
5
RADIOBIOLOGIC PRINCIPLES AND RISK MODELING
Risk models serve the primary purpose of representing radioepidemiologic data, but they must also conform with established radiobiologic principles. Current models and the resulting risk estimates are in apparent or real conflict with such principles, in two main aspects that have led to a lack of transparency and to continued controversy. The two main aspects are linearity vs. curvilinearity and the dose dependence of RBE. Both are closely related to the problem of threshold versus linear nonthreshold dependence on dose for radiation-related excess cancer rates.
LINEARITY VERSUS CURVILINEARITY
One of the major disagreements between radiobiologic observations and current risk models concerns the shape of the dose-response curve for gamma radiation. In the majority of radiobiologic observations after photon irradiation—from chromosome and cell-inactivation studies to findings on animal tumors—dependence on dose is found to be curvilinear; often it is described as a linear-quadratic dependence. In contrast, at low to moderate doses (<<2 Gy) there is no apparent deviation from linearity in the excess rates of solid cancer among atomic-bomb survivors, the primary source of risk estimates (Thompson and others 1994; Pierce and others 1996). As a consequence, dose proportionality is often used in current models.
The International Commission on Radiological Protection (ICRP) has concluded that linear dependence on dose is inconsistent with radiobiologic findings. In its derivation of nominal risk coefficients for photons, ICRP has therefore used the dose and dose rate effectiveness factor (DDREF) to account for a postulated curvilinearity in dose or for an assumed dose-rate effect. The value 2 was adopted both for solid cancers and for leukemia in ICRP Publication 60 (ICRP 1991). It was stated that that was the highest value consistent with the data on solid cancers, and that for leukemias the value was fully consistent with the observations of atomic-bomb survivors. However, there have been no actual numerical evaluations.
There is an evident contradiction in the use of linear models in risk modeling and the reduction of the resulting values when they are used for risk estimation. Accordingly, a broader approach that incorporates the assumed DDREF directly into the numerical models themselves is required. One way to achieve that is to use models that are linear-quadratic in dose dependence and in the derivation of confidence regions for the resulting linear and quadratic coefficients, α and β.
Figure 1 exemplifies the approach in terms of exploratory computations for solid-cancer and leukemia mortality in Hiroshima (RERF 1994, 1997). A linear-quadratic dependence on dose is used that has the form ![]() , where Dγ is the gamma ray organ dose and Dn the neutron organ dose. R corresponds to the limiting relative biologic effectiveness (RBE) of neutrons at low doses and in these computations is assumed to equal 15, which is close to the current radiation weighting factor assumed for fission neutrons. There would be little difference in the results if the quadratic term were taken to be of the form b(Dγ. +Dn)2.
, where Dγ is the gamma ray organ dose and Dn the neutron organ dose. R corresponds to the limiting relative biologic effectiveness (RBE) of neutrons at low doses and in these computations is assumed to equal 15, which is close to the current radiation weighting factor assumed for fission neutrons. There would be little difference in the results if the quadratic term were taken to be of the form b(Dγ. +Dn)2.
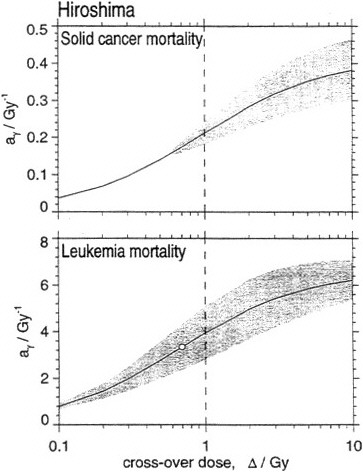
Figure 1. The gray areas give acceptable values (for the 95% confidence level) of parameter combinations aγ and Δ in linear-quadratic fit for all solid-cancer and all leukemia deaths in Hiroshima. ag: linear coefficient, that is, excess relative risk (ERR) per gray at low doses; Δ: 'crossover dose,' which equals ratio of linear and quadratic coefficient in the dose dependence for γ-rays. Diagrams are given for an assumed maximal RBE of neutrons R = 15. Data on solid cancers fit best to large values of Δ, that is, to linear dependence; but Δ = 1Gy cannot be rejected at the 95% confidence level, and this value corresponds to the DDREF = 2 assumed by ICRP. For leukemias, best estimate is obtained for Δ = 0.7 Gy, and this is fully consistent with DDREF =2.
The parameters aγ,, b, and R are estimated in terms of the familiar regression models. The results are comparatively insensitive to the value of R, and the resulting 95% confidence regions of the parameters are therefore given in Figure 1 for the value R = 15 which corresponds to current assumptions. Instead of the parameter b, the diagram gives the more familiar cross-over dose, Δ = aγ/b, that is, the photon dose where the quadratic component is equal to the linear component. Large values of Δ correspond to nearly linear dependence on dose, while small values belong to strongly curvilinear dependence. The value Δ = 1 Gy corresponds closely to the value DDREF = 2 which has been applied by the ICRP.
For all solid minors taken together, the best fit for this model is obtained for large values of Δ, that is, a linear dependence on dose. The excess relative risk is then 0.4/Gy, but the linear-quadratic dependence with crossover dose Δ = 1 Gy lies within the confidence region of the parameter estimates and corresponds, in agreement with DDREF = 2, to the excess relative risk 0.2/Gy. For leukemia, the best fit is obtained with Δ = 0.7 Gy, and this also agrees with DDREF = 2 relative to the purely linear dependence on dose.
The exploratory computations indicate that the present risk estimates, including the DDKEF = 2, are consistent with the Hiroshima data. The calculations are largely in line with an earlier analysis by Kellerer and Nekolla (1997). They are given here without detailed explanations because they are merely intended to indicate the general direction of more extensive and detailed evaluations of all available data that should be considered by a BEIR VII phase-2 committee. It might also be desirable to explore other options, such as true threshold models rather than the linear-quadratic dependence, for which analogous approaches can be used. An added feature that ought to be included in the modeling, and that can introduce some curvilinearity into the dependence on dose, is the use of newly developed techniques to account for errors in dose estimation.
THE DOSE DEPENDENCE OF RBE
The analysis of potential curvilinearity is, in the case of the atomic-bomb survivor data, inseparable from the issue of accounting for the RBE of neutrons. In past analyses, it has been common to treat neutrons as a minor contributor to the observed health effects and, in line with this assumption, to use the crude approximation of a simple dose-modifying factor. Instead of total absorbed dose, D = Dγ + D n, the approach uses a weighted dose, Dw = Dγ + wDn assuming that the RBE of neutrons is constant. The assumption of a constant RBE of neutrons is, however, directly in conflict with the universal observation—in almost all radiobiological investigations—that the RBE of neutrons assumes its highest values at low doses and decreases at larger doses. The use of the weighted dose Dw, in risk modeling is, accordingly, clearly at variance with basic radiobiological principles; it can be justified only as an approximation valid under the assumption that neutrons were minor contributors to the effects, even in Hiroshima.
That assumption remains tentative. If the current dosimetry system, DS86, is accepted, there is little likelihood that Hiroshima data and their comparison with Nagasaki data will permit conclusions on the contribution of neutrons to observed health effects. However, this does not imply that the contribution of neutrons must be minor in those who were exposed to low doses in Hiroshima. If a contrary conclusion was reached earlier in modeling, it was an artifact of using the weighted dose, Dw, even when a linear-quadratic dependence on dose was considered. To explain the problem, one needs to write out the linear-quadratic dependence on dose for the ERR. If the relation is formulated in terms of Dw, it takes the form:
The first two terms in the equation correspond-if one equates a with aγ and w with R—to equation 1, which is in line with radiobiologic findings and with an RBE of neutrons that decreases with dose. The last two terms, 2 b w Dγ Dn + b w2Dn2, however, are inconsistent with radiobiologic findings since neutrons exhibit a larger linear-, but not a larger quadratic-dose, component. Those terms therefore invalidate any exploration of curvilinearity of ERR with dose, except assumed small values of w.
The use of the realistic equation 1 for estimating the dose contribution from neutrons is, as has been shown (Little and Muirhead 1996; Kellerer and Nekolla 1997), unlikely to change the earlier conclusion (Preston and others 1991) that numerical values of the neutron RBE cannot be derived from data on the atomic-bomb survivors. But the added computations with the meaningful linear-quadratic dependence are desirable because, in contrast with earlier approaches, they can provide an inverse relation between photon and neutron risk estimates that results if various values of the RBE of neutrons are considered (Kellerer and Nekolla 1997). Figure 2 exemplifies, again in terms of explorative calculations for solid-cancer mortality in Hiroshima, the resulting dependence. The computations are constrained to ![]() , that is, the solutions are required to correspond to a DDREF of at least 2. The shaded area gives the resulting 95% confidence region for the absolute estimates of lifetime attributable fatality risk of solid cancers for photons and neutrons. The absolute risk coefficients are obtained by appropriate scaling of the excess relative risk aγ for photons and aγ R for neutrons. Values of the implicit parameter R are noted in the graph. Although no value of R can be rejected, there are slightly better fits for large values, as indicated by the standard-error region of the parameter combinations (heavy shading).
, that is, the solutions are required to correspond to a DDREF of at least 2. The shaded area gives the resulting 95% confidence region for the absolute estimates of lifetime attributable fatality risk of solid cancers for photons and neutrons. The absolute risk coefficients are obtained by appropriate scaling of the excess relative risk aγ for photons and aγ R for neutrons. Values of the implicit parameter R are noted in the graph. Although no value of R can be rejected, there are slightly better fits for large values, as indicated by the standard-error region of the parameter combinations (heavy shading).
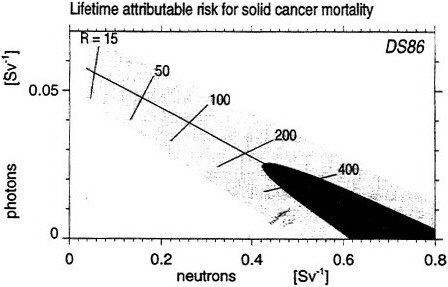
Figure 2. Absolute risk coefficients for mortality obtained from solid-cancer data in Hiroshima in terms of DS86 and the linear-quadratic relation of equation 1. Light and heavily shaded areas show 95% confidence and standard error regions of combinations of photon and neutron risk estimates. The calculations illustrate that the estimates of risk coefficients for protons and neutrons are inversely related; high RBE of neutrons cannot be excluded on the basis of the data but imply reduced risk estimates for photons. The values, R, of the neutron RBE at low dose that are considered here, must be distinguished from the radiation weighting factor, wR, which has been recommended by ICRP for the definition of the effective dose (unit: Sv). The risk coefficient for neutrons in the diagram is given per unit effective dose, taking wR=15 as the ICRP recommendation for the fission neutrons in Hiroshima1.
If R is assumed to equal the radiation weighting factor wR. =15 that corresponds, according to the ICRP recommendations to the fission neutrons in Hiroshima, the current risk estimates are approximated, both for photons and neutrons. For larger assumed values of R, the computation provides an upper bound to the absolute risk coefficient for neutrons which would be obtained if the RBE of neutrons were infinite, that is, if the
current dosimetry system (DS86) were valid and if all the excess cancer risk at Hiroshima were attributable to neutrons.
There are, in fact, more-severe restraints that exclude, with DS86, high values of R. Although not shown here, the calculations suggest, for larger values of R, there is not only a small linear component but also a vanishing quadratic component for gamma rays; this, however, is clearly inconsistent with the observations in Nagasaki, where there can be no doubt about substantial effects of the gamma rays at large doses. A combined analysis of the Hiroshima and Nagasaki data will thus be required and this will involve the consideration of added uncertainties, such as the still unresolved dosimetry of the factory workers in Nagasaki. As stated, the present exploratory computations are merely intended to indicate the general direction of the computational work that could be considered by a BEIR VII phase-2 committee.
Although the results in figure 2 must thus be seen as incomplete, they are important insofar as they indicate the inverse relation between photon and neutron risk estimates. This interrelation is disregarded in present use where the risk estimate for photons is taken to be substantially independent of the assumed RBE of neutrons and the neutron risk estimate is obtained as the product of the unchanged photon risk estimate and the assumed RBE of neutrons.
A scaling factor from excess relative risk to absolute risk has been used here that corresponds—in line with the model chosen by ICRP—to the assumption of a relative risk that does not decrease with time after exposure. More-realistic models will include such decreases and will lead to absolute risk estimates for solid-cancer mortality that are reduced by about a factor of 2 (Kellerer and Barclay 1992; UNSCEAR 1994).
POTENTIAL IMPACT OF NEUTRONS
The observations on the atomic-bomb survivors are the major basis for the estimation of radiation risks, but they are linked to a dosimetry system, DS86, that is still subject to uncertainties regarding the magnitude of the neutron component in Hiroshima. Activation measurements related to slow neutrons indicate an underestimation of neutron doses with DS86. A tentative modification of the neutron doses uses a correction factor, c(r), that depends on distance, r, from the hypocenter
where r is in kilometers (Straume and others 1992).
This correction would decrease the neutron contribution at high doses but substantially increase it in the low-dose region (see Figure 3). There is a possibility that accelerator mass-spectrometry measurements of nickel-63 in exposed copper samples—or the determination of another activation product of high energy neutrons—will, in the near future, provide additional evidence on high-energy neutrons at Hiroshima. In view of
that possibility, it is of interest for a BEIR VII phase-2 committee to consider potential implications of any suggested modifications to DS86 dosimetry for the risk estimates for survivors at Hiroshima and Nagasaki (Kellerer and Nekolla 1997).
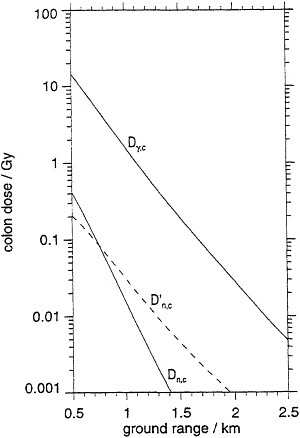
Figure 3. Dependence of the gamma ray and the neutron colon dose on distance from hypocenter in Hiroshima according to DS86 (solid lines) and neutron dose tentatively modified according to Straume and others (1992) (broken line). For conversion of kerma to organ dose, see Kellerer and Nekolla (1997).
Computations for solid-cancer mortality in terms of any modified dosimetry could provide new estimates of photon-and neutron-risk coefficients. Examples are shown in figure 4, which is analogous to figure 2.
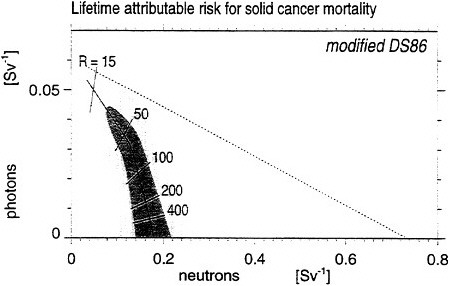
Figure 4. Absolute risk coefficients for mortality obtained from solid-cancer data in Hiroshima in terms of a tentatively modified DS86 and the linear-quadratic relation of equation 1. Light and heavily shaded areas show 95% confidence and standard error regions of combinations of photon and neutron risk estimates. The calculations illustrate that the estimates of risk coefficients for protons and neutrons are inversely related; high RBE of neutrons cannot be excluded on the basis of the data but imply reduced risk estimates for photons.
The results show that a modified dosimetry could exclude risk coefficients for neutrons that are substantially larger than now assumed. The broken line corresponds to the results shown in figure 2. See legend to figure 2 with regard to the difference between the parameter R and the radiation weighting factor wR, that is used in the definition of the effective dose of neutrons (in Sv).
With the dosimetry as modified here, roughly the same risk estimates are obtained for both photons and neutrons if a low neutron RBE, between 10 and 20, is assumed. Nevertheless, there are potentially major implications of any modified neutron dosimetry. The inverse relation between the risk coefficients for gamma rays and neutrons shows that very high values of neutron RBE would be consistent with the data. But they would correspond primarily to a largely reduced linear component in the dependence of dose due to photons, rather than an enhanced effectiveness of the neutrons. In fact, with this tentative modification, the solid-cancer data from Hiroshima would be consistent with a vanishing linear component for photons but a substantial quadratic component, that is, an effectiveness of gamma rays at larger doses in line with the Nagasaki observations. The maximal risk coefficient for neutrons, however, would differ little from the one now assumed.








