
ORL 50: 313-318 (1988)
© 1988 S. Karger AG Based
0301-1569/88/0505-0313$2.75/0
Acoustic Trauma Caused by the Telephone
Report of Two Cases
Jean-Philippe Guyot
Clinic of Otolaryngology, Head and Neck Surgery, Cantonal University Hospital, Geneva, Switzerland
Key Words. Acoustic trauma · Temporary threshold shift · Cord-type telephone · Cordless telephone
Abstract. Two patients with acoustic trauma resulting from the use of telephones have been evaluated. Both patients used a particular type of telephone which had the ringing device located in the ear receiver and no automatic gain control in the circuit. The output of the bell recorded on one of these telephones was in the 139-dB range on the A scale. The auditory insult resulted, in the case involving a cord-type telephone, from the transmission of a loud, extraneous sound probably due to a misfunction of the circuit and, in the second case, from the patient holding his cordless telephone against his ear when ringing occurred.
Acoustic traumata resulting from the use of cordless telephones have recently been reported. These telephones, in order to save space and weight, have the ringing device located within the ear receiver. There is no limiting circuit or automatic gain control either in the ringing device or in the earpiece transducer. Singleton et al. [1] reviewed 33 cases of hearing loss due to acoustic trauma from cordless telephones, cases collected either by him or by other members of the American Academy of Otolaryngology-Head and Neck surgery (AAO-HNS). In 30 patients the auditory insult resulted from the individual picking up the telephone when it was ringing and placing it to his ear without switching to the ‘talk’ mode. However, 3 patients used the telephone correctly; the injury resulted from a loud, extraneous crack sound which occurred while the telephone was used in the ‘talk’ mode. Most of these patients suffered from a permanent sensorineural hearing loss predominant in the low and midfrequencies. Subsequent reports have supported Singleton’s observation concerning this type of acoustic trauma [2, 3].
In Switzerland, the Federal Constitution has attributed the monopoly of telecommunications to the National Post-Telegram-Telephone Agency (PTT) [4]; only four accredited manufacturers provide telephones for the entire country and cordless tele-
Reprinted with permission from ORL 50(5):313–8, Copyright 1988, S.Karger AG Basel.
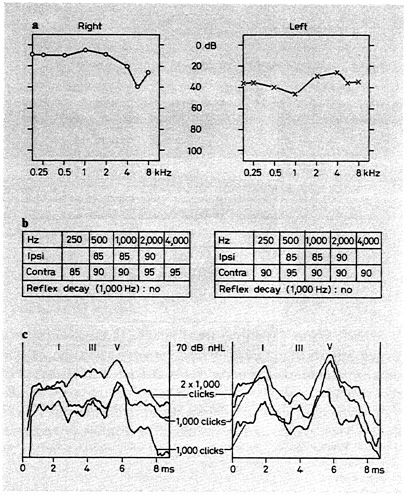
Fig. 1. Audiometrical results of the first patient suffering from an acoustic trauma due to a loud sound transmitted by a cord-type telephone. a Puretone audiogram. b Thresholds and decay of the stapedial reflex. c ABR (right ear on the left, left ear on the right). The audiogram shows a low and midfrequency sensorineural hearing loss of the left ear. The thresholds of the stapedial reflex are normal as well as the interwave intervals and amplitude ratios of the ABR.
phones are officially prohibited. Standards for maximum peak acoustic power (120 dB) are based on advice edicted by the International Telegraph and Telephone Consultative Committee (ITTCC). This present regulation is strict and thereby the ‘Caisse Nationale suisse d’Assurance en cas d’accident’ (National Insurance Company for Accidents, CNA) has not been notified of any case of hearing loss resulting from the use of telephones during the last two decades. However, in the past few years, unofficial telephones have become available on the market, thus escaping control by the PTT.
We report two cases of hearing loss in individuals using these unofficial devices. In 1 patient the auditory insult resulted from the transmission of a loud, extraneous crack sound by a cord-type telephone: this is the first case report of trauma caused by a non-cordless telephone.
Case Report
Case 1
A healthy 56-year-old woman was referred to the ENT Department of the University Hospital of Geneva on October 28, 1986. She had been treated for 3
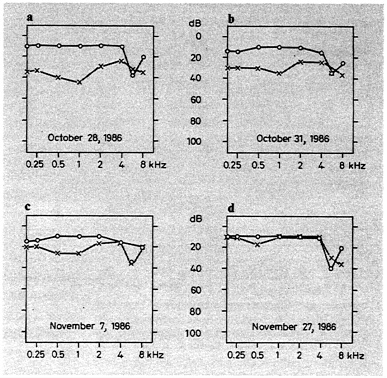
Fig. 2. Hearing thresholds of the first patient measured 6 h after the trauma (a), 3 days (b), 10 days (c) and 30 days after the trauma (d). The successive audiograms show the recovery of the hearing deficit due to a telephone-induced acoustic trauma within 4 weeks.
years for an idiopathic hypothyroiditis. That morning, she heard a loud crack sound in her left ear when answering the phone. She immediately complained of hearing loss and tinnitus in her left ear. The pitch of the tinnitus was subjectively comparable to the damaging noise perceived. The first audiometric evaluation was performed 6 h after the trauma occurred. The pure-tone audiometry demonstrated a midfrequency sensorineural hearing loss between 0.125 and 2 kHz. The auditory brainstem responses (ABR) showed normal interwave intervals and amplitude ratios. The thresholds of the stapedial reflex were normal (fig. 1) as well as the electronystagmography with caloric testing.
The tinnitus disappeared spontaneously after 3 days and her hearing gradually improved, with complete recovery within 4 weeks (fig. 2). The review of the cord-type telephone used by this patient revealed that it was made to receive several calls at the same time, and, like cordless units, had the ringing device located in the ear receiver. The ringing lasted 1 s. The peak impulse sound level of the ring was recorded on the A scale, using a standard 6-cm3 coupling for SPL (Bruel & Kjaer (B&K) 4152) connected to a B&K type
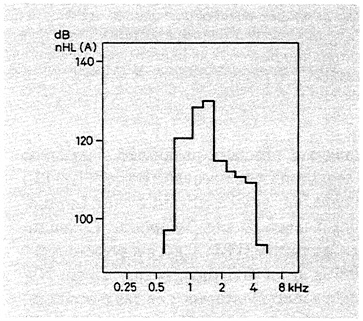
Fig. 3. Peak impulse sound of the ring of the cord-type telephone having caused the acoustic trauma in the first patient. The intensity of the ring of the cord-type telephone has been measured on the A scale using a standard 6-cm3 coupling for SPL (B&K 4152). The peak impulse sound reached 139.5 dB between 1 and 2 kHz.
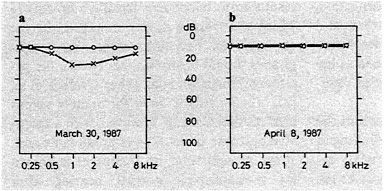
Fig. 4. Audiometrical results in the second patient who experienced acoustic trauma after exposure to the ring of a cordless telephone. a Audiogram obtained 3 weeks after the trauma showing a midfrequency sensorineural hearing loss of the left ear. b Audiogram obtained 4 weeks after the trauma showing the recovery to normal hearing 1 week later.
4145 1″ condenser microphone and a B&K sound level meter type 2218; it ranged from 134 dB in the ‘low talk’ position to a high of 139.5 dB in the ‘high talk’ mode. The fundamental frequency of this unit was 1,500 Hz (fig. 3). It was not possible to reproduce experimentally the extraneous crack sound heard by the patient.
Case 2
This young man was first seen in our ENT Department on April 6, 1987. Three weeks before, when using a cordless telephone, he omitted to switch to the ‘talk’ mode so that the bell rang directly into his left ear. He complained of an immediate hearing loss and tinnitus. The tinnitus disappeared within a few days. He noticed an improvement in his hearing level within 3 weeks but without complete recovery: he then came in for a medical visit. The pure-tone audiometry showed a midfrequency sensorineural hearing loss predominant between 1 and 2 kHz. The thresholds of the stapedial reflex and the electronystagmogram were normal. A second pure-tone audiometry, done 4 weeks after the acoustic trauma, revealed a normal hearing level (fig. 4).
Discussion
The midfrequency sensorineural hearing loss observed in both patients resembles the findings obtained in most of Singleton’s patients [1] emphasizing that a characteristic hearing loss results from this particular type of acoustic trauma. One case of significant loss in discrimination score without any significant change in pure-tone audiometry has been reported [3].
The hearing loss caused by cordless telephones results most frequently from the patient neglecting to switch from the normal ‘standby’ position to the ‘talk’ mode before placing the receiver to the ear so that the audiodevice will not continue to ring directly into the ear. In some instances, the injury has been reportedly caused by the transmission of a loud, extraneous crack noise likely resulting from a misfunction of the circuit of the phone. The case of our first patient illustrates that, although less frequent, this accident may also occur with cord-type telephones. The peak impulse sound level of the ringing was recorded up to 139.5 dB; it seems reasonable to assume that the accidental noise was transmitted at similar intensities. Such intensities are known to have a damaging effect on the inner ear. Most experimenters agree that mechanical factors are responsible for damage to the sensori-neuroepithelium at sound intensities higher than 120 dBA [5].
It is likely that other physicians have seen one or more isolated cases but have not
picked up on the midfrequency hearing loss, or paid any particular attention to them and therefore have not reported the cases. These accidents may easily be misdiagnosed as beginning Menière’s disease or sudden deafness due to viral infection.
The typical acoustic trauma notch in the 3- to 6-kHz range is not a common finding in this group of patients. This unfortunate experience with human subjects illustrates the findings of many experimental studies documenting the relation between maximum stimulation and maximum damage positions along the organ of Corti [6–8] by using pure tones or narrow band noises as stimuli. The morphological substrate underlying temporary threshold shifts (TTS) has been extensively studied with some controversial results. TTS may be detected without any significant ultrastructural change suggesting a metabolic disturbance; more intense stimulations result in temporary swelling of dendrites to inner hair cells. The resulting TTS lasts for several hours [9]. Vascular disturbances in the pathogenic sequences after an acute noise exposure have also been reported [10–13]. Changes in microcirculation may still be present 3 weeks after short-term and mild noise exposure [13]. In the light of the most recent studies, at the electron microscopy level, more subtle and consistent changes have been described. The most common finding observed in several different animal models [14–16] is depolymerization of the actin filaments at the base of the hair cells stereocilia reducing their stiffness which returned to normal within 6 weeks after exposure [16].
It is imperative that physicians and audiologists become aware of the potential hazard that telephones may produce under certain circumstances. The greatest danger results from telephones (cordless or not) in which the ringing device is located in the ear receiver. For this reason, these telephones should be prohibited. Unlike the patients of Singleton et al. [1] or Orchick et al. [2], our 2 patients have fortunately recovered normal hearing; however, such a favorable outcome is not always predictable and, at the present time, no treatment is known for reestablishing normal hearing after acoustic trauma.
References
1 Singleton, G.T.; Whitaker, D.L.; Keim, R.J.; Kemker, F.J.: Cordless telephones: a threat to hearing. Ann. Oto-Lar. 93:565–568 (1984).
2 Orchik, D.J.; Schmaier, D.R.; Shea, J.J., Jr.; Emmett, J.R.; Moretz, W.H.; Shea, J.J., III: Sensorineural hearing loss in cordless telephone injury. Otolaryngology 96:30–33 (1987).
3 Gerling, I.J.; Jerger, J.F.: Cordless telephones and acoustic trauma: a case study. Ear Hearing 6:203– 205 (1985).
4 Constitution Fédérale, article 36, 29 mai 1874.
5 Vertes, D.; Axelsson, A.; Hornstrand, C.; Nilsson, P.: The effect of impulse noise on cochlear vessels. Archs Otolar. 110:111–115 (1984).
6 Stockwell, C.W.; Ades, H.W.; Engström, H.: Patterns of hair cell damage after intense auditory stimulation. Ann. Otol. Rhinol. Lar. 78:1144– 1168 (1969).
7 Elliot, D.N.; McGee, T.M.: Effects of cochlear lesions upon audiograms and intensities discriminations in cats. Ann. Otol. Rhinol. Lar. 74:386– 408 (1965).
8 Clark, W.W.; Bohne, B.A.: Animal model for the 4-kHz tonal dip. Ann. Otol. Rhinol Lar. 87: suppl. 51 (1978).
9 Spoendlin, H.: Primary structural changes in the organ of Corti after acoustic overstimulation. Acta oto-lar. 71:166–176 (1971).
10 Kellerhals, B.: Pathogenesis of inner ear lesions in acute acoustic trauma. Acta oto-lar. 73:249–253 (1972).
11 Duvall, A.J.; Ward, W.D.; Lauhala, K.E.: Stria ultrastructure and vessel transport in acoustic trauma. Ann. Otol. 83:498–514 (1974).
12 Axelsson, A.; Vertes, D.; Miller, J.: Immediate noise effects on cochlear vasculature in the guinea pig. Acta oto-lar. 91:237–246 (1981).
13 Vertes, D.; Axelsson, A.; Lipscomb, D.M.: Some vascular effects of noise exposure in the chinchilla cochlea. Acta oto-lar. 88:47–55 (1979).
14 Tilney, L.G.; Saunders, J.C.; Egelman, E.; De Rosier, D.J.: Changes in the organization of actin filaments in the stereocilia of noise-damaged lizard cochlea. Hearing Res. 7:181–197 (1982).
15 Hunter-Duvar, I.M.: Morphology of the normal and the acoustically damaged cochlea. Scan. Elect. Micros. II Tri. 2:421–428 (1977).
16 Miller, J.; Canlon, B.; Flock, A.; Borg, E.: High intensity noise effect on stereocilia mechanics. Abstr. Midwinter Meet. Ass. Res. Otolar. 8:5 (1985).
Received: November 4, 1987
Accepted: November 9, 1987
Dr. Jean-Philippe Guyot
Clinic of Otolaryngology
Head and Neck Surgery
Cantonal University Hospital
24, rue Micheli-du-Crest
CH-1211 Geneva 4 (Switzerland)






