

14 Radon Toxicity
|
Environmental ALERT …
|
This monograph is one in a series of self-instructional publications designed to increase the primary care provider’s knowledge of hazardous substances in the environment and to aid in the evaluation of potentially exposed patients. See pages 21 to 23 for further information about continuing medical education credits and continuing education units.
|
Guest Contributor: |
Mark Upfal, MD, MPH |
|
Guest Editor: |
Jonathan M.Samet, MD |
|
Peer Reviewers: |
Charles Becker, MD; Jonathan Borak, MD; Joseph Cannella, MD; Bernard Goldstein, MD; Alan Hall, MD; Richard J.Jackson, MD, MPH; Jonathan Rodnick, MD; Linda Rosenstock, MD, MPH; Robert Wheater, MS; Brian A.Wummer, MD |

U.S. DEPARTMENT OF HEALTH & HUMAN SERVICES
Public Health Service
Agency for Toxic Substances and Disease Registry
Case Study
Chronic cough and weight loss in a nonsmoking 56-year-old woman
A 56-year-old housewife seen at your office has a 3-month history of chronic, nonproductive cough, which has recently become unresponsive to over-the-counter liquid cough suppressants. She denies having shortness of breath, wheezing, chest pain, hemoptysis, fever, chills, sore throat, hoarseness, or postnasal drip. Her cough is independent of time of day, physical activity, weather conditions, and exposure to dust or household cleaning agents. Furthermore, her daughter’s cigarette smoke does not seem to aggravate the cough. She notes that she has been feeling fatigued and, without dieting, has lost 18 pounds over the past 6 months.
Her past medical history is noncontributory. She is a nonsmoker and nondrinker and does not come in contact with any known chemical substances or irritants other than typical household cleaning agents. Her father died at age 65 of a myocardial infarction, and her mother had breast cancer at age 71. Her first husband died of a cerebrovascular accident 3 years ago. Newly remarried to a retired shipyard worker, she and her current husband live with her 28-year-old daughter and 9-year-old grandson in their New Hampshire home. She has not been outside the New England area for the last 5 years.
Results of the physical examination, including HEENT and chest examination, were normal. There is no cyanosis or clubbing of the extremities, and there are no palpable lymph nodes. Blood tests, including a complete blood count and chemistry panel, are normal, with the exception of a total serum calcium level of 12.7 mg/dL (normal range: 9.2 to 11.0 mg/dL). However, a chest radiograph reveals a noncalcified, noncavitary 3.5-cm mass located within the parenchyma adjacent to the right hilum. There are no other radiographic abnormalities. Results of a PPD skin test for tuberculosis are negative. Urinalysis results are normal.
![]()
(a) What is the differential diagnosis for this woman’s condition?
_________________________________________________________________
(b) What further testing might you order?
_________________________________________________________________
(c) List several environmental causes that have been associated with this patient’s probable disorder.
_________________________________________________________________
(d) What treatment options might you consider?
_________________________________________________________________
Answers can be found on page 18.
Exposure Pathways
Sources of Radon Exposure
❑ Radon, a colorless, odorless gas, is both chemically inert and imperceptible; it decays into a series of progeny, some of which are short-lived and emit bursts of harmful alpha particles.
❑ Soil is the main source of indoor radon; however, building materials and water supply can also be sources.
Radon gas is derived from the radioactive decay of radium, a ubiquitous element found in rock and soil. The decay series begins with uranium-238 and goes through four intermediates to form radium-226, which has a half-life of 1600 years. Radium-226 then decays to form radon-222 gas. Radon’s half-life, 3.8 days, provides sufficient time for it to diffuse through soil and into homes, where further disintegration produces the more chemically and radiologically active radon progeny (“radon daughters”). These radon progeny, which include four isotopes with half-lives of less than 30 minutes, are the major source of human exposure to alpha radiation (high-energy, high-mass particles, each consisting of two protons and two neutrons). This alpha radiation is responsible for cellular transformation in the respiratory tract, which results in radon-induced lung cancer.
Radon itself is imperceptible by odor, taste, and color, and causes no symptoms of irritation or discomfort. There are no early signs of exposure. Only by measuring actual radon levels can persons know whether they are being exposed to excessive levels of radon gas. Radon seeps from the soil into buildings primarily through sump holes, dirt floors, floor drains, cinder-block walls, and through cracks in foundations and concrete floors (Figure 1). When trapped indoors, radon can become concentrated to dangerous levels. When radon escapes from the soil to the outdoor air, it is diluted to levels that offer relatively little health risk.
Radon gas can enter a building by diffusion, but pressure-driven flow is a more important mechanism. Negative pressure in the home relative to the soil is caused by exhaust fans (kitchen and bathroom), and by rising warm air created by fireplaces, clothes dryers, and furnaces. In addition to pressure differences, the type of building foundation can affect radon entry. Basements allow more opportunity for soil gas entry, but slab-on-grade foundations (no basement) allow for less. In most cases, the slight increase of indoor radon due to home “tightening” for energy conservation is small in comparison with the amount of radon coming from the soil.
❑ Although slab-on-grade foundations allow for less soil gas entry than do basements, both types of foundations could permit entry of radon.
Normally, construction materials do not contribute significantly to indoor radon levels. In rare cases, however, building materials themselves have been the main source of radioactive gas. Building materials contaminated with vanadium mill tailings in Monticello, Utah, and uranium mill tailings in Grand Junction, Colorado, were an important source of radon. (Tailings consist of the sand-like material remaining after minerals are removed from ore.) Also, concrete made from phosphate slag in Idaho and Montana and insulation from radium-containing phosphate waste from the state of Washington have been found to emit high levels of radon.
Figure 1. Sources of radon and common entry points
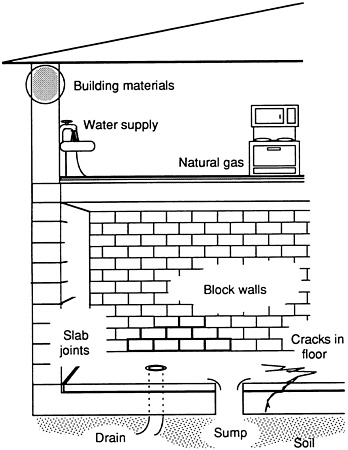
Radon may be carried into some homes via the water supply. With municipal water or surface reservoirs, most of the radon volatilizes to air or decays before the water reaches homes. However, water from private wells may be another matter. Groundwater that comes from deep subterranean sources and passes over rock rich in radium, such as that found in northern New England, may dissolve some of the radon gas produced from radium decay. As the water splashes during showering, toilet flushing, dishwashing, and laundering, radon is released into the air and may result in inhalation exposure. Radon may also be present in natural gas supplies.
|
(1) Additional information for the case study: Your local newspaper recently featured an article on radon and urged that all homes in your community be tested. Your patient tests her home and finds the living space averages 35 picocuries per liter (pCi/L). Discuss how construction of the patient’s house can affect this level. _________________________________________________________________ _________________________________________________________________ _________________________________________________________________ |
Hazard Assessment
Respiratory Dose and Units of Measure
❑ Radon can be detected only by testing.
Since the health effects of radon are insidious and have a long latency period, it is important to measure exposure to the gas empirically. Techniques for measuring radon are discussed below, in the subsection entitled Radon Detection (p. 11). Included here is a review of the basic unit of radon measurement and the factors that affect the risk associated with radon exposure.
The relationship between exposure to radon and the dose of decay products that reaches target cells in the respiratory tract is complex. Some factors that influence the pulmonary radiation dose include the following:
❑ EPA recommends remediation for homes with radon levels at or above 4 pCi/L.
characteristics of the inhaled air—free or unattached radon progeny deposit more efficiently than progeny attached to dust or other particles; of the attached progeny, only those adhering to the smallest particles are likely to reach the bronchi
amount of air inhaled—the amount and deposition of inhaled radon decay products vary with the flow rate in each airway segment
breathing pattern—the proportion of oral to nasal breathing will affect the number of particles reaching the airways
architecture of the lungs—sizes and branching pattern of the airways affect deposition; these patterns may differ between children and adults, and between males and females
biologic characteristics of the lungs—the dose increases as the mucociliary clearance slows and diminishes with increasing thickness of the mucous layer
It is possible, therefore, that two environments with the same radon measurement (e.g., a dusty mine and a home environment) may deliver different doses of alpha radiation to a person’s lungs. Likewise, two persons in the same environment may receive differing doses of alpha radiation to the target cells of their lungs because of differing breathing patterns and pulmonary architecture.
The concentration of various progeny is ultimately related to lung injury and thus might be the most appropriate measure of respiratory exposure. On the basis of both animal and human data, it can be assumed, however, that the higher the radon level a person experiences, the more likely it is that the person will develop lung cancer. For convenience, indoor air measurements, therefore, usually measure radon gas itself. These measurements are expressed in picocuries per liter (pCi/L) of air, where a picocurie is equivalent to 0.037 disintegrations per second. The U.S. Environmental Protection Agency (EPA) has recommended that remedial action be taken to lower the amount of radon in homes if the measured level is 4 pCi/L or greater.
Risk Estimates
❑ For a lifetime exposure at EPA’s recommended guideline of 4 pCi/L, EPA estimates that the risk of developing lung cancer is 1% to 5%, depending on whether a person is a smoker, former smoker, or nonsmoker.
Even conservative estimates based on current knowledge suggest that radon is one of the most important environmental causes of death. EPA estimates that approximately 14,000 deaths annually in the United States are due to lung cancer caused by indoor radon exposure. It has also been estimated that approximately 14% of all current cases of lung cancer are attributable to radon.
For a lifetime exposure to radon at 4 pCi/L, EPA estimates that the risk of developing lung cancer is 1% to 5%. The National Research Council estimates the risk at 0.8% to 1.4%.
❑ The overall risk of radon exposure is related not only to its level in the home, but also to the occupants and their lifestyles.
Many factors influence the risk of lung cancer due to radon exposure; among these are age, duration of exposure, time since initiation of exposure, and cigarette smoking (Figure 2). In assessing the risk of radon in a home, one must consider not only the level of radon, but also the occupants and their lifestyles. Are there any smokers? Any children? How much time is spent in the home? Where do occupants sleep? The highest radon levels are typically found in the lowest level of the house. If well water is the major source of radon, upper floors can be affected more than lower floors. In colder climates, radon levels are often higher in the winter and lower in the summer.
Figure 2. Radon risk evaluation chart
RADON RISK IF YOU SMOKE
RADON RISK IF YOU’VE NEVER SMOKED
Who’s at Risk
❑ Miners in uranium and other types of underground mines may have increased radon exposure.
❑ Approximately 6 million homes in the United States have radon levels above 4 pCi/L.
❑ Exposure to excessive radon levels increases the already elevated risk of lung cancer for smokers.
As early as the 16th century, Paracelsus and Agricola described a wasting disease of miners. In 1879, this condition was identified as lung cancer by Herting and Hesse in their investigation of miners from Schneeberg, Germany. Radon itself was discovered some 20 years later by Rutherford. Subsequently, an increase in the incidence of lung cancer among miners was linked to radon exposure in mines. Underground uranium mines found throughout the world, including the western United States and Canada, pose the greatest risk because of their high concentration of radon. Iron ore, potash, tin, fluorspar, gold, zinc, and lead mines also have been found to have significant levels of radon, often due to radium in the surrounding rock. In the past, it was not uncommon to use the tailings from these mines as fill on which to build homes, schools, and other structures.
Indoor radon has been widely recognized as a potential problem in Europe and the Scandinavian countries since the 1970s. Public awareness in the United States was heightened in December 1984, when Stanley Watras, a worker at the Limerick nuclear plant in Pennsylvania, began setting off radiation alarms when he entered the plant. The cause was traced to excessive radon levels in his home, which were found to be 500 times the level at which EPA currently recommends remediation (4 pCi/L).
In 1987, the federal government allotted $10 million to the states to determine the extent of radon contamination in homes and schools and subsequently amended the Toxic Substances Control Act to assist the states “in responding to the threat to human health posed by exposure to radon.” In 1988, EPA and the Office of the Surgeon General jointly recommended that all U.S. homes below the third floor be tested for radon. In 1990, Congress appropriated $8.7 million for grants to states to develop and enhance programs to reduce radon risk in homes and schools. It has become standard practice in some states to measure radon levels in homes at the time of real estate transactions.
The amount of radon emanating from the earth and concentrating inside homes varies considerably by region and locality. Nearly every state in the United States has dwellings with measured radon levels above acceptable limits. EPA estimates that 6% of American homes (approximately 6 million) have concentrations of radon above 4 pCi/L. In Clinton, New Jersey, near a geologic formation high in radium called the Reading Prong, all 105 homes tested were above the recommended guidelines; 40 had levels exceeding 200 pCi/L. In the Stanley Watras home, levels of 2700 pCi/L were found in the basement.
Areas of the country that are likely to have homes with elevated radon levels are those with significant deposits of granite, uranium, shale, and phosphate—all high in radium content and, therefore, potential sources of radon gas. Some homes in these areas, however, may not have elevated levels of radon. Due to the many determinants of indoor radon levels, local geology alone is an inadequate predictor of risk.
Currently, the only way to determine indoor radon concentration is by testing. A home located 100 feet away from the Watras’ home did not have measured radon concentrations that required remediation, yet both houses are located on the same geologic formation. Other factors found to predispose homes to elevated levels of radon include soil porosity, foundation type, location, building materials used, entry points for soil gas, building ventilation rates, and source of water supply. Further research is being conducted on ways to predict which homes are most likely to have significant levels of radon.
Several studies have shown that smokers exposed to radon are at greater risk for lung cancer than nonsmokers similarly exposed. It is generally believed that exposure to radon and cigarette smoking are synergistic; that is, the combined effect exceeds the sum of their independent effects. The risk of lung cancer from radon exposure is estimated to be 10 to 20 times greater for persons who smoke cigarettes in comparison with those who have never smoked. According to the EPA Office of Radiation Programs, a breakdown of the contribution of smoking and radon exposure to lung cancer deaths in the United States illustrates that of every 100 persons who have died of lung cancer, approximately 70 were current smokers, 24 were former smokers, and 6 had never smoked. It is estimated that radon contributed to 20% of the deaths in each category.
Data on the effects of radiation in children are limited, and even less is known about the effects of radon exposure in this age group. Cancer development in Japanese atomic bomb survivors suggests an increased susceptibility to radiation in children compared with that in adults. Children also have different lung architecture, resulting in a somewhat more concentrated dose of radiation to the respiratory tract, and children have a longer latency period ahead of them in which to develop cancer. However, there are currently no conclusive data on whether children are at greater risk than adults from radon.
|
(2) Who else in the home of the patient discussed in the case study could be at risk for lung cancer as a result of elevated radon levels? _________________________________________________________________ _________________________________________________________________ (3) Would your patient’s neighbors be equally at risk of exposure to radon? Explain. _________________________________________________________________ _________________________________________________________________ (4) How are the risks of radon exposure increased for your patient’s daughter, who is a smoker? How does the daughter’s smoking affect the risk for other members of the family? _________________________________________________________________ _________________________________________________________________ |
Physiologic Effects
❑ The primary adverse health effect of exposure to radon is lung cancer.
❑ The synergistic mechanism(s) of cigarette smoking and radon exposure are not known, although the adverse health effects of the combination are clear.
Radon exposure causes no acute or subacute health effects, no irritating effects, and has no warning signs at levels normally encountered in the environment. The only established human health effect currently associated with residential radon exposure is lung cancer. Epidemiologic studies of miner cohorts have reported an increased frequency of chronic, nonmalignant lung diseases such as emphysema, pulmonary fibrosis, and chronic interstitial pneumonia, all of which increased with increasing cumulative exposure to radiation and with cigarette smoking.
Epidemiologic studies and a recent study of groundwater radon and cancer mortality have found no association with extrapulmonary cancers, such as leukemias and gastrointestinal cancers. There is also no evidence that environmental radon exposure is causally associated with adverse reproductive effects.
❑ Radon progeny can be inhaled either as free particles or attached to dust. Free progeny preferentially deposit in the bronchi, the site of most lung cancers.
Due to their charged state and solid nature, radon progeny rapidly attach to most surfaces they encounter, including walls, floors, and airborne particulates. They can be inhaled, therefore, either as free, unattached particles or attached to airborne dust. The smaller dust particles can deposit the radon progeny deep in the lungs. Being ionized, the progeny tend to attach to the respiratory epithelium. Through mucociliary action, the progeny are eventually cleared from the respiratory tract, but because of their short half-life, they can release alpha particles before being removed. The total amount of energy deposited by the progeny is approximately 500 times that produced in the initial decay of radon. When these emissions occur within the lungs, the genetic material of cells lining the airways can be damaged, resulting in lung cancer.
The risk of lung cancer due to radon exposure is thought to be second only to that of smoking. The synergism between cigarette smoking and radon places the large population of current and former smokers at particularly high risk for lung cancer. Although the net consequence of cigarette smoking and exposure to radon decay products has been clearly demonstrated in smokers, the mechanism of interaction is still unclear.
Most of the lung cancers associated with radon are bronchogenic, with all histologic types represented. However, small cell carcinoma occurs at a higher frequency among both smoking and nonsmoking populations of underground miners in the initial years following exposure compared with the pattern of histologic types in the general population. Other types of lung cancers seen in radon-exposed miners are squamous cell carcinoma, adenocarcinoma, and large cell carcinoma.
|
(5) If the patient’s daughter described in the case study were pregnant, would the fetus be at risk from maternal exposure to airborne radon? _________________________________________________________________ (6) The patient’s husband developed mesothelioma as a result of asbestos exposure when he worked in the shipyards. What might have been the role of radon in the development of this condition? _________________________________________________________________ |
Treatment and Management
❑ Generally, the most effective methods to reduce the risk of lung cancer are smoking cessation and radon mitigation.
❑ The risk of cancer due to radon is often underestimated by the public; this bias may discourage assessment and abatement measures in the home.
Currently, no effective communitywide screening methods are available for medical prevention or early diagnosis and treatment of lung cancer (radon-induced or otherwise). Routine chest radiographs and sputum cytology are ineffective for lung cancer screening associated with cigarette smoking and would presumably be ineffective for lung cancer associated with radon as well. The most effective methods of prevention are reduction of radon exposure and modification of other simultaneous risk factors for lung cancer, such as smoking. Smoking cessation coupled with detection and mitigation of high radon levels is currently the only long-term solution for reducing the risk of lung cancer.
Several studies have noted optimistic biases in the public’s assessment of the risk due to radon. A New Jersey study found that this bias may discourage testing and subsequent implementation of control measures. In Maine, homeowners were found to greatly underestimate the risk, and abatement behavior was not significantly related to the actual risk.
Primary care physicians and public health professionals should promote public awareness so that the radon problem is seen in the proper perspective, leading to appropriate mitigation action when indicated. Physicians and public health officials should therefore test their own homes to relate their experience to others and to provide guidance on how to carry out the testing.
Radon Detection
❑ Radon levels cannot be predicted; they must be measured.
Radon levels cannot be accurately predicted solely on the basis of factors such as location, geology, home construction, and ventilation. A recent survey of Connecticut homes indicates that the age of the house and the presence of a cinder-block foundation have a statistically significant, positive correlation with radon levels. Measurement is the key to identifying the problem. Radon detection kits are available in most hardware stores.
Short-term testing (lasting a few days to several months) is the quickest way to determine if a potential problem exists. Charcoal canisters, charcoal liquid scintillation detectors, electret ion detectors, alpha-track detectors, and continuous monitors are currently the most common short-term testing devices. Short-term testing should be conducted in the lowest inhabited area of the home, with the doors and windows shut.
❑ The most common methods of radon measurement are charcoal canisters, charcoal liquid scintillation detectors, electret ion detectors, alpha-track detectors, and continuous monitors.
Long-term testing (lasting up to 1 year) will give a better reading of a home’s year-round average radon level than will a short-term test. Alpha-track detectors and electret ion detectors are the most common long-term testing devices. Exposed devices are sent via mail to a certified laboratory for analysis. These devices measure radon gas levels, rather than radon progeny; thus, the units reported are in picocuries of radon per liter of air (pCi/L).
The charcoal canister is a small can containing charcoal and a filter to keep out radon progeny. It is inexpensive ($10 to $25) and is generally used for short-term testing (3 to 7 days). The alpha-track device contains a small piece of plastic in a filtered container. As the radon gas that has entered the container decays, the alpha particles form etch tracks. These tracks can be counted using a special technique. The cost of the alpha-track device is roughly twice that of the charcoal canister, and it may be used to measure cumulative exposure over a longer period (several weeks to a year).
Radon Abatement
❑ The cost of remediation to reduce radon levels in the average home is about $1200.
❑ Available procedures to lower indoor radon levels are, dollar for dollar, very effective in saving lives.
❑ Subslab depressurization is one of the most effective methods of lowering radon levels in many homes.
How cost-effective is radon mitigation compared to other investments in health protection? The Swedish government plans to spend approximately $1000 per home reducing high radon levels, resulting in about $10,000 of cost per life spared. EPA estimates that the cost of remediation in most homes is less than $1500. The cost of radon testing and mitigation per life saved compares favorably with that of other government programs.
If excessive levels of indoor radon are found in a structure, low-cost, quick-fix methods should be implemented first. These include limiting the amount of time spent in contaminated areas and increasing ventilation. It is wise to consult with the state radiation protection office before implementing major abatement projects. Methods of reduction can be obtained from several sources listed in the Suggested Reading List and in the Sources of Information section.
Besides increasing ventilation, radon control measures include sealing the foundation, subslab depressurization (creating negative pressure in the soil), pressurizing the home, and using air-cleaning devices. Methods of increasing ventilation include opening windows, ventilating basements and crawl spaces, ventilating sumpholes and floor drains to the outside of the house, and increasing air movement with ceiling fans. Ventilation must be modified properly, however, since increased ventilation can depressurize the house in some cases, causing an increase of soil gas entry to the home. Heat exchangers provide away of bringing fresh air indoors without major heat loss, but these must be properly balanced or they can make the problem worse.
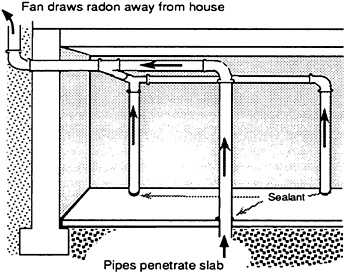
Preventing soil gas entry is more important than increasing whole-house ventilation. The former involves sealing the foundation and depressurizing the soil. Using vapor barriers around the foundation, sealing cracks and holes with epoxies and caulks, and sealing the crawl space from the rest of the house are all methods with some application. Subslab depressurization can reduce radon levels by as much as 99%. Suction puts the soil at a lower pressure than the inside of the home, preventing inward migration of soil gas. It involves sinking ventilation pipes below the foundation and continuously pumping out air (Figure 3). The cost to install subslab depressurization in an existing home is approximately $1000 to $2500 and about $100 annually for utility costs. The state radon office can be consulted to obtain a listing of radon mitigation contractors that have passed EPA’s Radon Contractor Proficiency (RCP) program (see page 17). If the equipment is installed during construction of the home, however, the cost of subslab depressurization is considerably less; it is much easier to install pipes during construction than to retrofit later. Physicians and other health professionals can perform a public service by becoming acquainted with local building codes and urging local jurisdictions to include the installation of capped pipes terminating in a space under the foundation to allow for later subslab depressurization if it is needed.
Figure 3. Subslab depressurization
|
(7) Where in your patient’s home should detectors be placed for radon screening? _________________________________________________________________ (8) What can you as a health professional do to decrease the risk of lung cancer among your patients? _________________________________________________________________ |
Standards and Regulations
❑ Currently, there are no enforceable regulations to control indoor radon levels, only guidelines and a national goal.
❑ The national goal is for indoor radon levels to be as low as those outdoors. About 0.4 pCi/L of radon is normally found in outside air.
Currently, no regulations mandate specific radon levels for indoor residential and school environments. There are only guidelines for remediation, such as the EPA recommendations and a national goal. EPA based its guidelines not only on risk considerations, but also on technical feasibility. There is thought to be no level at which the risk of exposure to alpha emitters is zero. An EPA drinking water standard is being developed. Many standards and guidelines for radon are currently being reviewed (Table 1), and changes may occur over time. EPA or state health departments should therefore be consulted for the most up-to-date standards.
Table 1. Standards and regulations for radon
|
Source* |
Focus |
Level |
Comments |
|
Indoor Radon Abatement Act |
Indoor air (residential) |
Indoor=outdoor (≈0.4 pCi/L) |
National goal |
|
NCRP |
Indoor air (residential) |
8 pCi/L |
Guideline |
|
EPA |
Indoor air (residential) |
4 pCi/L |
Current action level |
|
EPA |
Schools |
4 pCi/L† |
Guideline for action |
|
EPA |
Water |
Under development |
Proposal due 1993 |
|
NIOSH |
Occupational (mining) |
Advisory; exposure limit |
|
|
OSHA |
Occupational |
4 WLM§/yr |
Regulation |
|
MSHA |
Mining |
4 WLM§/yr |
Regulation |
|
*NCRP=National Council for Radon Protection; EPA=Environmental Protection Agency NIOSH=National Institute for Occupational Safety and Health; OSHA=Occupational Safety and Health Administration; MSHA=Mine Safety and Health Administration †EPA recommends action below 4 pCi/L in schools on a case-by-case basis §WLM=Working level month; a unit of measure commonly used in occupational environments (since WLM bears a complex relationship to pCi/L, physicians with responsibility for mine workers are urged to contact NIOSH or EPA for further information ¶ALARA=As low as reasonably achievable |
|||
In October 1988, the Indoor Radon Abatement Act was passed. This Act states that the “national long-term goal of the United States with respect to radon levels in buildings is that the air within buildings in the United States should be as free of radon as the ambient air outside of buildings.” The Act mandates that EPA update its publication, A Citizen’s Guide to Radon, and provide a series of action levels indicating the health risk associated with these various levels. The Guide will also provide information on the risk to sensitive populations, testing methods, and the cost and feasibility of mitigation techniques. Currently, EPA recommends remediation for homes and other buildings with levels above 4 pCi/L, with the caveat that corrective action be taken below this level on a case-by-case basis.
|
(9) Additional information for the case study: The local power company has offered free radon detection devices to all its customers. The average level of radon in the classrooms of your patient’s grandson is found to be 20 pCi/L. What is the community’s recourse to protect its children? _________________________________________________________________ _________________________________________________________________ _________________________________________________________________ |
Suggested Reading List
Anonymous. Standard procedures for radon measurement developed by the EPA. J Environ Health 1986;49:163–5.
Bierma TJ. Radon risk factors. J Environ Health 1989;51:277–81.
Council on Scientific Affairs. Radon in homes. JAMA 1987;258:668–72.
Kerr RA. Indoor radon: the deadliest pollutant. Science 1988;240:606–8.
National Research Council. Health risks of radon and other internally deposited alpha-emitters, BIER IV. Washington, DC: National Academy Press, 1988.
National Council on Radiation Protection and Measurements (NCRPM). Evaluation of occupational and environmental exposures to radon and radon daughters in the United States. Bethesda, Maryland: National Council on Radiation Protection and Measurement, 1984; NCRP report no. 78.
Nero AV, Schwehr MB, Nazaroff WW, Revzan KL. Distribution of airborne radon-222 concentrations in U.S. homes. Science 1986;234:992–7.
Nazaroff WW, Nero AV Jr, eds. Radon and its decay products in indoor air. New York: Wiley, 1988.
Lubin JH. Models for the analysis of radon-exposed populations. Yale J Biol Med 1988;61:195–214.
Health Effects
Harley N, Samet JM, Cross FT, Hess T, Muller J, Thomas D. Contribution of radon and radon daughters to respiratory cancer. Environ Health Perspect 1986;70:17–22.
Samet JM, Nero AV Jr. Sounding board: indoor radon and lung cancer. N Engl J Med 1989;320:591–4.
Related Government Documents
Centers for Disease Control. Radon progeny in underground mines. Atlanta: US Department of Health and Human Services, Public Health Service, 1987. Report no. (NIOSH) 88–101.
Centers for Disease Control. Radon exposure assessment—Connecticut. Atlanta: US Department of Health and Human Services, Public Health Service, MMWR 1989;38:713–5.
Centers for Disease Control. Lung cancer and exposure to radon in women—New Jersey. Atlanta: US Department of Health and Human Services, Public Health Service, MMWR 1989;38:715–8.
Centers for Disease Control. Health hazards associated with elevated levels of indoor radon—Pennsylvania. Atlanta: US Department of Health and Human Services, MMWR 1985;34:657–8.
Environmental Protection Agency. Radon reference manual. Washington, DC: US Environmental Protection Agency, Office of Radiation Programs, 1987. Report no. EPA 520/1–87–20.
Environmental Protection Agency. A citizen’s guide to radon: the guide to protecting yourself and your family from radon. 2nd ed. Washington, DC: US Environmental Protection Agency, Office of Air and Radiation, US Department of Health and Human Services, 1992. Report no. OPA-86–004 (to be revised).
Environmental Protection Agency. Radon reduction techniques for detached houses: technical guidance. 2nd ed. Washington, DC: US Environmental Protection Agency, Office of Research and Development, 1986. Report no. EPA 625/5–87/ 019.
Environmental Protection Agency. The national radon measurement proficiency (RMP) program: cumulative proficiency report. Washington, DC: US Environmental Protection Agency, Office of Radiation Programs. Report no. EPA 520/1– 88/024. (Published twice annually for various states, lists participating vendors of radon on detection equipment and services.)
Environmental Protection Agency. Radon measurements in schools: an interim report. Washington, DC: US Environmental Protection Agency, Office of Radiation Programs, 1989. Report no. EPA 520/1–89/010.
Environmental Protection Agency. Radon reduction methods: a homeowner’s guide. 3rd ed. Washington, DC: US Environmental Protection Agency, Office of Research and Development, 1989. Report no. OPA-89–005.
Environmental Protection Agency. Removal of radon from household water. Washington, DC: US Environmental Protection Agency, Office of Research and Development, 1987. Report no. OPA-87–011.
Public Health Service. The health consequences of smoking: cancer. A report of the Surgeon General. Washington, DC: US Department of Health and Human Services, Public Health Service, 1982. DHHS report no. (PHS) 82–50179.
Sources of Information
More information on the adverse effects of radon and the treatment and management of radon-exposed persons can be obtained from ATSDR, your state and local health departments, and university medical centers. Physicians and other health professionals may obtain materials from EPA for display. The federal EPA maintains an Office of Radiation Programs, 401 M Street SW, Washington, DC 20640, telephone (202) 260–9600.
Case Studies in Environmental Medicine: Radon Toxicity is one of a series. For other publications in this series, please use the order form on the back cover. For clinical inquiries, contact ATSDR, Division of Health Education, Office of the Director, at (404) 639–6204.
State Radon Contacts
Congress has mandated that each state set up an office to deal with requests for assistance.
ALABAMA
(800) 582–1866
ALASKA
(800) 478–4845
ARIZONA
(602) 255–4845
ARKANSAS
(501) 661–2301
CALIFORNIA
(800) 745–7236
COLORADO
(800) 846–3986
CONNECTICUT
(203) 566–3122
DELAWARE
(800) 554–4636
DISTRICT OF COLUMBIA
(202) 727–5728
FLORIDA
(800) 543–8279
GEORGIA
(800) 745–0037
HAWAII
(808) 586–4700
IDAHO
(800) 445–8647
ILLINOIS
(800) 325–1245
INDIANA
(800) 272–9723
IOWA
(800) 383–5992
KANSAS
(913) 296–1560
KENTUCKY
(502) 564–3700
LOUISIANA
(800) 256–2494
MAINE
(800) 232–0842
MARYLAND
(800) 872–3666
MASSACHUSETTS
(413) 586–7525
MICHIGAN
(517) 335–8190
MINNESOTA
(800) 798–9050
MISSISSIPPI
(800) 626–7739
MISSOURI
(800) 669–7236
MONTANA
(406) 444–3671
NEBRASKA
(800) 334–9491
NEVADA
(702) 687–5394
NEW HAMPSHIRE
(800) 852–3345 x4674
NEW JERSEY
(800) 648–0394
NEW MEXICO
(505) 827–4300
NEW YORK
(800) 458–1158
NORTH CAROLINA
(919) 571–4141
NORTH DAKOTA
(701) 221–5188
OHIO
(800) 523–4439
OKLAHOMA
(405) 271–5221
OREGON
(503) 731–4014
PENNSYLVANIA
(800) 237–2366
PUERTO RICO
(809) 767–3563
RHODE ISLAND
(401) 277–2438
SOUTH CAROLINA
(800) 768–0362
SOUTH DAKOTA
(605) 773–3351
TENNESSEE
(800) 232–1139
TEXAS
(512) 834–6688
UTAH
(801) 538–6734
VERMONT
(800) 640–0601
VIRGINIA
(800) 468–0138
WASHINGTON
(800) 323–9727
WEST VIRGINIA
(800) 922–1255
WISCONSIN
(608) 267–4795
WYOMING
(800) 458–5847
Answers to Pretest and Challenge Questions
Pretest
The Pretest questions are on page 1.
-
The differential diagnosis for the patient’s radiographic solitary pulmonary nodule would include
primary pulmonary malignancy
metastatic malignancy
granulomatous disease (for example, tuberculosis, coccidioidomycosis, histoplasmosis, nocardiosis)
AV malformation
pulmonary hamartoma
bronchial adenoma
pulmonary abscess
pseudonodule (e.g., nipple shadow, superficial skin lesion)
sarcoidosis
The following factors increase the likelihood of her having a pulmonary malignancy: radiographic appearance of the lesion (size and lack of calcification), age, symptoms of cough and weight loss, hypercalcemia, absence of residence in or travel to an area endemic for coccidioidomycosis (southwest United States) or histoplasmosis (Ohio/Mississippi Valley), absence of fever or evidence of infectious disease, and negative PPD skin test. The latter does not rule out tuberculosis but makes it less likely.
-
Initially, one or more of the following might be ordered:
search for previous chest radiographs for comparison
sputum studies for cytology and cultures (standard pathogens, fungus, acid-fast bacilli)
CAT scan
fiber-optic bronchoscopy with bronchial brushings and specimens for cytology and culture
Additional tests would follow, depending on results of these initial studies. If a primary lung cancer is detected, a metastatic workup (scans of the brain, liver, adrenals, and bones) may be indicated.
-
Environmental causes of lung cancer include
arsenic
asbestos
chloromethyl ethers
chromium
ionizing radiation (alpha, beta, gamma, or X-radiation)
nickel
polynuclear aromatic hydrocarbons (PAHs)
radon
tobacco smoke
-
The treatment issues for this patient are beyond the scope of this monograph, and treatment would not be recommended until further studies are completed. The patient should be referred to an oncologist and chest surgeon (if she is a surgical candidate) for evaluation before treatment. Depending on histologic type, local extension into adjacent anatomical structures, presence of metastases, and the general health of the patient, treatment options would include surgical excision, radiation, chemotherapy, and possibly immunotherapy.
Challenge
Challenge questions begin on page 4.
-
In addition to building location, the factors that influence radon gas entry into a home are
type and condition of the foundation
pressure differences between the soil and the inside of the home
building materials used
air exchange rate or ventilation
-
Anyone who spends a significant amount of time in the home would be at risk. Data are inadequate to assess individual susceptibility to radon-induced lung cancer; however, possible reasons to be additionally concerned about members of this family include that the patient’s daughter is a smoker, her grandson is still a child, and her husband has a past history of shipyard work with possible asbestos exposure. The amount of time spent at home by each family member should be considered. You might be concerned about her husband because exposures to both asbestos and radon may increase his risk of lung cancer significantly. Because he is retired, he may spend more time at home indoors, thus increasing his duration of exposure to radon.
-
No. Everyone in the community will not be exposed to the same radon level. Regional geologic differences such as granite deposits and soil structure are major determinants of indoor radon concentration; however, local variations can be great. Even assuming all homes in the community are built on the same geologic formation, the radon level in each home cannot be predicted. The only way to determine a home’s radon level is to test. The construction and condition of each house and the source of water supply may vary. Even if the neighbors were exposed to the same radon levels, they would not be at equal risk of health effects. The risk of lung cancer to each occupant does not depend only on the radon level, but also on the occupants themselves and their lifestyles.
-
The actions of radon and cigarette smoke are probably synergistic. For your patient’s daughter, who is a smoker, the risk of dying from lung cancer is 10 to 20 times greater than if she did not smoke. It is presently unknown how passive exposure to cigarette smoke affects the risk of developing lung cancer in relation to radon exposure.
-
No, it is unlikely that the fetus would be affected by airborne radon because alpha emitters act locally on the respiratory tract, and there are no firmly established systemic effects.
-
It is unlikely that radon would play any role in the development of mesothelioma because this is a malignancy of the pleural lining, not the lung. The risk for mesothelioma among asbestos workers is also not increased by smoking.
-
The test kit should be placed in the lowest lived-in level of the home (for example, the basement if it is frequently used, otherwise the first floor). It should be put in a room that is used regularly (like a living room, playroom, den or bedroom) but not your kitchen or bathrooom. Place the kit at least 20 inches above the floor in a location where it won’t be disturbed—away from drafts, high heat, high humidity, and exterior walls.
-
As a health professional, you can (a) motivate all smokers to quit smoking; (b) educate and act as a resource to patients regarding radon risks; (c) help families rank the risks of the many environmental pollutants they encounter; (d) refer the family to the health department, state radon office, or EPA for more information and relate to others your experiences in testing your own home; (e) encourage detection and mitigation of radon when indicated, and encourage appropriate building techniques for new construction.
-
There are currently no enforceable regulations to control indoor radon levels; therefore, there is no legal recourse. EPA recommends mitigation if the radon level indoors is above 4 pCi/L; the national goal is to reduce indoor radon levels to outdoor levels, about 0.4 pCi/L. Clearly the school’s classrooms exceed these levels. Education and persuasion of the citizenry are methods that may motivate the community to take remedial action.





















