
4
Behavioral and Social Sciences Research
INTRODUCTION
Basic behavioral and social sciences research is indispensible to the mission of the National Institutes of Health (NIH). Not only do psycho-social-biological factors directly affect disease outcomes per se, but also behavioral and social processes are linked to molecular, genetic, and neural processes affecting health and disease. Basic behavioral and social sciences research promotes health by predicting, preventing, and controlling illness, and by minimizing the impact of disease. A range of empirical investigations convincingly show that social and behavioral factors interact robustly with essentially every aspect of health and illness, spanning the entire disease process from vulnerability to diagnosis, treatment, course, prognosis, interface with health care systems, rehabilitation, and quality of life. The economic costs and human burdens of physical and mental disease result disproportionately from interrupting normal behavioral and social functioning.
Basic behavioral and social sciences research aims to measure, understand, and control processes that may later be applied to health and illness. As with all basic science, the direct link between fundamental research and health outcomes results from incremental discoveries that accumulate as an investment over time. There exist many examples of how basic behavioral and social sciences research has already increased knowledge about health and illness, including: (a) animal learning research has contributed to empirically validated behavioral treatments of various mental disorders, from phobias to addictions; (b) basic research on emotion explains disruptions by physical and mental illness, pointing to new treatments; (c) basic perception research informs diagnosis and treatment of neural disorders; (d) reliable results show how social networks shape all kinds of health behavior and psychobiological outcomes, from prevention to treatment to survival; (e) fundamental research on intergroup relations reveals underlying patterns and unconscious causes of health disparities for ethnic minorities, older adults, and sexual minorities; and (f) persuasion research reveals automatic processes that influence interactions with health care providers and determine both prevention and treatment outcomes.
Impressive gains in the science of brain, mind, and behavior provide new insights into health and illness, as well as new measurement methods, such as neuro-imaging and epigenetic indicators. At a much more macro level, environmental contexts and psychological, social, and cultural processes facilitate or constrain vulnerability to disease, risk behaviors, health promotion, proper health care, and re-entry into the community.
The behavioral and social sciences are as complex and variable as the natural sciences; not only do many factors affect individual and social behavior, but also these factors combine and interact in complicated ways. Partly because of the overall complexity of these sciences and partly for historical and cultural reasons, research support and research training in the behavioral and social sciences has lagged well behind those in other sciences. However, as noted, behavioral and social sciences contribute substantially to health research, primarily in psychosocial vulnerability, prevention behavior, treatment maintenance, and psychobiological response to treatment. Moreover, recent years have seen a tremendous leap in the sophistication of methods and tools in these sciences, leading to significant contributions regarding health behavior and contexts, as well as a realistic expectation that even more useful and effective answers to fundamental health questions will result from an investment of research training in these areas.
At the same time that these sciences have been maturing, our society has come to realize the absolute necessity of the research findings they produce for the understanding, treatment, and prevention of its health problems. As a result, scientists in these areas have been called on for advice to an ever-increasing degree by government agencies. Just one example is provided by the number and range of government-commissioned committees, panels, and reports assigned to
the Division of Behavioral, Social, and Economic Sciences (DBASSE) at the National Research Council. In the past 10 years there have been more than 300 publications (books) in response to DBASSE assignments, covering a wide range of areas that are directly or indirectly related to health concerns, including: children and families; education, employment, and training; environment; health and behavior; human performance; international studies; law and justice; national statistics; and population and urban studies. Their level of focus ranges from the individual level to the societal level, and they cover the entire range of social and behavioral sciences and extend even to such related fields (such as ecology and criminology). A few examples of reports directly relevant to health concerns include: Reducing Underage Drinking: A Collective Responsibility; Educating Children with Autism; Informing America’s Policy on Illegal Drugs: What We Don’t Know Keeps Hurting Us; Preventing Reading Difficulties in Young Children; Protecting Youth at Work: Health, Safety, and Development of Working Children and Adolescents in the United States; Work-Related Musculoskeletal Disorders: A Review of the Evidence; Understanding Risk: Informing Decisions in a Democratic Society; Understanding Violence Against Women; Preventing HIV Transmission: The Role of Sterile Needles and Bleach.
As described in the 2005 NRSA report:
The social and behavioral sciences deal with the most complex and the least predictable phenomena that affect the nation’s health. One tends to think of mental health in this context, and indeed mental health is an important concern at NIH (in NIMH in particular) and in the government and private sector generally. Yet mental health is only one part of a much larger picture, because many of the most important health problems we face are determined and strongly affected by behavioral, social, and economic factors. Consider just a few examples: At the level of behavior of the individual, the behavioral and social sciences produce knowledge about health issues, such as drug and alcohol abuse, obesity, violent behavior, smoking, maintenance of drug treatment regimens, stress management, ability to cope with illness, and health decision-making. There are many critical health issues that emerge at a larger scale. The economics of health care and delivery critically determine what diseases and problems are attacked, what research is carried out, and which populations are given treatment. The government has recognized these factors with multi-million-dollar investments in surveys such as the Health and Retirement Survey, the National Longitudinal Survey, and the National Survey of Families and Households. The social sciences provide critical insights and knowledge concerning our ability and willingness to deal with disability, choices that promote well being, the use of and willingness to expend income and assets for health purposes, distribution of health care (geographically, sociologically, and economically), use and misuse of nursing homes, health provider behavior, psychological and social effects on morbidity and mortality, social and psychological effects on treatment and recovery, transfer of assets and beliefs across generations, social support mechanisms, economics of alternative health-care systems, care-taking approaches, bereavement and its effects, and health decision making. Societal, behavioral, and economic factors all work together to produce such problems as drug abuse, smoking, alcohol abuse, anorexia/bulimia, and obesity. Treatable diseases are making a comeback in more virulent form because reliable methods cannot be found to insure that drugs are taken over their entire recommended time period. Social and sexual diseases, such as AIDS/HIV, are a large and increasing problem. Even crime and violence are in good part a health problem that requires behavioral and social science research. It is now accepted that many diseases that have historically been considered mainly a matter for biomedical research, diseases such as heart disease, lung disease, drug addiction, tuberculosis, and malaria, cannot be treated and understood without understanding provided by behavioral and social research. When these far reaching health implications of behavioral, social, and economic factors are added to the more direct implications of research for mental illnesses such as depression, schizophrenia, and various neurological illnesses, it is no surprise that the research demand in the behavioral and social sciences has grown rapidly in recent years.
The National Institute of Mental Health (NIMH) traditionally provided primary support for research in the behavioral and social sciences, and with secondary support from the National Institute on Aging (NIA) and the National Institute of Child Health and Human Development (NICHD). Other institutes provide support to a lesser degree, and recently there has been increasing support from the National Institute of General Medical Sciences (NIGMS). It should be noted that the primary mission of NIMH is research into prevention and treatment of mental disorders, and of NIA and NICHD is research into the health problems of young and aging populations; thus none directly supports research into key factors underlying such societal health problems. It is not the task of this committee to make recommendations concerning the allocation of research support in various institutes of NIH. It is the committee’s task, however, to make recommendations concerning research training and its funding, and the implications of social and behavioral research for such a wide array of health problems demand that research in most NIH institutes be informed by scientists knowledgeable in the basic techniques and methods of, and the findings of, the behavioral and social sciences. This particularly includes empirical design and quantitative and statistical methodology that has been so effectively refined in the social and behavioral sciences. Thus in institutes that do not presently have a direct focus on research in the behavioral and social sciences, at least some training needs be directed toward researchers with this focus.
CHARACTERISTICS AND DATA
Behavioral and Social Sciences Research Workforce
The behavioral and social sciences workforce is difficult to identify, since data sources do not distinguish between
Ph.D.s in the behavioral and social sciences or between scientists who are conducting basic or applied health-related research (or other research) and those who are involved in clinical practice. In studying the research training needs in the behavioral sciences, the workforce is defined as Ph.D.s trained in anthropology, sociology, the speech and hearing sciences, and psychology, with the exception of clinical, family, and school psychology. However, the committee believed that most non-research-oriented doctorates are now receiving Doctor of Psychology (Psy.D.) degrees, and so it decided to include clinical psychology in its assessment, although not the other practice-oriented fields. See Appendix C for a list of fields in the behavioral and social sciences. This decision was also supported by a small experiment in which NIH was asked to identify whether the research topic for the theses of a sample of the Ph.D. population in the above listed fields, including clinical psychology, would be considered for NIH funding. This analysis showed that about 90 percent of the research topics could be funded, and this led to the conclusion that a large portion of the clinical psychology Ph.D.s could pursue research careers. This may be an over estimate of the workforce, but it might provide a more accurate assessment.
Even in the treatment of what are to be considered biological diseases, behavior is a factor in getting patients to take their medicine or participate in physical activities that would help their condition. However, research in these areas is not isolated to the behavioral and social sciences but has an interdisciplinary component that can include fields in the life sciences, other social sciences, and even the physical sciences. This factor complicates the analysis, because people trained outside the social and behavioral science may be conducting research in this area. There is also a convergence of research areas across broad fields, such as the convergence between the psychology and neuroscience. This factor may lead to an undercount of doctorates in the behavioral sciences. For this study the behavioral and social sciences workforce is defined as graduates from universities in the United States with Ph.D.s in the fields listed in Appendix C, and those in or seeking careers in science and engineering fields.
Educational Trends
The pool of college graduates in the behavioral and social sciences from which graduate programs draw has increased from about 71,000 in 1986 to a little more than 160,000 in 2008 in the fields of psychology, sociology, and anthropology. In 1986, 11.4 percent, or 8,152, of these graduates matriculated to graduate programs in doctoral-granting institutions; by 2008 that fraction had dropped to about 7.3 percent or 11,700 students (see Figure 4-1).
This first-year enrollment has resulted in a total full-time graduate enrollment of about 40,847 in 1986, and it grew to about 69,300 in 2008. A portrait of the gender makeup of the full-time graduate students (Figure 4-2) shows a significant change over the past 30 years, from approximate gender parity
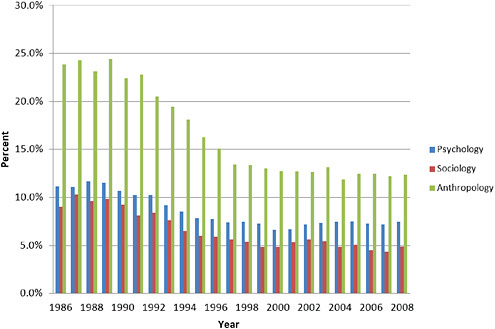
FIGURE 4-1 Percentage of college graduates that enroll as first-year graduate students by field in the behavioral and social sciences.
SOURCE: NSF. 2008. Survey of Graduate Students and Postdoctorates in Science and Engineering. Washington, DC: NSF.
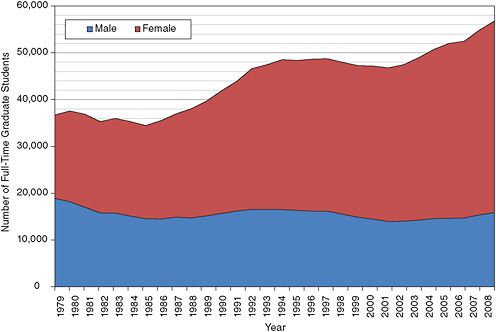
FIGURE 4-2 Gender of full-time graduate students in the behavioral and social sciences, 1979-2008.
SOURCE: NSF. 2008. Survey of Graduate Students and Postdoctorates in Science and Engineering. Washington, DC: NSF. in 1979, to a student population in 2008 where females out
numbered males by almost 3 to 1. Although there have been variations from year to year, the total number of male graduate students in this area hardly changed from 1992 to 2008.
These NSF data include all students in behavioral and social sciences programs at doctoral-granting institutions and therefore include students who do not complete a degree or receive a master’s degree and who do not pursue a doctorate. Clearly then these data must overestimate the pool of students who go on to earn a Ph.D. The National Research Council’s study of research-doctorate programs collected data on the number of students working toward a doctorate. These data cover only one year, 2006, but they are likely the best source that we have for information about students involved in research activities (see Table 4-1). They indicate that a little less than half, or 24,841 of the 52,000 graduate students in 2006, were in doctoral programs. They also show that the ratio of female to male doctoral students was 2 to 1, and in particular, was not as reported above.
The picture of financial support for graduate education at doctoral-granting institutions in the behavioral and social sciences is very different from that in the biomedical sciences (Figure 4-3). Traditionally about half of the graduate students are supported by their own funds or other sources that they have identified themselves, and teaching assistant-ships support as many students as fellowships, traineeships, and research grants. The proportion of support from these different mechanisms has changed little except for some recent growth in the students who are self-supported. This has implications both for post-graduation debt and for incentives to enroll in a postdoctoral program.
These data, like the data on enrollment, are useful in showing trends over time, but they include master’s degree students who may not receive financial support for their studies. Data from the Research-Doctorate Study for 2006 show a different pattern of financial support from the above. Of those programs reporting data, 78 percent said they fully support their doctoral students, and only 15 percent of such students are unfunded (see Table 4-2).
Doctoral Degrees Awarded
After steadily increasing through much of the 1970s, the number of doctoral degrees awarded in the behavioral sciences remained remarkably steady over much of the next 30 years (Figure 4-4), although there may have been a small decline in the past decade. The gender distribution in the number of doctoral degrees awarded since 1970 reflects the gender makeup of the graduate population in general as reflected in the number of doctoral degrees (Figure 4-4). From just a few hundred in 1970 the number of doctoral degrees to women grew to almost 3,000 by 2008, and at the same time degrees to men dropped from a high of about 2,700 in the mid-1970s to a low of about 1,400 in 2008.
TABLE 4-1 Number of Doctoral Students by Gender as Reported in 2006 for the Research-Doctorate Study
|
Field |
Male |
Female |
Number Doctoral Students |
|
Anthropology |
1894 |
3098 |
5039 |
|
Psychology |
4320 |
9646 |
14000 |
|
Sociology |
2189 |
3605 |
5802 |
|
Total |
8403 |
16349 |
24841 |
|
SOURCE: NRC. 2010. A Data-Based Assessment of Research-Doctorate Programs. Washington, DC: The National Academies Press. |
|||
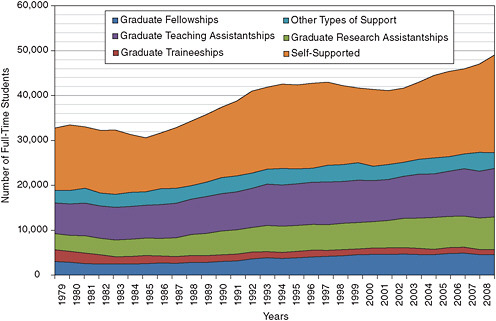
FIGURE 4-3 Financial support of full-time graduate students in the behavioral and social sciences, 1979-2008.
SOURCE: NSF. 2008. Survey of Graduate Students and Postdoctorates in Science and Engineering. Washington, DC: NSF.
TABLE 4-2 Financial Support of Students in the Behavioral and Social Sciences in 2006 as Reported in the Research-Doctorate Study
|
Field |
Fellowship or Traineeship |
Teaching Assistant |
Research Assistant |
Combination |
Less Than Full Support |
Unfunded |
Total |
|
Anthropology |
807 |
921 |
241 |
1087 |
379 |
1005 |
4440 |
|
Psychology |
2236 |
3341 |
2055 |
3718 |
775 |
1739 |
13864 |
|
Sociology |
761 |
1458 |
648 |
1186 |
418 |
807 |
5278 |
|
Total |
3804 |
5720 |
2944 |
5991 |
1572 |
3551 |
23582 |
|
SOURCE: NRC. 2010. A Data-Based Assessment of Research-Doctorate Programs. Washington, DC: The National Academies Press. |
|||||||
The time to degree for the doctorates in the behavioral and social sciences has been relatively constant during the past few years at about 9 years in psychology and 10 years in sociology, but these numbers are about 2.5 years higher than they were in the mid-1990s. These increases were greater than the corresponding increases in the biomedical sciences by about one-half a year. It is possible that these data on the time to degree also reflect time when a student is not actively working on the degree, and data from the Research-Doctorate Study show a time that is shorter by several years (see Table 4-3).
The median age at time of degree increased to almost 33 by the late 1990s and remained at that level up to at least 2008. These figures include such workers as clinical-practice
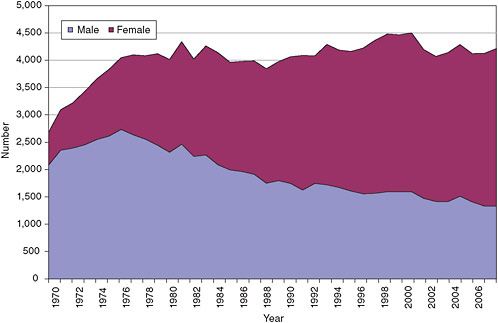
FIGURE 4-4 Doctorates in the behavioral sciences.
SOURCE: NSF, 2008. Survey of Earned Doctorates, 2008. Washington, DC: NSF.
TABLE 4-3 Average Median Time to Degree for the Doctorates 2004 to 2006 in the Behavioral and Social Sciences as Reported for the Research-Doctorate Study
|
Field |
Full- and Part-Time Students |
Full-Time Students |
|
Anthropology |
7.85 |
7.16 |
|
Psychology |
5.82 |
5.79 |
|
Sociology |
6.69 |
6.15 |
|
Total |
6.43 |
6.13 |
|
SOURCE: NRC. 2010. A Data-Based Assessment of Research-Doctorate |
||
Programs. Washington, DC: The National Academies Press. trainees in psychology and industry-employed trainees in the various behavioral and social sciences, which may have biased the data on the time to degree.
POSTDOCTORAL TRAINING
Between 1970 and 2008, the fraction of Ph.D.s in the behavioral and social sciences who were planning on a postdoctoral position increased from 223, or 11 percent of all Ph.D.s in the field, to 1,108, or 46 percent. Not surprisingly, females now make up about three-quarters of all Ph.D.s planning such additional training. In an earlier section, we offered a number of reasons for including clinical psychology in the behavioral and social sciences taxonomy. Another reason is the increased participation in postdoctoral training by individuals with degrees in clinical psychology (Figure 4-5). The fact that the proportion of Ph.D.s in the behavioral and social sciences who plan postdoctoral training increased from 20 percent in 1990 to nearly 50 percent in 2008 points to its importance in their career plans.
The large and increasing number of female Ph.D.s and females seeking postdoctoral training, as well as the increase in dual-career couples, suggests that the behavioral and social sciences may be a leading indicator of the need for employers to accommodate the work-life realities of the current generation of both women and men. Otherwise, training will be adversely affected by withdrawals of significant numbers of well-trained researchers—both male and female—for such purposes as child rearing. Afterwards, the rapid advances of science may make it difficult for such trained researchers to return to the workforce.
One positive trend is the increase in minorities with Ph.D.s. In the 1970s only 1 or 2 percent of the doctorates went to minorities, but that has changed, and in 2007 almost 15 percent of the doctorates were awarded to minorities (see Figure 4-6). Although this percentage is slightly higher than in the biomedical sciences, it needs to be higher still if the percentage of minority researchers is to more closely reflect the percentages of minorities in both the serving and served populations. Increasing the percentage of minority researchers will, of course, require an increased fraction of minorities in the B.S. degree pool.
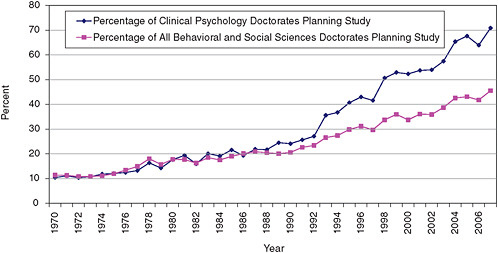
FIGURE 4-5 Postdoctoral plans for clinical psychology and all behavioral and social science doctorates.
SOURCE: NSF. 2008. Survey of Earned Doctorates, 2008. Washington, DC: NSF.
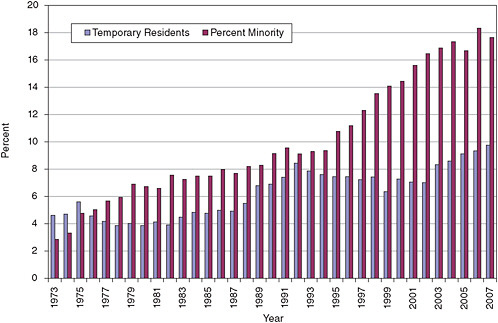
FIGURE 4-6 Percentage of the behavioral and social sciences doctorates by citizenship and race/ethnicity.
SOURCE: NSF. 2008. Survey of Earned Doctorates, 2008. Washington, DC: NSF. The pattern of increasing numbers of Ph.D.s in the
biomedical sciences going to researchers with temporary resident status is not apparent in the behavioral and social sciences. There was an increase in temporary resident Ph.D.s in these fields in the 1980s, but the proportion has remained about the same—8 to 10 percent—since that time.
Postdoctoral Appointments
Figure 4-7 shows the number of postdoctoral appointments by employment sector in the period 1973-2008; all sectors show a pattern of increases since 1991. The number of appointments has varied somewhat in recent years in the aca-
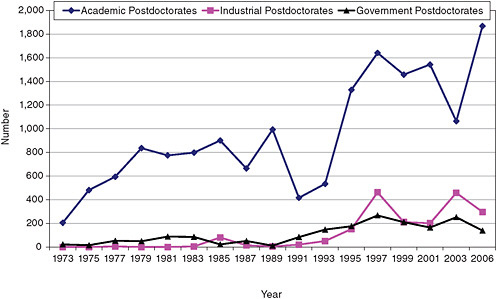
FIGURE 4-7 Postdoctoral appointments in the behavioral sciences.
SOURCE: NSF. Survey of Doctorate Recipients, 1973-2006. Washington, DC: NSF. demic and industrial sectors. The academic sector accounts for
three-quarters of the appointments, but there is growing participation in the industrial sector. A notable difference between the biomedical and the behavioral and social sciences fields is the ratio of citizens and permanent resident postdoctorates to temporary resident postdoctorates in academic institutions. Because the fraction of temporary resident Ph.D.s in the behavioral and social sciences is generally less than the fraction in the biomedical sciences, there are proportionally more citizens and permanent residents in postdoctoral positions in the behavioral and social sciences. The ratio in the biomedical sciences is 1.6 to 1, with more temporary residents, while in the behavioral and social sciences the ratio is 3.3 to 1, with more citizens and permanent residents. Looking at the overall behavioral and social sciences workforce, which approaches 90,000 individuals it is clear that the postdoctoral component is quite small, so clearly most did not seek additional postdoctoral training, although the number of postdoctorates is slowly increasing.
Table 4-4 shows the composition of postdoctoral positions in research doctorate programs in 2006. The total number is about half the number for all academic positions. Although females receive twice as many doctorates in the behavioral and social sciences as males, the number of males and females in postdoctoral positions are approximately the same.
EMPLOYMENT TRENDS
The behavioral and social sciences workforce has grown steadily from 27,356 in 1973 to a peak of 108,339 in 2006. Female Ph.D.s made up an increasingly large fraction of the total during these years (Figure 4-8). In 2006, they became the majority in the workforce.
The workplace distribution of the overall workforce is very different in the behavioral and social sciences than in the biomedical sciences (Figure 4-9). While academic employment is still the largest sector, industrial employment has grown at a rapid rate, and the non-profit or other sector
TABLE 4-4 Postdoctoral Appointments in Research Departments in the Behavioral and Social Sciences in 2006 as Reported for the Research-Doctorate Study
|
Field |
Male |
Female |
U.S. Citizen |
Permanent Resident |
Temporary |
Citizenship Unknown |
Total |
|
Anthropology |
50 |
53 |
60 |
6 |
33 |
4 |
107 |
|
Psychology |
438 |
480 |
565 |
37 |
255 |
60 |
944 |
|
Sociology |
27 |
36 |
45 |
1 |
9 |
9 |
67 |
|
Total |
515 |
569 |
670 |
44 |
297 |
73 |
1118 |
|
SOURCE: NRC. 2010. A Data-Based Assessment of Research-Doctorate Programs. Washington, DC: The National Academies Press. |
|||||||
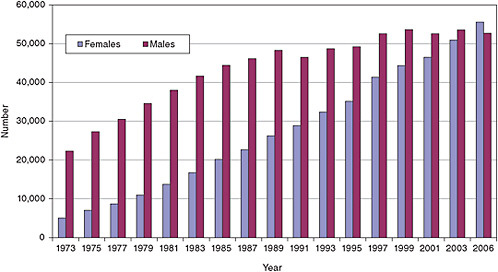
FIGURE 4-8 Distribution of behavioral and social scientists in the workforce by gender.
SOURCE: NSF. Survey of Doctorate Recipients, 1973-2006. Washington, DC: NSF.
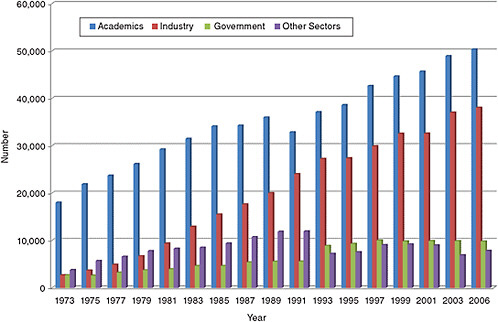
FIGURE 4-9 Employment sectors in the behavioral and social sciences.
SOURCE: NSF. Survey of Doctorate Recipients, 1973-2006. Washington, DC: NSF.
is comparatively larger than in the biomedical sciences. The overall workforce in the behavioral and social sciences is almost as large as in the biomedical sciences.
In 1985, the age distribution for the workforce, excluding postdoctoral appointees, was similar for the behavioral and the biomedical sciences, but by 2006, the median age in the behavioral and social science workforce was 2.5 years greater than in biomedical sciences (Table 4-5). Another way to look at the aging of the behavioral workforce is to compare the age distribution over time. There may be significant retirement in the next 10 years from the 51 to 76 age group, although, as noted previously, the concern for retirement portfolios and the improving health of older faculty may affect such a projection. (Figure 4-10; also see projections in Appendix D and E).
DETAILS OF ACADEMIC EMPLOYMENT
Academic employment in the behavioral and social sciences increased by more than 50 percent from 1973 to 2001, after which there has been a slow decline. However, much of the growth has been in non-tenure positions and in “other” academic categories, and by 1999 these categories represented about a third of the academic staff. These contingent faculty (adjunct, lecturer, and part-time staff) are disproportionately female, often involved exclusively in teaching, under-paid, without benefits, contract-vulnerable, and not necessarily involved in research. Data from the Research-Doctorate Study also show that females are underrepresented on the faculty of research departments (see Figure 4-11). While females were in faculty positions at a rate consistent with the proportion of Ph.D.s in the 1970s and early 1980s,
TABLE 4-5 Median Age Cohort for the Biomedical Sciences and the Behavioral and Social Sciences
|
|
Median Age in 1993 |
Median Age in 2006 |
|
Biomedical Sciences |
48.9 |
52.3 |
|
Behavioral and Social Sciences |
49.8 |
55.4 |
|
SOURCE: NSF. Survey of Doctorate Recipients, 1973-2006. Washington, DC: NSF. |
||
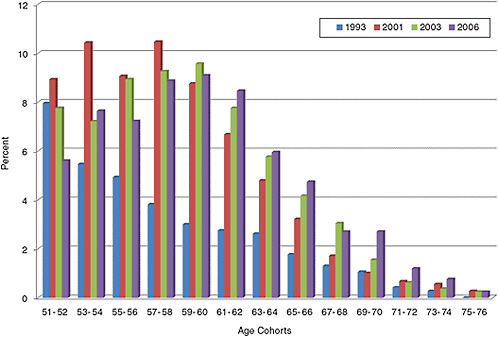
FIGURE 4-10 Age distribution of tenured behavioral and social sciences faculty.
SOURCE: NSF. Survey of Doctorate Recipients, 1973-2006. Washington, DC: NSF.
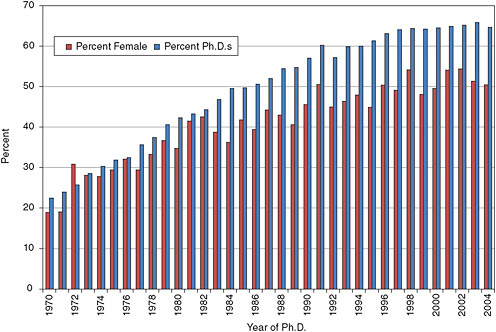
FIGURE 4-11 Percentage of female faculty in 2006 in the behavioral and social sciences by year of Ph.D. compared with the number of Ph.D.s in the same year.
SOURCE: NRC. 2010. A Data-Based Assessment of Research-Doctorate Programs. Washington, DC: The National Academies Press.
females in recent years are not in faculty positions in proportion to the number of Ph.D.s.
In contrast, the size of the tenured and tenure-track staff has been almost constant since the early 1990s (Figure 4-12). Over the past 10 years, as mentioned above, two-thirds of doctorates have been awarded to women, and this is reflected in academic appointments with about 60 percent of the combined tenure-track, non-tenured and other academic positions being held by women (Figure 4-13). However, women are over-represented in the combined “non-tenured and other” tracks. Those in tenured positions now make up 40 percent of the academic workforce, which is below their 53 percent representation in the academic workforce. Over time, however, this should change as more women in tenure-track positions receive tenure.
The number of underrepresented minorities in the behavioral and social sciences workforce has increased dramatically in the past several decades, from 520 in 1975 to 8,960 in 2006. For a number of years the number of minorities in the workforce has grown at a substantially greater rate than the total workforce.
RESEARCH TRAINING AND THE NATIONAL RESEARCH SERVICE AWARD PROGRAM
In general, the National Research Service Award (NRSA) program plays a smaller role in research training in the behavioral and social sciences than in the basic biomedical fields. The number of awards in the behavioral and social sciences as displayed in Table 4-6 are about one-tenth of those in the biomedical sciences. About 1 percent of the 26,600 graduate students in the behavioral and social sciences in 2008 had an individual NRSA, as compared with 9.3 percent in the biomedical sciences. It has been argued that much of the research in the behavioral and social sciences is not health related, but an analysis done during the 2005 NRSA study showed that 90 percent of the reviewed dissertation abstracts of behavioral and social sciences Ph.D.s were considered fundable by NIH personnel.
Since NIH has historically tended to focus on research that relates to the physical structure of the body and hence to fields in the biomedical and clinical sciences, the behavioral and social sciences have received less research and training support. This may also be seen in the fact that the NIH does not have an institute or center with the mission devoted to the support of basic and applied research in the behavioral and social sciences. Research training exists in institutes with other missions, such as NIMH, NIA, the National Institute on Drug Abuse, the National Institute on Alcohol Abuse and Alcoholism, and the National Cancer Institute, but it has decreased in recent years, as can be seen in Table 4-6. Even within the institutes that support training in the behavioral and social sciences, such training is directed at particular
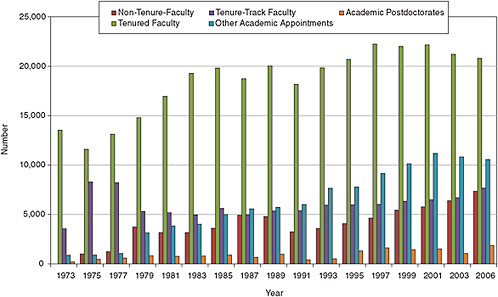
FIGURE 4-12 Academic employment in the behavioral and social sciences.
SOURCE: NSF. Survey of Doctorate Recipients, 1973-2006. Washington, DC: NSF.
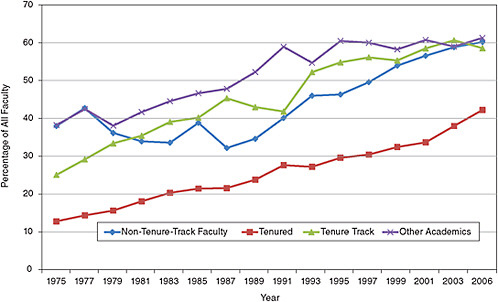
FIGURE 4-13 Female faculty positions in the behavioral and social sciences.
SOURCE: NSF. Survey of Doctorate Recipients, 1973-2006. Washington, DC: NSF.
TABLE 4-6 NRSA Trainees and Fellows, by Broad Field (Behavioral and Social Sciences), 1975-2008, Fiscal Year (Percentages are based on total NRSA funding at the NIH by mechanism)
|
|
Predoctoral |
Postdoctoral |
Both |
|||||||
|
|
Trainees |
% |
Fellowship |
% |
Trainees |
% |
Fellowship |
% |
Total |
Total % |
|
1975 |
208 |
16.2 |
125 |
80.6 |
32 |
3.8 |
146 |
10.0 |
511 |
13.6 |
|
1980 |
655 |
12.8 |
74 |
76.3 |
368 |
9.2 |
131 |
5.5 |
1228 |
10.6 |
|
1985 |
501 |
10.2 |
41 |
31.5 |
392 |
9.2 |
86 |
4.6 |
1020 |
9.2 |
|
1990 |
619 |
10.8 |
58 |
17.3 |
398 |
10.1 |
78 |
4.7 |
1153 |
9.9 |
|
1995 |
505 |
7.8 |
101 |
16.2 |
411 |
9.9 |
112 |
6.0 |
1129 |
8.6 |
|
2000 |
451 |
8.0 |
207 |
28.0 |
465 |
11.0 |
114 |
6.3 |
1237 |
10.0 |
|
2005 |
506 |
8.4 |
214 |
16.7 |
460 |
9.2 |
104 |
6.4 |
1284 |
9.2 |
|
2006 |
522 |
9.2 |
183 |
13.4 |
401 |
8.3 |
77 |
4.9 |
1183 |
8.8 |
|
2007 |
421 |
6.9 |
154 |
10.6 |
350 |
7.5 |
50 |
3.4 |
975 |
7.1 |
|
2008 |
416 |
6.3 |
147 |
9.6 |
301 |
6.3 |
50 |
3.4 |
914 |
6.3 |
|
SOURCE: NIH database. |
||||||||||
subfields and often does not require the interdisciplinary or multidisciplinary character of the training grants in the biomedical or clinical sciences.
Efforts are being made by the Office of Behavioral and Social Science Research (OBSSR) to foster interdisciplinarity by bringing together the biomedical, behavioral, and social sciences communities to work collaboratively to solve complex pressing health challenges. OBSSR is leading efforts in: biopsychosocial interactions, community-based participation research, systems science, genes, behavior and environment, social and cultural factors in health, health and behavior, and translational research. However, the office does not have the resources to support training in these areas and must depend on other institutes. In recent years NIGMS has increased its funding in the behavioral and social sciences but it does not have the resources to carry out the mission outlined by OBSSR.
As was shown earlier in Figure 4-2, less than a quarter of the graduate student population in the behavioral and social sciences in doctoral-granting institutions who have some type of support are supported on fellowships, traineeships, and research grants. Of this support it is generally thought that the National Science Foundation (NSF) provides a large portion of this support, but in reality, the support from NSF is only about a tenth of the total federal support and a third of the support provided by NIH (Figure 4-14). These data also show a decline in support by NIH and NSF in 2008.
It should also be noted that total graduate support declined in the 1980s, and the increase back to the earlier level is due mainly to NIH and other federal agency support. Much of the early decline was caused by reductions in the non-NIH part of the Department of Health and Human Services (HHS). By 2006, NIH research grants formed more than two-thirds of the support (Figure 4-15), which was a major shift from the early 1980s when the major source of support came from traineeships.
As is the case at the predoctoral level, NRSA support of postdoctoral training in the behavioral and social sciences is a fraction (between 10 and 15 percent) of that in the biomedical sciences (see Table 4-2). There are no data on the general postdoctoral support from NIH, but the picture for postdoctoral training support from all federal sources shows a growth in research grant support and a decline in trainee and fellowship support until 1990, with essentially constant support thereafter. The NIH’s efforts in the late 1970s and 1980s to shift research training in the behavioral and social sciences from the predoctoral to the postdoctoral level can be seen by comparing the level of predoctoral support in Figure 4-15.
RECOMMENDATIONS
Recommendation 4–1: Training programs in basic behavioral and social sciences that cut across disease and age categories should be housed at NIGMS consistent with the NIGMS congressional mandate. Given its disciplinary expertise, OBSSR should cooperate in this effort. NIGMS needs funds and appropriate staff dedicated to this new effort.
Recommendation 4–2: Training programs in basic behavioral and social sciences that bear specifically on particular diseases and age cohorts should be housed in all the relevant institutes and centers. Both basic and translational research training can be specific to institutes and centers. Given both its disciplinary expertise and its role in connecting institutes and centers, OBSSR should cooperate in this effort.
Recommendation 4–3: The target numbers to be trained in OBBSR should increase back to the 2004 baseline. In the case that an infusion of funds results from current
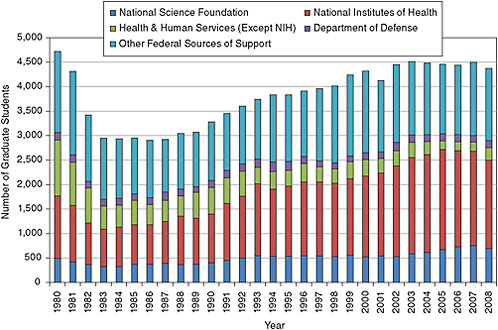
FIGURE 4-14 Federal sources of support in the behavioral and social sciences.
SOURCE: NSF. 2008. Survey of Graduate Students and Postdoctorates in Science and Engineering. Washington, DC: NSF.
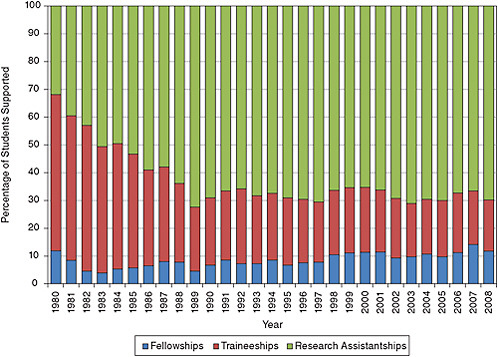
FIGURE 4-15 Types of support from the NIH in the behavioral and social sciences.
SOURCE: NSF. 2008. Survey of Graduate Students and Postdoctorates in Science and Engineering. Washington, DC: NSF.
federal health initiatives, the targets should increase to reflect the new positions that will open as a result. Future adjustments should be closely linked to the total extramural research funding in the biomedical, clinical, and behavioral sciences.
Bringing the level of support in the behavioral and social sciences in 2008 up to the level in 2004 will require the addition of about 370 training slots at a cost of about $15 million. Also, in recommending linking the number of NRSA positions to extramural research funding, the committee realizes that a decline in extramural research would also call for a decline in training.
Recommendation 4–4: All institutes are encouraged to make F30 fellowships accessible to qualified M.D./Ph.D. students. The F30 program should also be extended to clinical behavioral scientists in M.D./Ph.D. programs.
The F30 awards have proven to be a good way for students in M.D./Ph.D. programs to gain NIH support for their activities. They also provides a means of support for students at institutions that do not have an MSTP. Unfortunately this fellowship is not awarded by all NIH institutes, which restricts its overall value.
















