
5
Envisioning a Better System of Continuing Professional Development
The Institute of Medicine’s (IOM’s) report Health Professions Education: A Bridge to Quality (2003) called for improving the health care workforce and affirmed the quintessential value of education and training in advancing this mission. The report recommended a set of five competencies that all health professionals should possess. Ensuring that health professionals attain and maintain these competencies should be at the heart of a new continuing professional development (CPD) system, which would hold as its ultimate aim improving patient outcomes and protecting patient safety. As outlined briefly in previous chapters, an effective CPD system should ensure that health professionals are prepared to:
-
Provide patient-centered care. At its core, a CPD system will embody an ethical commitment to ensuring health and patient safety. CPD holds the promise of equipping clinicians with powerful tools to better communicate with patients, while strengthening their ability to advocate for disease prevention and wellness. CPD will enable clinicians to more easily keep pace with the evolving evidence base relating to their patients’ diverse values, preferences, backgrounds, and well-being.
-
Work in interprofessional teams. Team-based learning and training will be central to promote coordination and collaboration across health professions, helping them to learn with, from,
-
and about one another. Effective coordination and use of interprofessional teams of practitioners in the care setting requires practice and the development of a collaborative skill set that is not routinely taught at other levels of health professions education. Imparting such proficiencies should be a key feature of a CPD system.
-
Employ evidence-based practice. New knowledge generated by health research is a potent driver of CPD, providing rich sources of information in learning. Advances in health care can be made when research identifies and fills knowledge gaps. Clinical outcomes data for individual, team, and institutional assessment can identify the successes and areas of inadequacies of current practice, lay the groundwork for improvement, and continuously guide the evolution of a strengthened system of care.
-
Apply quality improvement. All professionals in health care should aim for continuous improvement of their performance to deliver the best patient care. CPD should model principles of quality improvement by continuously evaluating the quality of structure, processes, and outcomes of CPD activities. The CPD system will benefit when its providers and researchers collaborate with other professionals in the quality improvement community; efficiencies gained from such collaborations could yield important benefits to patients. For example, grounding the quality improvement efforts of health professionals into proven educational techniques will provide systems-based feedback to planners, policy makers, and participating health professionals. Through this collaboration, CPD can serve as a precise tool in the learning health care system, supporting provision of care toward the six quality aims.
-
Use health informatics. Modern health information technologies provide an unprecedented opportunity for capturing and rapidly analyzing real-time data at the point of care to help clinicians manage data, improve safety, make informed clinical decisions, and access information or community resources. The field of health informatics encompasses e-learning, electronic data collection, collation and analysis, electronic decision support, and information management from individuals to populations to illuminate best practices in health service delivery. The CPD system will enlist these resources to advance learning and quality care.
VISION FOR A SYSTEM OF CONTINUING PROFESSIONAL DEVELOPMENT
An effective continuing professional development system would offer significant improvement over today’s fragmented approach to continuing education. Whereas the current funding of CE by commercial groups may hold inherent conflicts of interest that shift the focus away from improving health professionals’ performance, a CPD system would promote patient-centered care. Moreover, a CPD system would help obviate some of CE’s current fragmentation by driving coordination of activities and fostering interprofessional teams. A CPD system would be thoroughly evidence-based in its delivery, innovation, and research, representing a marked change from the current disconnect between CE theory, research, and practice that have resulted in few evidence-based activities to support health professionals’ competence and patient outcomes. A CPD system would help clinicians achieve quality improvement, while peer-reviewed studies of CE can claim to support only minimum levels of competence and have infrequently proven effective for improving the quality of care. Although CE has minimally used health information technologies in training and education, a comprehensive CPD system would foster development and dissemination of technology-based approaches.
The structure of the CPD system needs to support the system’s goals and deliver systematic and timely information to health professionals based on their learning needs and the challenges they encounter in clinical practice. First, CPD research must be driven by learning theory inclusive of insights and advances from the social, biological, and health sciences. Second, funding for CPD should be guided by sound economic principles and should set a goal of improving patient outcomes, not promoting a particular product or service. Third, implementing an effective CPD system will require mobilizing the CPD enterprise to promote a culture of learning for patient care. Fourth, the CPD system must be accountable and transparent to the public.
In a comprehensive CPD system, individual health practitioners would be committed to and take control over their own professional development and learning. Achieving this will require making the system learner-driven and more responsive to learners’ requirements and flexible enough to adapt to the learning opportunities that present with the ever-changing needs of patients.
CPD needs to facilitate health professionals’ learning beyond the classroom and professional conferences. It must be an ongoing process that occurs at the point of care, in conversations with col-
leagues, and in the many other ways that clinicians resolve daily problems of patient care. A high-performing system would recognize that health professions education is not limited to formal educational activities and must integrate with the learning that health professionals internalize in their everyday practice.
CPD also must be tailored to the various stages of a health professional’s career. The learning needs and opportunities of novice health practitioners should be differentiated from those of intermediate or expert practitioners. These stages of expertise, defined by topics and experience, carry important implications for educational design. These processes are much more complex than simply knowing or not knowing. On a finer scale, knowledge of any clinical skill can be broken down into four progressive stages:
-
Declarative knowledge: the learner gains the awareness to identify a problem or to know what should be done;
-
Procedural knowledge: the learner not only understands that there is a problem to solve but also gains knowledge of how to go about solving it;
-
Competence: the learner advances to a stage where he can demonstrate or show how a problem is to be solved; and
-
Performance: the learner identifies the problem, knows how to address it, demonstrates the needed skill, and solves the problem in practice—the learner does what he has learned.
These stages of skill acquisition can serve as a useful framework for the assessment of clinical skill development (see Figure 5-1) (Moore et al., 2009).
As a fundamental requirement, all health professionals should understand the value of CPD and incorporate CPD into their careers. The importance of CPD should be infused as individuals enter their health professional training and should be reinforced and sustained throughout their careers. The tenets of CPD should therefore be anchored by lifelong learning. Understanding the importance of CPD through prelicensure training helps to firmly secure this pursuit as a lifelong professional commitment and a vitally important educational practice of responsible health professionals.
The CPD system should address clinicians’ learning needs at the point of care where practice-based inquiry and the learning needs of clinicians originate, and CPD methods should provide the skills or tools required to meet those needs. The system needs to further efforts to develop valid and reliable measures for assessing the progress of learners, the associated health care outcomes of patients, and
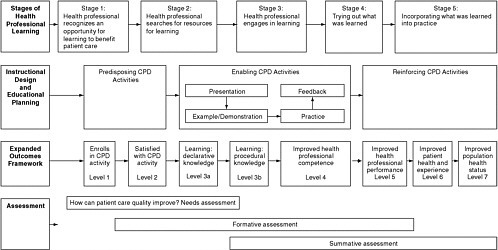
the value of the CPD system in improving health care. Figure 5-1 recognizes that health professionals’ learning needs are not all alike and that specific skills are necessary to meet specific needs. Different instructional design and educational plans will be required, depending on the given learning opportunity and stage of learning. Targeted learning methods can be used to teach a particular skill, from predisposing activities, to enabling activities, to reinforcing activities. As discussed in Chapter 2, appropriate outcomes, such as improvement in a health professional’s learning and/or behavior change, exist along a spectrum of outcomes levels. Proper use of targeted tools will lead to effective CPD, but not all learning activities are appropriate to advance all types of skills and to achieve all varieties of outcomes in all contexts. Resultant outcomes must be assessed to determine their value in specific contexts to the individual practitioner’s learning or performance, patient health, and population health.
After the formative assessment of the value of CPD outcomes, a summative needs assessment brings the CPD cycle back to where it began, with the identification of a new set of practice-based learning needs to be addressed through another round of tailored CPD (see Box 5-1 for an example). A CPD system based on this cycle will meet the needs of individual health professionals and the health care system to improve quality and patient safety.
Recommendation 2: To achieve the new vision of a continuing professional development system, the planning committee should design an institute that:
-
Creates a new scientific foundation for CPD to enhance health professionals’ ability to provide better care;
-
Develops, collects, analyzes, and disseminates metrics, including process and outcome measures unique to CPD;
-
Encourages development and use of health information technology and emerging electronic health databases as a means to provide feedback on professionals’ and health system performance;
-
Encourages development and sharing of improvement tools (e.g., learning portfolios, assessment resources) and theories of knowledge and practice (e.g., peer review systems for live documentation, such as wikis) across professions;
-
Fosters interprofessional collaboration to create and evaluate CPD programs and processes; and
|
BOX 5-1 CPD: One Surgeon’s Performance and Value A well-respected general surgeon at a community hospital subscribes to her profession’s major journal and reads the articles thoroughly to keep up with advances in the field. She is particularly impressed with the results of one study of a new laparoscopic procedure showing significantly short-ened hospital length of stay compared to open surgery. Reading the study carefully, she notes that it was performed at a major academic medical center whose staff had had many months of experience performing the procedure prior to the study. She would like to provide the same benefit to her patients that was found in the study, but recognizes that she and her staff are inexperienced with the new laparoscopic procedure and might do harm to patients while learning. This surgeon identified a specific learning need (practice of the laparoscopic procedure) for a patient-centered care goal, requiring a tailored continuing professional development (CPD) activity to achieve the needed training. At this point, it is important to recognize that the surgeon already had completed at least one CPD cycle related to the procedure: she learned of the procedure by reading her professional journal, assessed the value of this knowledge in her individual practice setting, and performed a needs assessment to identify the need for greater practice with the procedure before actually performing it. In this case, a surgical simulator CPD activity would allow needed practice of the laparoscopic technique by the surgeon and her team, avoid harm to patients that might accrue if the surgeon had simply attended lectures before attempting the procedure, and benefit the community hospital’s patients through a shorter hospital length of stay. |
-
Improves the value and cost-effectiveness of CPD delivery and considering ways to relate the outputs of CPD to the quality and safety of the health care system.
STEPS TO ENHANCE CONTINUING PROFESSIONAL DEVELOPMENT
The steps needed to support this vision include developing a new scientific foundation of CPD, developing new measures to assess CPD and its impact, developing and implementing health information technologies, identifying effective education improvement tools, enhancing interprofessional collaboration, and generating the “value proposition” for CPD that fully captures the value of CPD in improving health care quality and patient safety.
Developing a New Scientific Foundation for CPD
CE research is fragmented, may overlook insights from educational theory, and typically focuses too narrowly on professional learning in nonclinical contexts. CE research methods incorporate both qualitative and quantitative research designs. Research topics include the identification of theoretical constructs of change and learning and the measurement of improved patient outcomes associated with planned educational interventions. The construct of CPD refers to the body of concepts, variables, and theories that underlie the field. However, the current evidence inadequately answers questions regarding the effectiveness of learning activities and does not provide clear guidance for investing in CPD. A review of the research agenda and improvements in research will be critical to the success of the CPD system. Greater emphasis must be placed on integrating CPD research efforts that already exist, as well as on developing further research capabilities to create a new construct for CPD. Stronger research on theory, methods, and outcomes related to CPD will be the foundation for progress. This construct ought to improve health outcomes by effectively translating knowledge to support a continuous loop of research to inform practice and practice to inform research.
To facilitate understanding and evaluation of CPD techniques, CPD researchers need to adopt a common framework, whether focused on the educational theory supporting CPD or its clinical application. This framework should incorporate insights regarding CPD that have been gleaned from diverse disciplines, including adult education, psychology, sociology, health informatics, and organizational change. It also should integrate and harmonize the terminology and taxonomy used to describe CE methods in the health professions literature, employed by accreditors, and used by the various health professions. This step would result in a much-needed common language to facilitate communication and mutual collaboration toward building a new and shared culture of CPD.
A high-performing CPD system requires a stronger scientific foundation of CPD and includes a comprehensive research agenda to systematically identify gaps in evidence at the patient, practitioner, organizational, and societal levels. Once identified, these gaps should be pursued as opportunities and addressed through improvements in health professionals’ knowledge, skills, and attitudes. Coordination of efforts would be emphasized to streamline the generation and dissemination of innovations and reduce unwitting duplication of research efforts.
Developing New Measures to Assess CPD and Its Impact
A measurement system needs to be established to assess CPD and its impact on health professionals’ performance, which would provide needed guidance for investing in CPD. Measures should facilitate the identification and teaching of skills required to meet educational needs, and alignment of good learning and good health care. The measurement of CPD should allow for straightforward assessment at the higher levels of outcomes (Moore et al., 2009). Data from this measurement system should serve to enhance evidence-based CPD and the existing quality measurement enterprise, bridging the two fields, promoting their collaboration, and helping to ensure cross-disciplinary communication.
Developing standardized measures would represent an important step toward developing robust assessment of CPD, and an interprofessional approach to measure development will be important. Because CPD exists at the unique intersection of fields including health care, education, and the social sciences, metrics that match the unique nature of CPD will need to be developed. In a comprehensive CPD system, measures for evaluation of impact and value would be collected. Studies of costs, effects, and benefits of CPD would accelerate and more fully integrate CPD with systematic efforts involving quality improvement and patient safety. Organizations such as the National Quality Forum, the Agency for Healthcare Research and Quality, the National Committee for Quality Assurance, and the Institute for Healthcare Improvement, which have developed an infrastructure to set priorities, create and endorse performance measures, and publicly report data to improve care quality, would benefit from the additional resource of CPD in helping to assure the application and measurement of innovation in clinical practice.
Developing and Implementing Health Information Technologies
Over the past decade, modern health information technology has created innovative ways to support CPD. Computers, mobile computing devices (e.g., personal digital assistants, smart phones), computer networks linked through the Internet, and simulators have demonstrated their utility to help individuals and groups in their CPD. These tools can provide powerful knowledge acquisition opportunities, realistic simulations of case scenarios, unprecedented computer modeling and gaming for individual and team skills training, and timely data collection for audit and reflection. Further, decision support software accessible through computer or mobile technologies and social networking environments can amply support
|
BOX 5-2 Examples of Technology-Enabled CPD Current examples of technology-enabled continuing professional development (CPD) approaches and the gradual accumulation of evidence to support their effectiveness include the following:
|
tailored, just-in-time information and knowledge exchange opportunities for unstructured learning or tacit knowledge acquisition.
With the emerging technology-enabled CPD initiatives described in Box 5-2 and other initiatives, a new world of learning can be developed and integrated into learning environments for knowledge capture, dissemination, transmission, and reflection. These approaches and those using other emerging technologies, such as smart phones or social networking approaches, ought to be rigorously studied to validate their efficacy in supporting learning and, if found effective, integrated into mainstream CPD.
|
Identifying Effective Education Improvement Tools
Research has already made significant progress in identifying effective education methods. The attributes and principles of effective CE interventions noted in Chapter 2 include needs assessments to guide CPD providers and learners, interactivity, continuous integrated feedback, and the use of multiple learning methods. These attributes and principles are well known (Davis et al., 1999, 2006; Marinopoulos et al., 2007; Ratanawongsa et al., 2008), but little effort has been made to systematically translate them into practice so they can be broadly applied to CPD learning activities. Research on CPD needs to build on this existing knowledge base for effective learning
and should encourage the application of such research to improve the effectiveness of CPD methods.
A better system would identify effective learning activities based on standardized, transparent pilot testing and evaluation of resultant learning, performance improvement, and patient outcomes. Once promising CPD activities are shown to be effective, implementation mechanisms need to be developed and robust measures should be employed to determine their impact on patients and professionals.
The CPD system will seek to promote innovative learning strategies at the health professional, organizational, and systems levels. Innovation needs to be rewarded through research that pilots and disseminates promising new methods and employs standardized monitoring of impact. Lifelong learning, practice-based learning, workplace learning, and learning portfolios are examples of innovations in CPD that have significant promise for advancing the science of performance improvement based on existing evidence.
-
Lifelong learning is a necessary practice for any health professional, because of the rapidly advancing state of knowledge in all health care fields. There may be no more central skill for CPD than the ability to identify questions to be addressed in one’s practice, independently muster resources to address those problems, and reassess one’s learning needs as a matter of common practice. These skills typify the lifelong learner.
-
Practice-based learning is a term applied to any learning activity whose material for study and improvement is the practitioner’s workplace or panel of patients. Practice-based learning ensures that the skills and knowledge gained by professional learners are relevant to the patients they care for and their problems. As a result, practice-based learning has a higher probability of positively impacting those same patients.
-
Workplace learning emerges in a just-in-time fashion as part of everyday work activities. Workplace learning may be useful in preventing errors, supporting a culture of reflection on and in action, and encouraging sustained learning environments.
-
Learning portfolios are based on the adult learning principle of analysis of and reflection on experience. They enable practicing health professionals to document, formally assess, and learn from their clinical and educational experiences. Learning portfolios can be either web-based or exist in hard copy. As interactive professional development tools, some portfolios have built in milestones of accomplishment that can inform patients, the public, and regulators of the experiences
-
of a professional. Learning portfolios have been effectively used in a variety of learning environments (e.g., visual arts students, K-12 and college education). Specific to health care, learning portfolios were first adopted by nurses and midwives and have now spread to other health professions, especially in the United Kingdom, and they have been adopted in the United States by the Accreditation Council for Graduate Medical Education in the case of medical residents. They offer much promise to support lifelong learning for all health professionals.
Enhancing Interprofessional Collaboration
Collaboration among professions is necessary for the provision of optimal health care in modern health care settings (see Box 5-3). Interprofessional education through CPD can be the transformative force to promote and inspire seamless collaboration, help diffuse advances across fields, and optimize the way professionals operate, both individually and jointly. Interprofessional education is defined as “any type of educational training, teaching, or learning session in which two or more health and social care professions are learning interactively” (Reeves et al., 2009). Interprofessional education therefore not only educates clinicians from multiple professions together but also fosters the development of a culture that promotes interprofessional, team-based care for improved health care quality and patient safety. This culture shift cannot occur in isolation in the CPD community, but it will be critical throughout the trajectory of health professionals’ lifelong learning.
CPD is an ideal forum through which collaboration can promote team-based care, and greater inclusion can spark synergistic advances among professionals’ knowledge. At no other stage of health professionals’ training are they as exposed to, dependent on, and accountable to members of the health care team from professions other than their own. The greater amount of interaction and interdependence with other professions makes CPD a logical stage at which to foreground interprofessional collaboration and education. CPD methods can reduce barriers between professional silos, allowing interprofessional collaboration to carry over into practice.
Generating the Value Proposition for CPD
Demonstrating the value or business case for CPD is largely unexplored at present; its value will be in improving health care
|
BOX 5-3 Interprofessional Team-Based Learning and Care The stroke team at Saybrook Hospital took part in a CPD training initiative in care coordination that included group process analysis and quality improvement workplace learning discussions. The primary team consisted of the neurology service, intensivists, nursing personnel, radiology, ICU (intensive care unit) pharmacists, and respiratory therapy. The team studied the case of a stroke patient, upon presentation to the emergency room (ER) and transfer to the ICU. On assessment, the team discovered underlying, poorly controlled hypertension that contributed to the stroke, and the cardiology service was added to the team. In following this case over a prolonged hospital stay, roles of multiple team members were identified: the ICU team of physicians, respiratory therapists managing the patient’s mechanical ventilation, neurology service, nursing staff, physical and occupational therapists performing serial functional assessments, a nutritionist approving a low-salt diet to address the underlying hypertension, and the cardiology team ordering new medication to control the patient’s blood pressure. The team discussed how to share the care plan and other pertinent data needed to assess and recommend therapies and patient education. As the case progressed to discharge, blood pressure medication was titrated to the optimal dose, dietary changes were established, and referrals made for follow-up disease management services and a course of physical therapy. Upon recognizing that the only physical therapy facility accepting the patient’s health insurance was 20 miles from the patient’s home, the team strategized ways to facilitate care delivery and effectively transition to the patient’s primary care team. Soon after completing the CPD exercise, a patient with a major stroke was admitted through the ER to the ICU. Due to the lessons learned through CPD, the inpatient team implemented the identified strategies to enhance collaboration and deliver high quality care. The primary care doctor informed the inpatient team that the patient’s respiratory condition had been exacerbated by similar blood pressure medications in the past, and the cardiology team found an alternate blood pressure regimen. The primary care physician also informed the inpatient team that the patient did not have access to transportation to the physical therapy facility, prompting the inpatient physical therapist to arrange for care through a clinical trial at a nearby academic stroke rehabilitation center. The outpatient nutritionist was able to use the hospital nutritionist’s initial assessment and make needed adjustments rather than starting from scratch. These adjustments improved the quality of the care that this hypothetical patient received, as the result of team-based training through CPD. |
quality and patient safety. The value proposition for CE can be derived through its profit generation for academic centers, professional societies, industry, and the public. The value of CPD to the patient paying for care and to the health practitioner must also be considered, as well as the value to the health care system as a whole. Metrics to determine the value of CPD need to be developed, including clear methods of determining the impacts of CPD on the quality and cost of care. Ultimately, arriving at the value proposition for CPD will be essential to understanding the best ways to invest CPD resources.
COLLABORATION WITH STAKEHOLDERS FOR HEALTH CARE QUALITY
Both interprofessional and intraprofessional collaboration are necessary for a high performing CPD system. To maximize the quality of learning, organizations and groups driving continuing education need to work in synergy to develop a more effective and efficient system (see Box 5-4 for an example in medicine). Such programs ought to be organized within each health profession, coordinated with those of other health professions, and ultimately work in partnership with other health care organizations. The committee believes collaboratives are important to the functions of a CPD system and need to work with other organizations that have the funding and authority to pull the various stakeholders together from all relevant health professions.
A culture of learning to support quality will span both the CPD system and the quality improvement community. To benefit CPD, those in quality improvement should use the infrastructure already in place for data collection and reporting mechanisms. This relationship is logical: CPD is a major component of specialty certification, licensure, and credentialing for privileges and includes educational systems that are important for the dissemination of clinical innovations and knowledge derived from quality improvement and quality improvement research. The drive for competence and continuous improvement of service is integral to professionalism and the lifelong pursuit of knowledge. The benefits that each domain contributes to the other could be mutually reinforcing and exponentially accrued.
Others involved in CPD, including funders, providers, and regulators, share the common aims of optimizing health professional knowledge and patient health outcomes. A highly collaborative approach among these groups would likely drive more effi-
|
BOX 5-4 Example of a Collaborative on Continuing Medical Education (CME) The Conjoint Committee on Continuing Medical Education (Conjoint Committee) has advocated for reform of continuing medical education, recommending that leaders of organized medicine address accreditation, certification, credentialing, licensure, and funding of CME (Spivey, 2005). The Conjoint Committee recently proposed that each medical specialty and subspecialty should develop competency-based curricula to support member learning, self-assessment, and continuing competence (Jackson et al., 2007) and that state medical boards should require valid and reliable assessment of physicians’ learning needs (Miller et al., 2008). Most recently, the Conjoint Committee recommended that research in continuing medical education should be raised to a national priority (Miller et al., 2008). Member organizations include the following: Accreditation Council for Continuing Medical Education Alliance for Continuing Medical Education American Academy of Family Physicians American Board of Medical Specialties American Hospital Association American Medical Association American Osteopathic Association Association for Hospital Medical Education Association of American Medical Colleges Council of Medical Specialty Societies Federation of State Medical Boards Society for Academic Continuing Medical Education Four other member groups are participants in the Conjoint Committee but are not full voting members: Accreditation Council for Graduate Medical Education, Journal of Continuing Education in the Health Professions, National Board of Medical Examiners, and The Joint Commission. |
cient resource allocation and increase the value of available CPD activities.
Recommendation 3: The planning committee should design the Continuing Professional Development Institute to work with other entities whose purpose is to improve quality and patient safety by:
-
Collaborating with the Agency for Healthcare Research and Quality, the Centers for Medicare and Medicaid Ser-
-
vices, the Joint Commission, the National Committee for Quality Assurance, the National Quality Forum, and other data measurement, collection, cataloguing, and reporting agencies to evaluate changes in the performance of health professionals and the need for CPD in the improvement of patient care and safety; and
-
Involving patients and consumers in CPD by using patient-reported measures and encouraging transparency to the public about performance of health care professionals.
DISSEMINATION OF CPD
In a comprehensive CPD system, proven techniques and methods would be identified and disseminated systematically to provide the greatest benefit for the investment. Mechanisms for spreading effective learning methods could take a number of forms. Descriptive reports detailing these methods could be distributed widely to CPD providers and health professionals interested in advancing training. Alternatively, effective CPD methods could be taught by qualified CPD providers to other providers. This would require a much more coordinated effort of training and evaluation than currently exists among CPD policy makers, planners, and evaluators, but such coordination would greatly facilitate the dissemination of CPD advances and eventually be of great benefit to patients and clinicians.
With a framework of CPD research and practice improvement, CPD providers will progressively increase their adherence to evidence-based CPD and surveillance data and contribute knowledge regarding CPD, improvement, and patient safety. An innovative e-health infrastructure can provide this opportunity through a variety of methods. For example, multimethod educational materials and electronic newsletters could support just-in-time learning; social networking environments such as Facebook and Twitter could promote tacit knowledge acquisition and co-creation of clinical knowledge, increasing opportunities to engage in electronic communities of practice. Simulations could also be used to train individuals and teams in disease management techniques. As technology advances, so, too, do the opportunities for e-learning.
ENHANCING THE PROFESSION OF CONTINUING PROFESSIONAL DEVELOPMENT
In a better CPD system, schools, universities, and colleges would offer professional degrees or certificates with curricula designed to dramatically improve health professions education. Continuous learning—a much more dynamic approach to evidence development and application—would take full advantage of newer information technology to implement innovations. Programs and institutions dedicated to continuous learning and health care improvement would help the CPD system develop by providing a stable infrastructure and learning environment. Such institutions would house faculty expert in CPD. It is conceivable that many health professionals would want to learn in a specialized institution dedicated to developing comprehensive and integrated CPD programs, rather than collecting credits in a piecemeal and disjointed fashion. If these CPD programs were structured to provide premier educational opportunities, the professional drive to achieve excellence would likely also spur health professionals to enroll. Further, involvement in a community of professional learners and teachers to help individual practitioners advance would be a strong incentive for clinician enrollment, especially if the knowledge and skills they gained could be tied to improving the economics of their practice and improving the value of their care. As centers of CPD activity and scholarship, these institutions would be ideal vehicles to pilot-test and assess effective CPD curricula by providing reliable contexts for implementation and evaluation. Additionally, institutional structures for CPD could provide new levels of visibility and accountability for CPD and its resultant outcomes for learning, although health professionals would be responsible for their own learning and performance outcomes.
Current providers of CPD represent a resource for advancing CPD. CPD providers are skilled in needs assessment, instructional design, and program evaluation. Their roles as educators and mediators of health care quality improvement are critical but would be enhanced in a more effective CPD system, potentially leading to less variability, rational assessment standards for CPD pedagogy, and greater accountability. Ensuring that CPD providers receive access to quality data should improve the ability of assessment, education, and evaluative activities to influence the quality of care. Precision of research and evaluation also should improve with the development and availability of more valid and reliable outcome measures. CPD providers could also assume an important role in disseminating advances in CPD learning methods. Finally, like any
group of professionals, CPD providers need to be held accountable to an ethical standard that best protects against conflicts of interest within the CPD system. These changes would bolster the value of providers, increase their motivation to improve instruction, and accelerate advances in CPD.
PUBLIC INVOLVEMENT AND ACCOUNTABILITY
Patients and consumers must be partners in a high-performing CPD system that promotes a culture of quality and patient safety. Transparency to the public and direct patient feedback and communication to health professionals foster a culture of accountability and purposeful learning. Patient input through patient-reported measures in research or by simply asking patients how quality of care could be improved are two ways to promote public involvement in CPD. Oversight systems should prioritize public accountability. Finally, efforts should be made to educate the public about CPD as the major mechanism for maintaining health professionals’ competence. The health care system should adjust to shortcomings in the CPD system to assure the public of health professionals’ competence.
CONCLUSIONS
Imagine a health care system with the ability to rapidly adapt to the needs of patients, health professionals, and institutions through a shared commitment to CPD and high quality patient care. Imagine a health care system in which everyone is a learner, supported on the arc of professional development with knowledge of tailored learning goals, the tools to meet and surpass those goals, and a community of other learners with whom to share the process. A comprehensive CPD system would transform this vision of professional learning into reality. To attain this goal, a new set of resources needs to be brought to bear, including a new scientific foundation for CPD, measures to assess the progress that CPD achieves, health information technology to spark faster transmission of data and facilitate learning activities, exchange of effective professional learning tools, interprofessional CPD programs, and a clear understanding among all stakeholders of the value proposition for CPD. Suffused throughout a better system must be a culture of public accountability, professionalism, and appreciation for the value of innovations in professional development, which will impel the system to better fulfill its aims. The recommended Continuing Professional Development
Institute (CPDI) is needed to drive these necessary improvements in CPD. Through guidance and coordination of efforts at these various levels, the CPDI can help the current system evolve into an improved system of effective continuing professional development to benefit practitioners, patients, and the public good.
REFERENCES
Cook, D. A., A. J. Levinson, S. Garside, D. M. Dupras, P. J. Erwin, and V. M. Montori. 2008. Internet-based learning in the health professions: A meta-analysis. Journal of the American Medical Association 300(10):1181-1196.
Davis, D., M. A. O’Brien, N. Freemantle, F. M. Wolf, P. Mazmanian, and A. Taylor-Vaisey. 1999. Impact of formal continuing medical education: Do conferences, workshops, rounds, and other traditional continuing education activities change physician behavior or health care outcomes? Journal of the American Medical Association 282(9):867-874.
Davis, D. A., P. E. Mazmanian, M. Fordis, R. Van Harrison, K. E. Thorpe, and L. Perrier. 2006. Accuracy of physician self-assessment compared with observed measures of competence: A systematic review. Journal of the American Medical Association 296(9):1094-1102.
Fordis, M., J. E. King, C. M. Ballantyne, P. H. Jones, K. H. Schneider, S. J. Spann, S. B. Greenberg, and A. J. Greisinger. 2005. Comparison of the instructional efficacy of Internet-based CME with live interactive CME workshops: A randomized controlled trial. Journal of the American Medical Association 294(9):1043-1051.
IOM (Institute of Medicine). 2003. Health professions education: A bridge to quality. Washington, DC: The National Academies Press.
Jackson, M. J., H. A. Gallis, S. C. Gilman, M. Grossman, G. B. Holzman, D. Marquis, and S. Trusky. 2007. The need for specialty curricula based on core competencies: A white paper of the Conjoint Committee on Continuing Medical Education. Journal of Continuing Education in the Health Professions 27(2):124-128.
Marinopoulos, S. S., T. Dorman, N. Ratanawongsa, L. M. Wilson, B. H. Ashar, J. L. Magaziner, R. G. Miller, P. A. Thomas, G. P. Prokopowicz, R. Qayyum, and E. B. Bass. 2007. Effectiveness of continuing medical education. Evidence report/technology assessment no. 149. Rockville, MD: Agency for Healthcare Research and Quality.
Miller, S. H., J. N. Thompson, P. E. Mazmanian, A. Aparicio, D. Davis, B. Spivey, and N. Kahn. 2008. Continuing medical education, professional development, and requirements for medical licensure: A white paper of the Conjoint Committee on Continuing Medical Education. Journal of Continuing Education in the Health Professions 28(2):95-98.
Moore, D. E., J. S. Green, and H. A. Gallis. 2009. Achieving desired results and improved outcomes: Integrating planning and assessment throughout learning activities. Journal of Continuing Education in the Health Professions 29(1):1-15.
Ratanawongsa, N., P. A. Thomas, S. S. Marinopoulos, T. Dorman, L. M. Wilson, B. H. Ashar, R. G. Miller, G. P. Prokopowicz, R. Qayyum, and E. B. Bass. 2008. The reported validity and reliability of methods for evaluating continuing medical education: A systematic review. Academic Medicine 83(3):274-283.
Reeves, S., M. Zwarenstein, J. Goldman, H. Barr, D. Freeth, M. Hammick, and I. Koppel. 2009. Interprofessional education: Effects on professional practice and health care outcomes. Cochrane Database of Systematic Reviews 23(1).
Spivey, B. E. 2005. Continuing medical education in the United States: Why it needs reform and how we propose to accomplish it. Journal of Continuing Education in the Health Professions 25(3):134-143.






















