
Occupational Asthma Due to Toluene Diisocyanate Among Velcro-Like Tape Manufacturers
Jung-Der Wang, MD, ScD, Ping-Hung Huang, MD, Jia-Ming Lin, PhD, Shyh-Young Su, BS, and Min-Chien Wu, MD
During September-November, 1985, four employees of a factory were seen at the occupational clinic complaining of cough, shortness of breath, and wheezing. All four worked in the same area of the factory where an adhesive containing toluene diisocyanate (TDI) was applied to velcro-like tape during manufacturing. To confirm the diagnosis of TDI-induced asthma and determine the prevalence among workers, 38 workers were interviewed and examined (84%) in the factory. Air samples were also taken from several areas in the factory to determine the TDI concentration. For analysis, the factory was divided into three areas based on the concentration of TDI: low (0.012±0.002 ppm), medium (0.021±0.006 ppm), and high (0.047±0.054 ppm). The distribution of workers with symptoms of asthmatic bronchitis was highly associated with TDI concentration (p<0.001). After stopping work for a period of 10 days, workers in areas with a high concentration of TDI showed marked improvement in pulmonary function tests (PFTs). After isolation of the exposure site, improvement of the ventilation system, and substitution of the TDI with less volatile diphenylmethane diisocyanate (MDI), air concentration of isocyanates was usually below 0.007 ppm. Three of the four clinically overt asthma cases went back to work without any difficulty. The PFTs of affected workers showed a significant improvement 5 months later. We conclude that TDI was responsible for the occupational asthma among velcro-like tape manufacturers and that the TDI-induced impairment of pulmonary functions was at least partially reversible.
Key words: TDI, asthma, isocyanates, MDI
INTRODUCTION
During September-November, 1985, four employees of a factory in Taipei County were seen in an outpatient clinic of the National Taiwan University Hospital complaining of cough, shortness of breath, chest tightness, and wheezing. The symptoms tended to be worse at night and improved after long holidays. All four employees worked in the same area in the factory where an adhesive was applied to the velcro-like tape during the manufacturing process. A review of all the processes
Reprinted with permission from American Journal of Industrial Medicine 14(1):73–8, Copyright 1988, Alan R. Liss, Inc.
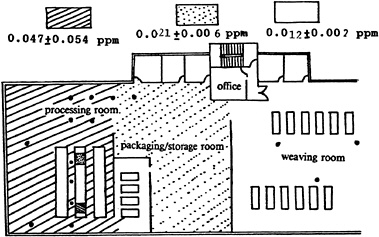
Fig. 1. Floor plan and distribution of TDI concentration in air samples of the velcro tape manufacturing factory. Big black dots indicate the place where samples were taken. ▨ indicates the place where the adhesive is applied to the tape; ![]() indicates the place where the adhesive is heated and dried.
indicates the place where the adhesive is heated and dried.
found that the adhesive resin contained toluene diisocyanate (TDI), a well-known cause of occupational asthma [NIOSH, 1978; Chan-Yeung and Lam, 1986; NIOSH, 1977b]. Because TDI-induced occupational asthma has never, to our knowledge, been documented in Taiwan, this study was conducted to determine the etiology and prevalence rate of this outbreak of workers’ asthma.
MATERIALS AND METHODS
The factory has 45 employees and has been in operation since 1984. Most of the employees were young women (median age 22 years). The female to male ratio was 3.2:1. The employees’ turnover rate was high; the average length of employment was 9.2 months. We tried to interview and examine all employees. Air samples were taken by midget impingers at different locations in the factory and they analyzed for TDI concentrations by colorimetric methods [NIOSH, 1977a]. Pulmonary function tests (PFTs) [Ferris, 1978] were also performed on workers, using a portable spirometer (Chest autospiror-298), during a usual workday, after a 10-day holiday, and 5 months after the improvement of the workplace by effective isolation and ventilation control. All tests were done in the morning (between 8:30–10:30 AM) at the factory office to avoid across-shift functional deterioration.
The factory was divided into three functional areas: the weaving area, where the tape is woven; the processing area, where the tape is dyed and the adhesive resin is applied; and the packaging/storage area. The three areas were connected through doors, with the packaging area in the middle of the other two (Fig. 1).
A case of asthma or asthmatic bronchitis was defined as any worker who
TABLE I. Incidence of Asthmatic Bronchitis Symptoms by Workplace and Air Concentration of Toluene Diisocyanate (TDI)*
developed symptoms of cough for more than 1 month and shortness of breath or wheezing for 1 month after working in this factory. Workers with a history of prior cardiovascular or pulmonary diseases, previous known exposure to pulmonary irritants, and previous smoking history were excluded from analysis.
Mantel extension for the test of trend [Mantel, 1963] and paired Student’s t-test were performed to evaluate the statistical significance.
RESULTS
Completed interviews and physical examinations were obtained for 38 of 45 (84%) workers; of these, four workers were excluded because of a smoking history. Among the remaining 34 workers, 14 met the case definition for asthma or asthmatic bronchitis. The highest attack rate occurred among workers in the tape processing area and the lowest was in the weaving area. Four of 14 cases of asthma compared with none of the noncases had wheezing rales on chest examination (p<0.0001). All four cases with auscultatory findings worked in the tape processing area.
Air samples collected from various locations in the factory revealed that TDI concentrations were highest in the tape processing area with a mean of 0.047±0.054 ppm (n=15), and lowest in the weaving area with a mean of 0.012±0.002 ppm (n=3). The packaging/storage area had intermediate levels of TDI with a mean of 0.021±0.006 ppm (n=3). A highly significant trend was noted between the increased concentration of TDI and the increased occurrence rate of asthma (Table I).
Since some workers left the company after the 10-day holiday, we successfully performed pulmonary function tests before and after holiday on only 21 workers, at the factory office between 8:30–10:00 AM before the start of work. Workers in the processing area had the greatest changes in pre- and post exposure FEV1 and FVC (Table II).
Based on the results of the investigation, we recommended that the factory install new ventilation hoods, improve the design of existing hoods, and isolate the process of applying TDI-containing adhesives to protect workers from TDI vapors. We also recommended the factory change the formula of the adhesive resin and substitute diphenyl methane diisocyanate (MDI) for TDI, because MDI has a higher vaporization temperature and a lower vaporization pressure [ACGIH, 1980]. Five months after these recommendations were implemented, workers were reexamined and air samplings were repeated. No worker complained of asthmalike symptoms. FEV1 and FVC measurements for 10 workers still employed at the time of follow-up
TABLE II. Change in Pre- and Postexposure One-second Forced Expiratory Volume (FEV) and Forced Vital Capacity (FVC) Among Employees Classified by Workplace
|
Workplace |
No. workers |
Change in FEV (mean±1 S.D., in ml) |
Change in FVC (mean±1 S.D., in ml) |
p-valuea |
||||
|
Processing |
9 |
−431±246 |
|
−334±279 |
|
|||
|
|
|
p=0.035 |
|
|
p=N.S. |
|
||
|
Packaging/storage |
4 |
−118+102 |
|
−146±123 |
|
p<0.005 |
||
|
|
|
p=N.S. |
|
|
p=N.S. |
|
||
|
Weaving |
8 |
+10±311 |
|
+36±145 |
|
|||
|
aStudent’s t-test; N.S.=not significant. |
||||||||
showed significant improvement in pulmonary function (Table III). The mean duration of employment of these workers before our examination was 7.7±4.6 months. Seven of 9 air samples showed undetectable concentrations of isocyanates; the other two samples were below 0.007 ppm at the processing area.
DISCUSSION
Diisocyanates are used quite extensively in many industries for manufacturing polyurethane resins of various physical properties, e.g., hard, flexible, or semirigid foams. They may cause irritation of eyes, respiratory tract, and skin. The irritation may be severe enough to produce bronchitis and pulmonary edema. It has been estimated that approximately 4.3–25% of workers exposed to an air level of .02 ppm TDI develop asthma. [Weill et al., 1981; Adams, 1975] Symptoms may develop weeks or months after exposure. Exposure to very low levels of TDI (<.005 ppm) may induce an asthmatic attack in individuals sensitized by previous exposure to TDI. Therefore, an IgE-mediated allergic mechanism has been postulated but not unequivocally confirmed as the cause of TDI-induced asthma [Chan-Yeung and Lam, 1986]. Another possible mechanism is through a pharmacologic reaction of the bronchus. In either case, the establishment of diagnosis may be through a bronchial provocation test [Pepys and Hutchcroft, 1975] or an epidemiological study. Because an epidemiologic approach can directly examine the workplace, we took this method and performed air measurements of TDI. The current threshold limit value (TLV) recommended by the American Conference of Governmental Industrial Hygienists is 0.005 ppm [ACGIH, 1986]. All 11 air samples originally taken in the processing area were above this level. The highest concentration measured, at the drying operation (Fig. 1), was 0.236 ppm, which was more than 47 times the TLV. The higher attack rates of asthmalike symptoms reported in our investigation may have been due to the difficulty in distinguishing true allergic cases from workers with other symptoms of pharmacologic reaction or pulmonary irritation, e.g., bronchitis, following exposure to high levels of TDI. We were able to show an objective reduction in pulmonary function for workers in areas with occasional high TDI concentrations. Both symptoms and pulmonary function tests improved after a period (10 days) away from the factory and also after improvements were made in the factory’s design and ventilation system. In fact, three of the four workers with clinically overt asthma went back to work without any symptoms. The fourth worker has not gone back to the factory, although she is currently asymptomatic and her lung function has returned to
TABLE III. Improvement in Pulmonary Function Tests Among Employees Under Different Working Conditions*
within normal. Therefore, we concluded that both asthma and other symptoms of pulmonary irritation were due to occupational exposure to TDI, and that the improvement in the work environment was effective.
Although some authors have reported that ventilatory functions may not fully recover among all sensitized workers after removal from TDI exposure [Adams, 1975; Weill et al., 1981], we did find a significant improvement of lung function among workers. Possible explanations for the discrepancy of these findings are: 1) many of our workers with symptoms of occupational asthma may not have been truly sensitized and developed symptoms simply because of the irritant effect of TDI; 2) our 10 workers had shorter durations of exposure to TDI, i.e., 7.7±4.6 months, which might only cause a more reversible effect.
This investigation clearly illustrates the impact of an occupational health hazard in a factory. The prevalence of occupational diseases in Taiwan is unknown but is probably high given the rapid industrialization and increased use of many potentially hazardous chemicals in manufacturing in recent years. At present, governmental agencies responsible for monitoring occupational diseases are grossly underfunded and understaffed. This investigation illustrates not only that occupational health problems exist in Taiwan, but they can often be remedied with minimal cost to industry. The key to improving occupational health among workers in Taiwan and elsewhere is to establish better procedures for licensing and inspecting factories and to train physicians and industrial hygienists to conduct proper health hazard evaluations and implement environmental control measures.
ACKNOWLEDGMENTS
This study was supported by a special grant from the Department of Health, Executive Yuan, R.O.C.
REFERENCES
Adams WGF (1975): Long-term effects on the health of men engaged in the manufacture of toluene diisocyanate. Br J Industr Med 32:72–8.
American Conference of Governmental Industrial Hygienists (ACGIH) (1980): “Documentation of the Threshold Limit Values.” Cincinnati: ACGIH Inc. 274–5, 401–2, 1–6(84).
American Conference of Governmental Industrial Hygienists (ACGIH) (1986): “Threshold Limit Values for Chemical Substances in the Work Environment Adopted by ACGIH for 1986–7.” Cincinnati: ACGIH.
Chan-Yeung M, Lam S (1986): State of the art: Occupational asthma. Am Rev Respir Dis 133:686–703.
Ferris B (1978): Epidemiology standardization project. Am Rev Respir Dis 118(suppl):55–88.
Mantel N (1963): Chi-square tests with one degree of freedom: Extensions of Mantel-Haenszel procedure. J Am Stat Assoc 58:690–700.
National Institute for Occupational Safety and Health (NIOSH) (1978): “Criteria for a Recommended Standard: Occupational Exposure to Diisocyanates, publication 78–215.” U.S. Dept of Health, Education, and Welfare.
National Institute for Occupational Safety and Health (NIOSH) (1977a): “NIOSH Manual of Analytic Methods.” U.S. Dept of Health, Education, and Welfare. 1:141–1.
National Institute for Occupational Safety and Health (1977b): “Occupational diseases: A guide to their recognition. Publication No. 77–181.” Washington D.C.: U.S. Government Printing Office 233–5.
Pepys J, Hutchcroft BJ (1975): State of the art: Bronchial provocation tests in etiologic diagnosis and analysis of asthma. Am Rev Respir Dis 112:335–65.
Weill H, Butcher BT, Dharmarajan V, et al. (1981): “Respiratory and immunologic evaluation of isocyanate exposure in a new manufacturing plant.” NIOSH Publication No. 81–125. NIOSH Technical Report, Washington DC: U.S. Government Printing Office.






