 5,000). The estimated total number of physicians needed for local public health agencies, then, would be 13,600. Again, because of the lack of specific data, the committee has chosen to express the estimated number of physicians needed in LHDs as a range from 10,000 to 15,000.
Such numbers would bring the estimated potential total number of public health physicians need for state and local public health agencies to between 12,500 and 18,500.
By using the same leadership and programmatic criteria outlined above, the federal public health agencies (primarily the U.S. Department of Health and Human Services and the U.S. Department of Defense, with smaller numbers in the Environmental Protection Agency and the U.S. Departments of Agriculture, Labor, and Veterans Affairs) could need 4,500 public health physicians (an increase of 500 over the current estimate). Looking at all of these estimates, the estimated number of physicians needed in governmental public health agencies ranges from 17,000 to 23,500. Given the difficulties in accurately estimating the number of public health physicians in practice today, as well as the difficulty of extrapolating that number to the number required to meet future needs, the committee has chosen to use expert opinion, as described above, to arrive at the conclusion that the country needs 20,000 physicians in public health careers, an increase of 10,000 over the current number engaged in public health careers. The number 20,000 provides a more comfortable margin that allows the inclusion of the public health physicians needed by community partner agencies, such as voluntary health associations, infection control physicians employed by hospitals or health care systems, and physicians employed by academic institutions, such as schools of medicine or public health. The committee is quite aware that greater accuracy
in estimating these numbers could be achieved if regular, comprehensive enumeration efforts were undertaken.
It is also essential to plan for the replacement of physicians leaving the public health workforce because of retirement or for other reasons. If it is assumed that an average career path in public health is 15 years (which is based on the assumption that some physicians enter the field late in their careers),5 the country needs approximately 1,350 properly prepared public health physicians every year to replace those leaving the existing workforce. This figure is arrived at by dividing the estimated number of physicians needed (20,000) by the estimated average length of a career in public health (15 years). The resulting number of 1,333 has been rounded to 1,350. Therefore, once the desired number of 20,000 public health physicians in governmental agencies is reached, the system must have the capacity to train at least 1, 350 new physicians each year to replace those leaving public health careers.
CONCLUSION AND RECOMMENDATIONS
Although this report is focused on education for physician careers in public health, it is important to note that many more physicians than those with public health careers engage in public health activities at some point. The committee has identified three broad groups of physicians who are considered to practice public health: all physicians, those who practice public health for a limited amount of time or in a limited role, and physicians who choose a career in public health. As can be seen from the preceding discussion in this chapter, estimating the number of physicians currently in public health careers, as well as the number needed for an adequate workforce, is hampered by a lack of data.
Although various attempts have been made to collect data on the number of public health physicians practicing in the United States, each is flawed in different ways, which makes it extremely difficult to estimate accurately both the current pool of public health physicians and the desired number. This, in turn, impedes efforts aimed at planning for the numbers and kinds of training programs needed to prepare physicians for effective public health practice. Therefore, the committee recommends that
-
the U.S. Congress designate funds for the Health Resources and Services Administration to conduct a periodic (every 3 to 5
-
years) comprehensive enumeration of the public health workforce, and filled and unfilled positions, with particular attention to physicians. The enumeration should include all civilian and military governmental agencies with public health responsibilities, public health academia, and significant voluntary agencies contributing to the public’s health. The enumeration should also include those physicians employed by private or public sector care delivery systems with public health responsibilities.
-
the information regarding public health physicians obtained in the periodic assessment of the public health workforce be used to project needs for public health physicians and public health physician education programs, and to determine the level of funding necessary to prepare physicians to fulfill those needs.
Using the data that are available, in addition to expert opinion, the committee has determined that the current public health physician workforce for governmental public health agencies is probably about 10,000. However, it estimates that an additional 10,000 public health physicians are needed to ensure an adequate public health physician workforce.
An effective public health system requires a well-trained workforce of sufficient numbers of individuals from diverse disciplines to address current and emerging public health needs. However, to ensure that the workforce is both sufficient in numbers and ready to act requires a basic understanding of exactly who comprises the workforce and how well they are trained. The contributions of public health to the well-being of the U.S. population are too important to allow the current uncertainty about the public health workforce to continue. Conducting the recommended periodic assessments of the public health workforce will allow much greater accuracy in developing the necessary programs and expertise for addressing important population health problems.
The next chapter explores pathways to physician public health careers and programs designed to educate physicians about public health.
REFERENCES
AMA (American Medical Association). 2005. Active physicians in U.S. & territories. Data from the American Medical Association physician masterfile. Chicago, IL: American Medical Association.
BLS (Bureau of Labor Statistics). 2006. Physician workforce estimates. Washington, DC: Bureau of Labor Statistics.
Gardner, J. W. 1990. On leadership. New York: Free Press.
Glass, J. K. 2000. Physicians in the public health workforce. In Update on the physician workforce. Rockville, MD: U.S. Department of Health and Human Services, Health Resources and Services Administration. Pp. 41-55.
HRSA (Health Resources and Services Administration). 2000. The public health work force. Enumeration 2000. Rockville, MD: Health Resources and Services Administration. U.S. Department of Health and Human Services.
IOM (Institute of Medicine). 1988. The future of public health. Washington, DC: National Academy Press.
———. 2003a. The future of the public’s health in the 21st century. Washington, DC: The National Academies Press.
———. 2003b. Who will keep the public healthy: Educating public health professionals for the 21st century. Washington, DC: The National Academies Press.
Mott, R. L. 2006. Military health. Paper presented at Second Meeting of the Committee on Training Physicians for Public Health Careers, Washington, DC.
NACCHO (National Association of County and City Health Officials). 2006. 2005 national profile of local health departments. Washington, DC: National Association of County and City Health Officials.
Parkinson, M. 2006. Presentation to the committee on training physicians for public health careers: Physicians for careers in public health. Paper presented at Third Meeting of the Committee on Training Physicians for Public Health Careers, Washington, DC.
Rowitz, L. 2001. Public health leadership: Putting principles into practice. Sudbury, MA: Jones and Bartlett.
———. 2006. Public health leadership development 2010: A seamless approach for the future. Paper presented at CDC Leadership Summit, Atlanta, GA.




















